
Abstract
Introduction:
Angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs) are widely used to block the renin-angiotensin system (RAS). Yet it remains uncertain whether these drugs are equally effective and safe.
Methods:
Systematic reviews and meta-analyses of ACEis/ARBs in diabetes and kidney disease published in PubMed, Chinese National Knowledge Infrastructure (CNKI) and Wanfang databases were searched for clinical outcomes including all-cause mortality, end-stage renal disease (ESRD), hyperkalemia and cough.
Results:
Eight meta-analyses included 2177–61,264 patients with follow-up of 6–108 months. RAS blockers reduced mortality (relative risk ratio (RR), 0.90, 95% confidence interval (CI), 0.86–0.95) without heterogeneity. The death protection was significant specifically with ACEis (RR, 0.85, 95% CI, 0.79–0.91), but not with ARBs. Protection against ESRD was homogenously evident by ARBs (RR, 0.79, 95% CI, 0.73–0.87), ACEis (RR, 0.79, 95% , 0.64–0.94), and both (RR, 0.79, 95% CI, 0.73–0.87). Significant side effects were hyperkalemia by ARBs (RR, 2.44, 95% CI, 1.13–5.26), and cough by ACEis (RR, 2.38, 95% CI, 1.75–3.22)
Conclusions:
In patients with diabetes and kidney disease, ACEis and ARBs are consistently protective for the development of ESRD. Use of ACEis alone additionally reduces deaths and increases the risk for cough. Use of ARBs alone increases the risk for hyperkalemia without additional benefit of death protection.
Keywords
Introduction
Diabetes mellitus (DM) and kidney disease are strong independent risk factor for death and renal failure.1,2 Moreover, DM and kidney disease hasten vascular complications.3–6 The combination of diabetes and kidney disease relates to a two- to four-fold increase in the risk of cardiovascular disease and death.7–11 The renin-angiotensin system (RAS) plays a major role in cardiovascular and renal dysfunction.12–15 Thus, RAS blockade by angiotensin-converting enzyme inhibitors (ACEis) and angiotensin-receptor blockers (ARBs) has been shown to reduce all-cause mortality in DM and kidney disease.16–18
Recently, a meta-analysis has shown that ACEis and ARBs may exert different effects on all-cause mortality in DM patients. 19 Yet, it remains uncertain whether ACEis and ARBs have differential effects on all-cause mortality, end-stage renal disease (ESRD), and adverse reactions. The objective of this updated study is to perform a meta-analysis of meta-analyses to assess the comparative effects of ACEis and ARBs on all-cause mortality, ESRD, and adverse reactions in patients with DM and kidney disease.
Methods
Eligibility criteria
All studies that met the following criteria were included: (a) systematic reviews and meta-analyses; (b) patients with DM and kidney disease; (c) randomized controlled clinical trials of ACEis and ARBs (any dose or type); and (d) clinical outcomes including all-cause mortality, ESRD, and adverse events such as hyperkalemia (defined as plasma potassium in excess of 5.5 mmol /l), cough, and headache; (e) relative risk ratios (RRs) were calculated with corresponding 95% confidence intervals (CIs).
Exclusion criteria
Exclusion criteria included: (a) studies of patients with a diagnosis of acute kidney injury, as defined by an abrupt (within 48 h) reduction in renal function, manifested by an increase in serum creatinine level (≥0.3 mg/dl or ≥26.5 µmol/l) with or without reduced urine output (<400 ml/day ); (b) duplicated articles; and (c) meta-analysis not meeting the inclusion criteria. Eligibility assessment was performed independently by two investigators (JS, YMH), using pre-designed eligibility forms, with all questions resolved by consensus with other authors.
Search strategy and databases
This updated systematic review and meta-analysis is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. We selected relevant studies published between 1 January 1980–15 June 2015, by searching PubMed, Medline, Chinese National Knowledge Infrastructure (CNKI), Chinese Science and Technology Periodical Database, and Wanfang databases. All potentially relevant articles including reference lists of retrieved papers were investigated as full text in English. For ambiguous or missing information, we contacted the authors where possible. We used the following combined text and MeSH terms: “Angiotensin converting enzyme inhibitors,” “Angiotensin II receptor blockers,” “Renin-angiotensin system,” “Meta analysis,” “Diabetes mellitus,” and “Kidney disease”. We also did a manual search, using the reference lists of published articles. In the next step, the title and then the abstract of papers were examined. Duplicated articles were excluded, and then potentially eligible studies were retrieved for perusal in full text. The extracted data included first author name or study title, year of publication date, country of origin, number characteristics of participants, details of intervention, outcome measures, intervention durations, adverse events, and relative risk ratio (RR) with the corresponding 95% confidence interval (CI). All articles were read by two independent reviewers (XNS, XZH), who archived data from the articles according to a standardized data extraction form. Disagreements were resolved in all cases by discussion among our team members.
