
Abstract
Background and objective:
The association between angiotensin-converting enzyme insertion/deletion (ACE I/D) gene polymorphism and the risk of overweight/obesity remains controversial. A meta-analysis was conducted to evaluate the association between ACE I/D gene polymorphism and overweight/obesity susceptibility.
Method:
All eligible studies were included in this meta-analysis by searching PubMed, Embase and Cochrane databases through April 2013 according to a predefined criteria.
Results:
Fourteen case-control studies including 3371 cases and 4490 controls were recruited for the analysis of the association between ACE I/D gene polymorphism and overweight/obesity susceptibility. A significant association was observed between DD genotype and overweight/obesity risk in overall populations and Africans (p=0.014 and 0.010, respectively). D allele was associated with the risk of overweight/ obesity in Africans (p=0.026). However, II genotype might not be a protective factor against overweight/obesity risk in overall populations, Africans, Caucasians and Asians.
Conclusions:
DD genotype is a risk factor for the overweight/obesity susceptibility in overall populations, particularly in Africans. D allele is a risk factor for the overweight/obesity susceptibility in Africans. Further larger studies are needed to confirm our findings.
Introduction
Obesity – an excessive accumulation of body fat – is the most prevalent, chronic medical condition across the world. 1 It poses a great threat to renal health and is an independent risk factor for cardiovascular diseases, 2 as well as influencing the functions of the endocrine system. 3 Moreover, central obesity is particularly associated with an increase of general mortality. 4 It is well documented that obesity is a multifactorial disorder involving the interaction of genetic and environmental factors. 5 To date, a few putative major genes for human obesity have been identified, it is speculated that a number of minor genes involved in the process of adipogenesis or in the regulation of adipocyte metabolism may also result in susceptibility to obesity. 6
Angiotensin-converting enzyme (ACE) is involved in adipocyte growth and function and the ACE-processed angiotensin II inhibits adipocyte differentiation. 7 A polymorphism has been identified in intron 16 in which a 287 base-pair alu sequence was found to be present (insertion or I) or absent (deletion or D) in the population. 8
A meta-analysis by Xi et al. 9 showed that ACE I/D gene polymorphism was closely associated with susceptibility to metabolic syndrome, a disorder closely associated with central obesity. In addition, an association of body mass index (BMI) with ACE I/D gene polymorphism was obtained in a Tunisian population. 10 In this sense, it is reasonable to postulate that ACE I/D gene polymorphism may be associated with susceptibility to overweight/obesity. However, a number of investigations regarding the association between ACE I/D gene polymorphism and overweight/obesity risk have generated mixed results in human studies.5,8,10-21 The contribution of ACE I/D gene polymorphism to the onset of overweight/obesity is still unclear. Meta-analysis of the association between ACE I/D gene polymorphism and overweight/obesity risk is rare. Thus, we performed this meta-analysis to investigate the association between ACE I/D gene polymorphism and overweight /obesity susceptibility with the aim of providing a much more reliable finding on the significance of this issue.
Materials and methods
Search strategy
We searched the published literature through April 2013 for related studies that investigated the association between ACE I/D gene polymorphism and the risk of overweight/obesity using PubMed, Embase and Cochrane databases. The search in PubMed or Embase was limited to English language. The followings were search terms: (1) overweight, obesity, and central obesity; and (2) angiotensin-converting enzyme, insertion/deletion, ACE I/D, and gene polymorphism. We also reviewed the reference lists of retrieved articles and reviews. If multiple publications of the same subjects occurred, we recruited the study with the most complete analysis.
Inclusion and exclusion criteria
Inclusion criteria: (1) case-control study; (2) the outcome of interest was overweight/obesity; (3) at least two comparison groups (overweight/obesity group vs. control group). Exclusion criteria: (1) case reports, editorials and reviews; (2) relationship between other genes and overweight/obesity risk; (3) multiple publications of the same data; and (4) study of the role of ACE I/D in diseases.
Data extraction and synthesis
Characteristics for each study were extracted and data were recorded as follows: first author’s surname, year of publication, ethnicity of study population, number of cases and controls for ACE I/D genotype. Frequencies of D allele were computed for case and control groups from the corresponding genotype distribution. Two authors independently conducted the data extraction and synthesis, with any disagreements resolved by discussion.
