
Abstract
Background:
Previous studies have investigated the association between a polymorphism (-455G>A) in the β-fibrinogen gene and the risk of cerebral infarction. However, these results are controversial. To shed light on these inconclusive findings, we performed a meta-analysis of studies relating the β-fibrinogen genetic polymorphism (-455G>A) to the risk of cerebral infarction.
Methods:
We identified literature published before July 2013 by searching PubMed, EMBASE, ISI Web of Science, the Chinese National Knowledge Infrastructure database (CNKI) and the Wanfang database in China and by reviewing the references of retrieved articles. We included studies that reported odds ratio (OR) with 95% confidence interval (CI) for the association between the β-fibrinogen genetic polymorphism and cerebral infarction risk. Publication bias was tested by a funnel plot, and the OR of all studies were combined dependent on the results of the heterogeneity tests among the individual studies. The software Review Manager (Version 5.2) was used for meta-analysis.
Results:
Twenty independent case-control studies containing 9477 subjects were included. Our results showed that the -455G>A polymorphism in the β-fibrinogen gene was associated with the increased risk of cerebral infarction [(AA+GA) vs. GG, OR=1.17, 95%CI: 1.04–1.31, p=0.008; A vs. G, OR=1.12, 95%CI: 1.01–1.23, p=0.03] in the Chinese population by a meta-analysis. However, we did not find this association in the Caucasian population [(AA+GA) vs. GG, OR=0.99, 95%CI: 0.87–1.11, p=0.84; A vs. G, OR=0.97, 95%CI: 0.84–1.13, p=0.73, respectively].
Conclusion:
The results of our meta-analysis indicate that the -455G>A polymorphism in the β-fibrinogen gene is a susceptibility marker of ischemic cerebral infarction in the Chinese population.
Introduction
Cerebral infarction (also called ischemic stroke), after ischemic heart disease, is the most common cause of mortality worldwide. 1 According to previous reports,2,3 ischemic cerebral infarction has caused approximately 5.7 million deaths in 2005. Ferri et al. 4 reported the prevalence of stroke and its related burden among older people living in Latin America, India and China in 2011. According to the report by Ferri et al., the prevalence of self-reported stroke ranged between 6% and 9% across most Latin American sites and urban China. Recently, Zheng et al. 5 reported that the prevalence of stroke in Xinjiang, in west China, ranged between 3.13% and 5.18%. China is the world’s most populous country; stroke is an enormous health care burden, representing the second leading cause of death and occurring in approximately 2 million people each year. 6 Stroke, including ischemic cerebral infarction, is considered to be the result of the interaction between genetics and environmental factors. Strong evidence from genetic association studies indicates that genetic predisposition, in addition to recognized risk factors, such as hypertension, smoking, diabetes, obesity and advanced age, contributes to the development of stroke. 7 In addition, individuals with a family history of stroke are more likely to suffer a stroke. Therefore, understanding these genetic influences may lead to better prevention and intervention of stroke.
Fibrinogen is composed of the α, β, and γ chains, which are encoded by three separate genes located in a 50-kb cluster on the long arm of chromosome 4. 8 The rate-limiting step in fibrinogen formation is the synthesis of the β-polypeptide chain regulated by a β-fibrinogen promoter. 9 One of the polymorphisms identified within this region is -455G>A, which is associated with -148C>T in the Caucasian population. 10 Several studies have shown that the -455G>A polymorphism is associated with increased plasma fibrinogen levels and increased risk of cerebral infarction.11–26 However, the relatively small sample size of this single study may not have been powerful enough to detect the slight effects of the -455G>A polymorphism on cerebral infarction; meta-analysis may provide more credible evidence by systematically summarizing existing data. In the present study, we have extensively reviewed the literature and performed a meta-analysis based on all eligible case-control studies to evaluate the association between -455G>A polymorphism in the β-fibrinogen gene and cerebral infarction susceptibility.
Materials and methods
Literature search and selection
We carried out a publication search in PubMed, EMBASE, ISI Web of Science, the Chinese National Knowledge Infrastructure (CNKI) database and the Wanfang database in China with the following search terms: (“fibrinogen” or “β-fibrinogen” or “beta-fibrinogen” or “FBG”), (“cerebral infarction” or “stroke” or “brain infarction” or “cerebrovascular disease” or “ischemic stroke”) and (“SNP” or “polymorphism” or “mutation” or “genetics”) using two independent investigators. Publication language was restricted to English and Chinese. Abstracts, reviews or editorials were not included. The references of all of the identified publications were searched for any additional studies, and the related articles option was used to search for further potentially relevant articles.