Quality assessment
The methodological quality of systematic reviews and meta-analyses was assessed by the Assessment of Multiple Systematic Reviews (AMSTAR) guidelines.20,21 This form of assessment has good inter-rater reliability, validity, and responsibility, and has been widely applied for measuring the methodological quality of systematic reviews. 22 Based on the recommendations of the Canadian Agency for Drugs and Technologies in Health (CADTH), those with score <4 were considered as low quality, 5–8 were considered as moderate, and 9–11 as high quality. 23 Two independent reviewers (JS, YMH) appraised the quality of the included reviews using AMSTAR scores. Each article was given an AMSTAR total score, based on the number of AMSTAR criteria that were fulfilled.24,25 A third reviewer (HLZ) served to resolve disputes.
Outcome measures
Outcomes were risks of all-cause mortality, ESRD, hyperkalemia (defined as plasma potassium in excess of 5.5 mmol/l), cough and headache.
Synthesis of data
Dichotomous outcome data from individual trials were analyzed by using RR measure and corresponding 95% CI. Data were pooled using the random-effects model when the heterogeneity was significant and the fixed effect model when the included studies showed homogeneity. We assessed the p value of the Chi-square test to determine heterogeneity and I2 to measure for inconsistency. Heterogeneity was assessed using the Chi-square test, with values greater than 50% regarded as being indicative of moderate-to-high heterogeneity and were calculated by using a random-effects meta-analysis model; 26 otherwise, we used the fixed-effects meta-analysis model. 27 The possibility of publication bias was quantified using the Begg’s and Egger’s test.28,29 A two-tailed p>0.05 was considered to show no bias. This was followed by confirmation with performing a visual inspection of Begg funnel plots in which RRs were plotted against their standard errors (SEs).
Results
Description of the included studies
The study selection process that resulted from our meta-analysis is shown in Supplementary Material, Figure 1. A total of 295 articles were initially identified. Eventually, eight meta-analyses met our inclusion criteria, enrolling 2177–61,264 (median, 21,871) patients.30–37 All the eight meta-analyses were published between 2005–2015 (Table 1). Two studies were conducted in China, three in Australia, one in England, one in New Zealand, and one in Thailand. Diabetes including diabetic kidney disease was found in seven studies and five studies concerned kidney disease including diabetic kidney disease. Four studies compared ARBs with placebo, and seven studies compared ACEis with control using other anti-hypertensive agents. The age of the participants ranged from 18–80 years. The duration of studies ranged from six months to nine years. Table 1 shows the characteristics of the meta-analyses included in the analysis.
Characteristics of the eight included meta-analyses.

ACEis: Angiotensin-converting enzyme inhibitors; ARBs: angiotensin receptor blockers.
Risk of bias within studies
As shown in Supplementary Material, Table 1, the range in the total AMSTAR score for the eight meta-analyses was 7–10 (theoretical range 0–11) and the mean (standard deviation (SD)) was 8.5 (0.77). Study quality in general was good: five of eight of studies had an AMSTAR score of ≥9, and the other three had an AMSTAR score of 7–8. Based on the recommendations of the CADTH, five studies were considered high quality, and three considered moderate quality.
Publication bias was quantified using the Begg’s and Egger’s test, p>0.05 was considered to be no bias. The p-values were 0.13 and 0.12 for all-cause mortality, 1 and 0.65 for ESRD, 1 and 0.79 for hyperkalemia, 0.73 and 0.45 for cough, and 0.30 and 0.28 for headache, indicating no evidence for publication bias.
Primary outcomes
All-cause mortality
Seven studies reported all-cause mortality (Supplementary Material, Table 2). Treatment with ACEis/ARBs significantly reduced all-cause mortality (RR: 0.90, 95% CI: 0.86–0.95), with homogeneity and consistency of the study results (I2=0.0%, p=0.618). Therefore, the fixed-effects model was used for statistical analysis (Supplementary Material, Figure 2(a)), the symmetric funnel plot suggested no significant publication bias (Supplementary Material, Figure 2(b)). Specifically, the level of death protection was significant by ACEis (RR: 0.85, 95% CI: 0.79–0.91, p<0.0001), but not ARBs (RR: 0.98, 95% CI: 0.89–1.07, p=0.579) (Figure 1(a)). No significant publication bias was found in the symmetric funnel plot (Figure 1(b)).

The differential effect of angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs) on the risk all-cause mortality in patients with diabetes and kidney disease. (a) Forest plot; (b) Funnel plot. CI: confidence interval; RR: relative risk ratio; SE: standard error.
