
Abstract
Summary
Acquired brain injury is a major cause of death and disability. Due to the impact of acquired brain injury on an individual's and a family's functioning, social workers are likely to encounter individuals and families affected by the condition. This study aimed to (1) identify the existing level of knowledge and skills of social workers in working with individuals with acquired brain injury and their families and (2) examine the training needs of social workers to improve their knowledge and skills in working with those with acquired brain injury. A series of semi-structured interviews with newly qualified social workers (six), brain injury specialist social workers (nine), team leaders (two), and commissioners (three) were conducted and analyzed using thematic analysis.
Findings
The data highlighted that social workers in England and Wales have no formal training around acquired brain injury but felt there was a need for different levels of training and guidance for social workers. Participants also discussed the need for better integration with health care and a greater focus on relational working to enact positive change for individuals and families.
Applications
Social work training should be embedded within prequalification training with additional postqualification training where appropriate. Work and training within social work should take an interdisciplinary approach. The authors have taken the data to develop a freely available online training program for social workers.
Introduction
Acquired brain injury (ABI) is a major cause of death and disability across the world. Injuries can be caused by trauma, road traffic accident, assault, and falls or by nontraumatic means, such as viral or bacterial infections, brain hemorrhage or hypoxia/anoxia. In the United Kingdom, there were 359,699 admissions to hospital due to ABI in 2019–2020 (Headway UK, 2023).
The impact of such injuries is varied, and good outcomes are achieved by many, but not all, individuals who have mild brain injuries (Hume et al., 2022; Nelson et al., 2019). For many others, however, and especially those who have more severe injuries, the impact can be profound and enduring, leaving individuals with a panoply of physical, cognitive, emotional, behavioral, and/or sensory difficulties that vary in severity (Ponsford et al., 2014). While some of the long-term outcomes are visible, the often-invisible impairments to memory, planning, reasoning, initiation, impulsivity, and attention can have a significant impact upon the person with ABI, their day-to-day functioning, and their roles and relationships (Holloway, 2014; Sariaslan et al., 2016).
Research evidence points clearly to the impact ABI has on family members (Flores, 2021; Holloway et al., 2019; Muliira et al., 2023; Thøgersen et al., 2022). Families report a high burden of care (Blake, 2008; Holloway & Ellis-Hill, 2022) due to taking on the day-to-day caring responsibilities for their loved ones, be it activities of daily living, or more “project management-type” roles of organizing appointments and calendars, structuring activities, and managing behavior and mood.
Owing to the impacts of ABI, social workers in England and Wales are likely to encounter individuals (adults and children) and families affected by the condition either directly because of the ABI or indirectly because of another presenting issue such as mental health problems. Social workers working with adults and children in England and Wales have varied roles, making use of The Care Act 2014, Mental Capacity Act (MCA) 2005, Mental Health Act 1983, Children and Social Work Act 2017, and other legislation in assessing and managing matters of safeguarding, risk, needs, and eligibility for service provision.
Social workers encounter people with ABI in many different contexts. For those with more severe injuries, for example, social workers may be involved at the point of discharge from hospital or rehabilitation to ensure appropriate social care assessments are carried out to enable access to social care support in a variety of ways. Social workers may also come across individuals with ABI in other areas of their work. Brain injuries are associated with higher rates of mental health difficulties (Howlett et al., 2022), suicidality (Madsen et al., 2018), and drug and alcohol misuse (Weil et al., 2021) and are overrepresented in the criminal justice system (McMillan et al., 2023) and among the homeless population (O’Connor et al., 2022).
There is a current dearth of academic literature in social work focused on individuals and families affected by ABI (Mantell et al., 2018). A systematic review exploring the evidence base examining how social workers work with their clients with brain injury identified 17 articles (Linden et al., 2023). This review noted a shortage of literature regarding ABI and social work practice but identified that social workers were potentially key professionals who could act as a conduit to service provision for individuals with ABI. Unfortunately, the review noted that many in the profession had not received training on ABI and are therefore ill-prepared to undertake assessments and form plans to meet needs.
Considering the paucity of engagement between academic social work and the condition, it is reasonable to question how social workers are trained and supported to learn about its consequences and apply this to their day-to-day practice. Evidence from outside the profession has been critical of the lack of social workers' knowledge of ABI and how this affects functioning and therefore impacts upon the social workers' role and performance (Adshead et al., 2019; Holloway, 2014; Holloway & Fyson, 2016; Moore et al., 2019; Norman, 2016; Norman et al., 2020; Odumuyiwa et al., 2019). In some cases, this lack of knowledge is implicated in the deaths of individuals who may potentially otherwise have lived had social workers and other professionals known more about the condition and its impact (Holloway & Norman, 2022). This contrasts with social work practice that used to take place in the United Kingdom where there were teams of brain injury specialist social workers (Grant, 2023).
A recent study (Bald et al., 2025) looked at the provision of training in brain injury across the United Kingdom. Despite brain injury being the leading cause of death and disability in the United Kingdom (Headway UK, 2023), 71% of social work educators stated that they received no training in brain injury. Social work educators were also asked if brain injury was included in their own taught courses. Sixty percent stated that there was at least one lecture on ABI, but only 27% had a full module on the topic.