Statistical analysis
Odds ratio (OR) was used as a measure of the association between ACE I/D gene polymorphism and overweight/obesity risk across studies. Heterogeneity of ORs among studies was tested by using the Q statistic (significance level at p<0.05). The I2 statistic, a quantitative measure of inconsistency across studies, was also calculated. The pooled ORs were computed using either fixed-effects model or, in the presence of heterogeneity, random-effects model. Moreover, 95% confidence intervals (CIs) were also computed. In order to avoid excessive comparisons, the OR was calculated using three methods: method 1, allele comparison (D allele vs. I allele); method 2, comparing DD homozygous with the other two combinations (DD vs. DI+II); and method 3, comparing II genotype with the other two combinations (II vs. DI+DD). A chi-square test using a web-based program was used to determine whether genotype distribution of the control population reported conformed to Hardy–Weinberg equilibrium (HWE) (HWE significance level at p<0.05). A sensitivity analysis was conducted when studies with controls did not conform to HWE, or HWE was not available due to the lack of data. Potential publication bias was assessed by Begg’s test and Egger’s test (p<0.05 was considered significant) when the number of the studies included was more than 10. All analyses were conducted using STATA version 12.0 (Stata Corp, College Station, TX); p<0.05 was considered statistically significant, except where otherwise specified.
Results
Study characteristics
We initially extracted 526 unique references from the PubMed (424), Embase (76) and Cochrane databases (26). Of these, 512 publications were excluded according to the inclusion and exclusion criteria. Fourteen articles were included in our analysis for the association between ACE I/D gene polymorphism and overweight/obesity risk (Figure 1). Seven5,8,12,14,15,17,19 studies were conducted in Asians, five11,13,16,20,21 in Caucasians, and two10,18 in Africans (one in Continental Africans 10 and one in Afro-Caribbeans 18 ). All papers were published in English. The extracted data were recorded as follows: first author’s surname, publication year and the number of cases and controls (Table 1). These 14 studies included 3371 cases and 4490 controls. The average frequency of the D allele was 57.38% in Caucasian patients and 55.38% in controls. For Asians, the average frequency of the D allele was 58.99% in the case group and 46.82% for controls. For Africans, the average frequency of the D allele was 64.84% in the case group and 57.68% for controls. The ratio of cases/controls for average frequency of the D allele in Asians was higher compared with that in Africans and Caucasians (Asians: cases/ controls=1.26; Africans: cases/ controls=1.12; Caucasians: cases/ controls=1.04).

Flow diagram of study selection.
Characteristics of studies assessing the effects of ACE I/D polymorphism on overweight/obesity risk.

ACE: angiotensin-converting enzyme; I/D: insertion/deletion; HWE: Hardy-Weinberg equilibrium.
Association of ACE I/D gene polymorphism with overweight/obesity risk
In this meta-analysis, a significant association between DD genotype and overweight /obesity risk was observed in overall populations (p=0.014; Figure 2; Table 2), whereas D allele was not associated with the risk of overweight/obesity (p=0.132; Table 2). In the subgroup analysis, DD genotype/D allele was associated with susceptibility to overweight/obesity in Africans (DD genotype: p=0.01, D allele=0.026; Figures 3 and 4; Table 2). Moreover, DD genotype/D allele was not associated with the risk of overweight/obesity in Caucasians and Asians (Table 2). II genotype might not be a protective factor against overweight/obesity risk in overall populations, Africans, Caucasians and Asians (Table 2).

Association between DD genotype and overweight/obesity risk in overall populations. CI: confidence interval; OR: odds ratio.
Meta-analysis of the association of ACE I/D polymorphism with overweight/obesity risk.

ACE: angiotensin-converting enzyme; I/D: insertion/deletion; OR: odds ratio: CI: confidence interval.

Association between DD genotype and overweight/obesity risk in Africans. CI: confidence interval; OR: odds ratio.