End-stage renal disease
ESRD was the outcome in four studies (Supplementary Material, Table 3). Use of ACEis/ARBs reduced the risk of ESRD (RR: 0.79, 95% CI: 0.73–0.87, p<0.0001) (Supplementary Material, Figure 3(a)) in fixed-effects model analysis (I2=0.0%, p=0.814). The symmetry of the funnel plot revealed little publication bias (Supplementary Material, Figure 3(b)). As shown in Figure 2(a), the protection against ESRD was similar for ACEis (RR: 0.78, 95% CI, 0.64–0.94) and ARBs (RR, 0.79, 95% CI, 0.73–0.87). The funnel plot demonstrated publication bias unlikely (Figure 2(b)).

The differential effect of angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs) on the risk of end-stage renal disease in patients with diabetes and kidney disease: (a) forest plot; (b) funnel plot. CI: confidence interval; RR: relative risk ratio; SE: standard error.
Hyperkalemia
The pooled data of four meta-analyses (Supplementary Material, Table 4) showed an increased risk of hyperkalemia with the use of ACEis/ARBs (RR, 1.76, 95% CI, 1.04–2.97) (Supplementary Material, Figure 4(a)). The symmetric funnel plot suggested no publication bias (Supplementary Material, Figure 4(b)). In fixed-effects model analysis shown in Figure 3(a), the increased risk of hyperkalemia was attributed to ARBs (RR, 2.44, 95% CI, 1.13–5.26), but not ACEis (RR, 1.33, 95% CI, 0.65–2.71). Consistently, little publication bias was evident by the symmetric funnel plot (Figure 3(b)).

The differential effect of angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs) on the risk of hyperkalemia in patients with diabetes and kidney disease: (a) forest plot; (b) funnel plot. CI: confidence interval; RR: relative risk ratio; SE: standard error.
Cough
The synthesized data of four studies (Supplementary Material, Table 5) suggested an increased risk of cough by the treatment with ACEis/ARBs (RR, 2.27, 95% CI, 1.64-3.15) (Supplementary Material, Figure 5(a)). Concerning the significant heterogeneity between the four studies (I2=68.5%, p=0.023), we used the random-effects model for statistical analysis. Publication bias was not significant in the funnel plot (Supplementary Material, Figure 5(b)). In the random-effects model analysis shown in Figure 4(a), the increased risk of cough was attributed to the use of ACEis (RR, 2.38, 95% CI, 1.75–3.22) rather than ARBs (RR, 1.47, 95% CI, 0.72–3.03). The symmetric funnel plot suggested no significant publication bias (Figure 4(b)).
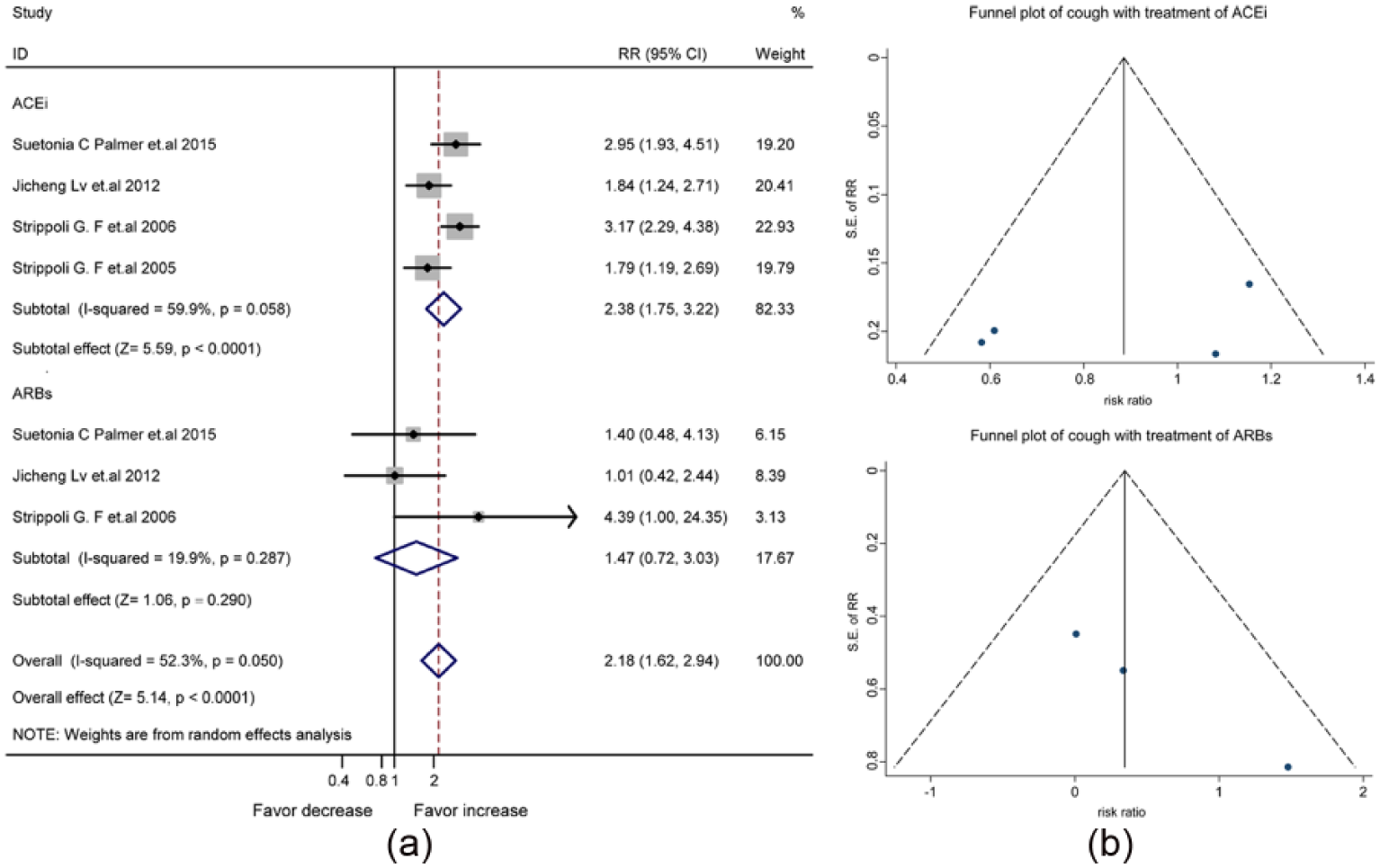
The differential effect of angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs) on the risk of cough in patients with diabetes and kidney disease: (a) forest plot; (b) funnel plot. CI: confidence interval; RR: relative risk ratio; SE: standard error.
Headache
The pooled data of three studies (Supplementary Material, Table 6) revealed that the risk of headache was not increased by the treatment with ACEis/ARBs (RR, 0.81, 95% CI, 0.61–1.08) (Figure 5(a)) in the fixed-effects model analysis (I2=0.0%). Consistently, the symmetric funnel plot suggested no significant publication bias (Figure 5(b)).

