
Abstract
We report a case of prenatal exposure to angiotensin II receptor antagonists (ARA II) from the beginning of pregnancy in a patient with a hypokinetic dilated cardiomyopathy. This case report emphasizes the fetal renal impact of prolonged intrauterine exposure to renin-angiotensin system (RAS) blockers, and highlights that this exposure can cause severe prenatal hypocalvaria. This delayed ossification can be reversible after birth, but the presence of anhydramnios indicates an early and irreversible block of RAS blockers in the fetus that is responsible for fetal kidney development abnormalities. This association carries a high risk of neonatal death. Prolonged exposure to ARA II or other RAS blockers remains prohibited throughout pregnancy.
Keywords
Introduction
Prenatal exposure to angiotensin II receptor antagonists (ARA IIs) cases are rare. Regarding fetal exposure to ARA IIs during the first trimester of pregnancy, the data are rather reassuring. Studies suggest that ARA IIs are not major teratogens when used during the first trimester.1–4
On the other hand, several case reports on renin-angiotensin system inhibitor fetopathies, including those caused by ARA IIs, were reported when they had been used beyond the first trimester of pregnancy.2,5–19 Our case highlights hypocalvaria and other fetal complications related to ARA II exposure throughout pregnancy. Current recommendations support a therapeutic class substitution in women treated with ARA IIs if pregnancy is desired. 20
The prognosis of children exposed in utero is not confined solely to the risk of neonatal renal failure. Indeed, skull ossification defect is a severe side effect that worsens the neonatal prognosis.5,21 This delayed ossification is encountered during prolonged prenatal exposure throughout pregnancy. It is secondary to chronic hypoxia related to arterial hypotension induced by arterial vasodilatation of the ARA IIs.22,23
Case report
A 34-year-old patient is hospitalized at 23 weeks of gestation (WG) for an evaluation of a severe intrauterine growth restriction associated with anhydramnios. This is the patient’s second pregnancy. She did not encounter any problems during her first pregnancy.
She received an ARA II (candesartan 16 mg/day) and a beta-blocker (bisoprolol 5 mg/day) because of dilated cardiomyopathy caused by two distinct processes: a probable toxic cardiomyopathy secondary to anthracycline chemotherapy in childhood for the treatment of an abdominal neuroblastoma; and peri-partum cardiomyopathy developed after her first pregnancy. Before the first pregnancy, there was no evidence of cardiac impairment. This cardiomyopathy was discovered 8 days postpartum when the patient had cardiogenic shock with a left ventricular ejection fraction of 25%.
Despite our advice following a risk assessment, the patient became pregnant while she was being treated with ARA IIs. At this time, her left ventricular ejection fraction was 45%. Owing to maternal chronic heart failure and poor clinical tolerance of angiotensin-converting enzyme inhibitors, the ARA II treatment could not be suspended or replaced. Although information was given about the risk of maternal cardiac function aggravation throughout pregnancy and the risk of prolonged prenatal ARA II exposure for the fetus, the couple decided to pursue this pregnancy. The first trimester obstetrical ultrasound performed at 11 weeks’ of gestation (WG) was unremarkable. An early fetal growth restriction was noted from 18 WG with a normal amniotic fluid volume and no unusual morphological element. The kidneys were seen and had a normal echopattern.
At 23 WG, the fetus had a growth restriction below the third percentile, anhydramnios, echogenic bowel and a disorder of the renal corticomedullary differentiation with a hyperechogenic renal parenchyma. The skull aspect was unusual and deformable under the probe with a major delayed ossification of the parietal bones and the occipital vault (Figures 1–3; Video 1). Cerebral morphology was normal for the age of the pregnancy. The dosage level of candesartan was lowered to 8 mg per day but it had no effect on the resumption of the fetal diuresis. A caesarean section was recommended at 26 weeks and 4 days of gestation due to maternal heart function deterioration with a left ventricular ejection fraction of about 15%. The couple was informed about the risk of a difficult resuscitation at this very early term associated with the risk of pulmonary hypoplasia and an impaired renal function. The patient gave birth to a male infant weighing 700 g who died at 3 minutes of life due to inefficient ventilation resulting from the expected major pulmonary hypoplasia. He presented a Potter sequence secondary to the prolonged anhydramnios, as well as an absence of occipital scale. X-rays and an autopsy were refused by the couple.

Major delayed ossification of the fetal cranial vault visualized in 2D ultrasound. The skull aspect is irregular, deformable under the probe with a punctuated aspect of the parietal ossification.
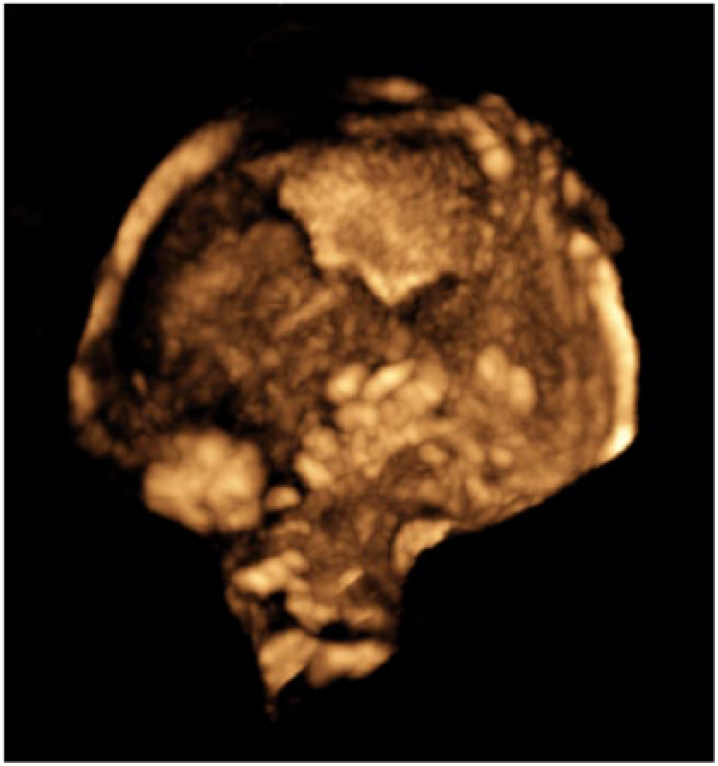
Volume reconstruction of the fetal skull confirming the absence of ossification of the occipital scale with enlarged fontanelles.

