
Abstract
Introduction:
The safety and actions of mineralocorticoid receptor antagonists on surrogate markers of cardiovascular disease as well as major patient level cardiovascular end-points in patients with chronic kidney disease are unclear.
Methods:
MEDLINE, EMBASE, Trip Database, Cochrane Central Register of Controlled Trials, Cochrane Renal Group specialized register, Current Controlled Trials and clinicaltrials.gov were searched for relevant trials.
Results:
Twenty-nine trials (1581 patients) were included. Overall, mineralocorticoid receptor antagonists lowered both systolic and diastolic blood pressure (–5.24, 95% confidence interval (CI) –8.65, −1.82 mmHg; p=0.003 and −1.96, 95% CI −3.22, –0.69 mmHg; p=0.002 respectively). There were insufficient data to perform a meta-analysis of other cardiovascular effects. However, a systematic review of the studies included suggested a consistent improvement in surrogate markers of cardiovascular disease. Overall, the use of mineralocorticoid receptor antagonists was associated with an increased serum potassium (0.23, 95% CI 0.13, 0.33 mmol/l; p<0.0001) and higher risk ratio (1.76, 95% CI 1.20, 2.57; p=0.001) of hyperkalemia. Data on long-term cardiovascular outcomes and mortality were not available in any of the trials.
Conclusions:
The long-term effects of mineralocorticoid receptor antagonists on cardiovascular events, mortality and safety need to be established.
Keywords
Introduction
Chronic kidney disease (CKD) is increasingly recognized as a cardiovascular risk factor with a graded inverse relationship between cardiovascular risk and glomerular filtration rate (GFR), which is accentuated by the presence of proteinuria. 1 The importance of the renin–angiotensin–aldosterone system (RAAS) in the progression of CKD and in the development of cardiovascular disease associated with this condition is widely recognized.2,3 The renal and cardiovascular benefits of inhibition of the RAAS have been demonstrated in multiple large trials of angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs), largely attributed to the prevention of the multiple adverse effects of angiotensin II. 4
Strong evidence suggests that ACEi and ARB drugs do not effectively inhibit aldosterone production in all patients and that aldosterone may also be a mediator of renal and cardiovascular damage in patients with CKD. 2 Mineralocorticoid receptors are present in the brain, heart and blood vessels as well as the kidney, and there is evidence of aldosterone production within these tissues. 5 Local mineralocorticoid receptor activation by aldosterone causes numerous pathological effects on the cardiovascular system including endothelial injury, inflammation, oxidative stress and fibrosis in the heart and vasculature, as well as the development of hypertension and autonomic dysfunction.5,6 This evidence has led to the suggestion that, potentially, some day all renal patients with be on a mineralocorticoid receptor antagonist (MRA) as a ‘renal aspirin’. 7
However, there is still a reluctance to use these agents in patients with CKD particularly because of the risk of further deterioration in renal function and the risk of dan-gerous hyperkalaemia. 4 Although the actions of MRA on proteinuria have been the subject of recent meta-analyses, the potential benefits of MRA on cardiovascular parameters and mortality in patients with CKD are not clear.8,9 We, therefore, analysed the actions of MRA on surro-gate markers of cardiovascular disease as well as major patient level cardiovascular end-points in patients with CKD.
Methods
This systematic review and meta-analysis was performed in accordance with the PRISMA statement. 10 The protocol and detailed methodology for this systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42013006795). 11 The following electronic databases and trial registers were searched from their conception to September 2013: MEDLINE, EMBASE, Trip Database, Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Renal Group specialized register, Current Controlled Trials and ClinicalTrials.gov. References of included articles and relevant review articles were hand-searched. Search terms including both MeSH and their derivatives: mineralocorticoid receptor antagonist, spironolactone, eplerenone, chronic kidney disease, and chronic renal failure. All searches were limited to human studies.
Type of studies
All fully published randomized-controlled trials (RCTs) examining the cardiovascular effects of both spironolactone and eplerenone in patients with CKD were included. Cohort studies, case series and case reports were excluded from the review owing to the high potential for bias in these study designs. Crossover studies were included provided there was evidence of a washout period and/or exclusion of a carry-over effect. All analyses were repeated excluding crossover studies. There was no language restriction.