Selection criteria
Studies that were case-controlled by design, involved unrelated subjects and examined the relationship of the β-fibrinogen gene -455G>A polymorphism to cerebral infarction were included in this analysis. The internationally recognized diagnostic criterion of cerebral infarction was applied. All of the included studies have clear diagnostic criteria for ischemic stroke, and the literature that included transient ischemic attack (TIA) or hemorrhagic stroke were excluded from the study. In all of the studies, the genotype frequencies were consistent with the Hardy–Weinberg equilibrium (HWE). When the detailed genotyping information of the polymorphism was not reported, authors were contacted to obtain the relevant information. Studies were excluded if (1) patients were less than 18 or more than 80 years of age, (2) original genotype data were not obtained, (3) they investigated the same or subset population of reported articles, or (4) they did not include an appropriate case-control design.
Data extraction
Two investigators independently extracted data and reached a consensus on all of the items. For each study, the following characteristics were collected: the first author’s last name, year of publication, country of origin, numbers of genotyped cases and controls, the genotype distribution of cases and controls for the -455G>A polymorphism and the genotyping methods.
Statistical analysis
For each study, we first examined whether the genotype distribution in controls was consistent with the HWE by the χ2 test. In the majority of selected studies, the authors only presented the number of genotypes and allele frequencies and the results of the chi-square tests for them. For further analysis, we calculated the odds ratio (OR) and 95% confidence intervals (CIs) comparing the carriers of rare alleles with wild-type homozygote. According to the obtained ORs and 95% CIs, we calculated the log (OR) values and their SE (standard error). Meta-analysis was performed using RevMan 5.2 software provided by the Cochrane Collaboration. We directly used the Q-test and the I2 test to examine the heterogeneity between each study. According to the heterogeneity test, if p>0.05, we select the fixed effect model, and if p<0.05, we select the random effect model to merge ORs. Analysis of sensitivity includes the difference of point estimation and CIs of the combined effects value for a different model to observe whether it changes the result. To test the publication bias, we used the RevMan 5.2 statistical software to make the funnel plot. The statistical significance of the pooled OR was determined with the Z test, and a p-value <0.05 was considered significant.
