
Abstract
Primary aldosteronism (PA) is estimated to occur in 5–12% of patients with hypertension. Assessment of aldosterone / plasma renin activity (PRA) ratio (ARR) has been used as a screening test in patients suspected of PA. Direct determination of renin (DRC) and calculation of aldosterone / direct renin concentration ratio (ADRR) could be similarly useful for screening patients suspected of PA. The study included 62 patients with indication for evaluation of the renin-angiotensin-aldosterone system and 35 healthy volunteers. In all participants we measured concentrations of serum aldosterone, plasma direct renin, and PRA after a night’s rest and again after walking for two hours. The concentrations of aldosterone, direct renin, and PRA were measured by isotopic methods (radioimmunoassay (RIA) / immunoradiometric assay (IRMA)). Correlations of ARR with ADRR in the supine position were r = 0.9162, r2 = 0.8165 (p < 0.01); and in the up-right position were r = 0.7765, r2 = 0.9153 (p < 0.01). The cut-off values of ARR and ADRR ≥ 100 presented highest specificity (99%) for the diagnosis of PA; however, quite acceptable specificity and sensitivity (> 80% and 100%, respectively) appeared for the ratios ≥ 30. We suggest that for practical and economic reasons ARR can be replaced by ADRR.
Introduction
Primary aldosteronism (PA) is one of the causes of hypertension, it is estimated that it may occur in 5–12% of patients with hypertension.1, 2 Some patients with PA have severe hypertension (sometimes drug-resistant) or mild hypertension with or without hypokalemia. In cases of hypertension and adrenal incidentaloma or hypertension with family history of early-onset hypertension or cerebrovascular accident at a young age (< 40 years), a search for PA is strongly recommended.3, 4
Determination of serum or plasma aldosterone, urine aldosterone, plasma renin activity (PRA), and calculation of aldosterone / PRA ratio have been the most widely used for screening patients suspected of PA. Direct determination of the renin concentration (DRC), which is less labor-intensive and time-intensive, and the calculation of aldosterone / direct renin concentration ratio (ADRR) could be similarly useful for screening patients suspected of PA. So far, not very many comparative studies evaluating both these indices have been performed.5–7
Aim of the study
The aim of the study was to determine whether the ratio serum aldosterone / PRA (ARR) can be replaced by the ratio serum aldosterone / DRC (ADRR).
Material and methods
Patients
62 patients directed for evaluation of renin-aldosterone-angiotensin system (11 males, 51 females, mean age 50, range 20–76 years), after setting final diagnosis, were grouped in 8 clinical subgroups: 10 with PA (6 with adrenal adenomas, 4 with adrenal hyperplasia), 25 with adrenal incidentaloma, 11 with adrenal adenoma and androgenization, 5 with pre-Cushing’s syndrome, and 6 with rare cases (secondary aldosteronism, essential hypertension, pheochromocytoma, and adrenal carcinoma). The control group included 35 healthy volunteers (7 males, 28 females, mean age 43, range 20–69 years).
All patients had elevated blood pressure (systolic blood pressure > 140 mmHg, and/or diastolic blood pressure > 90 mmHg). Investigations included routine hormonal and biochemical determinations and imaging procedures: ultrasonography (USG), computed tomography (CT), or magnetic resonance imaging (MRI). Antihypertensive medications which could have influence on the aldosterone-renin-angiotensin axis were usually stopped for at least 7–14 days.
The following combined diagnostic criteria for PA were established in our study: (1) serum aldosterone concentration > 15 ng/dl; (2) PRA ≤ 0.3 ng/ml per hour; (3) ARR ratio ≥ 40; (4) urine aldosterone concentration ≥ 12 μg/24hr.
Diagnosis of PA was confirmed in 6 of 10 cases by histopathological investigation of the removed adrenal tissue, and in one case by Captopril test. In the remaining there cases with bilateral lesions, a combined pharmacological treatment including aldosterone antagonists appeared fully efficacious and patients did not want to be further investigated.
All patients had blood collected after a night’s rest in the supine position (0 hr) and again in the up-right position after walking for two hours (2 hr). At each collection, blood was withdrawn into one EDTA2K tube (plasma) and one with clot activator (serum). Cooled samples were transported to the laboratory (within 10 minutes), and centrifuged in cool condition (4°C, 3500 rpm,10 minutes) The obtained biological material (serum, EDTA2K-plasma) was frozen under −30°C and stored until being assayed.