Echogenic bowel visualized in 2D ultrasound secondary to a probable ischaemic injury.
Discussion
In cases of prolonged exposure to ARA II, the association of a delayed ossification of the skull with anhydramnios gives a poor prognosis. All the prenatal malformations described are secondary to prolonged block of the renin-angiotensin system (RAS) in the fetus. 21 They are also described in some forms of tubular dysgenesis associated with well-known genetic mutations of RAS components. 24 The consequences of this exposure are not systematic and obstetrical ultrasounds can be normal throughout pregnancy. 6 Human studies regarding the fetotoxicity of a maternal exposure to ARA II are rare. No studies have examined the prenatal semiology according to the type of ARA II or the duration of the exposure. It is reported that candesartan has a higher affinity for angiotensin compared to other ARA IIs with a greater risk of fetal toxicity.12,25
This delayed ossification is mainly found when the fetus is exposed to ARA IIs from the second trimester of pregnancy. The chronic hypoxia secondary to the arterial hypotension induced by the ARA IIs can explain this delayed ossification. Indeed, the prolonged hypoxia limits the angiogenesis and growth of the membranous bones. These hypoxic consequences can also manifest as growth restriction or diffuse ischaemic phenomena, in particular in the digestive system, which is sensitive to variations in oxygenation. The inhibition of some osteoblast growth factors could be another physiopathological hypothesis to explain the delayed ossification.22,23 This same theory is also encountered in cases of hereditary proximal tubulorenal dysgenesis. 26 This ossification defect of the skull bones can be detected by ultrasound and predominates on the occiput without any repercussions for brain development. 27 Bones usually retain a normal shape and position but become hypoplastic. The sutures and fontanelles are symmetrically enlarged. 22
This delayed ossification may be reversible after birth.2,6,15–17 According to the literature
Neonatal prognosis of newborns with prenatal exposure to ARA IIs and hypocalvaria at birth.

WG : weeks of gestation; GA: gestational age; g: grams; FGR : fetal growth restriction; RTD: renal tubular dysgenesis; Supposed*: pulmonary hypoplasia is supposed in front of respiratory distress at birth; ARF : acute renal failure; CRF : chronic renal failure; D: day; M: month; + : presence; - : absence; NE : non-evaluated.
The most common fetal complication related to ARA II exposure remains renal toxicity. 30 The first ultrasound sign to look for is oligoanhydramnios linked to anuria complicating renal failure.6,7,22 Fetal anuria may be responsible for an authentic Potter sequence including pulmonary hypoplasia, facial dysmorphism and deformities of the extremities.5–9,21–23,31 The kidneys can be hyperechoic and increased in volume with or without a disorder of the corticomedullary differentiation.5–10,21,32 These images can be explained by a diffuse dilatation of the renal distal tubules or the presence of cortical cysts. 8 Many studies do not find any association with abnormalities of the urinary tract.7,9,10,32
It should be noted that the global fetal toxicity of ARA IIs is clearly demonstrated when they are prescribed during the second and third trimesters of pregnancy. Fifteen studies describing cases of prolonged ARA II fetal exposure are available in the literature.2,5–16,18,19 The neonatal mortality rate remains very high. Thus, out of 29 cases of antenatal exposure to ARA IIs, 7 postnatal deaths, 3 intrauterine fetal deaths, 5 medical terminations of pregnancy and 14 live births have been reported. Of these 29 cases, 26 cases of oligoanhydramnios were discovered during obstetrical ultrasound. Neonatal anuria is found in 11 out of 21 born alive newborns. Of these 11 live newborns with anuria, 64% died within a few hours or days (n=7). Pulmonary hypoplasia was found in 6 out of 29 cases: two of these died in utero and two were born alive but died within a few hours or days (67%). Finally, hypocalvaria was found following clinical or fetopathological examination in 16 out of 29 cases. Therefore, it appears that neonatal anuria and pulmonary hypoplasia are key elements in neonatal prognosis. In addition, oligohydramnios was shown to be reversible in many cases after discontinuation of ARA II treatment with favourable outcomes, although long-term outcomes have not yet been systematically assessed.
Conclusion
This observation underlines the absolute necessity to offer a preconception counselling appointment to women treated with RAS blockers. Fetal consequences secondary to a prolonged exposure to ARA IIs mimic tubular dysgenesis associated with genetic abnormalities of the RAS. The global fetal impact may be significant if the ARA II is continued beyond the first trimester. The delayed ossification that predominates at the level of the cranial vault can be detected in utero by ultrasound and remains a predictor of a poor prognosis when it is associated with oligoanhydramnios.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.