
Abstract
Typologies are a useful and widely employed instrument in comparative research, including the study of health care systems. This study analyses the effectiveness of extant classifications in representing health care systems globally, examining whether existing literature adequately helps to understand health care systems of the Global South. To this end, the study highlights key elements of health care systems in the Global South, in particular limited resources, segmentation and the involvement of non-domestic/international actors. In a further step, we conduct a systematic literature review of typological scholarship on health care systems, in which 42 classifications are identified and analysed regarding regional coverage, methods, as well as the criteria and categories they include. The results point to major limitations: First, there is a general lack of representation and systematic classification of health care systems of the Global South. Second, there is a bias as criteria for classification are developed inductively based upon health care systems of the Global North. Consequently, existing typologies mostly fail to take into account the particularities of the countries beyond high-income economies. The study concludes by putting forth recommendations for developing a more comprehensive, globally applicable typological framework.
Keywords
Introduction
When studying complex phenomena like health care systems, comparisons and, by extension, typologies, are useful means to gain a better understanding thereof. In particular, the usage of typologies enables the researcher to reduce the complexity of ‘messy’ empirical reality, enabling her to analyse similarities and variation systematically and detect and interpret patterns. To date, dozens of instruments for grouping and comparing countries’ health care systems have been introduced, which often diverge greatly regarding the background and interests of the researcher, temporal and geographical context, and data availability. Yet, while a great deal of typological work has already been undertaken in the field, existing approaches might still suffer from ‘blind spots’ or biases. Therefore, scholars emphasise the necessity of regularly revisiting and reviewing established classifications 1 to ensure their ongoing validity and relevance in portraying the complexity and constant changes of the empirical world (Freeman and Frisina, 2010; Lazarsfeld, 1937). In this article, we thus return to the scholarship that classifies health care systems to reassess their relevance and usability: Are present classifications able to capture the developments and variety of health care systems globally? In particular, do existing typologies reflect the particularities of health care systems of the Global South 2 ? Answering these questions is not only relevant for gaining an overview of how typological tools for studying health care arrangements are specified and applied, but can also advance reflection on the impact (typological) research has on the construction and evaluation of health care systems, particularly in the Global South.
Research on health care systems often describes the arrangements found in the Global South in terms of insufficient resources, limited institutional capacity, and great degrees of inequality and discrimination with respect to service provision (Mills, 2014). Although all health care systems, regardless of their resources, face numerous challenges, empirical research demonstrates great disparities between and within health care systems in low- and middle-income countries (LMICs) and high-income economies. From the many particularities of health care systems of the Global South, two issues were selected for detailed analysis: segmentation and the role of international actors. Both are related to the institutional/actor set-up of systems often measured by typologies. The former aspect has been chosen for consideration as it influences critical functions of the health care system and can potentially undermine the quest for universal health care. The latter is analysed as the domestic institutional and financial capacity of LMICs might be connected to a greater presence of foreign states, international organisations (IOs) and international non-governmental organisations (INGOs) (Kaasch, 2013; Ruger, 2007; Weyland, 2006). These particularities lead us to assume that existing typologies might not adequately capture a broader variety of health care systems worldwide, though we do acknowledge that such instruments are not able to portray the whole universe of the phenomena given that their fundamental purpose is to reduce complexity. Yet, we posit the need for a more encompassing tool for worldwide comparison.
In this article, we conduct a systematic literature review of the extant classifications of health care systems, with a particular view to their usability for classifying LMICs. In what follows, we begin by discussing characteristics of health care systems in countries of the Global South. We also provide a brief background to different forms of classification in the social sciences, reflecting on the use of inductive versus deductive logics, and qualitative versus quantitative methods for classification. We then move to describing the methods used to identify publications for review. In the section that follows, we summarise our findings from the review, analysing the regional scope, methodology and criteria for classification of the 42 identified typologies. Finally, we employ the findings from the review to evaluate the usability and relevance of extant typological scholarship for comparing health care systems globally, and conclude by offering recommendations for next steps for research.
Health care systems of the Global South
Health care systems of LMICs are far from homogeneous, ranging from state-led systems seen in Cuba and Brazil to systems that mainly rely on private financing like Azerbaijan and Equatorial Guinea (Global Health Expenditure Database, 2017). In recent decades, scholarship on LMICs has expanded rapidly, producing in-depth country analysis on countries such as China (e.g. He and Wu, 2017), India (e.g. Tavecchi and Rebecchi, 2018) and Ghana (Coleman, 2011), as well as comparative work on African (e.g. Azevedo, 2017), Asian (e.g. Aspalter et al., 2017) and Latin American (e.g. Mesa-Lago, 2007) countries, and inter-regional studies (e.g. Balabanova et al., 2011). Although the growing body of literature shows that health systems in the Global South are not uniform, research identifies characteristics shared by many LMICs. For instance, Hanson et al. (2003) and Mills (2014) catalogued 19 characteristics/constraints of health care systems in these countries, varying from staff shortage and low levels of health care access to inadequate regulation of the pharmaceuticals and private sectors. These characteristics can be split into three main categories: lack of and/or insufficient resources, weak state capacity in terms of regulation and administration of the systems, and burden of diseases.
Differences between Northern and Southern systems are even greater than within LMICs (Table 1). For instance, on average, in high-income countries, health care per-capita spending is 161 times greater than in low-income nations. In addition, there is a substantial difference regarding state involvement in financing health care between high- and low-income economies. In richer economies, states are, on average, responsible for almost 80% of health expenditure. In low-income countries, on the contrary, governments fund less than 25% of the services. Furthermore, the World Health Organization (WHO, 2019a) estimates that systems with less than 2.3 health professionals per 1000 inhabitants are unlikely to provide adequate essential services. Low-income countries fall below this threshold, with only 1.18 health professionals per 1000 inhabitants.
Selected indicators of health care financing, infrastructure and provision, by income groups (latest data available).
