
Abstract
Introduction:
The aim of this study is to evaluate whether the administration of renin-angiotensin system (RAS) inhibitors, angiotensin-I converting enzyme inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs), is associated with treatment outcome in patients with esophageal squamous cell carcinoma.
Materials and methods:
A total of 141 esophageal squamous cell carcinoma patients receiving esophagectomy were identified, and were divided into two groups: an ACEI/ARB group (n=20), and a non-ACEI/ARB group (n=121). The effect of ACEIs or ARBs on cell proliferation and vascular endothelial growth factor (VEGF) secretion of esophageal squamous cell carcinoma cell lines, CE81T/VGH and TE2, were investigated by 3-(4.5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide assay and Enzyme-linked immunosorbent assay (ELISA), respectively.
Results:
Use of ACEI/ARB (p=0.032), pathologic T stage (p<0.001), pathologic N stage (p=0.012), tumor stage (p=0.006), and tumor location (p=0.032) were significantly associated with superior overall survival. In multivariate comparison, use of ACEI/ARB (p=0.006), tumor stage (p=0.002), and tumor location (p=0.014) represented the independent prognosticators of superior overall survival. In cell lines, ACEIs/ARBs inhibit cell proliferation and VEGF secretion in a dose-dependent manner.
Conclusions:
ACEIs/ARBs administration is independently associated with superior overall survival in patients with esophageal squamous cell carcinoma receiving esophagectomy. Our data support further investigation of the role of RAS inhibitors as a potential therapy in esophageal squamous cell carcinoma.
Keywords
Introduction
Esophageal cancer is one of the most frequently occurring malignancies worldwide. In several Eastern and Asian countries, esophageal cancer is very common, and approximately 95% of esophageal cancers are squamous cell carcinomas. 1 Despite a significant improvement which has been made in surgical technique and chemoradiotherapy, the prognosis of patients with esophageal squamous cell carcinoma still remains unsatisfactory.2,3 The five-year survival of patients diagnosed with esophageal squamous cell carcinoma is less than 30%. 2 Therefore, the development of new targets for esophageal squamous cell carcinoma is worthwhile, especially those which already have available inhibitors.
The renin-angiotensin system (RAS) is associated with the regulation of blood pressure, and angiotensin I-converting enzyme inhibitors (ACEIs) and angiotensin II type 1 receptor blockers (ARBs) are some of the most widely used anti-hypertensive drugs. Lever and colleagues first reported that long-term use of an ACEI may protect against cancer in a retrospective cohort study, 4 and the potential role of the local RAS in tumor development and progression has received substantial attention. Previous studies showed that the angiotensin type 1 receptor is expressed in different malignancies, and has been reported to be significantly associated with tumor growth, metastasis, and angiogenesis.5,6 The local RAS is known to promote angiogenesis and proliferation via vascular endothelial growth factor (VEGF) or epidermal growth factor receptor (EGFR) expression,7,8 and ACEI/ARB suppress tumor progression by reduction of cancer proliferation and inhibition of neovascularization. Some studies also reported that treatment with ACEI/ARB combined with or without chemotherapy might improve clinical outcome in patients with various type cancers, including pancreatic cancer, urothelial cancer, and gastric cancer.9–12
However, to the best of our knowledge, there has been no study which investigated whether the administration of RAS inhibitors, such as ACEIs or ARBs, is associated with treatment outcome in patients with esophageal squamous cell carcinoma. In the present study, we retrospectively analyzed clinical outcomes in patients with esophageal squamous cell carcinoma receiving esophagectomy to clarify the impact of ACEIs and ARBs.