Hormonal assays
Aldosterone in serum was measured by radioimmunoassay (RIA) method (ZenTech, RIAZENco, Belgium). Urinary aldosterone was measured by the same RIA after acid hydrolysis (0.1 N HCl). Analytical sensitivity was 1.4 ng/L and functional sensitivity was 25 ng/L. According to the equipment’s producer, the reference value for serum aldosterone at rest in the supine position was 10–160 ng/L, and in the up-right position was 35–300 ng/L. The reference value for aldosterone in urine was 2.8–30 μg/24 h (value >12 μg/24 h was considered as a “gray zone”).
Intra-assay coefficients of variation (CV) were as follows: 13.7% for 42 ng/L, 3.8% for 177 ng/L, and 5.3% for 278 ng/L and inter-assay CV values as follows: 18.6% for 38 ng/L, 7.5% for 169 ng/L, and 6.2% for 284 ng/L.
PRA was measured by RIA, (CISbio, France). The standard 90 minutes incubation time was applied for Angiotensin I generation. Analytical sensitivity was 0.15 ng/ml per hour. According to the equipment’s producer, the reference value at rest in the supine position was 0.2–2.8 ng/ml per hour, and in the up-right position was 1.5–5.7 ng/ml per hour. Intra-assay CV values were as follows: 4.3% for 1.4 ng/ml per hour, 6.5% for 3.8 ng/ml per hour, and 7.2% for 16.0 ng/ml per hour. Inter-assay CV values were as follows: 9.9% for 1.4 ng/ml per hour, 4.9% for 3.9 ng/ml per hour, and 8.5% for 15.8 ng/ml per hour.
Direct plasma renin concentration (DRC) was measured by immunoradiometric assay (IRMA) equipment, (CISbio, France). Analytical sensitivity was 1 ng/L. According to the equipment’s producer, the reference value at rest in supine position in patients between 20–40 years of age was 3.6–20.1 ng/L and between 41–60 years 1.1–20.2 ng/L, and in the up-right position in patients between 20–40 years was 5.1–38.7 ng/L and between 41–60 years 1.8–59.4 ng/L. The intra-assay CV values were as follows: 3.6% for 3.8 ng/L, 1.5% for 65.4 ng/L, and 0.9% for 262 ng/L. The inter-assay CV values were as follows: 5.0% for 4 ng/L, 3.6% for 72 ng/L, and 4.0% for 263 ng/L.
The ARR was calculated using measurement of serum aldosterone concentration to PRA (ng/dl) / (ng/ml per hour) and ADRR — serum aldosterone concentration to DRC in plasma (ng/l) / (ng/l).
The study was approved by the Bioethics Committee of The Centre of Postgraduate Medical Education.
Statistical analysis
Data are expressed as medians (lower and upper quartiles) and means ± standard deviation (SD). The Kruskal-Wallis test, followed by Dunn’s post-hoc test and the multiple Mann-Whitney U-test were performed to estimate differences between groups. The relationship between the compared results was expressed using Sperman’s rank correlation analysis and Pearson linear correlation analysis. The cut-off values for ARR and ADRR in the supine (0 hr) and the up-right (2 hr) positions to confirm PA were based on receiver operating characteristics (ROC) curve analysis. A p-value of < 0.05 was considered to be significant and p < 0.01 highly significant. All statistical analysis was performed using statistical software (PQStat ver. 1.4.2.324).
Results
Clinical characterization of the studied groups of patients is presented in Table 1. Results of ARR and ADRR were significantly higher in patients with PA (p < 0.0001) in relation to other clinical subgroups of patients with androgenization, pre-Cushing’s syndrome, adrenal incidentaloma, and healthy volunteers (Table 2 and 3).
Clinical characterization of the studied subgroups of patients. Results are expressed as means ± SD.

Comparison of serum aldosterone, PRA, DRC, ARR, and ADRR in patients with PA and other clinical subgroups in supine position. Results are expressed as medians (lower and upper quartiles) and means ± SD.
