
Abstract
Hypothesis/Introduction:
The objective of this article is to investigate the effect of renin-angiotensin system inhibitors (RASIs) on intact parathyroid hormone (iPTH) levels in continuous ambulatory peritoneal dialysis (CAPD) patients.
Materials and methods:
All patients were divided into RASI-treated and non-treated groups. The relationships between the iPTH levels in CAPD patients and the clinical parameters and medication use were analyzed via linear regression.
Results:
A total of 149 CAPD patients were included in this study. The average iPTH level of the entire group was 189.4 pg/ml (range, 102.8–373.4 pg/ml). There were 79 (53.0%) and 70 (47.0%) cases in the RASI-treated and non-treated groups, respectively, with average iPTH levels of 139.0 pg/ml (range, 91.6–258.4 pg/ml) and 253.0 pg/ml (range, 134.3–467.2 pg/ml), respectively; this difference was statistically significant (p = 0.001). Multilinear regression analysis showed that age, dialysis vintage, serum phosphatemia, ALP, Hb and RASI use were independent factors that were associated with iPTH level.
Conclusion:
RASI use may be associated with a lower iPTH level in CAPD patients, although the underlying mechanism requires further study.
Keywords
Introduction
Chronic kidney disease-mineral bone disorder (CKD-MBD) is a common complication in CKD patients; the manifestations of this complication include mineral metabolism disorders, renal osteodystrophy, vascular calcification, and abnormal serum calcium (Ca), phosphorus (P), intact parathyroid hormone (iPTH), and active vitamin D (VitD) metabolism. With the development of two types of renal replacement therapies, hemodialysis and peritoneal dialysis, the survival period of CKD patients has been prolonged but at the cost of an increased incidence of CKD-MBD. iPTH, a uremic toxin, has also attracted the attention of researchers. iPTH can induce renal osteopathy, pruritus, and nervous system damage. The promotion of norepinephrine release in the atria and kidney through PTH receptor activation was found to be closely associated with occurrences of renal osteopathy and cardiovascular calcification as well as with a high risk of death.1–3
The renin-angiotensin-aldosterone system (RAAS) is a hormone-regulation system that plays important roles in the regulation of blood pressure, electrolyte levels, and blood volume stability. Studies in recent years have identified local RAAS hyperactivation as a major factor that leads to the fibrosis of important organs, such as the kidney, heart, and lung. More than a decade ago, studies had already confirmed that renin-angiotensin system inhibitors (RASIs) could delay the progression of renal lesions and provide protection to the kidney.4,5 However, the relationship between RAAS and iPTH has rarely been reported in either basic studies or clinical research. A recent study reported that RASIs might reduce the iPTH levels in hemodialysis patients. 6 Therefore, in an analysis of the peritoneal dialysis center database at our hospital, we investigated the effects of RASIs and related clinical parameters on the iPTH levels in continuous ambulatory peritoneal dialysis (CAPD) patients to provide a new perspective on the improved control of the iPTH levels in CAPD patients.
Subjects and methods
Study subjects
CAPD patients who regularly visited the peritoneal dialysis center at the Second Affiliated Hospital of Soochow University for follow-up from April to October 2013 were recruited as the study participants. The dialysis fluid used was a glucose dialysis fluid from Baxter International Inc (Deerfield, IL, USA). The inclusion criteria were as follows: patients who regularly received peritoneal dialysis in our center for >3 months and had been treated with hypertension and CKD-MBD drugs for >1 month and patients ≥18 years of age who had completed a basic clinical assessment and laboratory examination. The exclusion criteria were as follows: (1) patients with primary hyperparathyroidism, (2) patients diagnosed with tertiary hyperparathyroidism or who had undergone parathyroidectomy surgery. The present study was approved by the ethics committee of our hospital.
Methods
The dosages of the antihypertensive drugs, VitD, and calcium and the type and dosage of dialysis fluid were adjusted based on each patient’s condition during the follow-up to achieve an ideal blood pressure and ideal target levels of Ca, P, Ca × P, and iPTH in accordance with the 2003 United States (US) National Kidney Foundation Kidney Disease Outcomes Quality Initiative (NKF-K/DOQI) guidelines. Fasting blood samples were collected when the patients’ abdomen was empty. Information regarding the clinical parameters of the CAPD patients, including gender, age, dialysis duration, primary disease, the presence or absence of diabetes mellitus (DM), Ca, P, iPTH, hemoglobin (Hb), serum albumin, cholesterol, alkaline phosphatase (ALP), and serum creatinine (Scr) levels, and pulse pressure, as well as the use of drugs to treat hypertension (e.g. angiotensin II (Ang II) receptor blockers (ARBs), angiotensin-converting enzyme inhibitors (ACEIs), calcium channel blockers (CCBs), and α, β-blockers) and CKD-MBD (calcium carbonate (CaCO3), VitD), was collected. All patients were divided into either the RASI-treated or non-treated group based on their medication status.