Materials and methods
Patient selection
A total of 1011 patients with esophageal squamous cell carcinoma at Kaohsiung Chang Gung Memorial Hospital between January 1996–December 2011 were retrospectively reviewed. The use of hypertension medication history including ACEIs and ARBs was retrospectively retrieved from the medical records. Of these 1011 patients, 141 esophageal squamous cell carcinoma patients receiving esophagectomy were identified. These 141 patients were divided into two groups: an ACEI/ARB group (n=20), and a non-ACEI/ARB group (n=121). The pathologic tumor stages were retrospectively determined according to the 7th American Joint Committee on Cancer (AJCC) staging system by a pathologist (WTH) in our hospital without any information about clinical and outcome data and outcome data. 13
Cell culture and 3-(4.5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide assay
Human esophageal cancer cell CE81T/VGH (CE81T), 14 a cell line derived from a well-differentiated squamous cell carcinoma of the esophagus, was obtained from the Bioresource Collection and Research Center (BCRC), and cultured in Dulbecco’s Modified Eagle Medium (DMEM) supplemented with 10% fetal calf serum, 2 mmol/l glutamine, 100 U/ml penicillin, and 100 µg/ml streptomycin. Human esophageal cancer cell TE2, 15 a cell line derived from a poorly differentiated squamous cell carcinoma of the esophagus, was a generous gift from Wen-Chien Huang (Mackay Memorial Hospital, Taipei, Taiwan), and cultured in Roswell Park Memorial Institute (RPMI)-1640 medium supplemented with 10% fetal calf serum, 2 mmol/l glutamine, 100 U/ml penicillin, and 100 µg/ml streptomycin. To test the effects of cell proliferation of ACEI (captopril) and ARBs (losartan, irbesartan), cells were plated into 96-well, flat-bottomed plates at 3×103 cells per 100 ml medium per well. After overnight incubation, triplicate wells were treated with captopril, losartan, or irbesartan with different concentrations for 24 h. The relative percentages of metabolically active cells compared with untreated controls were then determined on the basis of mitochondrial conversion of 3-(4.5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide to formazine. In brief, after incubation, 10 ml of 3-(4.5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (Sigma, St Louis, Missouri, USA) solution (5 mg/ml) was added to each well for 3 h, and then the medium was replaced with 150 ml of dimethyl sulfoxide per well. Results were assessed in a 96-well format plate reader by measuring the absorbance at a wavelength of 540 nm using a Titertek Multiscan (Thermo, Finland).
Enzyme-linked immunosorbent assay (ELISA) for VEGF
Cells were cultured for 6 h in serum-free medium with different concentrations of captopril, losartan, or irbesartan. the conditioned medium was collected and centrifuged at 15,000×g for 10 min, and the VEGF concentration in the supernatants was assayed using VEGF ELISA kit (R&D Systems, Minneapolis, Minnesota, USA) according to the manufacturer’s instructions.
Statistical analysis
Statistical analyses were performed using the SPSS 17 software package. The chi-square test and Fisher’s exact test were used to compare data between the two groups. Overall survival (OS) was calculated from the date of diagnosis to death as a result of all causes. Disease-free survival (DFS) was computed from the time of surgery to the recurrence or death from any cause without evidence of recurrence.
The Kaplan–Meier method was used for univariate survival analysis, and the difference between survival curves was tested by a log-rank test. In a stepwise forward fashion, parameters with p values<0.05 at univariate level were entered into Cox regression model to analyze their relative prognostic importance. For all analyses, two-sided tests of significance were used with p<0.05 considered significant.
Ethics statement
The retrospective analysis was approved by the Chang Gung Medical Foundation Institutional Review Board. Written informed consent of the patients or their family was not judged necessary for this kind of retrospective study by the Chang Gung Medical Foundation Institutional Review Board.
Results
Patient characteristics
Of these 141 esophageal squamous cell carcinoma patients receiving esophagectomy, there were 136 men and five women with a mean age of 55 years (range: 29–80 years). The median follow-up was 45.5 months for the 75 survivors (7.7–274.1 months), and the median overall survival was 31.4 months (3.6–274.1 months) for the all patients. The pathologic tumor stage revealed T1 in 49 (35%) patients, T2 in 31 (22%) patients, T3 in 60 (42%) patients, and T4 in 1 (1%) patients, and N0 in 82 (58%) patients, N1 in 50 (36%) patients, N2 in 7 (5%) patients, and N3 in 2 (1%) patients, respectively. Additional analyses according to AJCC 7th staging system demonstrated stage I tumors for 39 (28%) patients, stage II tumors for 57 (40%) patients, and stage III for 45 (32%) patients. Further analyses of histological grades showed a grade 1 lesion in 10 (7%) patients, grade 2 in 106 (75%) patients, and grade 3 in 25 (18%), respectively. Primary tumor location was found to be upper in 21 (15%) patients, middle in 54 (38%) patients, and lower in 123 (47%) patients.
