
Abstract
Objectives:
To clarify the association of angiotensin-converting enzyme (ACE) gene deletion/insertion polymorphism with risk of pregnancy-induced hypertension.
Methods:
We systematically searched China National Knowledge Infrastructure, Wanfang database, Chongqing WeiPu database and PubMed up to March 2014 to collect related case–control studies. RevMan 5.0 software was used for meta-analysis after evaluating the quality of enrolled studies and extracting the data.
Results:
A total of 45 case–control studies was selected, including 10,236 subjects. The meta-analysis was assessed by odds ratios (ORs) and 95% confidence intervals (CIs) after genotype consolidation. In total, D allele vs I allele: OR 1.57, 95% CI 1.33–1.86; genotype DD vs genotype II + DI: OR 1.86, 95% CI 1.48–2.32; genotype II vs genotype DI + DD: OR 0.65, 95% CI 0.53–0.80. In the Asian population, D allele vs I allele: OR 1.80, 95% CI 1.36–2.38; genotype DD vs genotype II + DI: OR 2.25, 95% CI 1.53–3.30; genotype II vs genotype DI + DD: OR 0.56, 95% CI 0.41–0.76. In the Caucasian population, D allele vs. I allele: OR 1.24, 95% CI 1.08–1.44; genotype DD vs. genotype II + DI: OR 1.25, 95% CI 1.10–1.41; genotype II vs. genotype DI + DD: OR 0.96, 95% CI 0.83–1.11.
Conclusion:
The ACE gene insertion/deletion polymorphism is associated with the risk of pregnancy-induced hypertension.
Introduction
Pregnancy-induced hypertension (PIH) seriously affects the life safety and quality of life of mothers and infants. A large-scale study found that the probability of death of mothers diagnosed with PIH after pregnancy was significantly higher than that of normal pregnant women. 1 In addition, PIH is often combined with a number of other diseases, such as pulmonary oedema and liver dysfunction, which also increase the risk of death for pregnant women. 2 Angiotensin-converting enzyme (ACE) is a key enzyme of the renin–angiotensin system. ACE can convert angiotensin I into a strong vasoconstrictor, angiotensin II, and can inactivate the vasodilator bradykinin peptide, playing an important role in vascular physiological regulation. 3 Many studies4–6 currently show that ACE activity is significantly elevated in the serum of patients with PIH, whereas the ACE gene can modulate ACE activity in serum and tissues. 7 Therefore, the study of the ACE gene polymorphism has become an important research topic in the pathogenesis of PIH.8, 9 However, as a result of the difference in the distribution of the ACE gene in different races and regions, different statistical methods and different sample sizes in each study, the findings are inconsistent.
In this study, we performed a meta-analysis to clarify the correlation between ACE gene polymorphism (insertion/deletion (I/D)) and the risk of PIH.
Materials and methods
Document retrieval
We systematically searched China National Knowledge Infrastructure, Wanfang database, Chongqing WeiPu database and PubMed up to July 2014. We utilized ‘angiotensin-converting enzyme’ or ‘ACE’ and ‘pregnancy-induced hypertension’ or ‘PIH’ and ‘gene polymorphism’ or ‘genetics’ or ‘mutation’ as the search terms to retrieve related documents.
Inclusion criteria
All the included studies had to meet the following criteria: the published literature reported studies of the correlation between the incidence of PIH and ACE gene polymorphism; research methods constituted a case–control study; studies can directly or indirectly provide the frequency distribution of the ACE genotype in cases and controls; genetic polymorphism distribution of controls was in line with Hardy–Weinberg equilibrium; no language or race limitations.
Exclusion criteria
Duplicated literature and literature that did not provide valid data and for which the full text could not be obtained were excluded.
Quality assessment of literature
Referring to the Newcastle–Ottawa Scale, 10 qualities of all the included literature were assessed as to the object selectivity, comparability and exposure; each appropriate entry was described as a star, and each star represented 1 point; object selection accounted for 4 points; comparability accounted for 2 points and exposure accounted for 3 points.
Data extraction
Screening and data extraction of the included literature were conducted by two reviewers (HWM and HG); any inconsistency was resolved by discussion. Data extraction included the following terms: last name of the first author, publication year, country or region, sample size of cases and controls and numbers of each genotype in case and control subjects.
Statistical analysis
RevMan 5.0 software was used for statistical analysis; heterogeneity was detected using the Q test; when I2 was less than 50%, a fixed-effect model was use for meta-analysis; when I2 was greater than 50%, a random-effect model was used for meta-analysis. The combined odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using RevMan software, with a forest plot showing the characteristics of the various findings. In each study, the standard errors of the OR natural logarithm were taken as abscissa and the OR natural logarithm were used for the vertical axis to draw Begg’s funnel plot to examine publication bias. P<0.05 was considered statistically significant.
Results
The characteristics of included studies
As shown in Figure 1, a total of 244 documents was obtained after the initial search; excluding duplicate research and unrelated studies, 45 studies were eventually included the present study.11–54 The enrolled 45 case–control studies on the ACE gene I/D polymorphism and PIH included 10,236 subjects. Quality assessment showed that the 45 studies had large sample sizes, clear diagnostic criteria and comparability between the case group and the control group; all studies used polymerase chain reaction for genotype testing; the obtained data were clear; and the genetic equilibrium test showed that the gene distribution of the control group was consistent with Hardy–Weinberg equilibrium. The basic characteristics of each included study are shown in Table 1.