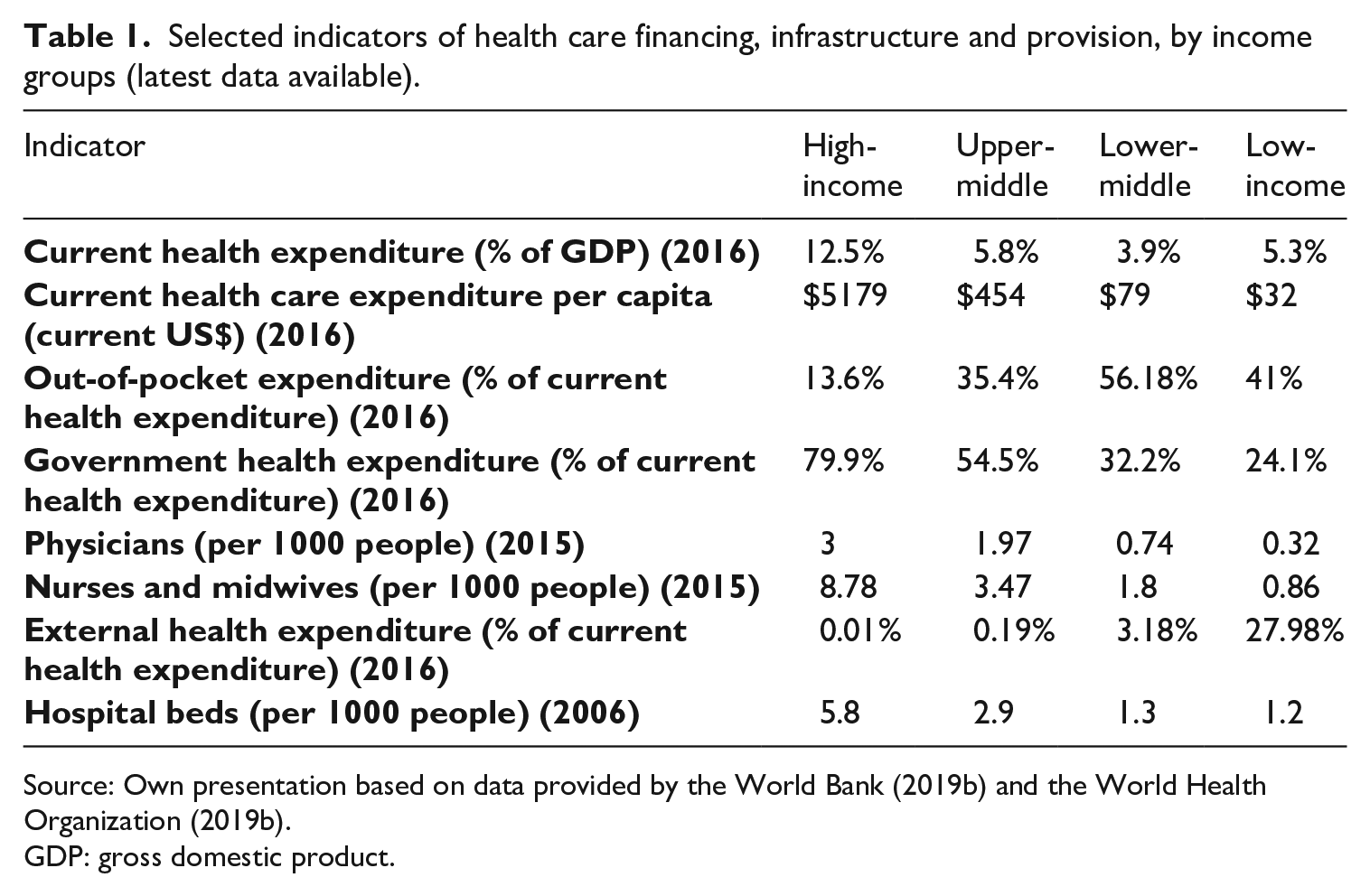
Source: Own presentation based on data provided by the World Bank (2019b) and the World Health Organization (2019b).
GDP: gross domestic product.
Given the limited or absent possibilities for domestic resource mobilisation, some LMICs heavily rely on international actors to finance, deliver services and administrate their systems. For instance, from 1990 to 2016, aid from bilateral, multilateral and other donors provided more than US$531 billion to economies of the Global South for financing health care (Institute for Health Metrics and Evaluation, 2017). In 20 nations, foreign transfers are responsible for more than one-third of all funds available for health (Global Health Expenditure Database, 2019). Often, the availability of external funds is contingent on the fulfilment of predetermined conditions, the so-called conditionalities. The failure to comply with these stipulations may undermine the full disbursement of the loan or jeopardise the prospect of receiving future loans or financing (Babb and Carruthers, 2008). The World Bank and the International Monetary Fund (IMF) are examples of IOs that use conditionalities to force countries to adopt specific health policy agendas (Clements et al., 2013; Kaasch, 2013). Regarding technical and staffing resources, non-profit actors, such as Médecins Sans Frontières and Red Cross, often take responsibility for delivering health services through the employment of health professionals or by running medical facilities.
Another feature of health systems of the South is segmentation, which refers to the coexistence of different modalities of financing, service delivery and affiliation, each of them targeting different population groups according to income, social status and/or type of employment (Frenk and Londoño, 1997; Mesa-Lago, 2007; Pan American Health Organization, 2007). In organisational terms, in segmented systems, public, not-for-profit and for-profit financing agencies and providers coexist (Pan American Health Organization, 2007; WHO, 2019c). Table 2 breaks down health care systems by financing source in selected LMIC nations, which often indicate the presence of multiple schemes, and shows the level of stratification of health care systems. Often, in countries presenting a ‘segmented model’, the poor are beneficiaries of public services due to their exclusion from formal employment. Meanwhile, the upper classes are covered by social and/or private insurance. Taking into account that public services only provide basic care, supplementary forms of insurance and out-of-pocket payments are used by those who are able to afford them (Frenk and Londoño, 1997). For the better off, therefore, private insurance becomes the primary system, given the rudimentary nature of public health care.
Health expenditure by finance scheme (% of current health expenditure) (2016).
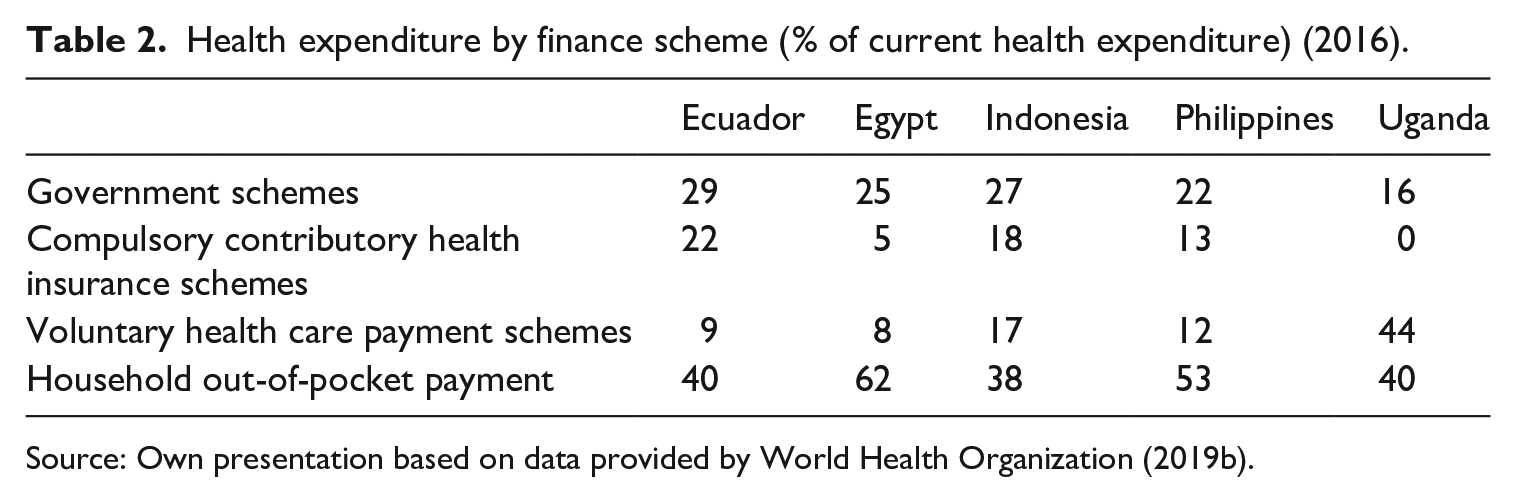
Source: Own presentation based on data provided by World Health Organization (2019b).
In summary, lack of resources and institutional capacity are characteristics of health care systems in the Global South. This diverges considerably from countries of the North. In particular, this chapter has shown that heavy reliance on international actors and segmentation are key features of systems in LMICs. Consequently, we argue that comparative work on health care systems should consider these characteristics. Before we investigate whether existing typologies capture these particularities, the next section discusses different ways of classifying.
