
Abstract
Background
To investigate the association between the CD14 –159C/T polymorphism and ischemic stroke (IS).
Methods
Relevant literature was searched by retrieving EMBASE, Web of Science, Chinese National Knowledge Infrastructure, and PubMed databases. R version 3.33 software was applied to calculate pooled odds ratios (ORs) and 95% confidence intervals (CIs).
Results
Seven qualified studies with a total of 2058 IS patients and 2123 controls were included. There was no significant association between the CD14 –159C/T polymorphism and IS risk in the total population (TT vs CC: OR = 0.84, 95% CI = 0.58–1.20; CT vs CC: OR = 0.96, 95% CI = 0.82–1.12; dominant model: OR = 1.02, 95% CI = 0.80–1.30; recessive model: OR = 0.82, 95% CI = 0.57–1.19). Similarly, subgroup analysis according to ethnicity and Hardy–Weinberg equilibrium also found no significant interrelation.
Conclusion
Our findings suggest that the CD14 –159C/T polymorphism does not contribute to the risk of IS. Well-designed studies with more subjects are required to further validate these results.
Introduction
Stroke is the leading cause of disability and the third highest cause of death in developed countries, with an estimated 5.7 million people worldwide dying of stroke annually.1,2 Ischemic stroke (IS), the most common type, accounts for approximately 85% of all strokes. 3 Increasing evidence suggests that IS is a complex clinical syndrome resulting from several risk factors including age, hypertension, diabetes mellitus, smoking, and dyslipidemia, all of which are important predictive factors for IS occurrence. 4 Recently, various epidemiologic studies have demonstrated that genetic factors also play an important role in the pathogenesis of IS.
Cluster of differentiation 14 (CD14) acts as a multifunctional high-affinity receptor for the binding of endotoxins, lipopolysaccharides (LPS), and other bacterial wall components that are involved in primary immune and inflammatory responses. 5 When stimulated by LPS via the CD14 receptor, monocytes express a large variety of inflammatory cytokines such as interleukin 1 and tumor necrosis factor that can activate the arterial endothelium. Furthermore, activated monocytes may contribute to atherogenesis by releasing platelet-derived growth factor that in turn leads to the proliferation of smooth muscle cells. 6
The CD14 gene contains several polymorphic sites, of which –159C/T (rs2569190) in the promoter region has been associated with differential expression levels of CD14 in monocytes and macrophages. Moreover, in atherosclerotic disease, the T allele of –159C/T has been suggested to affect circulating levels of soluble CD14. 7
Recently, accumulating evidence has indicated that the CD14 –159C/T polymorphism contributes to the development of IS. However, because of limited sample sizes, the results of these studies remain controversial or inconclusive. Therefore, in the present study, we performed a meta-analysis to investigate whether –159C/T is associated with IS risk.
Materials and methods
Literature search and selection criteria
We searched PubMed, Web of Science, Chinese National Knowledge Infrastructure, and EMBASE databases using a combination of the following key words: ‘cluster of differentiation 14 or CD14’, ‘genetic polymorphism’, ‘polymorphism’, and ‘variant’ in combination with ‘ischemic stroke’ or ‘IS’ (last updated on December, 2018). We evaluated potentially relevant genetic association studies by examining their titles and abstracts, and all published studies matching the eligible criteria were retrieved. If data or data subsets were published in more than one article, only the publication with the largest sample size was included. When a study reported the results on different ethnicities, we treated them as separate studies. Control subjects were those without history of vascular disease.
Criteria for inclusion and exclusion
Studies were included if they met the following criteria: (1) evaluated the association between the CD14 –159C/T polymorphism and IS, (2) case–control studies, and (3) detailed genotype frequencies of cases and controls were provided directly or could be calculated. The exclusion criteria were as follows: (1) studies with insufficient information such as not reporting genotype frequency or number, (2) abstracts, comments, reviews, and editorials, and (3) duplicate publications. In the latter case, only the most recent or complete study was included after careful examination.
Data extraction and quality assessment
For each research publication, the methodological quality assessment and data extraction were independently abstracted by two independent investigators using a standard protocol and data collection form according to the abovementioned selection criteria. In the case of disagreement regarding any item of data, the problem was fully discussed until a consensus was reached. Characteristics abstracted from the studies included the first author’s name, year of publication, country of origin, sources and numbers of cases and controls, and genotype frequencies.
Statistical analysis
We first assessed the Hardy–Weinberg equilibrium (HWE) of the control group in each study using the Chi-square test. The odds ratio (OR) and its 95% confidence interval (CI) were used to assess the strength of the association between the CD14 –159C/T polymorphism and IS. ORs and 95% CIs were also calculated to estimate the association between the CD14 –159C/T polymorphism and susceptibility or mortality of IS. Pooled ORs were calculated for the additive model (TT versus CC, CT versus CC), the dominant model (TT + CT versus CC), and the recessive model (TT versus CC + CT). Heterogeneity was investigated and measured using the I2 statistic, with I2 > 50% indicating evidence of heterogeneity. In the case of heterogeneity, the random effects model was used to calculate the pooled OR, whereas the fixed effects model was used in the absence of heterogeneity. One-way sensitivity analyses were performed to determine the stability of the results, with each study being omitted sequentially to reflect the influence of individual datasets on the pooled OR. Subgroup analysis based on race and HWE were performed to explore diversity among articles. Publication bias was evaluated using the funnel plot with Egger’s test. Meta-analysis was performed by using the meta-package of R 3.33 software.
Results
Study characteristics
The search strategy retrieved 58 relevant papers. Of these, seven case–control studies met the inclusion criteria8–14 and 51 studies were excluded. The study selection flow chart is summarized in Figure 1. The seven papers included 2058 cases and 2123 healthy controls. Three of the seven articles analyzed Caucasian subjects and four analyzed Asian patients. All included studies were shown to be in HWE for control genotype distribution except Lin et al. 8 and Satrupa et al. 14 Baseline characteristics of included studies are summarized in Table 1.