Flow chart of literature identification.
The characteristics of included studies.

ACE: angiotensin-converting enzyme; HWE: Hardy–Weinberg equilibrium; PCR: polymerase chain reaction.
The methodological quality of the included studies
In the 45 studies, there were 42 documents with more than 6 points, another three single-centre small sample studies were of lower quality; all the designs of experiments were group-matching; most case definition and criteria were clear; the majority of the controls were from the hospital population.
Meta-analysis
In total, the heterogeneity test showed there was a significant heterogeneity among the various studies (I2=81%, P<0.001), therefore the random-effect model was used to merge the ORs. Meta-analysis showed there was a significant association between ACE I/D polymorphism and PIH in the dominant model (OR 1.86, 95% CI 1.48–2.32, P<0.0001; Figure 2), recessive model (OR 0.65, 95% CI 0.53–0.80, P<0.0001; Figure 3) and allele model (OR 1.57, 95% CI 1.33–1.86, P<0.0001; Figure 4).

Forest plot of PIH risk associated with ACE I/D polymorphism in total population (DD genotype vs DI + II genotype). The squares and horizontal lines correspond to the study-specific ORs and 95% CIs, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of ORs and 95% CIs. ACE, angiotensin-converting enzyme; PIH, pregnancy-induced hypertension.
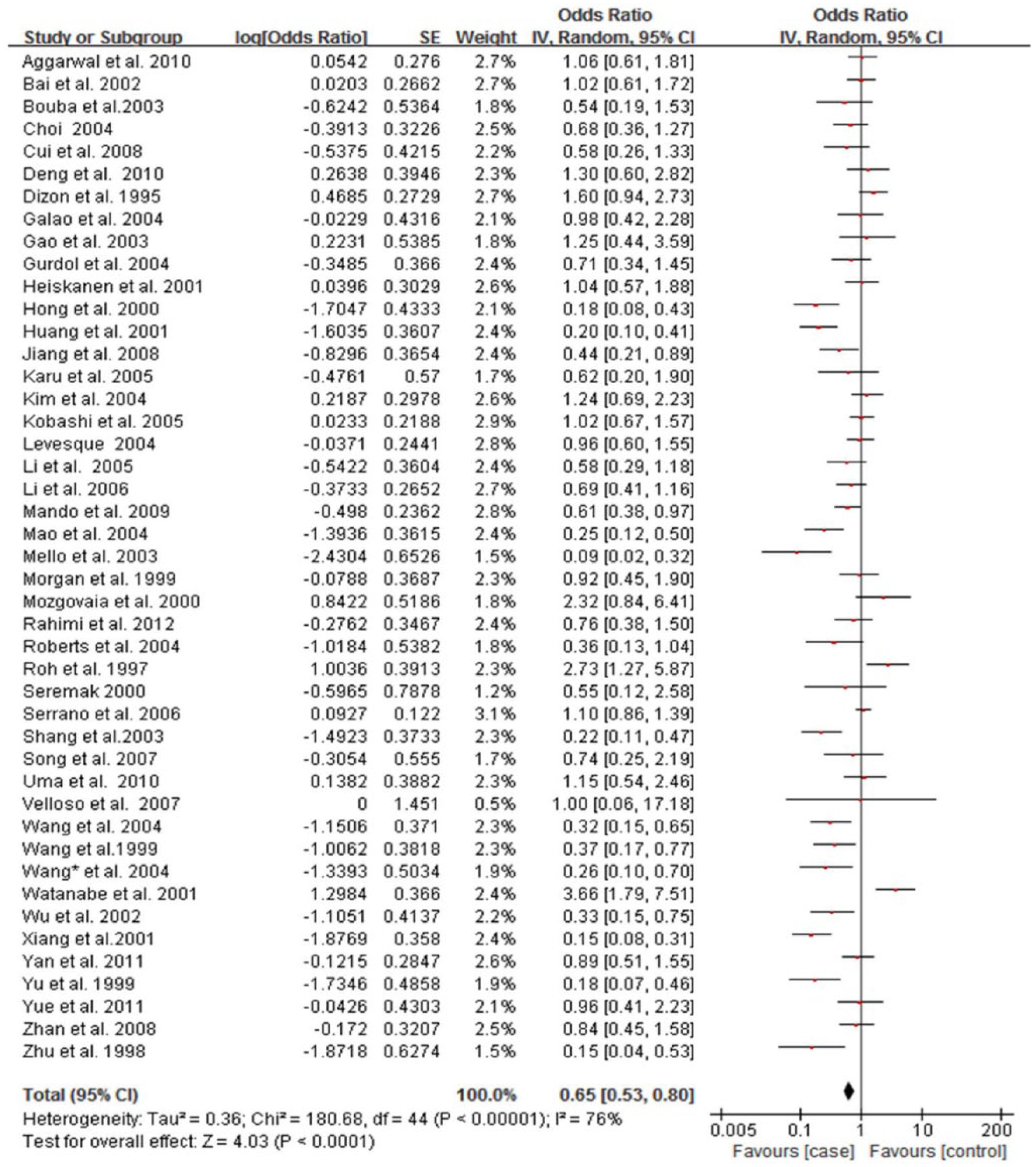