Statistical methods
The statistical analysis was conducted with the SPSS 17.0 software package (SSPS Inc, Chicago, IL, USA). Continuous variables with normal distributions were presented as χ ± s, variables with non-normal distributions were presented as medians (interquartile range), and count data were presented as percentages (%). Comparisons of measurement data between two groups were performed with the t test, and those of count data were performed with the χ2 test. An analysis of the relevant factors was performed according to the linear regression method. Factors independently associated with log iPTH were determined using multivariate linear regression analysis adjusted for other factors with a p value less than 0.10 in univariate analyses. A p value < 0.05 indicated a statistically significant difference.
Results
Basic conditions
A total of 149 patients were enrolled, including 94 males (63.10%) and 55 females (36.90%). The patients’ ages ranged from 20 to 90 years, with an average age of 54.82 years (±14.48 years). The average dialysis duration was 34 months (range, 24–48 months). Regarding the enrolled patients’ primary diseases, there were 101 cases of primary glomerular disease (67.80%), 15 cases of diabetic nephropathy (10.10%), five cases of hypertensive nephropathy (3.4%) and 28 cases of other diseases (18.80%).
All patients were divided into the RASI-treated and non-treated groups based on their medication status. There were 79 patients taking RASI, including benazepril (n = 10), irbesartan (n = 27), valsartan (n = 19), telmisartan (n = 12), losartan (n = 9) and olmesartan (n = 8). There were three patients taking benazepril and irbesartan, while another three patients were taking benazepril and valsartan. A comparison of the patients’ clinical data between the two groups showed that the iPTH levels of the patients in the two groups differed significantly (p = 0.001), whereas differences in the clinical parameters such as age, gender, dialysis duration, the Ca, P, and Hb levels, and the use of medications that affected Ca and P metabolism, such as CaCO3 and VitD, did not significantly differ between the two groups (Table 1).
Comparison of patients’ clinical data between the groups.
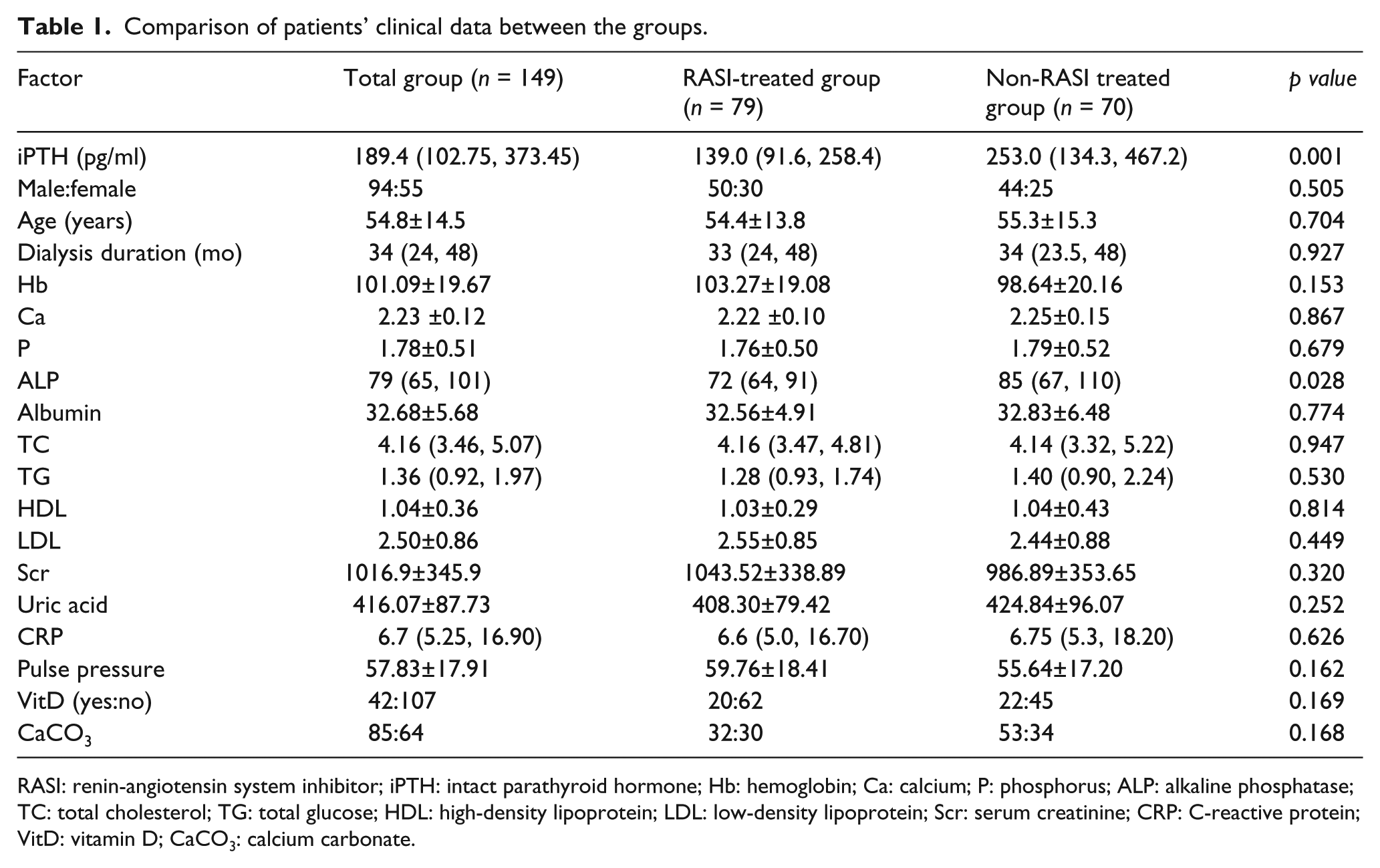
RASI: renin-angiotensin system inhibitor; iPTH: intact parathyroid hormone; Hb: hemoglobin; Ca: calcium; P: phosphorus; ALP: alkaline phosphatase; TC: total cholesterol; TG: total glucose; HDL: high-density lipoprotein; LDL: low-density lipoprotein; Scr: serum creatinine; CRP: C-reactive protein; VitD: vitamin D; CaCO3: calcium carbonate.