The mixed effect of angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs) on the risk of headache in patients with diabetes and kidney disease: (a) forest plot; (b) funnel plot. CI: confidence interval; RR: relative risk ratio; SE: standard error.
Discussion
In this updated meta-analysis of meta-analyses with moderate to high methodological quality, ACEis and ARBs are consistently protective for the development of ESRD in patients with diabetes and kidney disease, Use of ACEis alone additionally reduces the risk of death and increases the risk for cough. In contrast, use of ARBs alone increases the risk for hyperkalemia without additional benefit of death protection.
Patients with diabetes38,39 or kidney disease40–42 are at increased risk of death and renal failure. Prevalent in patients with diabetes or kidney disease is comorbidity with hypertension. ACEis and ARBs have been recommended for clinical treatment.43,44 Previous studies have demonstrated that ACEis and ARBs protect against the progression to renal failure in patients with kidney disease.44–46 In this updated meta-analysis, both ACEis and ARBs are protective for the development of ESRD in people with diabetes and kidney disease. Furthermore, ACEis are generally superior to ARBs in minimizing the risks of all-cause mortality and hyperkalemia. A major concern for the use of ACEis relate to the occurrence of cough. A possible rationale for the additional benefit of ACEis in contrast to ARBs on death protection may relate to angiotensin-(1-7).47,48 Moreover, ACEis also increase bradykinin levels to stimulate glucose metabolism 49 and trigger cough. In cases where the cough is intolerable, ARBs fit patients at risk of renal failure.
There are several potential limitations of this study. First, our results are subject to limitations inherent to any meta-analysis based on pooling data from different meta-analyses. Meta-analyses of ACEis and ARBs were not equivalent. Second, there is the possibility of overlap trials between the included meta-analyses. Third, substantial differences exist in the doses of the used drugs, duration of intervention, period of follow-up, and study population. It is hard to ensure quality control. Fourth, patients included in the reported meta-analyses have uneven baseline data, other concomitant conditions, and background therapies. These potential factors might have impacts on the interpretation of our findings.
Footnotes
Acknowledgements
The authors’ contributions were as follows: JS, YMH, and HLZ designed the study; JS collected and analyzed the data and wrote the manuscript; JS, MW, and XZH contributed to the collection and assembly of the data; WM, XZH, WL, and XXZ conducted the statistical analyses; JS, YNH, XZH, and HLZ interpreted the data; HLZ revised the manuscript and approved the submission. All authors agreed on the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Guilin Medical University (KY2011002), Program for Innovative Research Team of Guilin Medical University (PIRTGMU), National Natural Science Foundation of China (81270934, 81471054) and Innovation Project of Guangxi Graduate Education (YCSZ2015213).