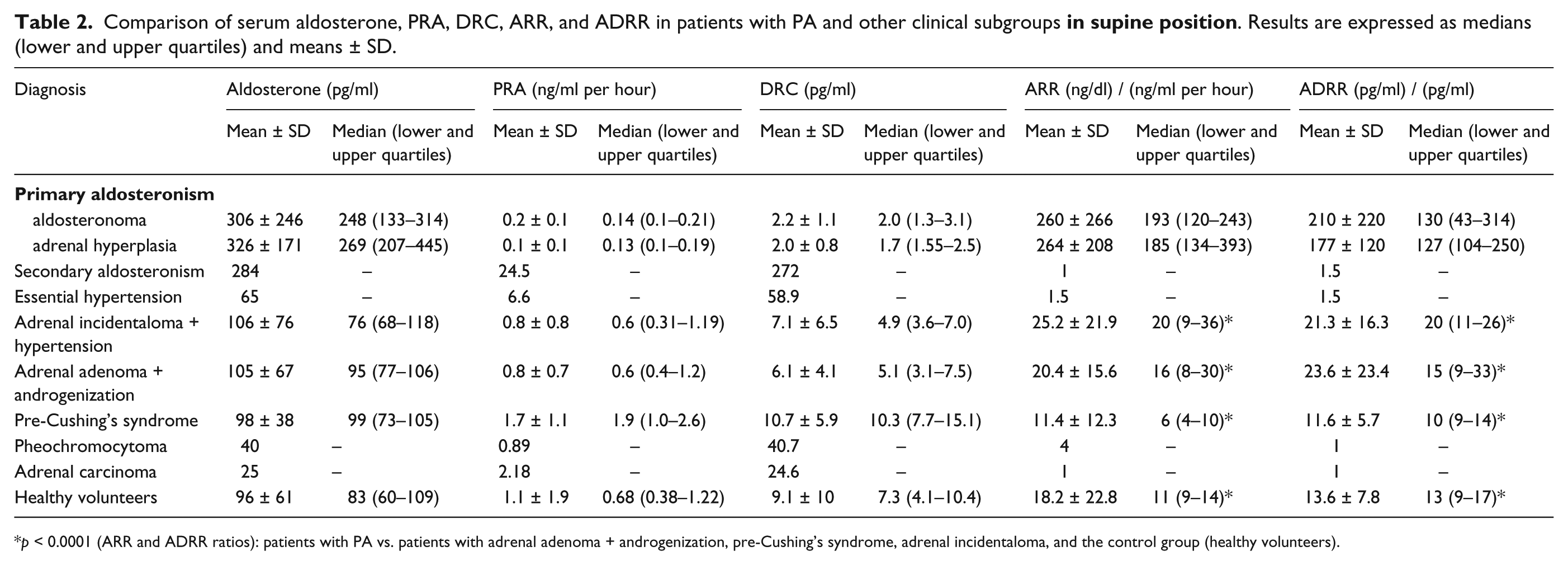
p < 0.0001 (ARR and ADRR ratios): patients with PA vs. patients with adrenal adenoma + androgenization, pre-Cushing’s syndrome, adrenal incidentaloma, and the control group (healthy volunteers).
Comparison of serum aldosterone, PRA, DRC, ARR, and ADRR in patients with PA and other clinical subgroups

p < 0.0001 (ARR and ADRR ratios): patients with PA vs. patients with adrenal adenoma + androgenization, pre-Cushing’s syndrome, adrenal incidentaloma, and the control group (healthy volunteers).
Correlation of ARR with ADRR in the supine position (0 hr) was r = 0.9162; r2 = 0.8165; p < 0.01 and correlation of ARR with ADRR after walking for two hours (2 hr) was r = 0.7765; r2 = 0.9153; p < 0.01. The results are presented in Figures 1 and 2.

Correlation of ARR (0 hr) versus ADRR (0 hr).