The aims of the current interview study were to (1) identify the existing level of knowledge and skills of social workers in working with individuals with ABI and their families and (2) examine the training needs of social workers to improve their knowledge and skills in working with those with brain injury.
Method
Study design
The study employed a qualitative design using online semi-structured interviews with four different groups of social work professionals (see participants below). Data from the interviews were analyzed using reflective thematic analysis (Braun & Clarke, 2006).
Participants and procedure
The study interviewed four groups of social work professionals: six newly qualified social workers, nine social workers with specialist ABI knowledge and many years of practice experience with this client group, two social work team leaders, and three commissioners of social work services, here identified as NQSW, SP, TL, and C.
The study employed a purposive sampling approach with the aim of gathering data from the four separate participant groups. The study was advertised on social media and sent to individuals known to the research team. Targeted populations and individuals were encouraged to cascade details of the study onto other potential participants. If participants were interested, they contacted a member of the research team who provided an information sheet and consent form and arranged an interview to take place online using the video call software platform Zoom lasting approximately 1 hr. All participants received a debrief at the end of the interview. Ethical approval was gained through the University of Essex Human Research Ethics Board with standard ethical principles as outlined by the British Psychological Society (BPS) being employed.
All interviews were recorded using Zoom's in-built recording option and saved to a secure folder accessible only by the research team. The interview was semi-structured and uses open-ended questions that were designed as prompts rather than following a strict interview schedule. Data were then transcribed using Otter.ai and were then edited multiple times to ensure accuracy, before being reviewed by the wider research team. All identifiable information was removed from the transcripts, and to protect the identity of participants, participant codes were applied to each, identifying only the participant group to which individuals belonged.
Analysis
Thematic analysis was used because it provides a flexible approach to qualitative analysis and is widely used for understanding services and training needs (Terry et al., 2017). Analysis was conducted in accordance with the six stages outlined by Braun and Clarke (2006). The first author coded the transcripts initially, familiarizing herself with the data by reading the transcripts multiple times. An inductive process was undertaken to describe and interpret the observations and patterns in the data. Initial codes were refined into themes that were then renamed and organized using Microsoft Word. The first author referred to the original transcripts throughout analysis and often reflected on their position and how it may influence their interpretation of the data.
On completion of the initial analysis, two additional members of the research team (M.H. and C.B.) reviewed the findings against the original transcripts to ensure participants' comments were appropriately reflected and that the results accurately addressed the aims of the study following Guba's (1981) approach to trustworthiness in qualitative data analysis. Further validation checks were employed by discussing findings with members of the research project's experts-by-experience group who provided their own insights into the information provided. Participants were also given the opportunity to comment on the analysis and provide feedback.
Findings
Analysis of the interview data across the four groups of professionals produced seven themes, with associated subthemes (see Figure 1). The main themes were (1) good old-fashioned social work, (2) training needs, (3) experiential/self-directed learning, (4) multifaceted and huge impact of brain injury, (5) fighting the service, (6) integration of health and social care, and (7) advocacy.
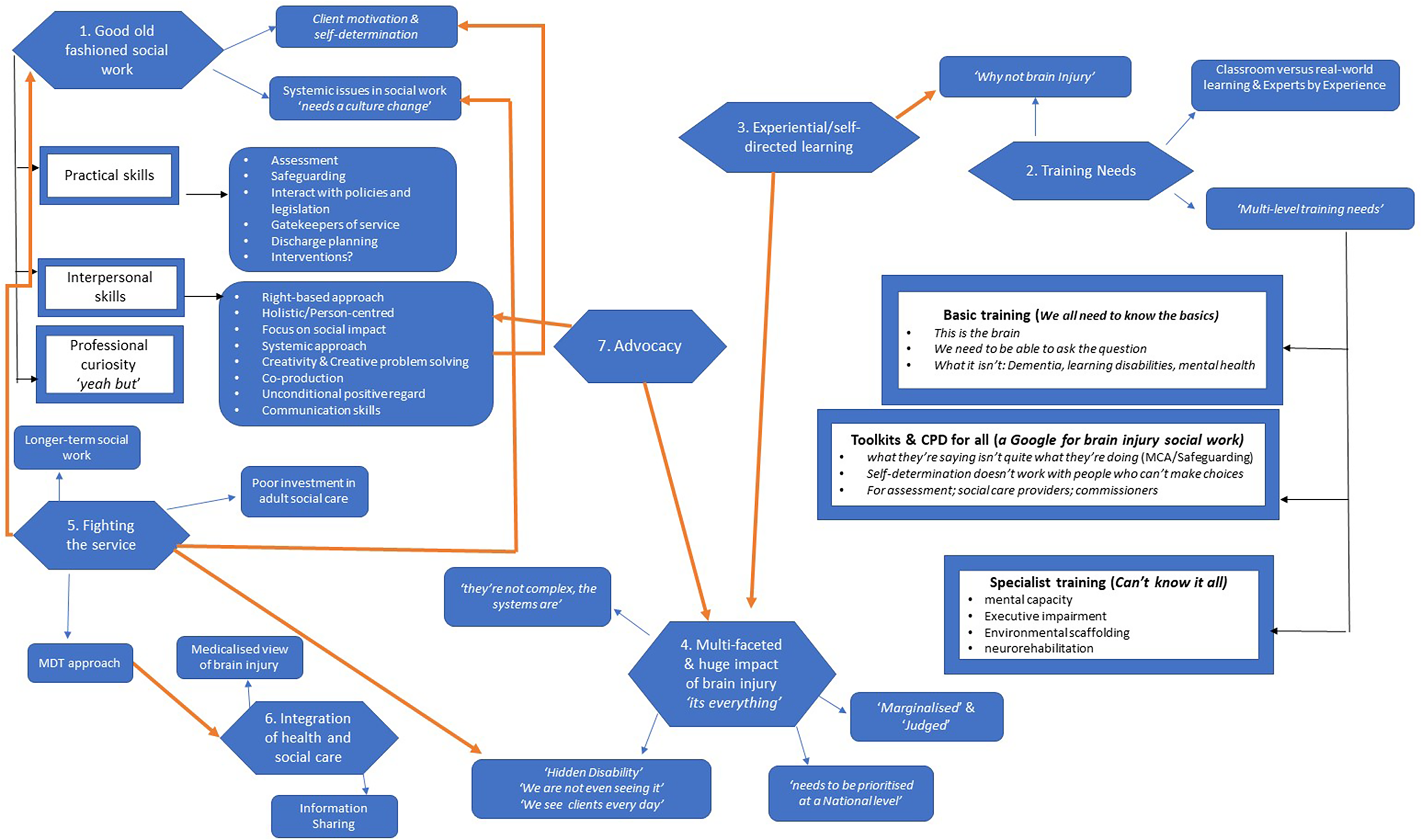
Thematic map of themes and sub-themes.
Theme 1: Good old-fashioned social work
The professionals in all four groups (commissioners, specialist social workers, team leaders, and newly qualified social workers) all discussed the role of the social worker more generally and how it might apply to ABI. Specifically, specialist social workers discussed a need for the social care system to return to the principles of good old-fashioned social work (a return to the basic interpersonal and practical skills, along with professional curiosity, that sit at the heart of social work practice). Experienced professionals talked about social work being about a form of case management, integrating information from a range of professionals, helping to support a care plan, and overseeing a process of neurorehabilitation in a holistic, person-centered manner. The participants saw themselves as gatekeepers (e.g., providing referrals to other services) to social care services for clients. …it's an ability to kind of hold complex and nuanced ideas about people, and to keep all of those moving parts in mind, as you try to deliver a service that's meaningful to the person and also have an overview and make sure that you're headed somewhere you know, where you're headed. ( in adults we don't necessarily look at somebody's diagnosis. (