Among these 141 patients, 29 patients received medication for hypertension and of these, 20 patients took an ACEI (n=5) or an ARB (n=15). Other anti-hypertensive drugs included beta-blockers (n=1), and calcium-channel blockers (n=8). The kinds and doses of antihypertensive drugs were decided by cardiologists in our institute. All patients with hypertension continued to receive these anti-hypertensive drugs at least six months after esophagectomy. The type of these anti-hypertensive agents is listed in Table 1. The characteristics of the ACEI/ARB group (n=20) and non-ACEI/ARB group (n=121) are shown in Table 2. Baseline characteristics did not differ significantly among these two groups, apart from at the pathologic N stage. Patients in the ACEI/ARB group had significantly more lymph node positive disease than those in the non-ACEI/ARB group (p=0.007).
Number of patients receiving antihypertensive drugs.
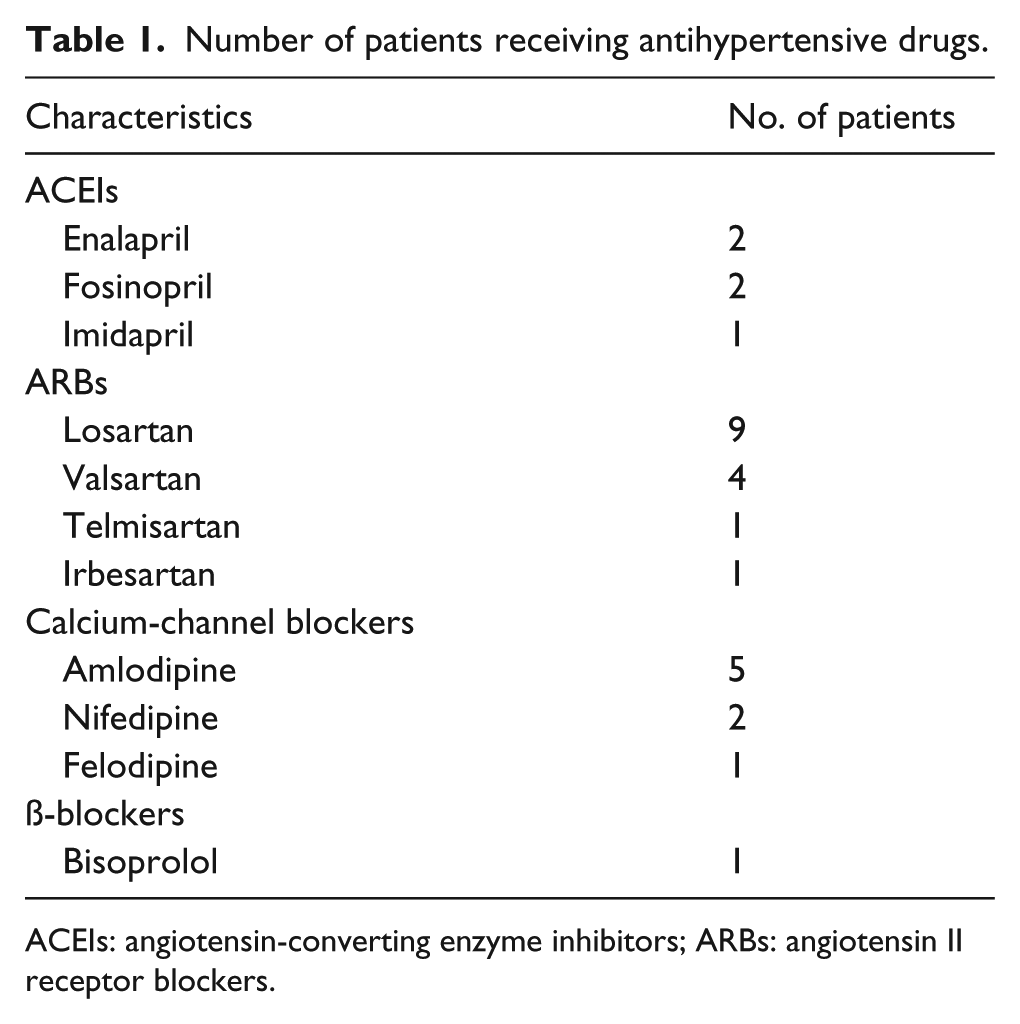
ACEIs: angiotensin-converting enzyme inhibitors; ARBs: angiotensin II receptor blockers.