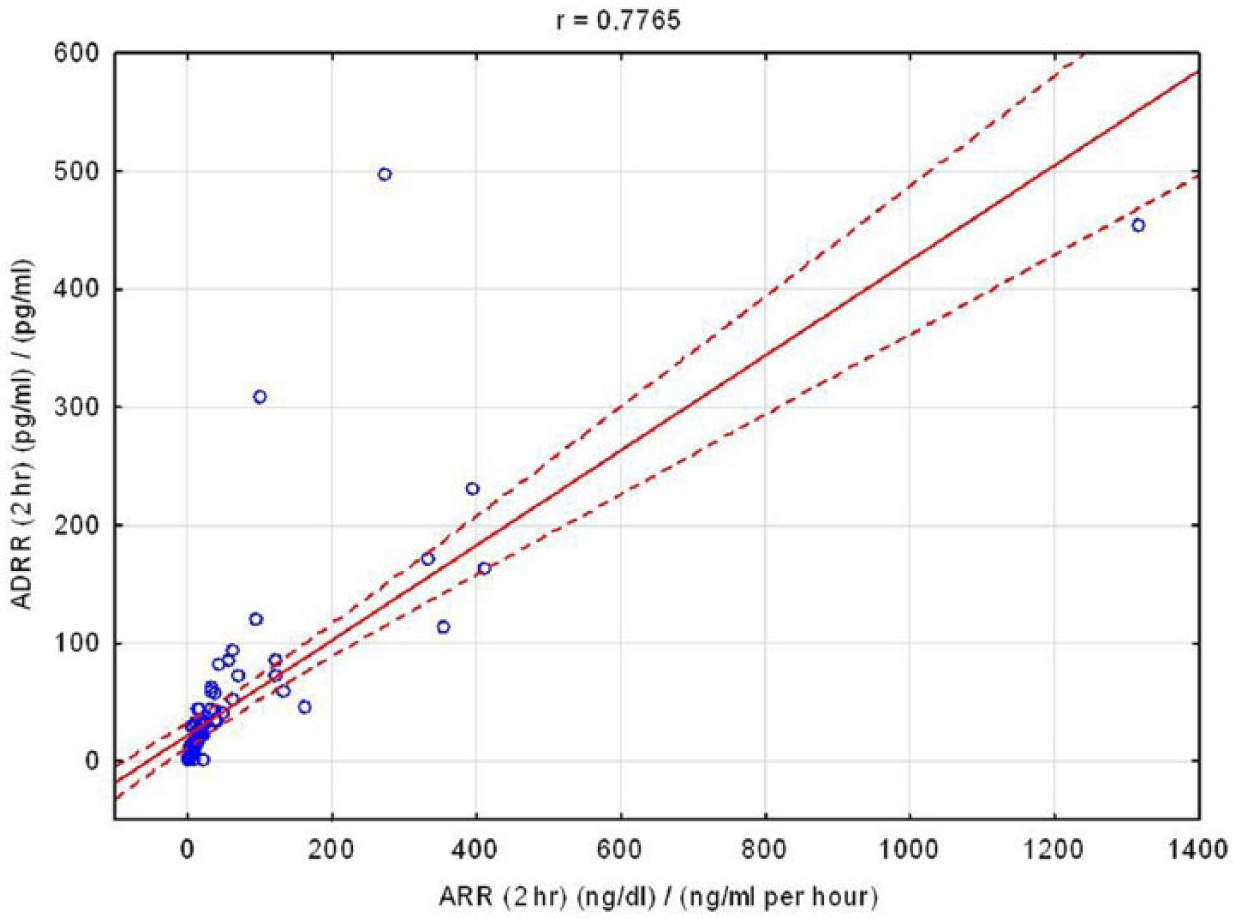
Correlation of ARR (2 hr) versus ADRR (2 hr).
In Table 4 we present a comparison of indices: ARR and ADRR in 10 confirmed cases of PA.
Comparison of indices: aldosterone / PRA and aldosterone / DRC, in 10 confirmed cases of PA.