Types of participants
Studies enrolling adult participants, with CKD stages 1–5 (as defined by the Kidney-Disease Outcomes and Quality Initiative (K-DOQI) guidelines, including dialysis patients and kidney transplant recipients) were included. 12
Types of interventions
We included studies of both unselective (spironolactone) and selective (eplerenone) MRA with or without concomitant use of ACEi and/or ARB given for at least four weeks.
Types of outcome measures
Data on the effects of MRA on the following outcome measures were examined: systolic and diastolic blood pressure (BP); parameters of arterial stiffness including pulse wave velocity (PWV); endothelial function and oxidative stress; carotid intima-media thickness (CIMT); left ventricular (LV) ejection function; LV mass; cardiovascular morbidity and mortality; hyperkalaemia (serum potassium> 5.5 mmol/l); decline in renal function and other adverse events including gynaecomastia.
Two reviewers (CJF, KPN) independently screened retrieved articles, discarded studies that did not meet the inclusion criteria, assessed the eligibility of the selected studies and extracted data using a standard collection form. 11 A third party settled any disagreements. In the case of multiple publications of the same trial, all outcomes and results were grouped together and single data extraction was performed on the most complete dataset.
Study quality
The risk of bias assessment tool developed by Cochrane Renal Group 13 was applied to each study. Two authors (CJF, KPN) independently assessed the quality of each included study on selection bias (sequence generation, allocation concealment), detection bias (personnel and participant, outcome assessors), attrition bias (incomplete outcome data), reporting bias (selective outcome reporting) and other potential biases. Disputes were settled by discussion with a third author.
Statistical assessment
Meta-analysis was conducted to generate pooled estimates of the outcomes using RevMan 5.2 software (©2012, The Cochrane Collaboration, UK). Data were pooled and a random effect model was used as summary effect measure. Relative risk ratio or weighted mean difference with accompanying 95% confidence intervals (CIs) were used to report individual and summary effect measures for dichotomous or continuous data respectively. Chi 2 tests for heterogeneity were performed to examine whether the degrees of freedom were greater than the Cochran Q statistic, with α of above 0.05 as statistical significance. In addition, we also calculated the I2 statistic to provide the estimated percentage of