Forms of classification
Comparison represents one important basis of social science research: It is useful in understanding phenomena and their particular empirical manifestations as well as in finding regularities (Della Porta, 2010; Ragin, 1987). One approach for facilitating comparative research is the development and application of typologies/classifications. As descriptive and heuristic devices for grouping cases, typologies are useful for concept formation and empirical analysis (Collier et al., 2008; Kluge, 1999). Accordingly, typological research has a strong tradition not only in the study of health care systems but also in welfare (state) research in general (see, for example, Arts and Gelissen, 2010; Powell and Barrientos, 2011) and other branches of social policy (e.g. Barrientos, 2013; Bettio and Plantenga, 2004).
Typologies can be constructed either as unidimensional classifications that rely on one sole category for distinguishing types or as more complex, multi-dimensional frameworks. It has to be noted, however, that even more elaborate classifications result in relatively standardised and strict rosters, which have both benefits and limitations. Researchers may well choose different comparative approaches in studying health care systems which are equally informative and relevant. Nonetheless, in this article, we focus solely on reviewing typologies of health care systems because, first, (influential) classifications can particularly impact further research and policy prescriptions (e.g. Kaasch, 2013; van Kersbergen and Vis, 2015) and, second, a limited scope enables a more in-depth study.
The processes of typology construction and classification of cases are far from uniform. In our review below, we focus on two important differences that classifications of health care systems exhibit: the underlying logic of typology construction and the method of classification. First, we examine underlying logics of classification, shedding light on the question of how classificatory frameworks have been developed. There are two ideal-typical modes of logical reasoning: induction and deduction. In the case of inductive logic, reasoning is based on particular observations of the phenomenon rather than theory. Here, typology development is based on the analysis of empirical data – emerging types are therefore ‘real’. Being rooted in observations, the application of inductive logic makes it more likely to arrive at accurate and empirically relevant types. The very same feature proves problematic, however, as inductively led typologies are very space and time-dependent, making them highly context-specific, which may limit their relevance beyond the included case sample (cf. Freeman and Frisina, 2010; Kluge, 1999). Deductive logic, on the contrary, is based on ‘a set of theoretical propositions’ (Freeman and Frisina, 2010), relying on abstract thinking about how to compare a social phenomenon. Consequently, categories of deductively led typologies are selected based on conceptual and theoretical considerations, a process which may result in types that have no empirical correspondents. For this reason, deductive logic facilitates typologies that are more universally applicable, while it carries the risk of typologies becoming far too abstract to be useful in empirical research (Freeman and Frisina, 2010).
The second criterion employed for reviewing health care system typologies below regards the classification of empirical instances: Which kind of method is used to classify cases? Here, we differentiate broadly between quantitative methods on one hand and qualitative methodological procedures on the other (Collier et al., 2008; Kuckartz, 1999). 3 Quantitative classification may use specific ‘grouping’ methods like cluster and factor analyses, whereas it is also possible to assign cases quantitatively to existing (deductive) typologies by calculating case membership through the use of indicators or indices. A qualitative classification, by contrast, is based rather on case descriptions and relies on non-standardised assignment; this procedure can also exist in conjunction with inductive as well as deductive logic. In the ‘Results’ section, when we turn to discussing extant health care system typologies, we will revisit the benefits and disadvantages of different kinds of typologies outlined in this section.
Methods
In order to analyse the strengths and weaknesses of extant typological approaches for health care systems, we performed a systematic literature review. The review identifies relevant published materials that are concerned with health care system typologies and summarises and assesses aspects of the papers. The search was conducted relying on a clearly defined set of terms and inclusion criteria that allows for reproducibility. As we are interested in synthesising as much evidence as possible, we did not refer to any period of observation in our search strategy, including all relevant literature irrespective of publication date or observation period. Although the searches were conducted in English, the selected databases comprise articles in other languages that contain English abstracts.
We performed the literature review between January and March of 2019, using the search terms ‘healthcare system*’ OR ‘health care system*’, ‘delivery of healthcare’ OR ‘delivery of health care’, ‘healthcare’ OR ‘health care’ in combination with ‘comparison’ or ‘cross-country’, and ‘typolog*’, ‘classification*’, ‘taxonom*’, ‘categor*’, or ‘systematic*’. 4 We searched the following databases: PubMed, Sociological Abstracts, Web of Science, Scopus and OpenGrey. The latter was added to broaden our inclusion criteria to incorporate grey literature (project reports, working papers, policy briefs, etc.), alongside monographs/edited volumes and peer-reviewed literature. We also reviewed articles, conference publications, books and texts mentioned in the reference lists of the papers identified through our review, and publications that we had previous knowledge of even when they were not retrieved during our database search (i.e. studies from unstructured search). The articles selected for review meet three pre-established criteria: They (a) consider health care systems solely, as we excluded studies that classify more than one policy field or welfare states in general; (b) order and group systems even when authors do not use the term typology, adopting different nomenclatures such as model, cluster and pattern; and (c) claim the creation of a new classificatory tool. Regarding the last criterion, it is important to note that our review found countless studies referring to already existing health care system categorisations in order to justify case selection, without, however, aiming at producing new rosters.
Even though systematic literature reviews are more frequent in the field of public health (e.g. epidemiology) than in social policy, using a rigorous means of identifying relevant typological scholarship (a) allows the identification of leading publications; (b) allows replication; and (c) provides a good overview of case selection, concepts, variables and methods (Powell et al., 2020). The method, however, is not without limitations. First, one may argue that the results of systematic literature reviews might mostly encompass research conducted in high-income nations, where publications are indexed to be picked up by search engines. In an effort to include research focusing on or including countries of the Global South, we also conducted unstructured searches in order to minimise bias towards Global North publications. This represents 24% of our data. Second, typologies might be ‘hidden’ in comparative papers on health systems. Often, these are ‘residual’ contributions and are not specified in articles’ abstracts and keywords, hindering the possibility of being retrieved by our search. Unfortunately, these papers are not analysed as they do not explicitly dialogue with the health care systems’ typological scholarship.
Our initial screen resulted in 3005 publications. After excluding duplicates, we arrived at 2551 papers. Most of the publications identified through the search were related to public health research and the evaluation of specific health programmes and diseases (e.g. classification of diseases, clinical studies), rather than analysing health care systems as a whole. Therefore, after a first screening of titles, abstracts and keywords aimed at excluding public health and medical papers, 281 papers were scrutinised. Then, only studies that met our criteria were included in the review. Ultimately, 41 papers were selected for final review; however, this study analyses 42 classifications, 5 as Kam (2012) develops two analytical rosters. The review process is displayed in Figure 1.