Subtheme 1a: practical skills
“I love doing things, rolling my sleeves up and getting dirty”
Practical social work skills were identified as including assessments for clients and their carers/family members, safeguarding, interacting with policies and legislation to offer legally informed support to individuals, acting as gatekeepers to services and discharge planning. …it's really kind of focused on … promoting their human rights and trying to support people to make their own decisions … my focus is as a BIA [best interest assessor] social worker is strongly aligned with, you know, the promotion of human rights, basically. ( We are gatekeepers to services. We need to understand what someone's needs are and engage with the right services for support. (
One of the more contentious points that arose from the interviews was the concept of social work as an intervention. The more experienced social work participants felt that they used to view themselves as part of an intervention but that modern-day social work was more about referral to other services. Sometimes they just need you to listen, to be there, to sit with them. To sit with families, show you understand and that you care. ( I think we sometimes forget to think of ourselves as an intervention … we focus on referring to services or engaging services and forget what we as social workers can do. (
Subtheme 1b: interpersonal skills
“It's that overall ability to build a relationship with the whole family”
Participants believed that a large part of social work involved effective interpersonal skills. This was linked to a strong focus on holistic/person-centered ways of working, a rights-based approach, and the social impact of someone's disability. We look at things holistically the training has made us … It's just now they just need to make sure that brain injury is also added to it. ( I'm all about kind of human rights and least restrictive, you know, principles and trying to support … people to make their own decisions. (
Participants also highlighted that successful social work focused on systemic ways of working, looking at people within the context of their environment and social network and not working with clients in isolation. It was felt that where family was present and did not pose a safeguarding risk, they should be included in the social work process, although this often was not the case. We need to work with the whole family … I have a client living in a flat away from his wife because he can’t climb the stairs to their first floor flat. ( The families are broken, they don’t know where to go for support. (
Participants talked passionately about the skill of social workers being creative in organizing solutions to problems and working with clients in the spirit of coproduction. These skills require good communication skills and a process of unconditional positive regard for clients, which all relate to social work as a form of intervention. My interpersonal skills, my questioning skills, my empathy, being empathetic to whatever situation my client is in. So it brings out all those things you learn in school, then you have to use them. ( I think when you see social work at its best. And I have seen and worked with a lot of very good social workers, they are very creative. (
Subtheme 1c: professional curiosity
“They don’t always tell you what their needs are … it is up to us to use our professional curiosity to find out”
Professional curiosity is a term used within the context of social work to describe the natural inquisitiveness that professionals should demonstrate. This may be trying to “see the world through their [the client's] lens” or being thorough in a professional's approach to information gathering and asking tough questions about the way processes and procedures are being employed in daily practice. The culture needs to be of curiosity, competence, thoroughness, exploration, analysis, reflection, all the kinds of things that you know, social work kind of values and the principles of it. ( I teach my students to ask the difficult questions, play dumb … someone says something, challenge it, the “yeah but” questions … Yeah but is that how it's supposed to be, is that what the system says? Why do you do it like that? (
Subtheme 1d: systemic skills in social work
“I get quite embarrassed to say that I’m a social worker”
While talking about the ideals of good old-fashioned social work, participants noted some of the difficulties of working within the current context. These were generally linked to the problems outlined in Theme 5 (fighting the service; see below).