heterogeneity observed. I2 values of 25%, 50% and 75% correspond to low, medium and high levels of heterogeneity. Any heterogeneity was further explored. When appropriate, subgroups of different MRA (selective or non-selective), comparator (active or placebo/standard treatment) and concomitant ACEi and/or ARB were analysed. A two-sided p-value of <0.05 was considered significant for all analyses.
Results
Search results
A total of 2823 articles were identified, of which 66 articles met the general inclusion criteria. Full-text assessment of these articles identified 29 eligible studies (31 articles)14-44 (Table 1), enrolling a total of 1581 patients for qualitative synthesis and 28 eligible studies enrolling a total of 1548 patients for meta-analysis (Figure 1).
Characteristics of the populations and interventions in the included trials.

All values were expressed as mean ± standard deviation. Abbreviations: AII: angiotensin II; ACEi: angiotensin-converting enzyme inhibitor; AIx: augmentation index; ARB: angiotensin II receptor blocker; α1m: α1-microglobulin; b.d.: twice daily; BMI: body mass index; BNP: B-type natriuretic protein; BP: blood pressure; CAPD: patients on continuous ambulatory peritoneal dialysis; cfPWV: carotid-femoral pulse wave velocity; CKD: chronic kidney disease; CMR: cardiovascular magnetic resonance; Cr: serum creatinine; CrCl: creatinine clearance; DM: diabetes mellitus; EF: ejection fraction; eGFR: estimated glomerular filtration rate; GN: glomerulonephritis; HbA1c : haemoglobin A1c; HD: patients on haemodialysis; hsCRP: high sensitivity C-reactive protein; K+: potassium; KIM-1: kidney injury molecule 1; LFABP: liver-type fatty-acid binding protein; LV: left ventricular; LVMI: left ventricular mass index; MCP-1: monocyte chemoattractant protein 1; Na+: sodium; NAG : N-acetyl-β-D-glucosaminidase; NGAL: neutrophil gelatinase associated lipocalin; NT-proBNP: N-terminal-pro brain natriuretic peptide; NYHA: New York Heart Association; PAC: plasma aldosterone concentration PAI-1: plasminogen activator inhibitor-1; PIIINP: amino-terminal propeptide of type III procollagen; PRA: plasma renin activity; pt: participants; PWA: pulse wave analysis; RCT: randomized controlled trial; SBP: systolic blood pressure; sE-selectin: soluble E-selectin; s-ICMI: soluble-intercellular adhesion molecule; s-VCAMI: soluble vascular cell adhesion molecule I; TNF-α: tumour necrosis factor alpha; uACR: urine albumin:creatinine ratio; UAE: urine albumin excretion; VWF: von Willebrand factor
denotes exclusion criteria
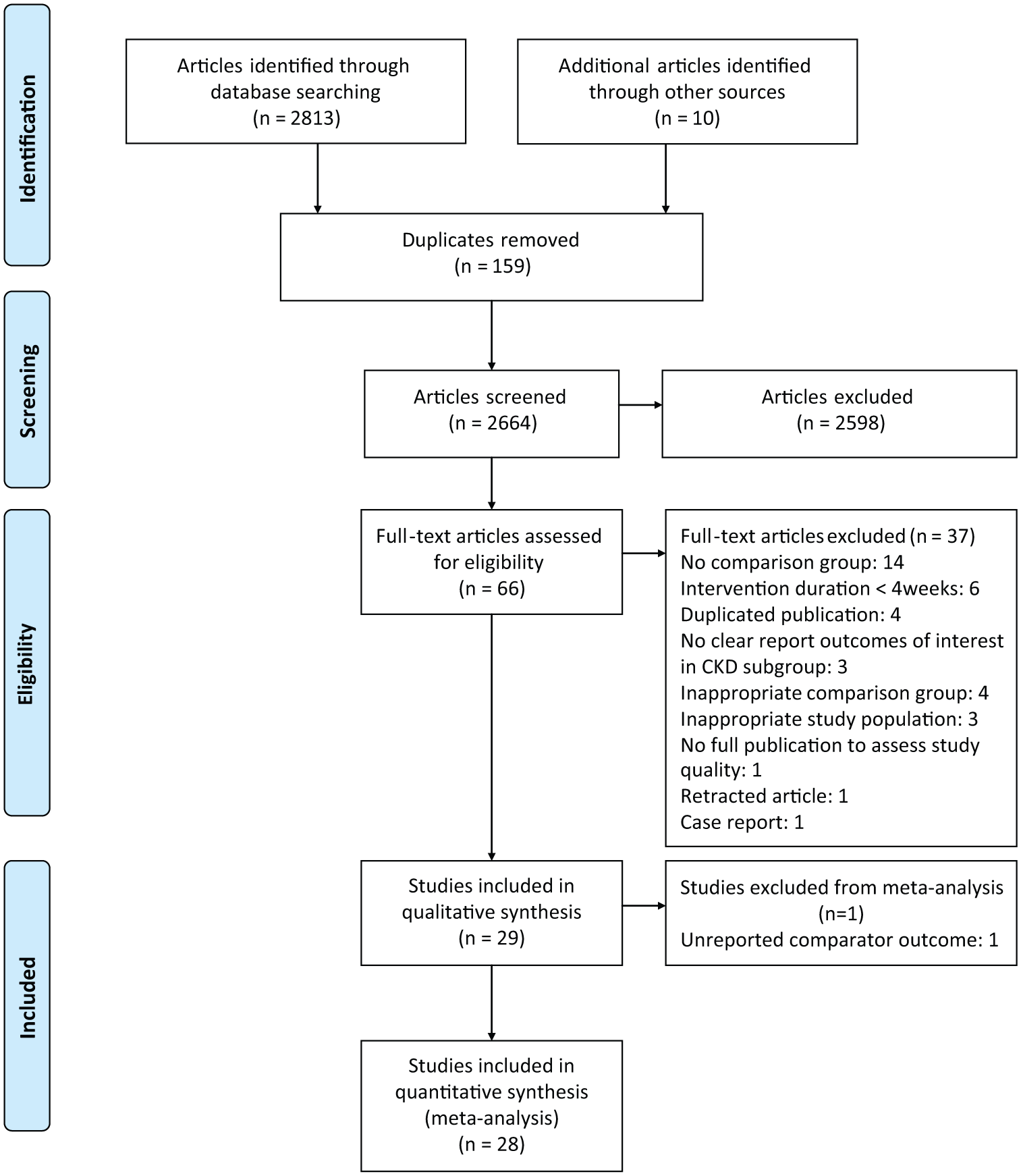
Study flow diagram.