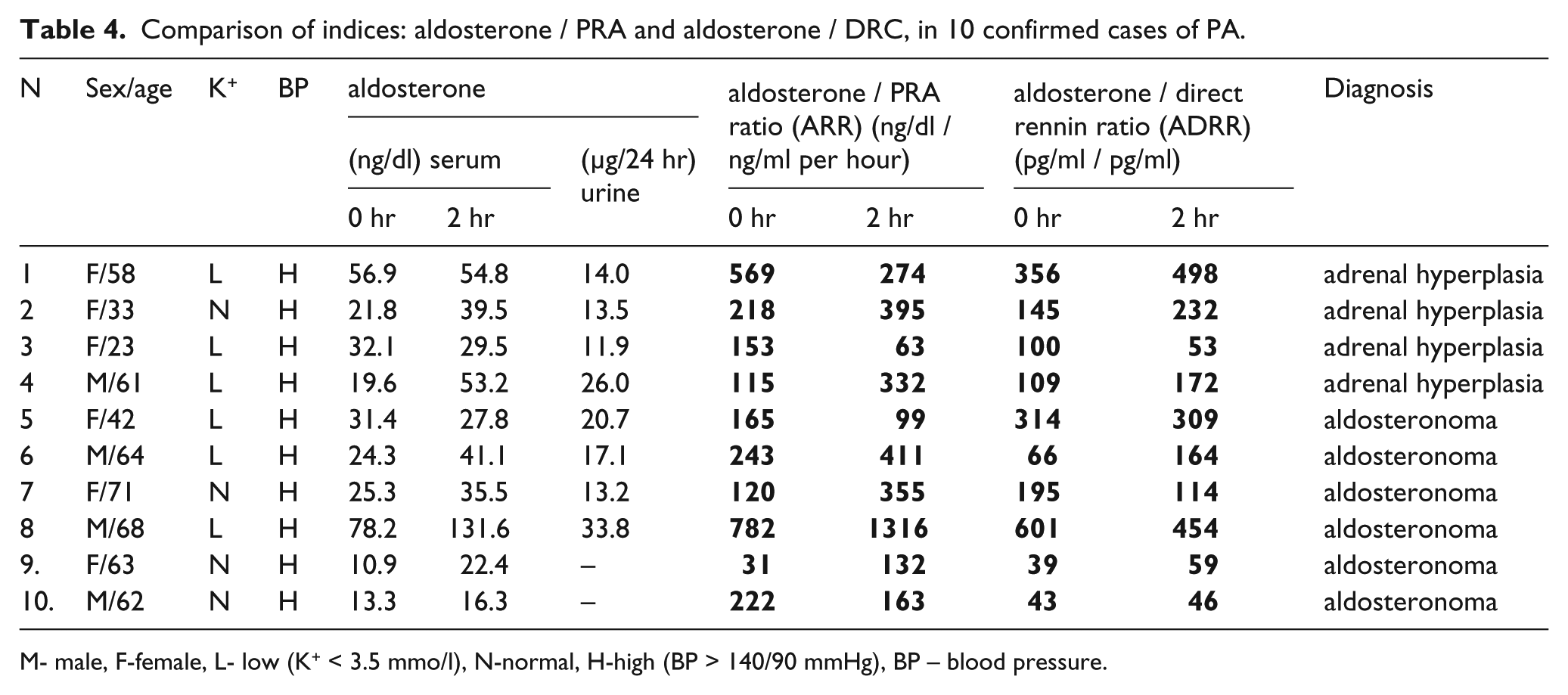
M- male, F-female, L- low (K
The areas under the curve (AUC) for ARR (0 hr), ARR (2 hr), ADRR (0 hr), and ADRR (2 hr) were as follows: 0.98, 0.99, 0.98, and 0.97 respectively, and the cut-off values were as follows: 115, 132, 100, and 164 respectively. The sensitivity and specificity calculated for three levels of the cut-off values of ARR and ADRR are presented in Table 5.
Specificity, sensitivity, and accuracy of the chosen cut-off values of ARR and ADRR at 0 hr and 2 hr.

Discussion
In patients with adrenal adenoma and hypertension, ARR has been proposed as a screening test for PA.
The first introduction of ARR as a screening test was done by Hiramatsu et al. in 1983. 8 This approach, followed usually by one of the confirmatory tests, indicated that PA is much more common than it has been estimated in the past. The variety of PRA and aldosterone assays, expressing results in various units and various positions of blood collection caused a marked variation in the ARR cut-off value, which ranged from 20 to 100. 9 The reported sensitivity and specificity of the ARR, calculated usually for the up-right position, varied between 64% and 100%, and 87% and 100%, respectively. 10 , 11
In our study we collected blood both after a night’s rest (0 hr), and again after 2 hours (2hr) of up-right position, and presented the sensitivity and specificity for three levels of the cut-off values of ARR and ADRR.