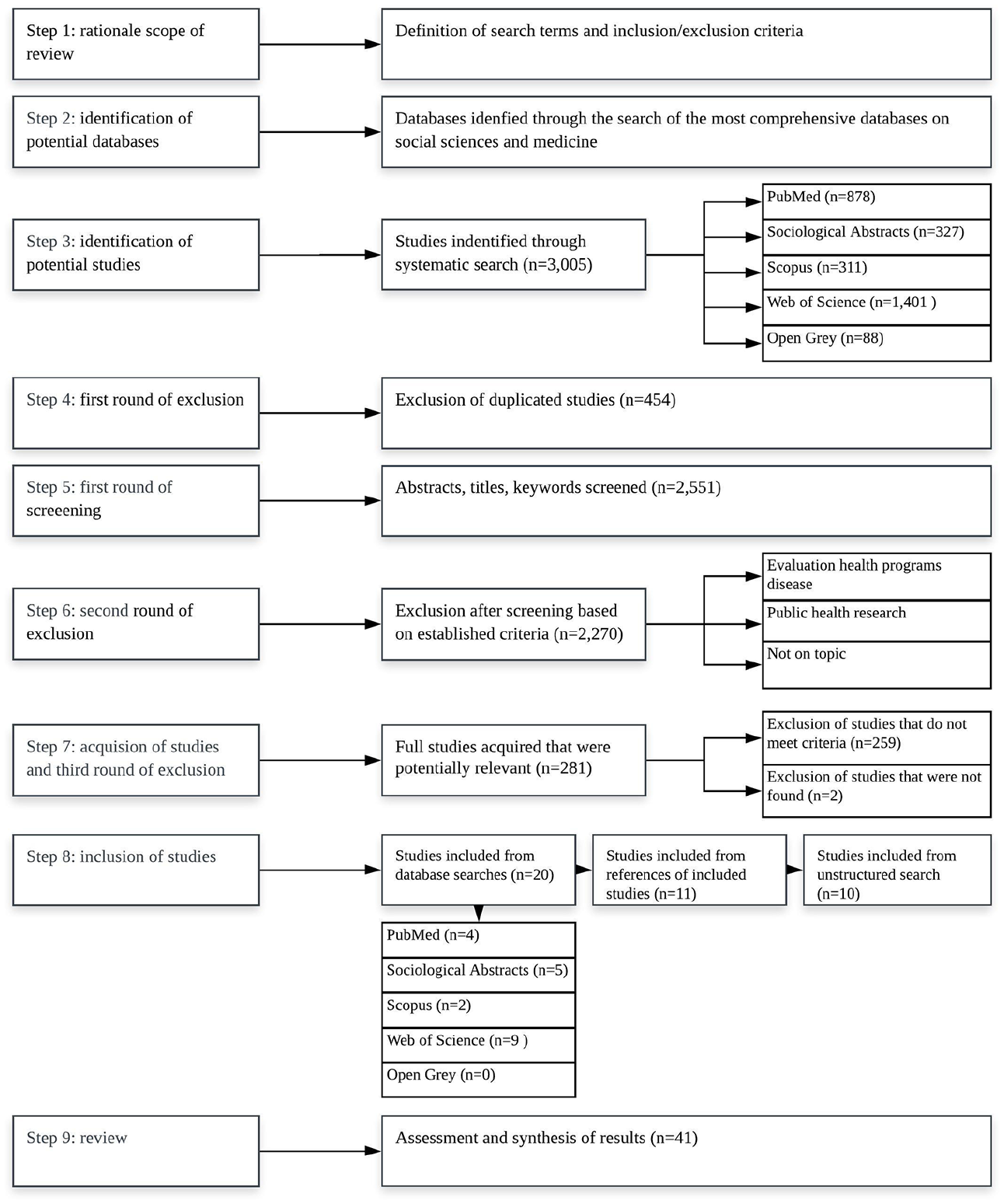
Flow diagram of the review process.
Results
This section presents the results of this study. First, we elaborate on the temporal distribution and regional coverage of the literature on health care system typologies. Second, we summarise typologies according to their logical approach towards classification, as well as in terms of the methods used to differentiate types and unit of analysis. Third, we show the most relevant elements of health care systems identified by respective studies, gathering information on which categories of the health care system researchers use to build a typology.
Temporal and geographical distribution
The first comparative analysis of health care systems our review identified was Roemer’s (1960) ‘world scanning’ of the relationships between public health departments and medical care administration, while the most recent studies were published in 2018. Therefore, we are looking at six decades of efforts at classifying health care systems. Figure 2 displays the exponential evolution in number and temporal distribution of health care system typologies. From 1960 to 1986, our review identified only five typologies (Anderson, 1963; Field, 1973; Maxwell, 1975; Roemer, 1960; Terris, 1978). The Organisation for Economic Co-operation and Development’s (OECD, 1987) systematic classification; the much-improved health databases; as well as Esping-Andersen’s (1990) seminal book, The Three Worlds of Welfare Capitalism, mark the beginning of a new period in the development of health care system typologies, when there is an exponential increase in the number of studies putting forth new systematic classifications. The OECD study on financing and delivery of health care has proved to be one of the most influential studies in the field (Burau and Blank, 2006). In addition, Esping-Andersen’s book created an ‘industry’ of comparative social policy, and still is the main reference to analyse and categorise welfare states and social policies (Danforth, 2014; Powell and Barrientos, 2011). The work, however, neglected service sectors, which makes up the core of health care systems (Moran, 2000; Reibling, 2010), resulting in an independent area of research within welfare state scholarship.
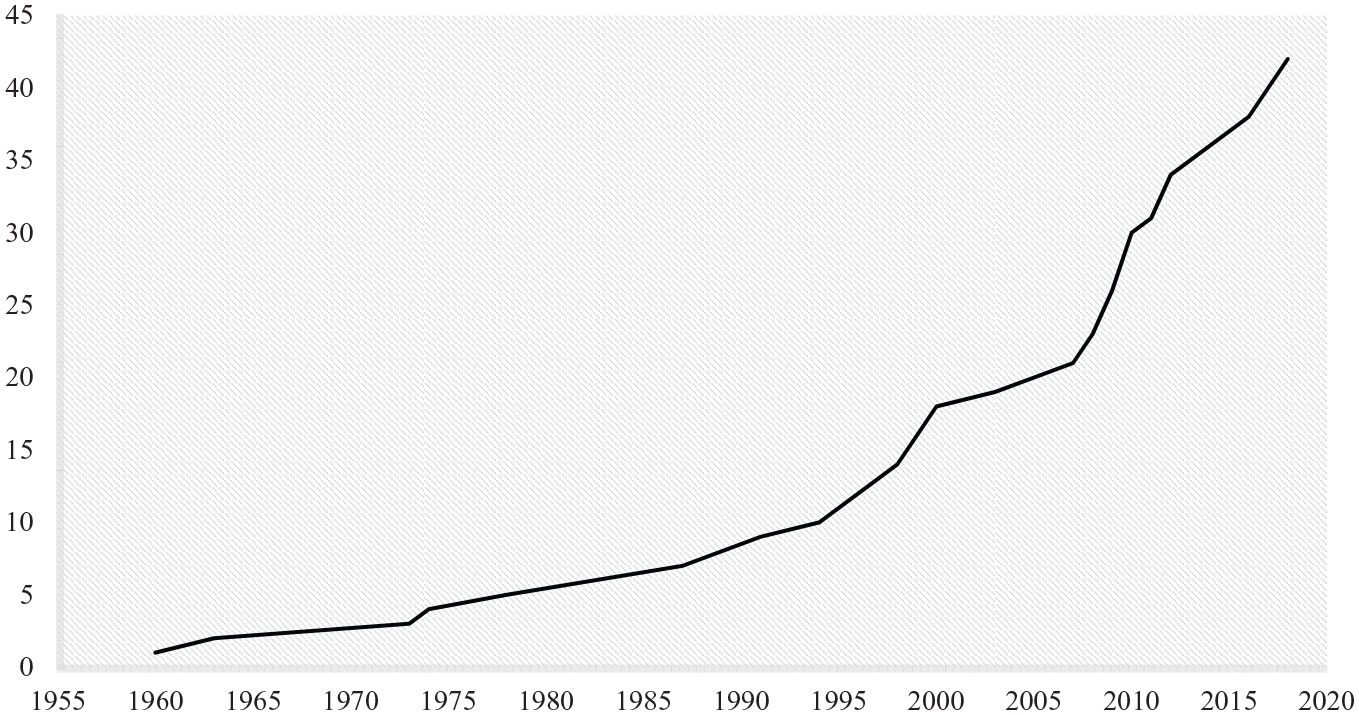
Health care typologies’ exponential evolution in number and temporal distribution.