Trial characteristics
The characteristics of included studies are detailed in Table 1. Ten studies were crossover studies. One study examined patients on peritoneal dialysis, 39 two studies examined patients on haemodialysis38,42 and the remaining studies examined patients with CKD. All but two14,16 of these studies excluded patients with advanced CKD (estimated GFR<30 ml/min per 1.73 m2) although it was not clear how many patients with this level of renal function were actually recruited. We did not identify any eligible study involving renal transplant recipients. Spironolactone was used in 23 studies and eplerenone in six. Active comparator arms involving the use of additional antihypertensive agents were noted in 13 studies with the rest involving MRA treatment being compared against placebo or standard care. Concomitant use of ACEi and/or ARB was reported in 24 studies. Study duration ranged from eight to 104 weeks and study population ranged from 12 to 268 participants. None of the studies were powered to detect hard primary outcomes. Proteinuria/albuminuria was the primary outcome in 17 of the studies with cardiovascular outcomes as secondary end-points.
Risks of bias in the included studies are shown in Table 2. Most of the studies did not report enough information for adequate assessment of risk on most of the parameters assessed.
Risk of bias summary.

Effects of interventions
End of treatment BP
Twenty-one studies reported data on BP suitable for analysis. Three protocols required the use of additional antihypertensive agents to be initiated during the study in order to achieve a BP <130/80 mmHg in both the intervention and control arms22,27,41 and were therefore excluded from the analyses leaving 18 RCTs with 1129 patients. Spironolactone was used in 16 studies and eplerenone in two.
Overall, there was a significant reduction of systolic BP with MRA (–5.24, 95% CI −8.65, −1.82 mmHg; p=0.003: Figure 2(a)) although there was high heterogeneity (Chi2=90.03, p<0.001, I2=80%). Exclusion of the only study examining the effects of MRA in patients with CKD and resistant hypertension 14 resulted in a small change in treatment effect (–3.56, 95% CI −5.30, −1.83 mmHg; p<0.001) but reduced the heterogeneity (Chi2=20.74, p=0.2, I2=18%). Exclusion of crossover studies made little difference (–3.56, 95% CI −5.85, −1.27 mmHg; p=0.002) with low–medium heterogeneity (Chi2=18.61, p=0.1, I2=36%). Overall, MRA lowered systolic BP (–3.31, 95% CI −4.78, −1.84 mmHg; p<0.001) versus placebo with low heterogeneity (Chi2=8.06, p=0.6, I2=0%) but not when compared with another anti-hypertensive agent (–3.77, 95% CI −8.25, 0.71 mmHg; p=0.1) although this analysis had moderate heterogeneity (Chi2=12.66, p=0.05, I2=53%).

Effect of mineralocorticoid receptor antagonists on (a) systolic blood pressure and (b) diastolic blood pressure.
Spironolactone reduced systolic BP (–3.56, 95% CI −5.61, −1.51 mmHg; p<0.001) with low heterogeneity (Chi2=20.29, p=0.2, I2=26%); it was more effective than placebo (–3.23, 95% CI −5.19, −1.28 mmHg; p=0.001; I2=6%) and active comparators (–3.64, 95% CI −6.36, –0.91 mmHg: p=0.009; I2=38%). Analysis of the two studies using eplerenone suggested a systolic BP lowering effect but this failed to achieve statistical significance (–3.77, 95% CI −7.83, 0.29 mmHg; p=0.07; I2=0%).
Similar results were noted with respect to diastolic BP (Figure 2(b)). Overall, there was a significant reduction of diastolic BP (–1.96, 95% CI −3.22, –0.69 mmHg; p=0.002) although there was moderate heterogeneity (Chi2=31.43, p=0.03, I2=43). Heterogeneity was significantly reduced (Chi2=15.02, p=0.6, I2=0%) by the exclusion of the only study on patients with resistant hypertension 14 with only a small change on the treatment effect (–1.42, 95% CI −2.29, –0.55 mmHg; p=0.001). Further exclusion of crossover studies made little difference (–1.37, 95% CI −2.44, –0.30 mmHg; p=0.01) with low heterogeneity (Chi2=13.04, p=0.4, I2=8%). Against placebo, MRA lowered diastolic BP (–1.62, 95% CI −2.73, –0.51 mmHg; p=0.004; Chi2=5.05, p=0.9, I2=0%) but not when compared with another anti-hypertensive agent (–0.84, 95% CI −3.07, 1.40 mmHg; p=0.4; Chi2=10.21, p=0.1, I2=41%).