Results
Literature search
A flow diagram of the literature search is shown in Figure 1. The primary search generated 499 potential articles. Of these, 417 studies were excluded after duplicates were removed, and 36 studies were further excluded after reading the title or abstract because of obvious irrelevance to our study aim. In all, 46 studies appeared to be potentially relevant for inclusion in our study. Twenty studies were further excluded because they did not detect the -455G>A genotype. Therefore, 26 full-text articles were reviewed. One study was further excluded for no control population. Therefore, a total of 25 articles met the inclusion criteria.11,19,24,25,27–47
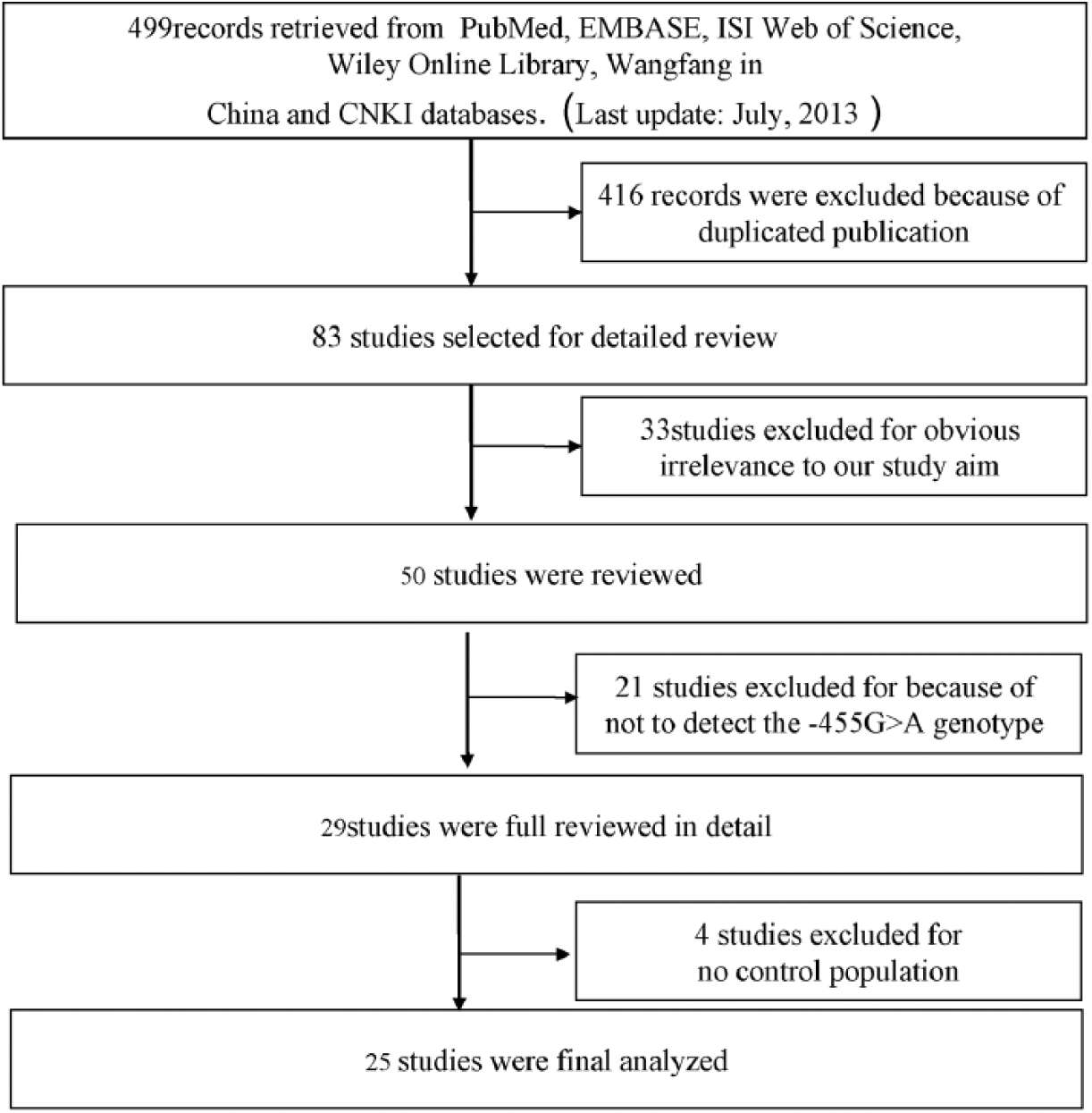
Flow diagram of study identification.
Study characteristics
The characteristics of the included studies are summarized in Table 1. The 25 included studies were published between 2000 and 2013 and comprised a total of 3822 cerebral infarction cases and 5655 control subjects. All of the subjects included in these studies were from Chinese or Caucasian populations. A classic polymerase chain reaction assay was performed in all of these 25 studies. The genotyping method in all of these studies was PCR-RFLP, and the genotype distributions among the controls of all studies were in agreement with HWE.
The characteristics of included studies.

Meta-analysis
The association between the -455G>A polymorphism and susceptibility to cerebral infarction was analyzed in 25 independent studies with 3822 cerebral infarction cases and 5655 control subjects. The Q-test in both of the genetic models showed no significant heterogeneity in total (p=0.96, I2=0%; p=0.90, I2=0%, respectively), in the Chinese population (p=0.93, I2=0%; p=0.87, I2=0%, respectively), and in the Caucasian population (p=0.99, I2=0%; p=0.96, I2=0%, respectively). Therefore, the fixed effect model was used to analysis this association. In total, we did not find any association of the -455G>A polymorphism with cerebral infarction [(AA+GA) vs. GG, OR=1.06, 95%CI: 0.99–1.15, p=0.11; A vs. G, OR=1.08, 95%CI: 0.99–1.19, p=0.09, respectively] (Figure 2 and Figure 3). After the data were stratified according to ethnicity, our results showed that -455G>A was associated with the increased risk of cerebral infarction [(AA+GA) vs. GG, OR=1.17, 95%CI: 1.04–1.31, p=0.008; A vs. G, OR=1.12, 95%CI: 1.01–1.23, p=0.03, respectively] in the Chinese population by a meta-analysis (Figure 4 and Figure 5). However, we did not find this association in the Caucasian population [(AA+GA) vs. GG, OR=0.99, 95%CI: 0.87–1.11, p=0.84; A vs. G, OR=0.97, 95%CI: 0.84–1.13, p=0.73, respectively] (Figure 6 and Figure 7).