Forest plot of PIH risk associated with ACE I/D polymorphism in total population (II genotype vs DI + DD genotype). The squares and horizontal lines correspond to the study-specific ORs and 95% CIs, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of ORs and 95% CIs. ACE, angiotensin-converting enzyme; PIH, pregnancy-induced hypertension.

Forest plot of PIH risk associated with ACE I/D polymorphism in total population (D allele vs I allele). The squares and horizontal lines correspond to the study-specific ORs and 95% CIs, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of ORs and 95% CIs. ACE, angiotensin-converting enzyme; PIH, pregnancy-induced hypertension.
In the Asian population, we also found the association of ACE I/D polymorphism with PIH risk in these three models: D allele vs I allele: OR 1.80, 95% CI 1.36–2.38; genotype DD vs genotype II + DI: OR 2.25, 95% CI 1.53–3.30; genotype II vs genotype DI + DD: OR 0.56, 95% CI 0.41–0.76 (Figure 5).

Forest plot of PIH risk associated with ACE I/D polymorphism in Asian population (A) DD genotype vs DI + II genotype; (B) II genotype vs DI + DD genotype; (C) D allele vs I allele. The squares and horizontal lines correspond to the study-specific ORs and 95% CIs, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of ORs and 95% CIs. ACE, angiotensin-converting enzyme; PIH, pregnancy-induced hypertension.
However, in the Caucasian population, we only found the association of ACE I/D polymorphism with PIH risk in the dominant model and allele model (D vs. I: OR 1.24, 95% CI 1.08–1.44; DD vs II + DI: OR 1.25, 95% CI 1.10–1.41) but not in a recessive model (II vs DI + DD: OR 0.96, 95% CI 0.83–1.11) (Figure 6).