Spironolactone reduced diastolic BP (–1.33, 95% CI −2.23, –0.43 mmHg; p=0.004; I2=0%); it was more effective than placebo (–1.39, 95% CI −2.53, –0.26 mmHg; p=0.02; Chi2=3.88, p=0.9, I2=0%) but not more effective than an active comparator (–0.58, 95% CI −3.00, 1.87 mmHg: p=0.5; Chi2=9.77, p=0.08, I2=41%). Analysis of the two studies using eplerenone suggested a non-significant diastolic BP lowering effect (–2.73, 95% CI −6.14, 0.68 mmHg; p=0.1: Chi2=0.31, p=0.6, I2=0%).
Arterial stiffness
Two studies examined aortic PWV as the primary outcome.17,19 In a randomized, open-label study of 46 patients with CKD stage 3–4, 24 weeks of treatment with eplerenone did not significantly reduce PWV nor BP. 17 In a larger, double-blinded, placebo-controlled RCT of 112 patients with CKD stages 2–3, treatment with spironolactone for 40 weeks significantly reduced PWV (–0.8 ± 1.0 vs. –0.1 ± 0.9 m/s, p<0.01) and increased aortic distensibility with a significant reduction in blood pressure. 19
Endothelial function/oxidative stress
Two studies examined the actions of MRA on endothelial function with neither study showing a significant effect.27,34 Takebayashi et al. 40 demonstrated a significant reduction in 8-iso-prostaglandin F2α, a marker of oxidative stress, with spironolactone while no significant change occurred with amlodipine 2.5 mg daily after 12 weeks of treatment.
CIMT
Only one study examined the actions of MRA on CIMT. Spironolactone thrice weekly post-dialysis was shown to significantly reduce the progression of CIMT after two years as compared with placebo. 42
LV ejection function and mass
Among patients on haemodialysis or peritoneal dialysis with a clinical diagnosis of heart failure (New York Heart Association III–IV and ejection fraction <45%), spironolactone thrice weekly in addition to ACEi or ARB was shown to significantly improve LV ejection fraction after 24 weeks as compared with placebo.38,39 Whilst there was no detectable difference in LV ejection fraction between those receiving spironolactone and placebo in a RCT of 112 patients with CKD stage 2–3 without a clinical diagnosis of heart failure and with normal left ventricular function, Edwards et al demonstrated significant improvements in other indices of systolic and diastolic function including LV long-axis systolic function, torsion, myocardial deformation and markers of LV relaxation and suction in the spironolactone group. 20 In patients with diabetic nephropathy, myocardial perfusion reserve improved after six weeks of eplerenone while there was no change in the control group treated with hydrochlorothiazide. 27 Three RCTs examined the effect of MRA on brain natriuretic peptide with all studies reporting significant reductions.20,29,34 Two placebo-controlled studies examining the actions of MRA on LV mass reported a reduction with the use of spironolactone after 40 weeks (–14 ± 3 g; p<0.01) 19 and after six months (–8 ± 4 g; p=0.02). 38
End of study serum potassium and hyperkalemia events (K+> 5.5 mmol/l)
Twenty-one studies (1015 patients) reported end of study potassium. Overall, the use of MRA was associated with an increase in serum potassium (0.23, 95% CI 0.13, 0.33 mmol/l; p<0.001) but with high heterogeneity (Chi2=90.29%, p<0.001, I2=77%; Figure 3). Two studies used additional potassium supplementation or potassium binders.24,27 Exclusion of these two studies made little difference to the result (0.24, 95% CI 0.12, 0.36 mmol/l; p<0.001) with persistent high heterogeneity (Chi2=87.80, p<0.001, I2=78%). Exclusion of crossover studies did not materially affect the result (0.25, 95% CI 0.11, 0.40 p<0.001: Chi2=67.48, p<0.001, I2=82%). Excluding three studies in which MRA was not co-administered with an ACEi and/or ARB did not significantly affect the result (0.22, 95% CI 0.11, 0.34 mmol/l; p<0.001: Chi2=80.48, I2=78%). Excluding the single study on dialysis patients made minimal difference to the result (0.24, 95% CI 0.14, 0.34 mmol/l; p<0.001: Chi2=86.73, p<0.001, I2=77%). Spironolactone (0.26, 95% CI 0.14, 0.37 mmol/l; p<0.001) but not eplerenone (0.14, 95% CI −0.08, 0.36 mmol/l; p=0.2) increased end of study serum potassium although both analyses had high heterogeneity (Chi2=69.45, p<0.001, I2=77%; Chi2=18.21, p=0.001, I2=78% respectively).