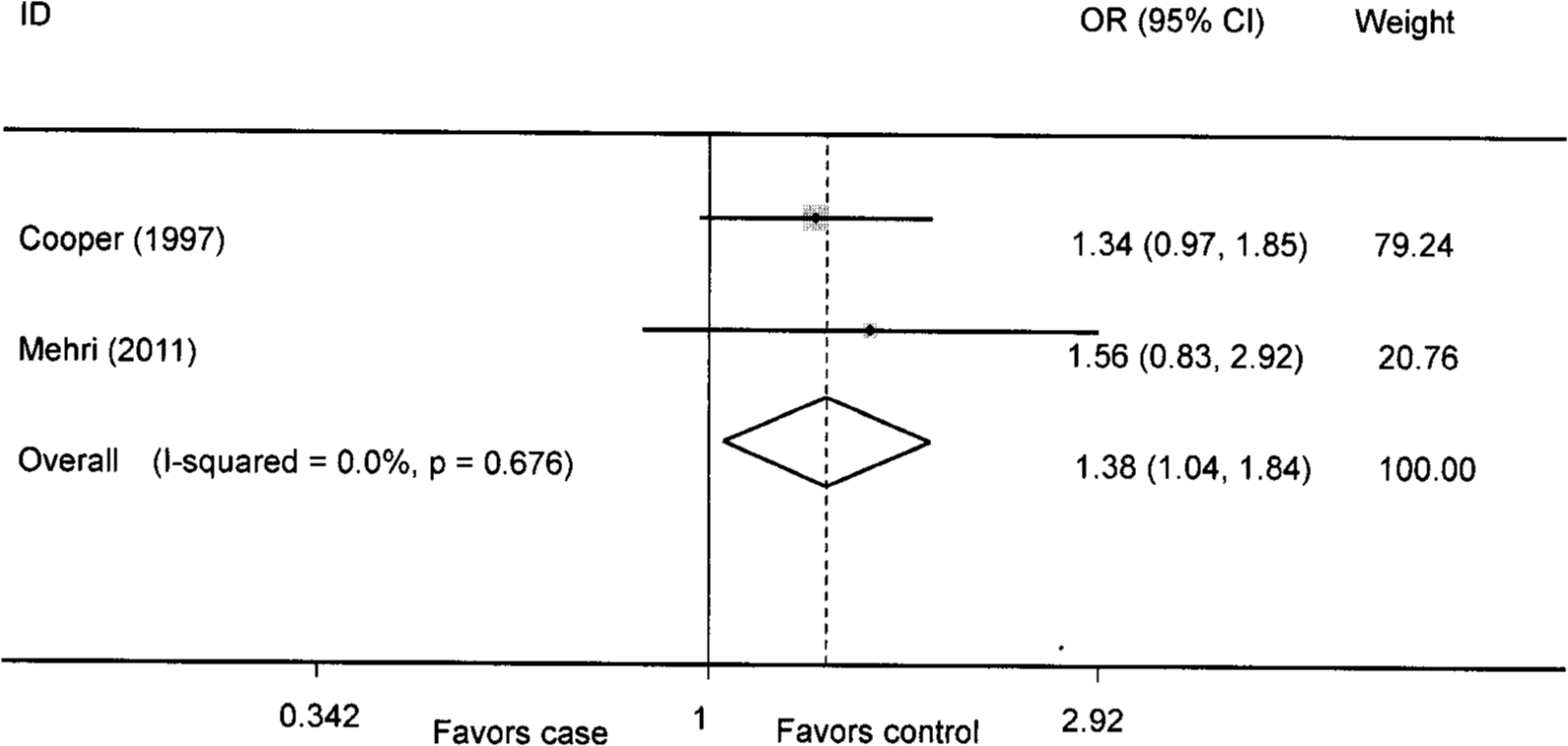
Association between D allele and overweight/obesity risk in Africans. CI: confidence interval; OR: odds ratio.
Sensitivity analysis
Two studies5,16 in which detailed numbers of DD, DI or II genotypes in the control groups were not available were excluded; the genotype distributions of the control groups in the remaining studies were all in HWE. Therefore, we included 12 studies8,10-15,17-21 in the sensitivity analysis.
For overall populations, similar results were found in the sensitivity analysis compared with those in the non-sensitivity analysis. DD genotype was significantly associated with overweight/obesity risk in overall populations. For Africans, the results from sensitivity analysis were similar to those from the non-sensitivity analysis. Significant associations were observed between DD genotype/D allele and the risk of overweight/obesity in Africans. Moreover, for Caucasians and Asians, the results from sensitivity analysis were similar to those from the non-sensitivity analysis. II genotype might not play a protective role against overweight/obesity risk in overall populations, Africans, Caucasians and Asians, which were similar to those from the non-sensitivity analysis (Table 2).
Evaluation of publication bias
There was no significant publication bias for overall populations (D vs. I: Begg p=0.360, Egger p=0.182; DD vs. DI+II: Begg p=0.855, Egger p=0.535; II vs. DI+DD: Begg p=1.000, Egger p=0.724).
Discussion
To our knowledge, this is the first meta-analysis to assess the association between ACE I/D gene polymorphism and overweight/obesity risk. We observed that the DD genotype was associated with the development of overweight/obesity in overall populations, and the results from the sensitivity analysis were similar to those from the non-sensitivity analysis. No publication bias for overall populations was observed. All these indicated the results for overall populations were robust.
Ethnic differences might affect the association between ACE I/D gene polymorphism and overweight/obesity risk. In our study, the ratio of cases/controls for average frequency of the D allele was 1.26, 1.12 and 1.04 in Asians, Africans and Caucasians, respectively. Of note, the ratio in Asians was the highest, whereas no significant association between D allele/DD genotype and overweight/obesity risk was observed in Asians. This was mainly because of the study by Yang et al., 5 in which the HWE was not available; the ratio would be 1.00 if this study was excluded. In Africans, we found that the D allele and DD genotype were associated with susceptibility to overweight/obesity, and the results from the sensitivity analysis were similar to those from the non-sensitivity analysis. However, there were only two studies included for the meta-analysis in Africans, which made it difficult to draw a robust conclusion for Africans. More studies in Africans are needed for a robust result. We also found that II genotype seemed not to play a protective role against the risk of overweight/ obesity in overall populations, Africans, Caucasians and Asians.