The number of classified cases ranges from 3 (Anderson, 1963; Tuohy, 1999) to 1172 (Bazzoli et al., 1999). 6 The 42 typologies order, in total, 1828 cases and 103 countries. 7 The 31 countries that appear most often are considered high-income according to the latest World Bank (2019a) classification, with the United Kingdom (34), France (26), Germany (25), Italy (24) and the United States (24) at the top. High-income countries are classified 505 times, while upper-middle-income, lower-middle-income and low-income nations are categorised 67, 27 and 8 times, respectively. 8 Figure 3 shows coverage by region and income group according to the United Nations (2019) and the World Bank (2019a). Extant typologies mostly focus on advanced economies, as 83% of all classified countries belong to high-income regions of the world. Most striking, though, is the lack of any systematic classification of African countries, which account for fewer than 2% of all cases covered. 9
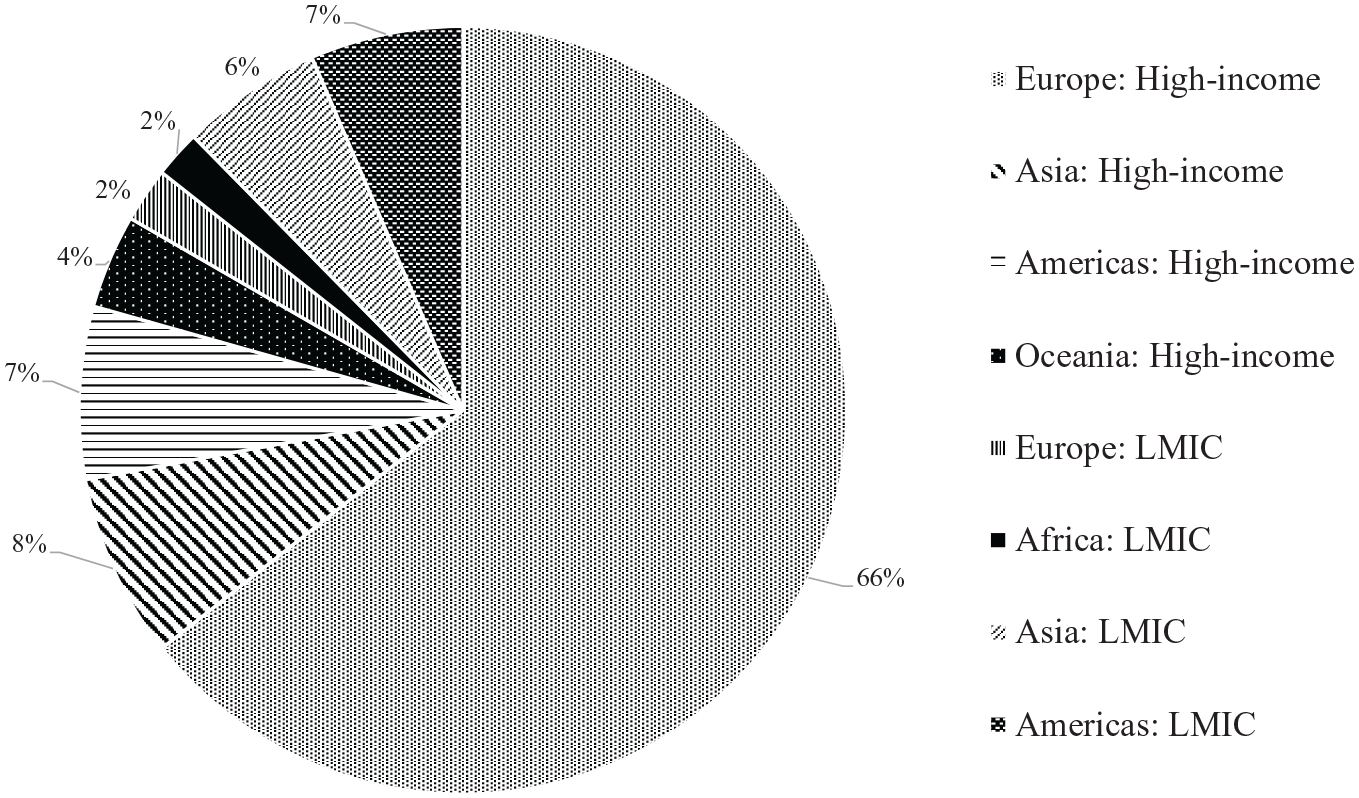
Frequency of covered regions.
Only 12 typologies include Global South countries/regions as cases. Roemer (1960), Field (1973) and Terris (1978) focus on the evaluation of whole continents and regions, rather than individual countries (e.g. Asia, Africa and Latin America). Frenk and Donabedian (1987), Roemer (1991), Elling (1994) and Lassey et al. (1997) cover the most diversified pool of cases, ranging from high-income nations located in North America and Western Europe to under-studied countries like Lebanon, Ghana and Haiti. Furthermore, Mackintosh et al. (2016) classifies private sectors in 11 countries in Asia, Africa and Latin America. Our review also comprises typologies that are limited to specific regions of the Global South: Frenk and Londoño (1997) and Mesa-Lago (2007) target Latin America cases, and Borisova (2011) former communist countries in Central and Eastern Europe and Asia. Sam (2014) includes two upper-middle-income countries (Malaysia and Thailand) into the analysis together with OECD and Asian high-income nations.
Logics of classification, methods and unit of analysis
The reviewed typologies differ with respect to a more deductive or a rather inductive approach to examining health care systems. They also employ different methods to group cases into types and consider distinct units of observation. Figure 4 presents a tentative organisation of the examined studies regarding two main criteria: (a) whether types derive from theory or from observation of real cases and (b) whether clustering of cases depends on qualitative evidence or on the adoption of statistical methods or on the creation of indexes based on quantitative classification. It is important to note that the great majority of these publications, especially the early ones, do not clearly state how the typologies were built. In these cases, the assessment of the adopted approach is our own. Moreover, the dichotomous distinctions employed are not always clear-cut and many approaches rely on an iterative process or mixed approach. In these cases, we assess the typology according to the more prominent logic used by authors.