In this study, iPTH levels did not reveal a normal distribution and were therefore transformed into log-10 values for further analysis. The correlations between the iPTH and each clinical parameter and medication status were determined. The iPTH level was found to correlate positively with the dialysis duration and the serum P, ALP, and Scr levels and negatively with age and the Hb levels. The iPTH level did not significantly correlate with any other clinical parameter. The iPTH level was significantly lower in the RASI-treated group than in the RASI non-treated group (139.0 (91.6, 258.4) pg/ml vs 253.0 (134.3, 467.2) pg/ml, p < 0.001), and similarly, the iPTH level was significantly lower in the DM patient group than in the non-DM patient group (149.5 (79.1, 263.9) pg/ml vs 202.3 (103.4, 409.9) pg/ml, p = 0.033); both of these differences were statistically significant. The iPTH level was significantly higher in 1.25% calcium concentration dialysate-treated patients than in 1.75% calcium concentration dialysate-treated patients (257.2 (109.1, 417.9) pg/ml vs 160.5 (101.2, 254.7) pg/ml, p = 0.004). Patients taking VitD had a higher level of iPTH than those who were not (373.5 (221.9, 478.8) pg/ml vs 149.5 (81.6, 251.6) pg/ml, p < 0.001). A comparison between the patients who used CCBs, α, β blockers, and CaCO3 and those who did not use these agents revealed no significant difference in the iPTH levels (Table 2). The results of an additional multiple linear regression analysis revealed that age, dialysis duration, serum phosphatemia, Hb, ALP, 1.25% calcium concentration dialysate and RASI use were found to be independently associated with the log iPTH level (Table 3).
Factors associated with log iPTH (using univariate linear analysis).

iPTH: intact parathyroid hormone; SHPT: secondary hyperparathyroidism; OR: odds ratio; CI: confidence interval; Hb: hemoglobin; Ca: calcium; P: phosphorus; ALP: alkaline phosphatase; TC: total cholesterol; TG: total glucose; HDL: high-density lipoprotein; LDL: low-density lipoprotein; Scr: serum creatinine; CRP: C-reactive protein; RASIs: renin-angiotensin system inhibitors; ARBs: angiotensin II receptor blockers; ACEIs: angiotensin-converting enzyme inhibitors; CCBs: calcium channel blockers; CaCO3: calcium carbonate; DM: diabetes mellitus.