Effect of mineralocorticoid receptor antagonists on serum potassium.
Twenty-six studies (1619 patients) reported episodes of hyperkalemia. Overall, use of MRA was associated with a higher risk ratio (RR) (1.76, 95% CI 1.20, 2.57; p=0.004) of hyperkalemia with low heterogeneity (Chi2=13.73, p=0.8, I2=0%). Neither the exclusion of crossover studies (RR 1.77, 95% CI 1.19, 2.64, p=0.005; Chi2=10.89, p=0.7, I2=0%) nor exclusion of studies without concomitant ACEi and/or ARB (RR 1.76, 95% CI 1.18, 2.60; p=0.005: Chi2=13.62, p=0.8, I2=0%) materially affected the result. Excluding the single study on dialysis patients made very little difference to the results (RR 1.80, 95% CI 1.23, 2.65, p=0.003: Chi2=12.65, p=0.9, I2=0%). Both spironolactone (risk ratio 1.97, 95% CI 1.29, 3.00; p=0.002: Chi2=10.82; p=0.8, I2=0%) and eplerenone (risk ratio 1.97, 95% CI 1.29, 3.00; p=0.002: Chi2=2.70, p=0.4, I2=0%) were associated with increased risk of hyperkalemic events.
End of treatment serum creatinine and GFR
Seventeen studies (827 patients) reported change in serum creatinine. Overall, there was no significant change in serum creatinine (0.04, 95% CI −0.03, 0.11 mg/dl; p=0.3) with low heterogeneity (Chi2=22.77, p=0.2, I2=22%; Figure 4(a)). Exclusion of seven crossover studies made no appreciable difference to the result (0.02, 95% CI −0.09, 0.13 mg/dl; p=0.7), although there was moderate heterogeneity (Chi2=20.82, p=0.7, I2=52%). Fourteen studies used spironolactone (665 patients) and three (162 patients) used eplerenone with neither agent affecting serum creatinine (0.04, 95% CI −0.04, 0.12 mg/dl; p=0.1 and 0.04, 95% CI −0.15, 0.23 mg/dl; p=0.7, respectively). Only two studies did not allow concomitant use of an ACEi and/or ARB. Excluding these two studies did not alter the result (0.02, 95% CI −0.05, 0.09, p=0.6).

Effect of mineralocorticoid receptor antagonists on (a) serum creatinine and (b) glomerular filtration rate.
Twenty-one studies (1217 patients) reported changes in GFR. Overall, there was no significant change in the pooled estimate (0.03, 95% CI −0.08, 0.14 ml/min per 1.73 m2) with low heterogeneity (Chi2=15.05, p=0.8, I2=0%; Figure 4(b)). As for serum creatinine, sub-analyses, excluding crossover studies and studies not allowing concomitant use of ACE and/or ARB, as well as separate analyses for spironolactone or eplerenone, did not significantly affect the result.
Data for doubling of serum creatinine and incidence of end-stage kidney disease was not extractable in a format required for analysis or not reported in the included studies.
Cardiovascular morbidity and mortality outcomes
Mortality outcome was reported in three studies, all of which included patients on dialysis only.38,39,42 The study durations ranged from six months to two years and included 100 patients. There were six deaths in the placebo arm and three in the MRA arm.
Short-term cardiovascular morbidity data was available in two RCTs.30,38 In a RCT of 81 patients with diabetes, the hospitalization rates for cardiovascular events were not different for spironolactone, losartan or placebo. 30 In contrast, in a RCT study of 16 haemodialysis patients with heart failure, there was a significantly higher number of cardiovascular-related hospitalization events due to ischaemic heart disease and decompensated congestive heart failure in the placebo than in the spironolactone arm (12 vs. 2 events, p>0.01). 38
Other adverse events
Very few studies reported adverse events with any consistency. In all of the studies included, only nine reported breast tenderness/gynaecomastia with a further two reporting them as a cause for study withdrawal. In total, only 10 cases of gynaecomastia/breast tenderness were reported.