Subtheme 1e: Client motivation and self-determination
“The MCA is a balance between protectionism and empowerment. This is possible to achieve only if you have a good knowledge of how disability impacts someone”
Participants noted potential for conflict between a rights-based approach to working and supporting people with ABI who may have little, or limited, awareness of the extent of their own disabilities. The participants with greater knowledge and experience of working with clients with ABI identified that modern social work is predicated on client motivation and self-determination, meaning that clients should want to be involved or engaged with services and it is important to ensure they have the right to choose. While in many circumstances, this is an admirable goal, when working with individuals who may struggle with awareness about their difficulties, such an approach can lead to them not being able to gain access to much-needed services. Furthermore, in the case of individuals with executive impairments, they may be unable to initiate tasks that may be wrongly perceived as a lack of motivation. I think sometimes there is that … tendency for … social workers … to kind of use that blanket kind of approach … if they have capacity … it's their choice, we don't need to get involved, we, you know, almost as a, as a reason to not provide services or not pursue, you know, that person to support them or, you know, safeguard them. ( Our drug and alcohol services won’t take referrals from the neuro team, they won’t take referrals from us. Clients have to self-refer … That's fine but what if the client doesn’t have the ability to make that self-referral? They place too much emphasis on motivation and self-determination. They don’t understand the problem with that for someone with brain injury. (
Theme 2: training needs
“We have training, but we don't have enough training focused on brain injury at all”
All participants identified a dearth of training in ABI at the prequalification level. Participants expressed a need to know about the range of impacts of ABI and how they impact an individual and the social workers’ ability to effectively work with them. …if you ignore the effects of the brain injury, if you don't even know about what it might mean, being impulsive, doesn't mean you just bought a bar of chocolate on your way home from work. It's different. And if you don't learn about those things, then you are not promoting the person's rights because you’re either leaving them completely at sea, or you are over protecting them, you know, and if the MCA is all about the balance of empowerment and protection, then the way you get the balance between empowerment and protection where the person has had a brain injury is by knowing the most you can about that brain injury for them. (
Subtheme 2a: classroom versus real-world learning
“We need more real-world examples, be it videos etc”
While participants appreciated the need for theoretical knowledge that was classroom based, many identified a need for more practical teaching that allowed them to understand how social work was carried out in the real world and how best to work with client groups. This was highlighted as being particularly important when considering clients with complex needs. Some of the newly qualified social work participants noted that they had felt unprepared for some of their encounters with clients on starting in practice. it's just a huge amount of training. And I think probably a part of that is kind of classroom … theory, a lot of it is just it needs to be done with people. ( I wasn't prepared for that I wasn't prepared to go into those homes and see those things. No amount of training will prepare you for seeing those things physically. So, and then you start building your resilience, because you don't learn resilience building classroom, you have to actually do the job to be able to become resilient. (
Subtheme 2b: why not brain injury?