Forest plot of cerebral infarction and -455 G>A polymorphism (AA+AG vs. GG) in total, the horizontal lines correspond to the study-specific OR and 95% CI, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95%CI. In this analysis, the fixed-effects model was used.
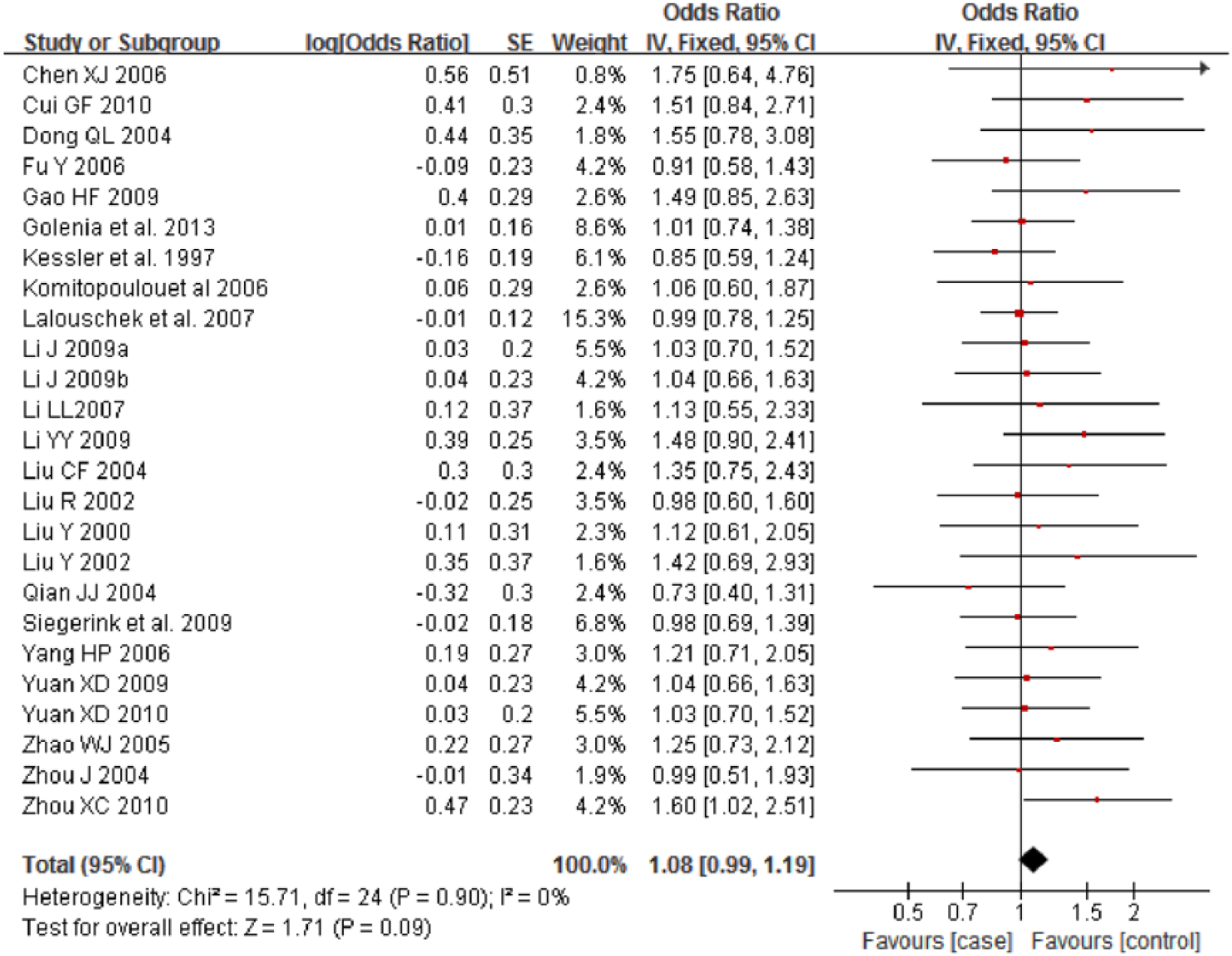
Forest plot of cerebral infarction and -455 G>A polymorphism (A vs. G) in total, the horizontal lines correspond to the study-specific OR and 95% CI, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95%CI. In this analysis, the fixed-effects model was used.