Flow chart of literature search and selection.
Characteristics of the included studies for meta-analysis.

HWE, Hardy–Weinberg equilibrium; PCR-RFLP, PCR restriction fragment length polymorphism; HB, hospital-based.
Meta-analysis results
A summary of meta-analysis findings of the association between the CD14 –159C/T polymorphism and IS risk is shown in Table 2 and Figure 2. We found no evidence of a significant association between CD14 –159C/T and IS (TT vs CC: OR = 0.84, 95% CI = 0.58–1.20; CT vs CC: OR = 0.96, 95% CI = 0.82–1.12; dominant model: OR = 1.02, 95% CI = 0.80–1.30; recessive model: OR = 0.82, 95% CI = 0.57–1.19). When stratified according to ethnicity (Figure 3), meta-analysis results also showed no significant association for Caucasians (TT vs CC: OR = 0.86, 95% CI = 0.62–1.19; CT vs CC: OR = 0.88, 95% CI = 0.66–1.18; dominant model: OR = 0.87, 95% CI = 0.67–1.14; recessive model: OR = 0.93, 95% CI = 0.71–1.22) or Asians (TT vs CC: OR = 0.81, 95% CI =0.45–1.44; CT vs CC: OR = 0.99, 95% CI = 0.83–1.19; dominant model: OR =0.85, 95% CI = 0.54–1.34; recessive model: OR = 0.75, 95% CI = 0.41–1.40). Similarly, when articles were stratified according to HWE (Figure 4), no significant association was found that was consistent with HWE (TT vs CC: OR = 0.78, 95% CI = 0.43–1.42; CT vs CC: OR = 0.88, 95% CI = 0.62–1.25; dominant model: OR = 0.86, 95% CI =0.55–1.36; recessive model: OR = 0.71, 95% CI = 0.38–1.31). Sensitivity analysis was performed by assessing the influence of each individual paper on the pooled OR by sequentially deleting single studies (Figure 5). No single article was found to influence the pooled ORs, suggesting that the results are stable.

Forest plots for the association of the CD14 –159C/T polymorphism with risk of IS (CT versus CC). CD14, cluster of differentiation 14; OR, odds ratio; CI, confidence interval.

Subgroup analysis by ethnicity for the association of the CD14 –159C/T polymorphism with risk of IS (CT versus CC). CD14, cluster of differentiation 14; OR, odds ratio; CI, confidence interval.

Subgroup analysis by HWE for the association of the CD14 –159C/T polymorphism with risk of IS (CT versus CC). CD14, cluster of differentiation 14; OR, odds ratio; CI, confidence interval.

Sensitivity analysis of the pooled ORs for the CD14 –159C/T polymorphism. CD14, cluster of differentiation 14; OR, odds ratio; CI, confidence interval.
Summary of comparative results.