“Why isn’t it included? We do mental health, dementia, learning disabilities, why wouldn’t you teach about brain injury”
Participants questioned why ABI was not included in the prequalification syllabus. Those who were more experienced identified it as being an important area due to the numbers of individuals with ABI, while those with less experience were surprised by the extent of the figures and wondered why this did not make it a vital component of basic training. I've had various training in mental capacity, safeguarding, mental health, alcohol training, but not directly focused on brain injury, how it impacts all the people and how social workers can work with adults … when you're talking about capacity and things like that, or not having, I've not heard it specifically like it. ( … there are so many people with a brain injury, there are so many people that may have had a mild brain injury that might have not even gone through the system. And I think if you've got a social worker that's got even a little bit of knowledge, then that, you know, might just trigger something … that what they're saying doesn't quite add up with what they're doing. Or I remember that training that I did …. (
Subtheme 2c: multilevel training needs
When discussing their understanding of ABI, all participants provided perspectives on the types of information and level of training they felt would be appropriate in ABI for social workers. Participants stated that they found exposure to the stories of those with lived experience helped to cement learning by placing the issues in the context of the individual and their family. I would love to see lots of shared experiences from people who have, you know, had a stroke, gone through a care pathway, got the right help. ( I have learnt so much from listening to the stories of my clients. (
Most participants felt that there needed to be a basic level of knowledge included within prequalification training with growing complexity of information presented at later time points. Generally, participants felt that all trainee social workers should be given basic information about the brain and what brain injury is, how it affects people, and how it differs to other conditions such as mental health difficulties and learning disabilities. I believe strongly that to be a good generic social worker you need at least some knowledge in all areas. ( … a lot needs to be done in schools and the university curriculum needs to change, we need to add more self neglect, we need to add more brain injury, we need to look at how brain injury impacts or how some people brain injury, self neglect. (
Many of the participants also highlighted the need for further information about ABI provided to social workers through Continuing Professional Development (CPD). Aspects that were viewed as being important within this context included how executive impairment impacts mental capacity (e.g., the frontal lobe paradox; George & Gilbert, 2018), the difficulties of relying on self-determination, and how ABI should be factored into assessments. It would be around very much understanding the numbers, understanding what impact that will have on us as a local authority … what services we need now and into the future to be developed to meet the needs of this population. ( Some people … just assume that somebody with a brain injury is making … an unwise decision, because that's what the MCA kind of teaches you. But, you know, it's about having that knowledge that it doesn't quite apply in the same way when you're presented with someone with brain injury …. (
Many of the participants felt that the level of knowledge and understanding required when working with a vast array of such complex needs meant that there was a need to return to a specialist model of brain injury social work. Others expressed concerns with specialist models of practice as this may lead to social workers in local areas being unable to recognize and meet the needs of their clients. Additional concerns arose around specialist knowledge being lost from services where insufficient resources were made available to ensure new professionals gained opportunities to undertake specialist training. Therefore, most participants agreed that there needed to be a breadth of knowledge about ABI among all social workers but that it would be useful to also have more highly trained professionals that could be referred to in the case of clients with complex situations and needs. We all need some knowledge, but we need to be able to go to someone who is an expert when we reach the limits of our understanding. ( We have social workers specialize in mental health … in different aspects of vulnerabilities … it would be appropriate to have a brain injury social worker, specialized in, in that sort of support …. (
Theme 3: experiential/self-directed learning
Participants were asked about their own experiences of ABI training during prequalification and postqualification courses. None of the participants identified having had brain-injury-specific training, with very few even having had a single lecture on the topic. Even the specialist social workers identified that their specialist knowledge had been self-taught out of necessity when presented with a client with ABI. I didn't feel like I had enough knowledge when I was confronted with a case of someone who had brain injury. And so that, that, obviously, that made me take it upon myself to, you know, to do my own research. ( They said he had learning disabilities but I started to think, well hang on. I did my research and realised it was brain injury and he had been in a learning disabilities team all these years. ( I had to do my research … go online, do the research to see what limitation so that I know what kind of support I needed to put in place … What is the boundary? What can they do? How does this affect the day-to-day life? And yes, I had to do that myself. (
Theme 4: multifaceted and huge impact of brain injury
The participants in this study discussed the wide-reaching impact that ABI can have on a person's life and on the lives of their family. They talked about the different presentations of brain injury in individuals and the hidden nature of cognitive impairments, particularly executive dysfunction. Participants with greater knowledge of ABI identified them as lifelong, life-limiting injuries that impact every aspect of people's daily lives. …it's everything. And the more you get to the more you work within it, the more you realize how you take for granted how much the brain is doing in a given moment to keep us you know, comfortable and sorted and knowing what we're doing…. ( There are so many, accidents, falls, sports, concussions, women who have been hit, thrown against walls, strangled. They don’t all come straight from hospital. We see them in our mental health teams, in domestic abuse services, in substance use services, learning disability, even dementia services. (
Subtheme 4a: Hidden disability
While the impact of ABI was seen as complex and multifaceted, one of the key features noted by many participants was the often-hidden nature of cognitive impairments. Participants noted the complexities that a hidden disability of this nature presented during assessment of needs and risk. A particular focus was placed upon executive impairment that can lead to difficulties with idea generation, planning, problem-solving, and decision-making and can impact people's insight into their disability. Participants noted that this lack of insight can lead to individuals stating that they are independently capable of performing certain tasks, when they are in fact unable to do so in reality. It's also about justice … It's hidden and it's scapegoated … we’re missing it. We don't understand it. We don't know what to do with it. We're not even seeing it in the first place to legitimize it. ( I say this a lot to people … look, if they were in a wheelchair, if they've got a spinal cord injury, you wouldn't expect them to walk a flight of stairs. So why are you expecting somebody with a cognitive impairment to process this information in the way that you're giving it to them? (