Forest plot of cerebral infarction and -455 G>A polymorphism (AA+AG vs. GG) in the Chinese population, the horizontal lines correspond to the study-specific OR and 95% CI, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95%CI. In this analysis, the fixed-effects model was used.

Forest plot of cerebral infarction and -455 G>A polymorphism (A vs. G) in the Chinese population, the horizontal lines correspond to the study-specific OR and 95% CI, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95%CI. In this analysis, the fixed-effects model was used.
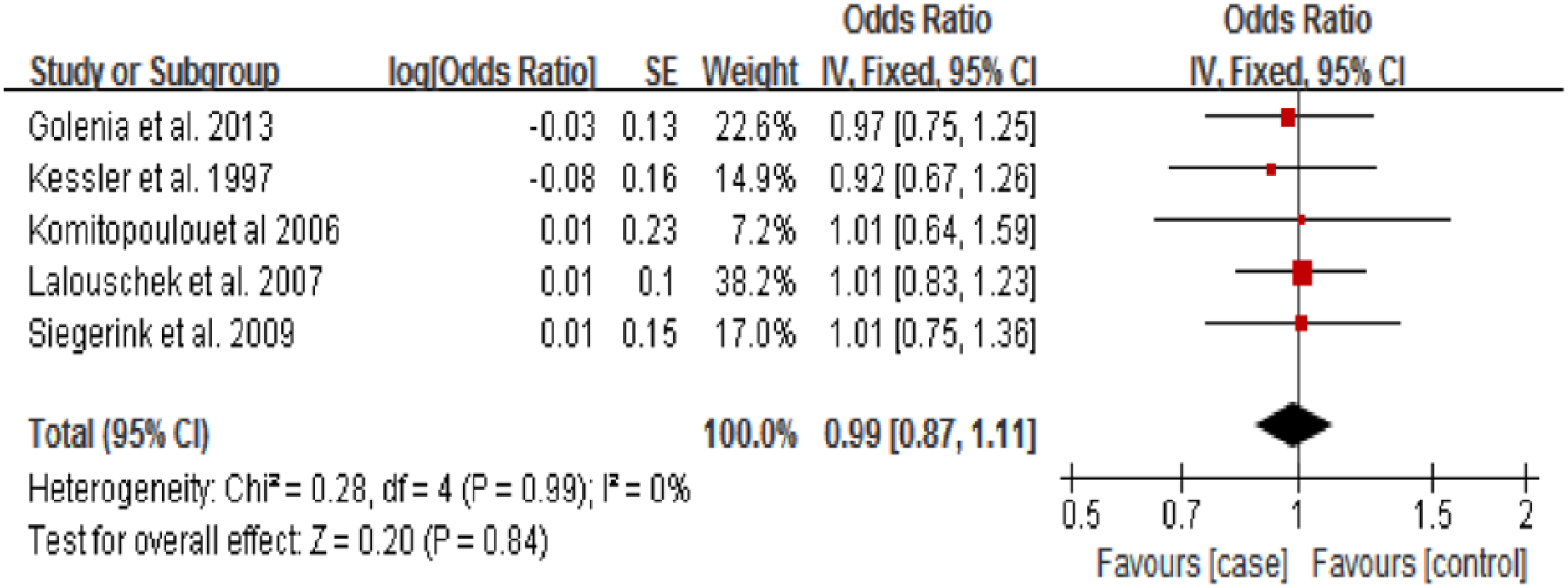
Forest plot of cerebral infarction and -455 G>A polymorphism (AA+AG vs. GG) in the Caucasian population, the horizontal lines correspond to the study-specific OR and 95% CI, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95%CI. In this analysis, the fixed-effects model was used.

Forest plot of cerebral infarction and -455 G>A polymorphism (A vs. G) in the Caucasian population, the horizontal lines correspond to the study-specific OR and 95% CI, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95%CI. In this analysis, the fixed-effects model was used.