Discussion
Our study shows that MRA potentially improves multiple surrogate markers of cardiovascular disease although these studies were relatively few and most included a low number of patients. The majority of the endpoints studied are, to a greater or lesser extent, BP dependent and perhaps one of the more important findings from this analysis is that of a significant reduction in systolic and diastolic BP with MRA even when already treated with an ACEi and/or ARB. Indeed, control of hypertension is arguably the most important intervention for reducing the increased risk of cardiovascular disease and to slow progression to later stages of CKD. Two other important endpoints with prognostic significance, arterial stiffness and LV mass, are causatively influenced by BP. 6 Indeed a positive effect on arterial stiffness was only observed in association with BP reduction in one study, 19 a finding not replicated in another without any effect on BP. 17 Given that MRA use is associated with a significantly increased risk of hyperkalemia it remains to be seen whether the use of other, ‘safer’, antihypertensive agents, producing the same degree of BP reduction would achieve the same effects. No studies have been powered to examine the impact of MRA on cardiovascular morbidity and mortality or indeed any other patient-centred endpoints.
Inhibition of the RAAS with either ACEi or ARB in patients with CKD reduces the rate of deterioration of renal function and the increased cardiovascular risk associated with this condition. 2 While treatment with MRA might be thought to be of limited efficacy in patients on ACEi or ARB therapy, detailed study of patients on this treatment reveals that in many cases use of ACEi and ARB decreases levels of circulating aldosterone only for a period of weeks. In 10–50% of patients’ circulating aldosterone concentrations return to pre-treatment levels (a phenomenon termed ‘aldosterone breakthrough’). 45 There are reports that patients who demonstrate aldosterone breakthrough have a worse prognosis than those who do not. 45 It has been suggested that the use of MRA in this context would be beneficial, especially in the context of renal impairment, and there are many animal and human studies to support this. 2
A further important and not unexpected finding of this analysis was that there was a significant increase in serum potassium concentrations and a significant increase in the risk of hyperkalemia. In general, there were no data available to examine the influence of baseline renal function on any of these parameters (as has been previously described in robustly conducted meta-analyses examining the actions of MRA on proteinuria).8,9 On theoretical grounds, there is reason to believe that hyperkalemia might be more prevalent in patients with lower GFR values and it is important to note that the actions and safety of MRA in patients with GFR below 30 ml/min per 1.73 m2 have not been examined in significant numbers of patients. Also, other potential adverse effects of MRA such as gynaecomastia have been poorly reported and are likely to represent an underestimate of the true incidence. Reduction in proteinuria, a recognized association with cardiovascular risk, was the commonest endpoint of the studies examined and MRAs are effective at lowering proteinuria.8,9 However, studies of agents that reduce proteinuria have not always produced concomitant reductions in mortality. 46
Our study has a number of strengths and limitations. We followed current guidelines and identified a large number of studies. The major limitation is the lack of long-term studies on mortality and cardiovascular events. The majority of the studies included had enrolled few patients and were powered to observe differences in surrogate endpoints, mainly reduction in proteinuria. Most studies did not adequately report study methods to assess trial quality. Consistent with other reviews we were also unable to perform separate analyses based on baseline renal function, as data stratified by renal function were unavailable from all the studies.8,9 Furthermore, there are very few studies done on dialysis patients and it is possible that the benefits and risks of MRA on dialysis and non-dialysis patients could potentially be different.
Long-term studies analysing the effect of MRA on cardiovascular events and mortality are warranted. Studies should also examine whether the actions of MRA are independent of BP reduction ideally by using a control drug resulting in equal effects on BP. Furthermore, these studies should analyse the efficacy of MRA in patients who exhibit aldosterone breakthrough versus those who do not as the beneficial or adverse effects might be different between these two groups. Other factors that could potentially affect response, such as ethnicity, 47 level of kidney function, dialysis and transplant status, need examining.
Our increasing understanding of the myriad adverse effects of aldosterone in CKD patients justifies further study of the potential benefits and risks of MRA drugs in these patients. The current evidence does not support recommending treatment with MRA for patients with CKD to lower their cardiovascular risk. The next few years are likely to see exciting advances especially with the development of aldosterone synthase inhibitors 48 and more cardiac selective MRA. 49 For now, the concept of MRA being a ‘renal aspirin’ 7 will have to wait.
Footnotes
Acknowledgements
Primary Care Clinical Sciences is a member of the NIHR National School of Primary Care. The views expressed in this article are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Health Research (NIHR) (Post-Doctoral Fellowship to CJF).