Clinicopathological parameters in 141 patients with esophageal squamous cell carcinoma receiving esophagectomy according to angiotensin-converting enzyme inhibitor (ACEI)/angiotensin II receptor blocker (ARB) administration.

Statistically significant. Chi-squared test, or Fisher’s exact test was used for statistical analysis.
Impact of ACEIs/ARBs on clinical outcomes
In univariate analysis (Table 3), T1+2 (p=0.008), N0 (p=0.003), and stage I (p=0.001) were significantly associated with superior disease-free survival. Use of ACEI/ARB (p=0.032, Figure 1), T1+2 stage (p<0.001), N0 (p=0.012), stage I (p=0.006), and tumor location over middle or lower third esophagus (p=0.032) were significantly associated with superior overall survival. The median overall survival was 75.3 months and 58.3 months in the ACEI/ARB group and the non-ACEI/ARB group, respectively.
Risk factors for predicting disease-free survival and overall survival in 141 patients with esophageal squamous cell carcinoma receiving esophagectomy.

ACEIs: angiotensin-converting enzyme inhibitors; ARBs: angiotensin II receptor blockers; CI: confidence interval; HR: hazard ratio.
Statistically significant.

The Kaplan–Meier survival curves are plotted to predict overall survival in the 141 esophageal squamous cell carcinoma patients receiving angiotensin-I converting enzyme inhibitor (ACEI)/ angiotensin II receptor blocker (ARB) or not.
In multivariate comparison, stage I (p=0.006, odds ratio (OR): 0.44, 95% confidence interval (CI): 0.24–0.79) were significantly associated with increased disease-free survival. Use of ACEI/ARB (p=0.006, OR: 0.28, 95% CI: 0.11–0.70), stage I (p=0.002, OR: 0.38, 95% CI: 0.21–0.71), and tumor location over middle or lower third esophagus (p=0.014, OR: 0.45, 95% CI: 0.23–0.85) represented the independent predictive factors of superior overall survival.
RAS inhibitors suppress cell proliferation and VEGF secretion in esophageal squamous cell carcinoma cell lines
Our clinical data showed that the use of ACEIs or ARBs is significantly associated with the prognosis in patients with esophageal squamous cell carcinoma. Therefore, we tested whether the RAS inhibitors, captopril, losartan, and irbesartan, can inhibit cell proliferation and VEGF secretion in esophageal squamous cell carcinoma cell lines, CE81T/VGH and TE2. Captopril, losartan, and irbesartan all displayed a growth-inhibitory effect (Figure 2) and inhibited VEGF secretion (Figure 3) in a dose-dependent manner in esophageal squamous cell carcinoma cell lines, CE81T/VGH and TE2.

Angiotensin-I converting enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB) display a growth inhibitory effect in a dose-dependent manner in two esophageal squamous cell carcinoma cell lines: (a) irbesartan in CE81T/VGH cells; (b) irbesartan in TE2 cells; (c) losartan in CE81T/VGH cells; (d) losartan in TE2 cells; (e) captopril in CE81T/VGH cells; (f) captopril in TE2 cells. *Significant difference in growth inhibition. Columns: mean; bars: standard deviation.