Several factors may account for our findings regarding the association between ACE I/D gene polymorphism and overweight/obesity risk. First, the renin–angiotensin system (RAS) has been hypothesized to inhibit adipogenesis, 22 which limits the storage capacity of adipose tissues and allows ectopic lipid storage that results in lipotoxicity. ACE is expressed in adipose tissue, which indicates that ACE may be involved in adipocyte growth and metabolism resulting in the regulation of obesity-related traits. 23 Angiotensin II, the major effector of RAS, inhibits adipocyte differentiation and promotes myocytic lipid deposition. 24 Moreover, angiotensin receptor blockers activate peroxisome proliferator-activated receptor (PPAR)-gamma activity and adiponectin secretion. 25 Second, ACE I/D gene polymorphism may be a major determinant of serum ACE levels. 26 Serum ACE levels are markedly higher in the DD genotype than those in the DI or in II genotype; the number of the D allele corresponds to increasing concentrations of serum ACE, 27 consistent with our results that the DD genotype was associated with overweight/obesity risk in overall populations and Africans, and the D allele was associated with the susceptibility to overweight/obesity in Africans. Third, as many genes and polymorphisms contribute to RAS activity, the interaction between ACE I/D gene polymorphism and other functional sequence variants might affect the results. 28 Finally, comorbidities, gender, and ethnic background may affect the results. For example, one study by Settin et al. 8 showed that there was no marked association between ACE I/D gene polymorphism and non-complicated overweight/obesity risk, and two studies5,20 demonstrated that the association between ACE I/D gene polymorphism and overweight/obesity risk was gender dependent. All these prove at least the existence of other factors affecting the role of ACE I/D gene polymorphism in the onset of overweight/obesity, which offers an insight into investigating the association between ACE I/D gene polymorphism and overweight/obesity risk in different populations.
There have been a number of meta-analyses and studies reporting the association between ACE I/D gene polymorphism and the risk of obesity-related diseases. A meta-analysis by Xi et al. 9 reported that the D allele was associated with the risk of metabolic syndrome. A meta-analysis by Li 29 showed that the D allele was linked with essential hypertension in the whole Chinese population. A meta-analysis by Niu et al. 30 showed that the D allele was associated with susceptibility to type 2 diabetes. One study by Celik et al. 31 showed that the DD genotype was associated with an increased insulin resistance in women with polycystic ovary syndrome. A study by You et al. 32 showed that the D allele was closely associated with reduced high-density lipoprotein cholesterol levels. A study by Passaro et al. 33 showed that a gene interaction existed between PPAR-γ2 and ACE I/D polymorphism on BMI and fat mass. These previous findings strongly suggest that ACE I/D gene polymorphism is associated with the risk of disorders related to overweight/obesity.
In our meta-analysis, we found that DD genotype was associated with the risk of overweight/obesity in overall populations and Africans. The D allele was correlated with overweight/obesity risk in Africans. However, these findings should be interpreted with caution; first, heterogeneities across studies included might affect the results of our meta-analysis, although a random-effects model had been conducted. Second, the variable study designs and small sample size limited the statistical power. Third, although the definition of overweight/obesity in the majority of included studies is >25kg/m2, some studies13,15,16 also used waist circumference and serum levels of triglyceride, cholesterol or low-density lipoprotein as standards of overweight/obesity. The relationship between these factors and genotype and phenotype merits attention. For example, Passaro et al. 33 reported that ACE DD subjects had a higher BMI and fat mass. Min et al. 34 reported that ACE II genotype was associated with a higher blood pressure. Kotaska et al. 35 reported that the ACE D allele was the most frequent genetic variant in risk groups of dyslipidemic patients. Borzyszkowska et al. 36 reported that ACE DD genotype carriers had higher total cholesterol, low-density lipoprotein cholesterol and lower high-density lipoprotein cholesterol levels. Meta-regression analysis was unavailable due to the limited data. More association studies should be performed in the future. Finally, the interaction between ACE I/D gene polymorphism and other loci involved in the development of overweight/obesity might be present.
In conclusion, DD genotype is a risk factor for susceptibility to overweight/ obesity in overall populations and Africans. The D allele is a risk factor for susceptibility to overweight/obesity in Africans. The II genotype might not be a protective factor against the overweight/obesity risk in overall populations, Africans, Caucasians and Asians. However, more case-control studies are needed to elucidate the role of ACE I/D gene polymorphism in overweight/obesity risk in different populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.