It is not easy to determine the optimal cut-off value because actually it depends on particular conditions of testing and the laboratory methods.
Tiu et al., 11 who measured serum aldosterone level and PRA, showed that the cut-off values of ARR above 66.9 presented 100% specificity but 64.5% sensitivity, whereas with the cut-off value 23.6 the sensitivity and specificity were 96.8% and 94.1, respectively. Therefore, they mention that if the ARR value is less than 23.6, clinicians can be assured that the likelihood of PA is extremely low.
Olivieri et al. 12 observed in their work good correlation of PRA and DRC (r = 0.87, r2 = 0.75; p < 0.000), and cut-off values of ARR and ADRR, with the measured plasma aldosterone, was 50 for ARR and 32 for ADRR.
In the study of Unger et al., 13 who also measured plasma aldosterone level, ROC analysis suggested that an ADRR value of 90 might indicate a diagnosis of PA (sensitivity 100%, specificity 98.6%, AUC = 0.99) and with the cut-off value of 62 (with plasma aldosterone concentration ≥ 200 ng/l), the sensitivity and specificity were 100%, respectively, for the diagnosis of PA.
In the paper of Rossi et al., 14 the AUC for the ADRR was 0.870 ± 0.058 and for the ARR it was 0.973 ± 0.028.
In our study, comparison of the AUC, performed for both indices, showed that both indices for the cut-off value above 100 had a very high discriminative ability above 95%.
The correlations of both indices (ARR and ADRR) were as follows: for the supine position (0 hr) r = 0.9162, r2 = 0.8165 and after walking two hours (2 hr) r = 0.7765, r2 = 0.9153. A similar correlation was observed in a study of Ferrari et al. 15 In their work, the correlation between ARR and ADRR indices in the supine position for one hour was r = 0.96.
The reported values of ARR were mostly determined by changes in PRA (depending mainly on the assay sensitivity) but in part they could be influenced also by the noted differences in aldosterone levels measured in plasma or serum. 16 Such differences were reported also by Taylor et al. 17 who used high performance chromatography and tandem mass spectrometry. Fisher et al. 18 also noted marked differences in aldosterone levels determined in various laboratories but he did not compare results in plasma (EDTA) and serum samples obtained from the same patients. Fisher only suggested that the differences were due to different assays and possibly various pre-analytical conditions.
Determination of DRC instead of PRA was proposed because it offers advantages with regard to sample processing, easier procedure, and better precision (one measurement instead of the calculated difference of two measurements: heated and blank samples).
ADRR appeared quite similar to ARR if the results were expressed in ng/L / ng/L for ADRR and ng/dl / ng/ml per hour for ARR, respectively.
Numerous factors which affect aldosterone, direct renin, renin activity, and the calculated ratio (body posture, potassium level, and hypotensive and diuretic drugs) are listed in clinical practice guidelines.3,4 These effects are in general similar for DRC and PRA, apart from a few clinical conditions, namely pregnancy and estrogen administration, especially use of oral contraception (leading to low renin and high PRA due to the increased production of angiotensinogen), and congestive liver failure (high direct renin corresponds with low PRA due to a low level of angiotensinogen).16,19
Pre-ovulatory surge in estrogen followed by the raising progesterone level may also be a cause of false positive aldosterone / renin ratio using DRC (but not PRA) during the luteal phase of the menstrual cycle. 20
There is no doubt that measurement of direct renin is easier and more economical than PRA. However, it should be noted that both calculated ratios can be used only as a screening investigation, and, according to guidelines, if possible should be confirmed by one of the accepted confirmatory tests, and, if necessary, by adrenal venous sampling.2–4, 9
Conclusions
The cut-off values for ARR (0 hr), ARR (2 hr), ADRR (0 hr), and ADRR (2 hr) ≥ 100 presented highest specificity for the diagnosis of PA, however, quite acceptable for the screening test specificity and sensitivity, appeared for the ratios ≥ 30.
ARR and ADRR in general show good correlation. We think therefore that for practical and economic reasons ARR can be replaced by ADRR.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by The Centre of Postgraduate Medical Education grant no. 501-1-08-11/12 and 501-1-08-11-13.