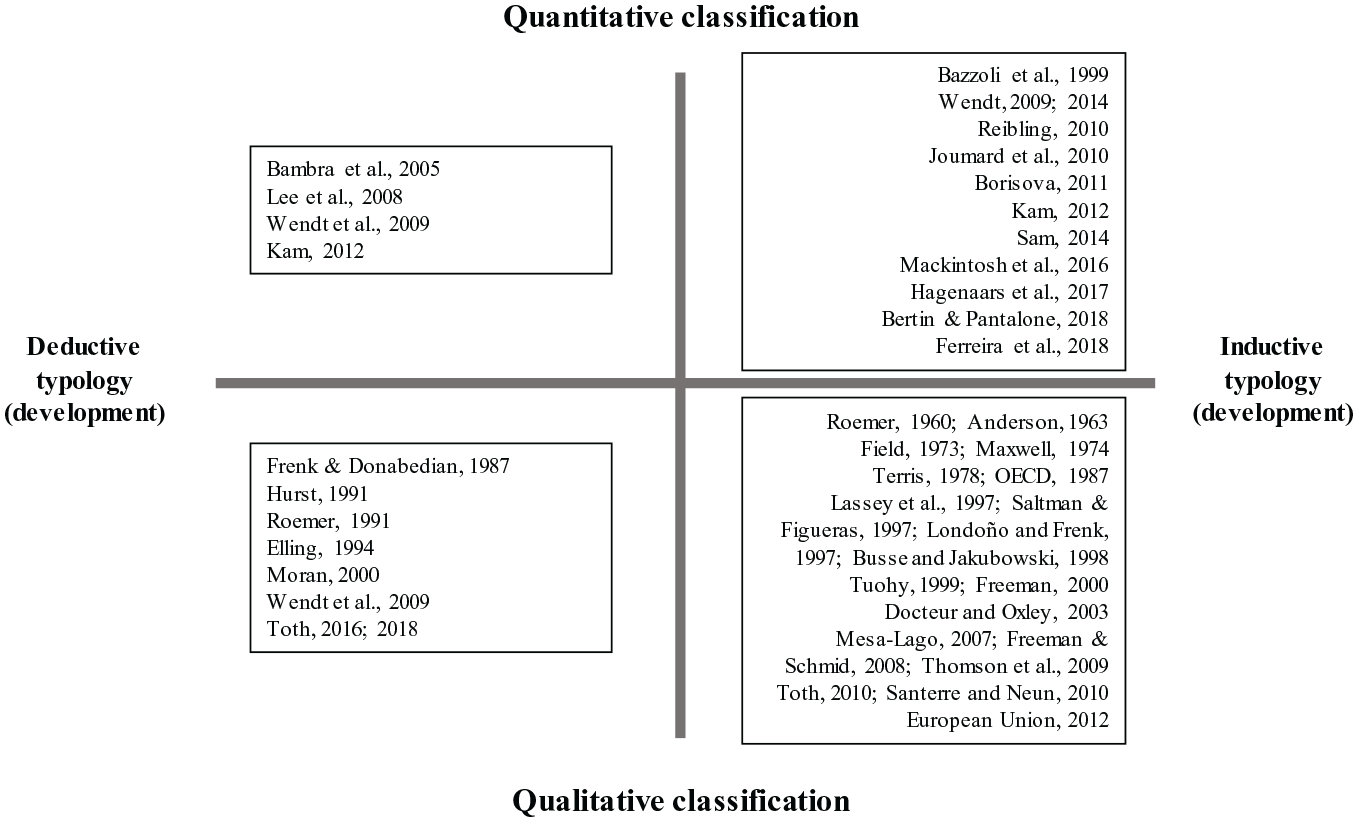
Methodological and theoretical grid for typologies.
Whereas most typologies qualitatively assess types of health care systems (27), 10 advancements in the production of comparative health statistics and an increasing reliance on quantitative indicators measuring institutional features of health care systems have given rise to typologies (16) based on the statistical clustering of cases and the creation of indexes built on quantitative data used in combination with inductive and deductive logics. Most typologies (31) employ an inductive approach to group cases. The typologies (19) shown at the bottom right-hand side of Figure 4 combine an inductive approach to typology construction with classification based on qualitative methods. The 12 classifications sorted into the top right-hand corner are also based on empirics, but the grouping of real cases follows a quantitative analysis and is the result of statistical procedures, mostly through cluster or factor analyses. These methods are necessarily inductive as the resulting clusters are always directly based on the characteristics of the sampled cases. Regarding the typologies considering countries outside of North America, Europe and the OECD world, they mainly adopt qualitative approaches to classification (9), as quantitative comparable data can be limited. Furthermore, 66% of LMICs tools employ an inductive approach to classification, in which types are drawn from empirical observation.
The 11 typologies on the left-hand side of the figure choose a deductive approach: They develop a theory-based grid, which defines potential system types. For example, Frenk and Donabedian (1987) produce a matrix, which differentiates between concentrated and dispersed state control and eligibility based on citizenship, contribution or poverty. Hurst (1991) arrives at six possible types distinguishing the public or private nature of health care coverage and three logics of provider remuneration in public or private systems. In a second step, such a deductively developed typology can then be used to classify real cases, either in a quantitative or qualitative way. The typologies placed in the top left-hand field of the figure provide deductive devices and attempt to quantify differences among types. Bambra (2005), for instance, departs from the decommodification index informed by Esping-Andersen’s work and quantitatively assesses systems.
Regarding the unit of analysis, 81% of the typologies (34) analyse health care systems at the national level. These studies usually classify cases such that whole countries are assigned to one specific type based on the dominant system in place (e.g. Thomson et al., 2009; Wendt et al., 2009). The study conducted by Bertin and Pantalone (2018) observes health care systems at the sub-national level, classifying 20 Italian regions. The earlier typologies of Field (1973), Roemer (1960) and Terris (1978) have both countries and whole continents as units of analysis, as they classify entire regions of Africa, Asia and Latin America and Eastern Europe. Differently, four typologies classify systems instead of countries: Toth (2016) assumes that all health care arrangements are hybrids and proposes putting aside the traditional logic of classifying whole countries. Bazzoli et al. (1999) catalogue different health care systems and networks present in the United States. Mesa-Lago (2007), meanwhile, identifies all systems in place in the country, creating aggregated national types – for example, Colombia is classified as quadripartite as it has four co-existing systems. Finally, Frenk and Donabedian (1987) suggest the most flexible roster in which countries, regions and/or systems can be used as units of observation. Although Mackintosh et al. (2016) and Frenk and Londoño (1997) classify whole countries, they acknowledge the existence of different systems: Mackintosh et al. (2016) classifies countries’ private sectors and their interlinkage with other health care arrangements, and Frenk and Londoño (1997) assign a specific type (segmented model) to indicate the division of distinct social strata into different schemes.
Approach to classification: categories and criteria
The reviewed studies highlight different categories of health care systems. We have thematically identified 14 main patterns used to classify systems, based on the information provided by the authors. Most of the studies refer to provision of services (29), financing (29) and regulation (28). Often, authors combine two or three of these categories, resulting in multi-dimensional typologies (e.g. Hurst, 1991; OECD, 1987; Wendt et al., 2009). Under the financing category, we grouped all themes related to the input of resources into the system (e.g. expenditure, financing schemes). Service provision comprises the elements related to the delivery of health care services, such as human resources, infrastructure and ownership. Finally, all elements that deal with the regulatory and administrative function of the systems were included under the regulation category. Besides regulation, studies use different terms to refer to this function, such as stewardship (Ferreira et al., 2018), governance (Bertin and Pantalone, 2018; Freeman, 2000; Hagenaars et al., 2018) and organisation (Borisova, 2011).
Furthermore, entitlement or eligibility to health care refers to the basis upon which beneficiaries are allowed to access health services. These categories are taken into account in three typologies (Frenk and Donabedian, 1987; Lee et al., 2008; Toth, 2010). In a similar vein, coverage considers the number/share of population covered and appears in the typologies developed by Kam (2012), Santerre and Neun (2010) and Joumard et al. (2010). Studies emphasising the access of patients (Bambra, 2005; Lassey et al., 1997; Reibling, 2010) to providers deal essentially with the regulation of relations between the respective actors, taking into consideration the presence of gatekeeping systems. Technology refers to the use and availability of high-technology medicine and the intense application of skilled labour (Lassey et al., 1997; Moran, 2000). Health outcomes (Ferreira et al., 2018; Sam, 2014) and satisfaction with health services (Toth, 2010) go beyond merely classifying formal arrangements, including information on the implementation of health care. The remaining subcategories (scope of benefits, articulation, class struggle, economic system, economic distribution) appear in just a handful of studies.