Factors associated with log iPTH (using multivariate linear analysis).

iPTH: intact parathyroid hormone; SHPT: secondary hyperparathyroidism; OR: odds ratio; CI: confidence interval; Hb: hemoglobin; P: phosphorus; ALP: alkaline phosphatase; Scr: serum creatinine; RASIs: renin-angiotensin system inhibitors; DM: diabetes mellitus.
Discussion
Studies have shown that in stage 3 CKD, the iPTH level has already undergone a compensatory increase independent of the serum Ca and P levels. 2 Additionally, the 2003 K/DOQI guidelines recommended that the patients’ clinical parameters, including the Ca, P, and iPTH levels, should be actively monitored at stage 3 CKD and should be maintained at the target levels of each corresponding stage. Secondary hyperparathyroidism (SHPT) can lead to significant increases in the incidence rates of excessive bone resorption, soft tissue and blood vessel calcification, and cardiovascular events among chronic renal failure patients. Therefore, studies of the relevant factors that affect the iPTH levels, as well as early intervention and control, are of particular importance for CKD patients.
The results of the present study demonstrated that the iPTH level correlated positively with the dialysis duration and the serum P, ALP, and Scr levels and negatively with age and the Hb level. A consensus has been reached regarding the hypothesis that a long dialysis duration, hyperphosphatemia, a high ALP level and low calcium (1.25%) concentration dialysate can increase iPTH. A high Scr level might reflect the intake of a high protein and high phosphorus-containing diet and insufficiently adequate dialysis, thus resulting in increases in the levels of other uremic toxins, such as serum P and iPTH. Younger patients tend to have higher iPTH levels; this finding might result from the fact that younger patients have better developed muscle tissues and more rapid metabolisms, and consequently, the toxin levels in their bodies are slightly higher than those in older patients or in those with lower metabolic rates. Currently, the relationship between Hb and iPTH is not yet completely understood, although obvious anemia is a common clinical phenomenon in patients with PTH. Studies have indicated that high PTH levels might directly inhibit hematopoiesis in the bone marrow and could shorten the lifespans of red blood cells, 7 thereby increasing the osmotic fragility of red blood cells and accelerating hemolysis. 8 Therefore, controlling PTH levels could reduce the incidence of renal anemia.
The present study showed that the iPTH levels in the RASI-treated group were significantly lower than those in the RASI non-treated group; this finding was consistent with the results of a Japanese multicenter, large-sample study 6 that reported the ability of RASIs to reduce iPTH levels in hemodialysis patients. However, the underlying mechanism remains unclear. We speculate that RASIs might reduce iPTH levels in hemodialysis patients via the following mechanisms:
A study by Mizobuchi et al. 9 showed that the iPTH levels in a group of uremic rats treated with enalapril were significantly lower than those in a control group of uremic rats. Additionally, the same study also showed that enalapril could reduce the Scr levels in the rats. Therefore, the authors proposed that enalapril did not directly act on the parathyroid gland to reduce iPTH levels but instead reduced the iPTH levels through its protective effects on the kidney. However, in our study, a comparison of the Scr levels in the RASI-treated and non-treated groups did not reveal a significant difference; therefore, we think that the effect of RASIs on iPTH levels is independent of the Scr levels.
Another mechanism might be associated with CKD-MBD. An in vitro study 10 confirmed that changes in the extracellular Ca concentration could induce juxtaglomerular cells to secrete renin; therefore, abnormal serum Ca levels might also affect iPTH levels through this pathway. Regarding the influence of RAAS on CKD-MBD, a preliminary human study showed that the iPTH levels significantly increased after an infusion of Ang II, suggesting that RAAS might indirectly affect iPTH levels via the serum Ca levels. 11 CAPD patients exhibit severe mineral and bone metabolism disorders; therefore, the increase in serum Ca and decrease in serum P levels caused by high iPTH levels and mediated through enhanced osteolysis is an important link that leads to excessive bone destruction and osteoporosis. Accordingly, we considered that RASIs might reduce the iPTH levels and improve the aforementioned symptoms. Studies have shown that Ang II could promote osteolysis and bone resorption by osteoclasts and inhibit osteoblast activity, thus leading to osteoporosis. 12 Other studies have also shown that ACEIs not only effectively controlled hypertension but also demonstrated a certain efficacy against osteoporosis in elderly patients. 13 Our study results were consistent with those of the above-mentioned studies. It should be noted that our study did not demonstrate the above-described functions of ACEIs; this discrepancy might be because the number of patients in our center who used ACEIs was limited.