Subtheme 4b: The system 's full of barriers that makes it complex
Individuals with ABI were identified by many participants as having complex needs in that they often required support from multiple services for their injury, mental health issues, and drug or alcohol problems. While the complexity of these individuals posed a challenge for the professionals working with them, many of the participants identified that a larger difficulty was the way in which health and social care services are set up that prevents groups of professionals from providing holistic support and care to individuals. A lack of information sharing across or between organizations meant that multiple complex needs were rarely met. Social workers are good at rehabilitation, Mrs. Smith's broken a leg, she's going to improve over the next few days. This [brain injury rehabilitation], it's not rehabilitation … there needs to be a word for it … it's not that X is going to improve back to how they were before and then you just say goodbye. They're going to improve to be different. Yep. But but equally and differently able. ( The nursing home won't have had the right level of tools and support in terms of understanding the full constraints … as a result of their injury. We have the cognitive side of it … I think that's a hidden side of the response that we probably need to focus on. (
Subtheme 4c: Marginalized and judged
Some of the participants discussed individuals with ABI regularly falling through the gaps in services. Their complexity and the often-challenging behavior they display can lead to them being wrongly labeled as “refusing to engage with support” or being abusive. Participants noted that this can lead to individuals being judged by professionals and marginalized by the services that are meant to protect and support them. …they aren't diagnosed with brain injury … there's often … those comorbidities in terms of alcohol use. And it's implied, I suppose that that's, again, that's a lifestyle choice that they're choosing to live … like that. ( We picked up on patterns … there's more to it than unwise decision making or lifestyle choice. This person's got a bit of a poorly brain somewhere, they're not able to control their emotions and their impulse control, they're not able to hold information in mind and use it, they've got no idea about how they're doing in the moment, they're not initiating tasks. ( We misunderstand anger as a response … we avoid it or shut it down … Anger is an expression of unmet need … why are they angry? (
Subtheme 4d: ABI needs to be prioritized at a national level
The participants in this study either currently worked for local authority adult social care services or had done so in the past. Participants identified difficulties within local social care systems that meant that ABI was often overlooked by commissioners. However, a larger challenge noted by participants was the failure to recognize the number of cases of ABI at a national policy-making level. Local commissioner participants highlighted that they often look to national strategies to help them decide how to allocate funds for local services. The absence of ABI as a national priority has therefore, in their opinion, led to an absence of local services within both the National Health Service (NHS) and social care. …the national priorities … when you think about sort of brain injury … if you look at the … intermediate care pathways … for people out of hospital. What is needed to enable … people with an acquired brain injury to be supported in the most proper way? They are most probably the most complex people. ( This is one of the of the data [numbers of cases of ABI in the United Kingdom] that needs to be kind of highlighted, especially at a senior management level, so they could be an understanding of what it's about and how it can be seen as part of something else. (
Theme 5: Fighting the service
Among all the participants, there was a clear sense of frustration with current systems in social care. More experienced social workers lamented the comprehensive changes to systems over the years that they perceived to have resulted in shorter time allocations for assessments, less contact time with clients and families, and a move away from offering direct support and intervention and returning to what participants referred to as good old-fashioned social work. Newly qualified social workers also expressed similar concerns, feeling that the system in which they were working did not reflect the model they had felt they were signing up to during training. Even commissioners expressed concerns that the systems were not always fit for purpose and were set up in a way that often undermined people's access to care rather than supporting it. I've been in situations like that, where I've had to sit in front of a whole team of people saying, when does this stop? When do you start listening to us? Do we have to get into a serious case review before anybody listens to me? ( …the challenge that I have encountered is mostly around the fact that I'm making threshold decisions over the phone. And most of the time … have never seen the families. (
Subtheme 5a: Long-term social work
More experienced social work participants recalled previous structures that allowed them to work with clients long term, enabling them to build strong professional and trusting relationships with them and their families and to learn about their functioning. In the modern workplace, social work systems, short-term working, closing of cases where people are still accessing care services, and high turnover of staff no longer allow for this model of long-term working. This can result in individuals with ABI and their families’ expressing frustrations at having to repeatedly tell their stories and be reassessed by various social workers rather than having any sense of continuity of care. my old colleagues, what they describe to me now is not what I tried to do … It's a box ticking exercise a lot of the time … when I was in social services, you know, we were able to keep cases open long-term. So you built that relationship …. But now, that's not the case. You know, it's a constant sort of throughput…. ( People need long term support. It doesn’t end when they leave hospital, or 6 month or 12 months down the line. When you have a brain injury, you need lifelong care. (
Subtheme 5b: Poor investment in adult social care
While participants identified many shortcomings in the current social care system that had led to perceived poorer working practices and outcomes for clients, a lack of investment in adult social care generally was seen as one of the most significant factors impacting service provision. …ultimately, they're taking what we decide back to a manager who may or may not know anything about this and is responsible for a budget and probably just gets told no. ( They [commissioners] don't know what to specify in commissioning briefs and contracts. Hence, you can find service providers cashing in on this, charging very large sums of money for services…. Then commissioners try to push this back on NHS funding for those services…. But for ongoing funding, you will have people who have brain injuries which means that they are going to require a lot of support for the lots of years to come. ( We’re always the poor cousin. The money goes to children's services and adult services are overlooked, forgotten, expected to cope with what little we have, and it is very little. (