Forest plot of PIH risk associated with ACE I/D polymorphism in Caucasian population (A) DD genotype vs DI + II genotype; (B) II genotype vs DI + DD genotype; (C) D allele vs I allele. The squares and horizontal lines correspond to the study-specific ORs and 95% CIs, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of ORs and 95% CIs. ACE, angiotensin-converting enzyme; PIH, pregnancy-induced hypertension.
Sensitivity analysis and publication bias
Sensitivity analysis was performed by the exclusion method one by one. We did not find that the combined OR values change significantly, which indicated the meta-analysis was stable and reliable.
Seen from the funnel plot analysis (Figure 7), the symmetry of each genotype funnel plot was good, displaying no publication bias. Evaluation of the funnel plot symmetry with Begg’s test and Egger’s test showed that there was no significant publication bias in the various publications, and the selected studies were more representative.

Begg’s funnel plot for publication bias test. Each circle denotes an independent study for the indicated association. Log[OR], natural logarithm of OR. Horizontal line stands for mean effect size.
Discussion
In the present study, we found that the ACE genetic polymorphism (I/D) was associated with the risk of PIH. The human ACE gene is located on the long arm of chromosome 17, region 2, zone 3, which is a single copy gene. There is a 287 bp I/D polymorphism in intron 16, and it makes the human ACE gene produce three genotypes, DD, DI and II. At present, it has been found that the ACE gene can regulate the level of human serum ACE concentration. Human serum ACE is at the highest level of activity in DD genotype carriers, and the activity level of human serum ACE with DI genotypes was followed. Human serum ACE is at the lowest level of activity in subjects with the II genotype.55–58
To date, much research11–54 has been focused on the ACE gene I/D polymorphism and PIH, but the results are controversial. Aggarwal et al. 27 found that although the level of activity of human serum ACE with the DD genotype was higher than that with other genotypes in northern India, in the distribution of genetic frequency there is no difference between the case and control groups. Seremak-Mrozikiewicz et al. 25 found that the frequency distribution of the D and I alleles of the ACE gene were inconsistent in cases and control groups, and confirmed that the D allele may be a risk factor for PIH. Bai et al. 34 also found in the PIH group the frequency of the D allele was higher than that in the control group. The authors also found the serum concentration of ACE was higher in the PIH group than that in the control group. Kaur et al. 11 found that the frequency of the DD genotype in the PIH group was 60%, while it was only 30% in the control group; the difference was significant. And the frequency of the D allele in patients with PIH (74%) was higher than that in the control group (56%). However, they did not find a significant difference in the concentration of serum ACE between the two groups.
In the present study, the meta-analysis showed that the ACE gene I/D polymorphism was associated with the risk of PIH. Both the D allele and DD genotype are risk factors for PIH, while the II genotype may be a protective factor. The present study included 45 studies, involving 10,236 subjects. In these studies, there were three ethnicities including Asian, Caucasian and South African populations. Only one study reported the data for South African individuals, but we did not analyse this study independently. Therefore, in stratification analysis, we divided the studies into Asian and Caucasian populations. We found a similar association, that the D allele carriers have a higher risk of PIH than those with the I allele of the ACE polymorphism with PIH in these two ethnic population. Although we clarified the relation between the ACE polymorphism and PIH, the heterogeneity between each study must be explained. The presence of heterogeneity among the included studies may be associated with the following factors:
The occurrence of PIH may not only be associated with genetic factors but may also be related to environmental factors. In the analysis of included studies, the authors only compared the difference of genotypes between case and control groups, and did not analyse the influence of other risk factors.
Some studies did not consider ethnic and other confounders in the selection of cases, which may also have some impact on the results.
Lack of access to the ethnic, age, occupation and lifestyle of subjects from the included studies, subgroup analysis cannot be further conducted to exclude heterogeneity.
Some of the included publications in the present study had no confirmatory test and there could be genotyping errors, which would impact our results to some extent.
In conclusion, this analysis showed that the subjects with the D allele have a higher risk of having PIH. However, PIH is a complex disease resulting from the interaction between many factors. Our results require verification in a larger sample and more rigorous case–control study or cohort study in the future.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.