It was also considered that the mechanism might involve the 1,25-dihydroxyvitamin D-fibroblast growth factor (FGF) 23-Klotho (1,25(OH)2D3-FGF-23-Klotho) pathway. FGF-23 is a negative regulatory factor of 1,25(OH)2D3 in the VitD metabolic regulation system, where it acts to suppress the PTH inhibitory and intestinal P reabsorption-promoting functions of 1,25(OH)2D3 and maintain P homeostasis in the body, thus playing important roles in the occurrence and development of CKD-MBD. 14 Klotho is a newly discovered anti-aging gene, 15 the expression of which is found primarily in the kidney; therefore, Klotho has received extensive attention. FGF-23 binds to and activates its receptor FGFR1. The latter is coexpressed only with the Klotho transmembrane protein; in other words, FGFR1 is functional only if it can form a Klotho-FGFR complex. Klotho protein expression is reduced in the kidneys of CKD patients; consequently, the target organs are resistant to FGF-23 and cannot maintain P and 1, 25(OH)2D3 homeostasis throughout the body. Therefore, under the persistent influences of high extracellular P, low extracellular Ca, and significantly reduced serum calcitriol levels in CKD patients, PTH synthesis and secretion increase along with FGF-23 expression to downregulate the renal expression of residual 1-hydroxylase, thus causing calcitriol deficiency and a subsequent increase in PTH. 16 Mitani et al. 17 observed the function of Ang II with respect to the regulation of Klotho gene expression in the kidney and found that a long-term injection of Ang II into rats downregulated Klotho messenger RNA (mRNA) and protein expression in the kidney. A study by Qiaoling et al. 18 demonstrated that the type I Ang II receptor was a key molecule in the Ang II-mediated regulation of Klotho gene expression. The inhibitory effect of Ang II on Klotho gene expression is dose dependent and can be antagonized by valsartan. Therefore, we considered that in CAPD patients, RASIs might block the inhibitory effect of Ang II on the Klotho gene and thus allow the upregulation of Klotho mRNA and protein expression to increase the affinity between the target organs and FGF-23, thus reducing PTH synthesis throughout the body.
The results of the present study showed that the iPTH levels in DM patients (149.5 (79.1, 263.9) pg/ml) were significantly lower than those in non-DM patients (202.3 (103.4, 409.9) pg/ml, p = 0.033); the underlying mechanism behind this difference might also be associated with the Klotho protein. Klotho expression is considered an excellent indicator of insulin resistance (IR). However, there is currently no consensus on the Klotho-mediated regulation of insulin and the insulin-like growth factor 1 (IGF-1) signaling pathway or on the effect of Klotho on IR. Kurosu et al. 19 reported that Klotho played an anti-aging role through the inhibition of insulin and IGF-1 signal transduction. A study by Holzenberger et al. 20 confirmed that Klotho could reduce IGF-1 signaling pathway activity without altering the insulin level or activity. A recent study 21 showed that Klotho did not inhibit the insulin and IGF-1 signal transduction pathways; however, whether Klotho might affect insulin sensitivity via FGF-23 activation remained inconclusive. Therefore, a reduction in the iPTH levels in DM patients might be associated with FGF-23 activation, although the underlying mechanism awaits further study.
In summary, the results of an analysis of data from our center revealed that the overall iPTH levels were relatively high in CAPD patients and were found to correlate with patient age, dialysis duration, the Hb, serum P, ALP, and Scr levels, DM status, and RASI use. The multivariate regression analysis showed that hyperphosphatemia, a high ALP level, and RASI use were independent risk factors that affect the iPTH level.
The present study is a clinical study; therefore, the underlying mechanisms of the effects of RASIs and DM on the iPTH levels could not be proven at a molecular level. Furthermore, in this study, we didn’t test aldosterone levels and renin activity in peritoneal dialysis patients. The interaction relationship of the renin-RAS-aldosterone axis and PTH level needs further investigation. Because the present research involved a single-center, small-sample sized, cross-sectional study, the effect of high iPTH levels on the prognosis of CAPD patients was not investigated. Therefore, additional multicenter cohort follow-up studies and basic research studies are needed in the future.
Footnotes
Conflicts of interest
None declared.
Funding
This work was supported by a grant from the National Natural Science Foundation of China (no 81302584).