As noted by participants, one of the consequences of the lack of investment in adult social care was a shortage of staffing that led to greater time pressures and resulted in social workers in the adult sector being incredibly time poor. This also led to high levels of stress and overwork in local authorities, resulting in staff burnout and exacerbated staff turnover rates. We would love to provide more long-term work but the resources aren’t there. We don’t have time, people leave the role, continuity is really hard…. We would need an increase in staffing of at least 50% nationally to be able to offer long-term social work. ( …the volume of referrals that come through … it's something to reflect on … when you're dealing with a complex situation … a social worker in my team can get allocated six referrals to screen within a work day … Think about the fact that you're … writing a mini assessment … that would determine or justify your decision in terms of the threshold … it basically means that you have an hour or less than two hours…. So sometimes you're making decisions based on very limited information. (
Subtheme 5c: Multidisciplinary team (MDT) approach
The participants with good knowledge and understanding of ABI discussed the “silo” in which social workers often find themselves working. All specialist brain injury social workers drew attention to the need for MDT working to truly understand the impact of ABI on individuals and their families and to understand the importance of neurorehabilitation. Without this approach to working, social workers were left “in the dark” about how to support the needs of people with ABI, and healthcare professionals were left frustrated by the lack of support from social care to people with ABI after leaving the hospital. Participants highlighted the biopsychosocial nature of ABI and how this lends itself to an MDT approach where all professionals work together to meet the needs of the individual and their families. Its realising that that you don’t need to know everything … about brain injury. If you work with medics, physios, OTs, they focus on the bits they know and then we can come in and … think “ok so how does that impact on someone's…social lives, ability to live a life outside of hospital.” ( the NHS, medical model, working with them … I see it as a positive in terms of providing the adequate and holistic support for my client … we are all sitting around the table, we are all discussing about the cases … all of them bringing the expertise in, and that's really helpful in terms of providing that holistic support. (
Theme 6: Integration of health and social care
Closely linked with the subtheme of MDT working was the concept of integrative health and social care teams. Participants identified that as a biopsychosocial condition, ABI clients and their families were better served by organizations that coordinated and managed health and social care packages in an integrative way. This was particularly noted in the case of budgets. Many of the participants felt an integrated approach would reduce the problem of decisions around funding and increase the ease with which MDT working could be achieved. Within adult services, we need better connections about health conditions and what that means in terms of developing policies, developing service specifications, which are meaningful to practitioners, you know, so they have clear guidance about what they should be operationally commissioning. And there should be a dialogue around structures in place to bring that together. ( I’ve been in meetings when they [NHS teams] literally say “k-ching” that's your money, we don’t need to pay for that. It shouldn’t be like that, we need to work together to provide the right care for others, not fight over whose budget it comes out of … There's a real sense of an us and them culture with health. (
Subtheme 6a: Medicalized view of brain injury
Another benefit to a more integrative model of health and social care was seen as a move away from viewing certain conditions through either a purely health or social lens. Many conditions, including ABI, commence as medical conditions that then have psychological and social consequences for individuals. Therefore, viewing ABI from a purely biomedical perspective is unlikely to support the needs of people living with the condition or support their families. Social workers are in a unique position to work with healthcare professionals to bring a more nuanced social perspective to ABI and the impact it has on daily life. They [NHS team] bring us in with a few days to go … this person is coming out of hospital … all they see is they are medically fit to leave. But what about their housing, their benefits, their family? ( We've been late in the day really understanding that our intermediate care services need to be much more flexible, and offer a whole range of different routes out of hospital … how do we make that journey for someone … more person-centred. ( …brain injury, maybe people look at it as it has to be something that that is … managed by medication alone … looking at the medical model, really concentrating on that, and not the social aspect of support for people that has brain injury. (
Subtheme 6b: Information sharing
An issue raised by many of the commissioners and specialist social workers was a lack of information sharing across different organizations that often led to failures in providing suitable care. The integration of health and social care systems was viewed as a possible way of improving information sharing, especially during discharge planning; accessing social care services after discharge; and assessing risk and support needs. …the problem is that the local authority because they think that physical health, all of them are the same, they wait and keep waiting … until it's three days to discharge because they … still thought that everybody's [physically] disabled and the care is the same for everyone. ( They [NHS team] bring us in with a few days to go … this person is coming out of hospital. We need more time than that to plan, assess, make sure they are discharged safely, to a place of safety. We need more time, there needs to be a discharge plan in place before they leave hospital. (
Theme 7: Advocacy
The newly qualified social workers in the study noted that due to the difficulties inherent in current social work systems and the hidden nature of ABI, there was a need for better advocacy for individuals. This was seen as being something that involved social workers as advocates, employing external advocacy organizations to support with assessments or involving family or friends in the assessment process. Interestingly, advocacy was not directly discussed by specialist social workers. However, throughout the interviews, these professionals noted the importance of family within the ABI context and how their inclusion was fundamental to understanding and assessing the needs of people with ABI. I also find it challenging that we had to go and if you like, advocate for the people we support before the management of the local authority for us to be able to actually support them. ( Luckily, he [client] had a friend that could tell me what his history was, for my practice going forward with him, I had to now look at the fact that he has a brain injury and not dementia, as the carers thought. (
Discussion
The findings of this study demonstrate that social workers feel there is a need for training around brain injury that covers basic biological information as well as more complex information about the interplay between biological, psychological, and social factors that make supporting individuals with brain injuries complex but vital to achieve. The experienced professionals in our study identified that they had not received any formal training around ABI and that their knowledge had been garnered through self-directed study and professional curiosity when confronted by individuals with ABI. While there was some discrepancy in the views of the different participant groups within the study (e.g., specialist social workers understandably had a greater insight into training content and were able to provide more deeper reflections on the issues with working with clients in practice), all participants drew broadly similar conclusions about the need for access to training and concerns about the need for advocacy, better MDT working, and better systemic practices.