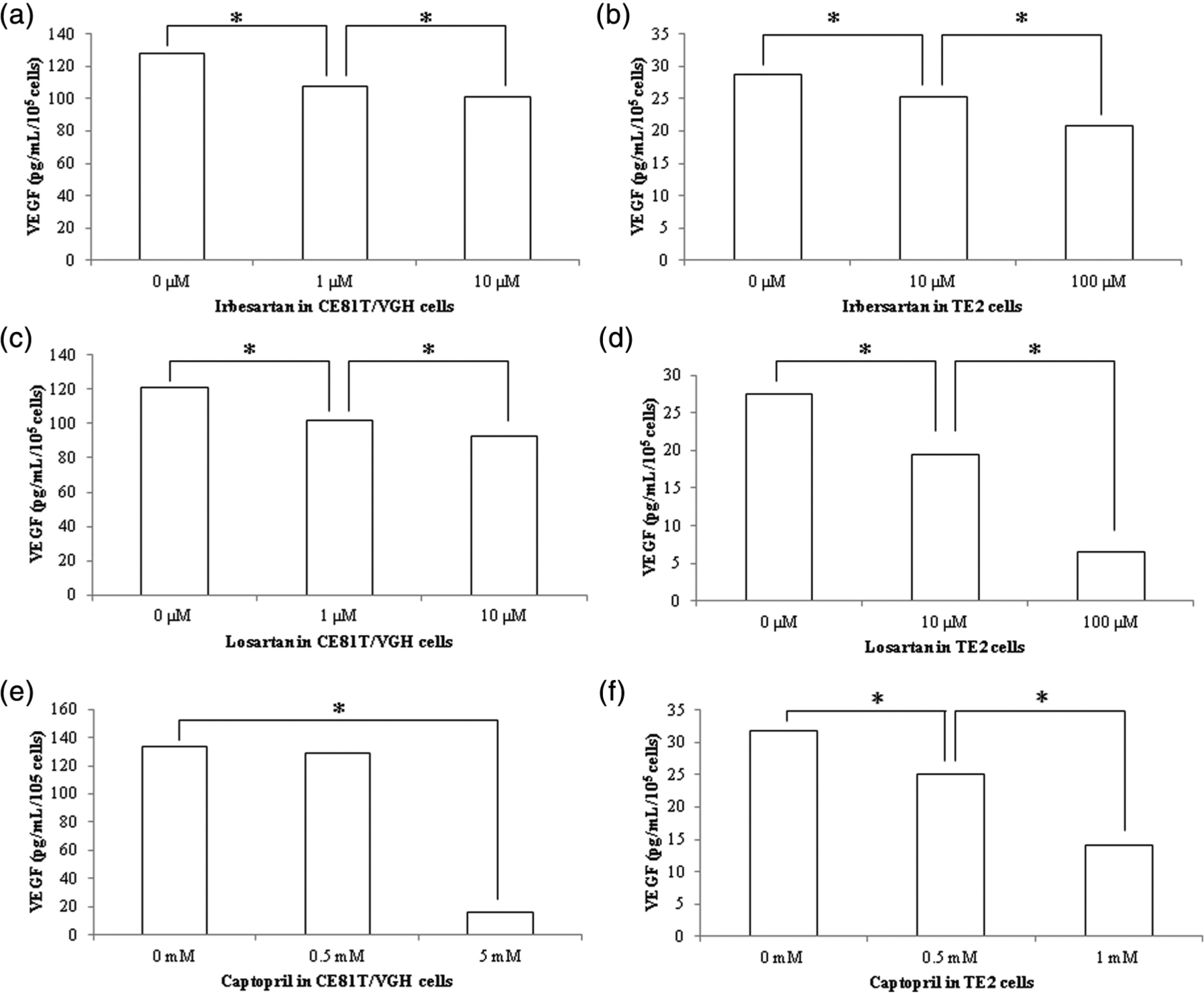
Angiotensin-I converting enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB) inhibited vascular endothelial growth factor (VEGF) secretion in a dose-dependent manner in two esophageal squamous cell carcinoma cell lines: (a) irbesartan in CE81T/VGH cells; (b) irbesartan in TE2 cells; (c) losartan in CE81T/VGH cells; (d) losartan in TE2 cells; (e) captopril in CE81T/VGH cells; (f) Captopril in TE2 cells. *Significant difference in VEGF secretion.