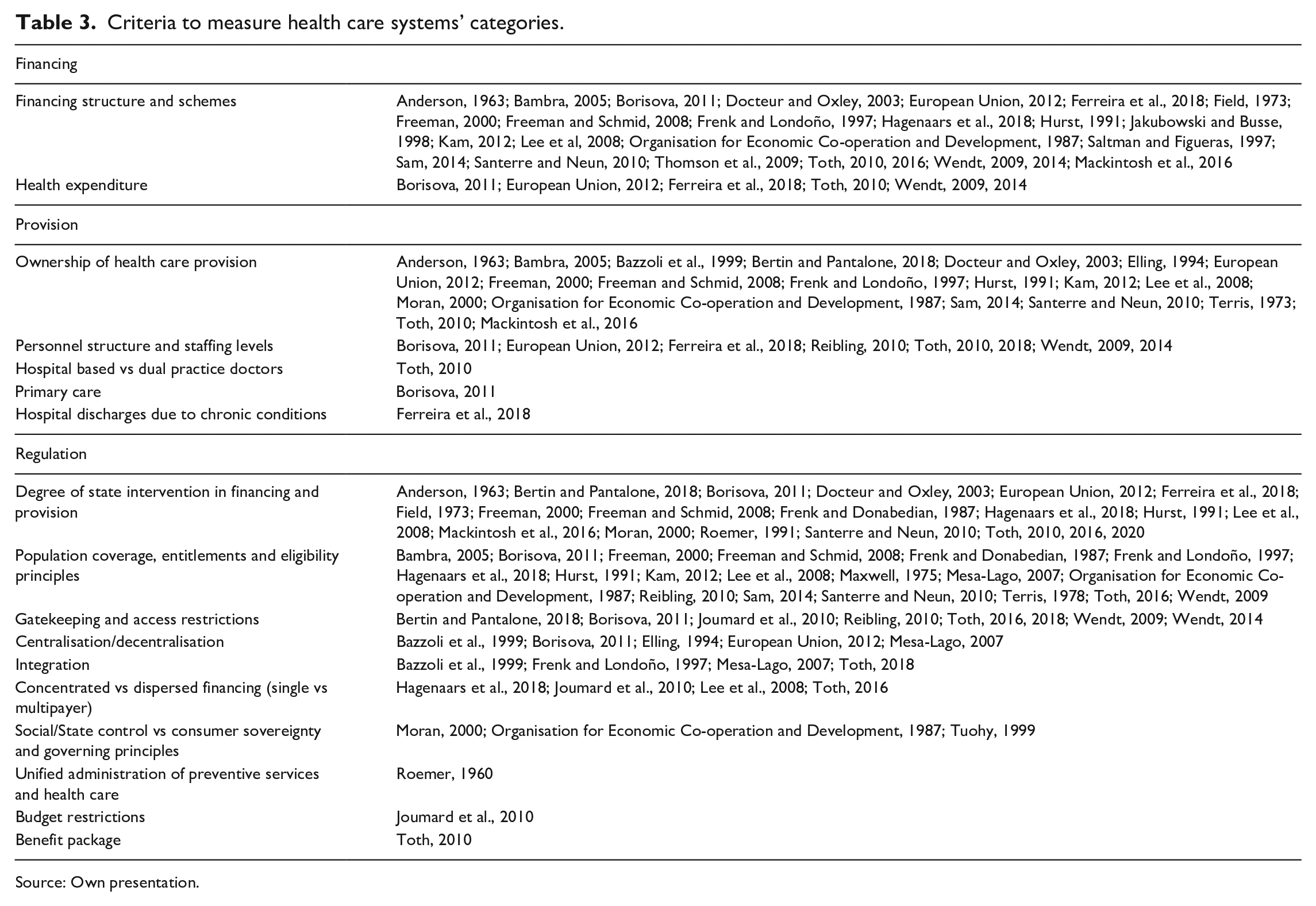
Table 3 presents the different ways by which typological approaches measure the three most used health care categories. To map all the criteria used to operationalise the aforementioned dimensions, we have summarised them thematically, assigning them to one of the main constitutive categories previously discussed: financing, provision and regulation. Although some studies consider basis of entitlement/eligibility, coverage, benefit package and access as separate categories of health care systems, in line with many researchers, we include them here as elements of regulation.
Criteria to measure health care systems’ categories.
Source: Own presentation.
Regarding the financing category, typologies mostly seek to measure the financing mix of systems (25). The main health financing schemes identified are tax financing, social insurance financing, private voluntary insurance and out-of-pocket spending. Besides financing schemes, some typologies (6) include the total level of health spending in order to discern the generosity of systems. Few studies, such as Saltman and Figueras (1997) and Jakubowski and Busse (1998), develop unidimensional typologies based on financing aspects alone. In most typologies, the dominant financing scheme, the public financing share or more detailed indicators of financing are combined with other categories to identify types.
Concerning the provision of services, typologies reveal five different criteria to classify health care systems, although three of them (hospital based vs dual practice doctors, primary care, and hospital discharges due to chronic conditions) are only used in three studies. Therefore, typologies almost exclusively measure service provision in ownership terms (20). The most frequently employed criterion for ownership is the share of hospital beds in public ownership, although some studies also differentiate between for-profit and not-for-profit institutions. Meanwhile, staffing levels and facilities consider the availability of resources involved in the delivery of services (e.g. physician density, number of hospital beds).
Despite the great variety of aspects typologies use to measure regulation, state intervention (20) and basis of entitlement/eligibility and coverage (20) are the most utilised criteria. Degree of state intervention into financing and provision considers the extent of state control over provider autonomy, the extent of control over consumers versus consumer sovereignty, and free choice of providers. Population coverage, entitlements and eligibility principles take into account the segments of the population that have the right to access services. Residence or citizenship-based entitlements characterise national health services systems, national health insurance systems, as well as systems of socialist economies. In insurance systems, entitlements are related to contributions or private insurance premiums.
Whether the administration of the system is centralised at one single governmental level, or shared by central, state and municipal levels is also taken into account (5). In a similar vein, the integration (4) of the systems is measured, which refers to mechanisms adopted to unify the system across all organisational and provision components. Typologies also differentiate between payer type (4): single-payer health care systems, which translate into universal and comprehensive coverage; the payer being a public entity; and multipayer systems, which feature two or more providers responsible for the regulation of coverage (Petrou et al., 2018). Gatekeeping and access control (8) are used to describe potential access restrictions, as they refer to the structure of service provision in the inpatient (specialists vs general practitioners vs nurses) and in the outpatient (focus on primary vs secondary and tertiary care) sectors. The additional five criteria are only considered by a handful of studies.
Taking into consideration only the classifications covering countries of the Global South, they often utilise well-established measurements also common in high-income countries’ classifications. However, scholars dealing with LMICs shed light on some specificities of their cases. While analysing transition countries, Borisova (2011) emphasises the smaller role of primary care in comparison to curative impatient care. Frenk and Londoño (1997) and Mesa-Lago (2007) take into account integration, measuring the extent to which different population groups can access institutions of the health care system and whether functions are assigned to same or different bodies. Interestingly, both typologies only classify Latin American countries. Decentralisation, the transfer of health responsibilities from the central to local governments, is evaluated by Borisova (2011), Elling (1994) and Mesa-Lago (2007).
Do existing health care system typologies reflect the particularilities of the Global South?