The participants in this study felt that ABI training should be a fundamental part of both prequalification and postqualification training to address the complex issues faced by clients and their family members. Participants noted the invisible nature of ABI that leads to issues being missed without training and that leaves people marginalized and judged if they do not have appropriate advocacy and support.
Finally, our participants highlighted some of the structural and organizational issues that are impeding changes to social care delivery, namely, a lack of longer-term, systemic working; a lack of integration with healthcare services and professionals; and artificial budgetary boundaries. This possibly reflects a shift in social work practice away from a more systemic case-managed and family-inclusive approach to assessment and working and a greater focus now being placed on a short-term, siloed, nonspecialist care management approach to social work. Combined with difficulties around staff shortages, poor access to resources, and financial constraints in adult social care, participants painted a bleak picture of the social care landscape where professionals do not feel appropriately trained, are excluded from interdisciplinary working where they may be able to benefit from wider professional knowledge of ABI (and contribute to it), and are being deprived of the time required to appropriately form relationships with clients, observe their functioning, and work alongside them.
The findings of this study are in keeping with previous literature identifying that individuals with ABI and their families feel that their needs are currently going unmet by statutory services (Norman et al., 2022), with the greatest unmet need falling within the area of social care provision and interactions with social workers (Holloway et al., 2019; Norman et al., 2020; Odumuyiwa et al., 2019). These findings also fit with the previous work undertaken by the research team that highlighted a dearth of literature in the social work field surrounding ABI (Linden et al., 2023) and a lack of formal prequalification training on social work courses in England and Wales (Bald et al., 2025). It is also important to note that these issues regarding the structure and culture of social work within the health sector and how limited resources and a lack of knowledge prevents an effective social work contribution to MDT working have been noted in previous literature (Maxhakana, 2021; Maxhakana & Sithole, 2024).
Strengths and limitations
This study recruited social workers, team leaders, and commissioners from across England and Wales as well as Scotland. This helps to provide a clear picture of the training needs of social workers across a range of different local authorities within the region. Similar difficulties, lack of knowledge and lack of training, were found across all locales. A comparison is now needed with how social work practice meets the needs of those with ABI and their families in other international countries.
While the study was able to recruit sufficient social workers (newly qualified and specialist) to reach data saturation, the research team was unable to recruit satisfactory numbers of team leaders and commissioners. The team leaders highlighted that brain injury is often dealt with within differing pathways across various local authority social care departments. More information is needed to understand how that may impact the knowledge, understanding, and training needs of social workers. Furthermore, while the commissioners identified similar elements that may suggest data saturation, they too highlighted multiple ways in which services are commissioned that may impact service delivery. Therefore, the study was unable to capture sufficiently comprehensive information about the way in which service structures could be modified to support social worker training around brain injury.
Recommendations
The current study highlights a need for social worker training around brain injury to be embedded within the Social Work England training curriculum across England and Wales, as well as elsewhere in the United Kingdom. Social workers require easily accessible CPD to improve their knowledge of ABI and how to effectively work with clients and families. Finally, the authors recommend a systemic shift in the organizational structures surrounding social work that allows a return to a more holistic model of care that employs “good old-fashioned social work” and allows for interdisciplinary team working. Working more holistically would enable social workers to understand and incorporate diversity and to work more inclusively with individuals across a range of areas, not just ABI. Further work is needed to address the structures with social work and social work education that are currently hampering inclusive and holistic practice.
Conclusions
The findings from this study identify a series of factors that have led to social workers being poorly equipped to support individuals and their families after ABI. Difficulties surrounding the current curricula and the training of new social workers, as well as current work practices and the isolation of social work away from multidisciplinary colleagues, alongside inadequate resourcing of adult social care mean that the profession is unable to meet the needs of individuals and their families after what is likely the greatest challenge in their lives. A failure to adequately train and support social workers, a failure to work alongside colleagues with needed skills and knowledge, and a failure to resource and facilitate practice that is commensurate with the needs of people affected by ABI leads to clear harm, secondary harm, and unnecessary expenditure across wider health, social care, and prison services. The first step, educating social workers new to the profession, can be the first means to addressing other structural issues, reducing harm, and reducing waste of resources.
Footnotes
Ethics
Ethical approval for this project was given by the University of Essex Human Research Ethics Board (ETH2122-1055).
Authors’ contributions
AN, MH, CB, AA, MC, ML, and AB contributed to the design of the study. MH, CB, and AA conducted the interviews. AN led the initial round of coding and theme development. This was further adapted by MH, CB, AA, TS, TA, KM, AR, LD, SG, and SS. All authors were involved in drafting and reviewing the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute for Health Research (NIHR), reference number NIHR202980.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the sensitive nature of interview data, raw data are not available, but a full table of quotes can be obtained from the corresponding authors.