HWE, Hardy–Weinberg equilibrium; OR, odds ratio; CI, confidence interval; Na, Number of comparisons.
Publication bias
Examination of the funnel plot suggested that there was no evidence of publication bias (Figure 6).
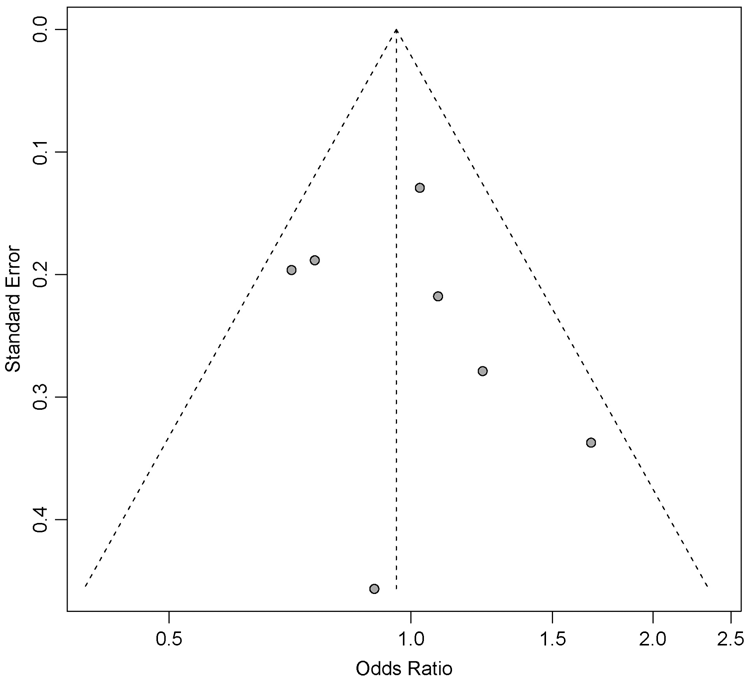
Funnel plot for publication bias in the selection of CD14 –159C/T polymorphism studies.
Discussion
IS is a multifactorial disease whose pathogenesis is not yet fully understood. 15 However, both genetic and environmental factors have been shown to be underlying mechanisms of IS, with some single nucleotide polymorphisms of susceptibility genes found to exert their effects in IS development. 16 A link between the CD14 –159C/T polymorphism and heart disease has been suggested in studies of myocardial infarction and coronary heart disease,17,18 but its relationship with IS is unclear. To better assess this, we conducted a meta-analysis to increase the statistical power of individual studies and hence obtain a more reliable result.
We included seven independent case–control studies in this meta-analysis, including a total of 4181 subjects comprising 2058 patients and 2123 healthy controls. Our findings showed that the CD14 –159C/T polymorphism did not appear to be a significant susceptibility factor for IS. Subgroup analysis by ethnicity also found no association between this polymorphism and IS susceptibility for Asians or Caucasians. Additionally, when limiting the analysis to studies that met HWE, no significant relationship was detected, suggesting that this meta-analysis is relatively credible.
These findings suggest that the risk of IS is not associated with the CD14 –159C/T polymorphism. This could be explained by the fact that several genes are associated with IS susceptibility, indicating that interactions between genes should be considered. Indeed, the CD14 –159C/T polymorphism was found to be in significant linkage disequilibrium with CD18 codon 441 polymorphisms, and two described polymorphisms were reported to synergistically increase the susceptibility to IS. 10 Alternatively, the findings may be related to the substantial heterogeneity present among the studies included in the current analysis. Heterogeneity can derive from any variation in genetic constitution and/or environmental traits among different populations, as well as from different sample selection criteria and varying study designs. 18
Several limitations of this meta-analysis should be addressed. First, the total pooled sample size was still relatively small, so may not have provided sufficient power to estimate the association between the CD14 –159C/T polymorphism and IS. Second, we did not perform subgroup analyses to examine the effects of age, sex, and interactions between genes and the environment because of a lack of sufficient data. Finally, the meta-analysis was subject to the methodological limitations of the original research studies.
In summary, our meta-analysis found no evidence for an association between the CD14 –159C/T polymorphism and IS risk. To date, research has been insufficient to identify such an association. Large datasets should therefore be considered in future studies to further evaluate the effect of gene–environment interactions.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Medical and Health Science and Technology Plan of Zhejiang Province (Program no. 2019KY134) and the Hangzhou Health and Family Planning Technology Plan (Program no. 2018Z07).