Test of heterogeneity and sensitivity
No heterogeneity between the studies was observed in our analyses (p>0.05, I2=0%). For the sensitivity analysis, we deleted a single study from the overall pooled analysis each time to check the influence of the removed data set on the overall ORs. The pooled ORs and 95% CIs were not significantly altered when any part of the study was omitted, which indicated that any single study had little impact on the overall ORs.
Publication bias
A funnel plot and Egger’s test were performed to assess the publication bias of the literature. Symmetrical funnel plots were obtained in the SNP and tested in both models. Egger’s test further confirmed the absence of publication bias in this meta-analysis (p>0.05) (Figure 8).

Begg’s funnel plot for publication bias tests. Each point represents a separate study for the indicated association. Log OR represents natural logarithm of OR. Vertical line represents the mean effects size. A: Chinese population; B: Caucasian population.
Discussion
In this meta-analysis, we found a positive association between the -455G>A polymorphism in the β-fibrinogen gene and ischemic cerebral infarction risk in the Chinese population by a meta-analysis. The results demonstrated that -455G>A was associated with an increased risk for developing ischemic cerebral infarction in the Chinese population.
Prospective studies with large samples have suggested that plasma fibrinogen level is an independent risk factor for coronary artery disease or stroke.48–50 It is well known that elevated plasma fibrinogen levels can be affected by environmental and genetic factors. Polymorphisms of the β-fibrinogen gene, including the β-455 G/A polymorphism, which is especially involved in the rate-limiting steps of the formation of the β-chain, have been shown to be closely related to the elevation of the plasma fibrinogen level.11,19,24,25 Several studies have suggested that the -455 G/A polymorphism is associated with an elevated plasma fibrinogen concentration and ischemic stroke.27–42
Previously, two meta-analyses performed by Gu et al.51,52 examined the relationship between the -455G>A polymorphism and ischemic stroke. Gu et al.’s study involved 26 studies related to the -455G>A polymorphism and ischemic stroke. The authors found that the FGB-455G/A polymorphism is associated with ischemic stroke and coronary artery disease in the Chinese population. However, the authors found significant heterogeneity between each study. Therefore, the authors performed the meta-analyses using the random effect model to merge the OR values. Furthermore, the authors extracted the non-adjusted OR value and 95% CIs rather than the adjusted ORs and 95% CIs in the majority of the included studies to perform meta-analysis. This may be the main reason for the heterogeneity. By contrast, we extracted the adjusted ORs and 95% CI for the majority of the selected studies and combined the results of the 25 articles to pool analyze the relationship between the -455 G>A polymorphism and cerebral infarction. The results showed that there was a 17% increased risk for cerebral infarction for the variant genotypes (GA+AA) compared with the wild GG homozygotes in the Chinese population. Although our results were in line with Gu et al., we did not find heterogeneity between the studies. Therefore, our results were more credible.
Furthermore, it is characteristic of meta-analysis to combine comparable studies to increase the sample size and statistical power and to draw a more compelling result. However, meta-analysis confounds factors such as publication bias, method of sampling, different genetic backgrounds of subjects, different protocols and quality of analysis. In the present study, we did not find publication bias, and the genotypes in all of the studies were detected with genetic DNA from blood samples using PCR-RFLP genotyping methods. All of the studies checked the genotypes for quality control. Genotype distributions of controls in all studies were consistent with HWE.
In addition, exploring heterogeneity is one of the important goals of meta-analysis. In the present study, no significant heterogeneity was found among the included studies. Sensitivity analysis also showed that omission of any single study did not have a significant impact on the combined ORs. This made the results of this meta-study more reliable to some extent.
However, there remained some limitations in this meta-analysis. Although the genotyping methods used in all of the studies were the same, other clinical factors, such as age, sex and different chemotherapies in each study, might lead to bias. Determining whether these factors influence the results of this meta-analysis would need further investigation.
Conclusion
Our study suggested that the -455G>A polymorphism in the β-fibrinogen gene was associated with a mildly increased risk of ischemic stroke in the Chinese population. Larger, well-designed epidemiological studies with ethnically diverse populations and functional evaluations are warranted to confirm our findings.
Footnotes
Authors’ contributions
SYC and YDZ conceived the study, participated in the design, collected the data, performed statistical analyses, and drafted the manuscript. JWZ, RDW, and XYC conceived the study, participated in the design, and helped to draft the manuscript. All authors read and approved the final manuscript.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.