Discussion
In the era of hypertension treatment, RAS inhibitors, such as ACEIs or ARBs, are widely used. There has been an increase in the number of reports which emphasize the importance of RAS inhibitors in organ protection, in conditions such as diabetic nephropathy, diabetic retinopathy, and cardiac hypertrophy. 16 With respect to anti-tumor effects, Lever et al. first reported that long-term use of ACEIs may protect against cancer in a retrospective cohort study, but no significant association was found with the use of other antihypertensive drugs. 4 Since then, several studies have recognized the potential role of the local RAS in the clinical impact of several types of cancer treatment.9,10,12,17,18 To the best of our knowledge, this retrospective study is the first report to clarify the clinical outcome of the use of ACEIs or ARBs in esophageal squamous cell carcinoma.
In our study, we investigated the use of ACEIs/ARBs and other standard prognostic factors in 141 patients who underwent esophagectomy. Patients with T1+2, N0 or stage I had superior survival compared with those with ≥T3, ≥N1 or stage II+III in our analysis. It was reasonable that patients with early stage survived for longer than those with advanced stage. 19 In addition, we found that tumor location was associated with patient outcome. Kato et al. also reported that there were less R0 resections for tumors with higher location. 20 Nowadays, tumor invasion (T stage), numbers of lymph node involvement (N stage), and tumor location have been incorporated into the 7th AJCC staging system.13,21 Our findings were similar to previous results. Most importantly, the Kaplan-Meier analysis in the present study showed that patients administered ACEIs or ARBs had a significant survival benefit. Several studies have investigated the clinical impact of RAS inhibitors in different cancers. Nakai et al. reported the use of an ACEI or ARB in combination with gemcitabine was an independent prognostic factor for both progression-free survival and overall survival in advanced pancreatic cancer patients. 9 Sjoberg et al. reported that the use of ACEIs might decrease the risk of developing esophageal adenocarcinoma. 17 Wilop et al. reported that addition of an ACEI or ARB to platinum-base first line chemotherapy might contribute to prolonging survival in patients with advanced non-small-cell lung cancer. 18 Two prospective studies also showed that use of a ACEI or ARB was effective as a salvage therapy in the treatment of renal cell carcinoma and prostate cancer.22,23 Our results further support previous clinical findings.
To date, the role of adjuvant therapy in patients with resectable esophageal squamous cell carcinoma is still controversial.24–26 In our study, Kaplan-Meier analysis showed that patients administered ACEIs or ARBs had significantly superior survival compared to patients in the non-ACEI/ARB group, and the median survival was 75.3 months and 58.3 months, respectively. The use of an ACEI or ARB was an independent prognosticator of superior overall survival. Our results suggest that ACEIs or ARBs may be considered as potential adjuvant treatment for esophageal squamous cell carcinoma patients receiving esophagectomy.
The local RAS is known to promote angiogenesis and proliferation via VEGF or EGFR expression,7,8 and previous preclinical studies reported that tumor development and progression were influenced by ACEIs or ARBs in glioma, breast cancer and head and neck cancer.8,27–29 However, little is known about the effect of the RAS inhibitors in esophageal squamous cell carcinoma. Wang et al. reported that ACEIs suppress new vessel formation and inhibit tumor growth of esophageal carcinoma xenograft. 30 In that study, the ACEI treatment group showed significant higher tumor inhibitory rate (p<0.05) and less vascularization (p<0.05) than the control group. In our study, ACEI (captopril) or ARBs (losartan, irbesartan) both demonstrated dose-dependent inhibition of cell proliferation and VEGF secretion in esophageal squamous cell carcinoma cell lines, CE81T/VGH and TE2. These results indicate that the RAS inhibitors may serve as a new therapeutic approach for esophageal squamous cell carcinoma.
Our study had several limitations. First, it was a retrospective study in a single institute and the sample size was small, so unknown sources of bias may exist in the findings. Second, due to the limitation of small sample size of patients with ACEIs or ARBs, the difference in doses or types of ACEIs/ARBs was not fully evaluated.
Conclusions
The results of our retrospective analysis suggest that ACEI or ARB administration may improve clinical outcomes in patients with esophageal squamous cell carcinoma. A prospective clinical trial with larger population is warranted in order to clarify the role of RAS inhibitors in the treatment of esophageal squamous cell carcinoma.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by grants from the Chang Gung Memorial Hospital (CMRPG8B1261 and CMRPG8B0431).