Our systematic literature review of existing health care system typologies, the aim of which is to assess their competence to capture the particularities of the Global South, points to limitations in coverage, and methodological and content terms. One of the main observations we draw from this study is that health care systems of the Global South are rarely included in typological work: Only 12 out of 42 typologies include LMICs. The classified cases consist of a 1:5 ratio of Global South to Global North countries, as the latter is grouped 505 times, while the former only 102 times, even though there are 80 high-income economies in the world and 138 LMICs. However, there is still the possibility that typologies focusing on high-income nations are suited for the inclusion of LMICs, or that existing typologies focusing on countries and/or regions of the Global South include relevant characteristics of said systems. Therefore, we now turn to the following questions: Can typologies classifying Global North systems potentially be expanded to include cases from the Global South? Do extant Global South typologies consider all identified important characteristics of health systems in LMICs? That is, can extant classificatory frameworks be used as universal and encompassing instruments of classification?
Regarding methodological limitations, the overreliance on inductive approaches to classification often automatically excludes countries falling outside the perimeters of high-income economies, sweeping aside cases that cannot be properly measured in numeric terms. This is a widespread problem, as 74% of the reviewed typologies are constructed inductively. The bias here not only follows from a general neglect of LMICs in the research, but is also rooted in the issue of data availability: Inductively generated classifications often use OECD health statistics, which focuses on the Global North and has only recently included more data on countries from the South. Internationally comparable data on health systems with a global country sample tend to be restricted to recent years and, for many countries of the Global South, are limited in scope, hampering the analysis of a larger range of arrangements. Mackintosh et al. (2016), for instance, develop a sophisticated tool for analysing Global South nations, but while the study is able to use comparable data for measuring one of its dimensions, the other two rely on non-systematic descriptions. As a result, the use of inductive typologies to classify systems globally may result in poorly informed classifications, particularly when the researcher plans to create a tool for applicability beyond their sample of cases.
As we have demonstrated in ‘Health care systems of the Global South’ section, health care systems of the Global South differ from arrangements of the North both in terms of amounts of resources and the institutional set-up of the systems. In particular, we identified two particularities of systems in the South: the role of international actors and segmentation. Our review shows that typologies in general employ similar criteria for classifying systems, not acknowledging important differences between and within regions. Moreover, the content/criteria used to assign systems to types have not changed much since the first classification was developed in the 1960s. Regarding the presence of international actors, none of the examined typologies account for their role in maintaining and shaping health care systems. Also, none of them quantifies external resources. This is not only true for more proliferate typologies classifying Global North countries, but also for typologies solely covering LMICs. As already discussed, previous literature highlights how sensitive emerging nations are to international pressures and preferences, particularly where dependency on foreign aid is involved. Therefore, the literature neglects an important element of health care systems, as foreign actors are engaged in providing funding, technical training and skilled workers to countries under socioeconomic constraints, and IOs usually play a role in influencing domestic health policies and systems, even if the extent of that role is not always clear (Gomez and Ruger, 2015).
Although a prominent feature of health systems in the Global South, segmentation is explicitly addressed in only six typologies (Bazzoli et al., 1999; Frenk and Donabedian, 1987; Frenk and Londoño, 1997; Mackintosh et al., 2016; Mesa-Lago, 2007; Toth, 2016). Interestingly, four out of these six typologies dealing with the stratification of health services examine LMICs. The rationale of having a dominant system, covering the absolute majority of the population, seen in classifications focusing on high-income economies fails to capture this fundamental aspect of health care systems of the South. This finding is remarkable when taking into account that segmentation, although not as prominent a feature as in emerging economies, can also be found in some wealthy countries, most notably in the United States (see, for example, Marmor, 2010; OECD, 2011). Research taking countries rather than systems as units of analysis assumes that services are equally available to the whole population, disregarding internal segregation in terms of coverage and quality of care.
It can be argued, therefore, that neither reviewed typologies targeting Global North countries nor frameworks focusing on LMICs are fit to compare the analysed particularities of Global South health care systems. Tools cannot be easily extended if important features, such as external actors and segmentation, are neglected conceptually, resulting in the absence of frameworks able to map and compare worldwide systems.
Conclusion
The present study reviewed extant scholarship on health care system typologies to analyse whether existing classifications reflect the particularities of health care systems of the Global South. By examining geographic and temporal scope, approaches and methods of classification, and elements of health care systems, we identified limitations that impede on the ability of current classifications to capture important features of health care systems in the Global South. First, the overwhelming use of inductive logic has led to a preponderance of typologies with strong Global North biases that do a poor job of characterising the empirical reality of the Global South. Second, the limited number of typologies dealing with the Global South results in a lack of a systematic classification of health care systems in emerging nations. Although typologies aimed at classifying countries of the Global South offer important insights into the representation of segmented systems, none of the reviewed typologies takes into consideration the role of international actors.
While these findings confirm our initial hypothesis on the limited coverage and usability of extant health care system typologies, it is worrying both in terms of research and practices. As (well-known) typologies focus mostly on the Global North, it is reasonable to assume that these types and models are more influential in shaping researchers’, policymakers’ and advisers’ images of health care systems and what they (should) look like. This could amplify the ‘invisibility’ of less included countries and regions when considering policy prescriptions and proposals, which are often modelled after ‘high-income, European welfare states’ (Kaasch, 2013). Furthermore, types can often also be (mis)interpreted as portraying ‘best’ models or ‘benchmarks’, which might also lead to (implicit) standard setting for other countries. Finally, research itself tends to revolve around established paradigmatic models, as van Kersbergen and Vis (2015) argue for Esping-Andersen’s (1990) welfare regime typology. Therefore, a focus and reproduction of existing frameworks can hinder novel knowledge production, making it harder to research ‘unfamiliar’ cases or theoretical considerations.
While new typologies that cope better with the diversity of health care systems worldwide would remain idealised reflections of real systems, they can contribute to broadening our understanding of health care systems and to improving analysis tools. Looking ahead, the findings of this article point to the need for new avenues of typological research that incorporate the heterogeneity of health care systems worldwide. This article focuses on the issues of international actors and the issue of segmentation, but other aspects related to health care systems in LMICs found in our review should also be explored (e.g. decentralisation, integration). In addition, health care system typologies scholarship must dialogue with the growing literature on health care systems in LMICs to incorporate the ways in which scholars develop comparative metrics. A more comprehensive typology can serve as a universal framework for comparison, adaptable to the whims of data availability and the choice of quantitative versus qualitative methods.
Supplemental Material
NO_CHANGES_Revision_Appendix_1 – Supplemental material for Classifications of health care systems: Do existing typologies reflect the particularities of the Global South?
Supplemental material, NO_CHANGES_Revision_Appendix_1 for Classifications of health care systems: Do existing typologies reflect the particularities of the Global South? by Gabriela de Carvalho, Achim Schmid and Johanna Fischer in Global Social Policy
Supplemental Material
Revision_Appendix_2 – Supplemental material for Classifications of health care systems: Do existing typologies reflect the particularities of the Global South?
Supplemental material, Revision_Appendix_2 for Classifications of health care systems: Do existing typologies reflect the particularities of the Global South? by Gabriela de Carvalho, Achim Schmid and Johanna Fischer in Global Social Policy
Footnotes
Acknowledgements
We would like to thank Dr Lorraine Frisina Doetter and Kirsten Bergert for their comments on early versions of this research, and Charlotte Grupp for editorial support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Deutsche Forschungsgemeinschaft (DFG, German Research Fundation) – Projektnummer 374666841 – SFB 1342.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.