
Abstract
Summary
Physical abuse in care settings is a social problem with detrimental effects for residents, but effective prevention is dependent on staff reporting. In Sweden, designated officials, commonly social workers, are required to investigate reports of mistreatment. The aim of this study was to analyze what designated officials considered serious in reported incidents of physical abuse in two different care settings: care for older people and care for people with intellectual disabilities. Similar cases of physical abuse were chosen to demonstrate differences between judgments and provide a picture of how designated officials judge the relative seriousness of abusive situations. Interpretative content analysis and analytic induction were used to analyze reports of staff-to-resident abuse and resident-to-resident abuse in the two care areas.
Findings
There were no differences between incidents described as serious and those described as non-serious. Resident-to-resident abuse was the most commonly reported incident, particularly in dementia care and care for people with intellectual disabilities, and was rarely considered serious. Older people in dementia care were the highest risk group. In staff-to-resident abuse, staff were singled out as scapegoats. Organizational issues, rather than the details of abusive incidents, guided investigators’ judgments of seriousness. Tendencies to normalize violence and apply a narrow understanding of violence were found in the investigator’s judgments, particularly in resident-to-resident abuse.
Applications
Safeguarding adults from physical abuse in institutional settings is dependent on staff reporting and thorough investigations. This study shows that more training in assessing violence for social workers investigating reports is needed.
Introduction
Physical abuse against older people and people with intellectual disabilities in institutional settings is a social problem globally (Burns et al., 2013; Collins & Murphy, 2022; Fyson & Patterson, 2019; Hughes et al., 2012; Lachs & Pillemer, 2015; Moore, 2016). The detrimental effects of abuse on residents, such as pain, physical injuries, and increased rates of depression and anxiety, are well documented (Hughes et al., 2012; Lachs & Pillemer, 2015; Moore, 2016). Many incidents of abuse are also assumed to go unreported because residents have difficulties voicing their concerns or fear they will not be listened to or believed (Dong et al., 2014; Hollomotz, 2012; Lund, 2021). The discovery, investigation, and prevention of physical abuse in institutional settings is therefore highly dependent on staff reporting.
Many countries have some form of adult protection services that investigate abuse. In Sweden, staff are required to report all kinds of mistreatment within social care, and a designated official investigates all reports. Previous studies have shown that designated officials use different strategies when judging incidents of mistreatment and that there is a general lack of consensus of what is regarded a serious event (Manthorpe & Martineau, 2011; Trainor, 2015).
The aim of this article is to analyze what designated officials judged to be serious in reported incidents of physical abuse in two different organizational settings: care for older people and care for people with intellectual disabilities. Similar cases of physical abuse from the two areas were chosen to demonstrate differences in judgments and provide a picture of how designated officials frame the seriousness of abusive situations. Throughout the article, we use the terms “service user” and “resident” interchangeably for a recipient of care.
Context of mandatory reporting in Sweden
Mandatory reporting of mistreatment within social services in Sweden is regulated by the Social Services Act [SSA] (2001). The aim of the regulation is to protect at-risk service users, amend and improve services, and enable staff to report all mistreatment without risk of reprisal, thus increasing quality of care (National Board of Health and Welfare [NBHW], 2014). Reports are investigated by a designated official within each municipality. Designated officials are mostly trained social workers, and a university degree in social work or social care is required. In some municipalities, legal practitioners and registered nurses may work as designated officials (hereafter referred to as investigators).
Since the adoption of provisions in 1999 (care for older people) and 2005 (care for people with disabilities), there have been several amendments. Critical issues and problems with the implementation of the reporting process have been identified without any real solutions being reached. A key question concerns the definition of mistreatment, which includes acts or omissions due to negligence or for any other reason by a person that “entail or have entailed a serious threat to, or have had consequences for, the life, safety or physical or mental health of an individual” (NBHW, 2014, p. 49). NBHW (2014) is a manual for practitioners and gives a wide range of example incidents and situations that may be relevant to report, however, staff still have difficulty knowing what to report (Health and Social Care Inspectorate [HSCI], 2016). Although it is mandatory for staff to report mistreatment, there are no punishments tied to the regulation, and it is very likely that many incidents go unrecorded. In the government bill that preceded the legislation (Sweden's Ministry of Health and Social Affairs, 1998), the issue of possible punishments was discussed, but it was dismissed because it was considered important to encourage staff to report rather than punish those who did not. Staff have also shown hesitance to report because they feel they are blamed for all failures. The media often reports on scandals in nursing homes, for example, leading to associations between mandatory reporting and a “shame-and-blame culture,” in which staff are singled out as scapegoats for organizational shortcomings. According to the legislation, it is better to encourage staff to report to improve the quality-of-care provision (Sweden's Ministry of Health and Social Affairs, 1998).
How to determine the seriousness of an incident is another critical issue. Investigators provide a summary of each incident reported, as well as the associated causes and response, and offer a preliminary judgment on the degree of seriousness. Incidents are categorized according to the following judgments: mistreatment, risk of mistreatment, serious mistreatment, risk of serious mistreatment, or no mistreatment. If an incident is considered serious mistreatment, the municipal social welfare board must refer the investigation to the HSCI (NBHW, 2014). However, there is not much guidance for investigators in determining seriousness. They must lean on the definition of mistreatment: an incident that causes “serious consequences” for a service user's health and well-being. This is particularly challenging for investigators when service users themselves cannot express themselves fully, which may be the case for those suffering from cognitive impairment. In such cases, investigators must rely on interviews with staff or relatives and documented changes in service users’ mood, expressions, or other visible traits. However, far from all investigations in our study included such documentation. Overall, while there is a manual for investigators to follow, they have considerable discretion when conducting investigations. Only incidents that are deemed to be serious by an investigator undergo further inquiry by the regulatory body.
Physical abuse in care organizations
The focus of this study was on two different types of physical abuse in care settings: staff-to-resident and resident-to-resident. Staff-to-resident physical abuse is defined as intentional physical force resulting in physical harm or distress (Hirt et al., 2022). Increased risk of staff-to-resident abuse has been linked to individual staff in terms of burnout, psychological stress, and negative attitudes toward older people or people with intellectual disabilities (Botngard et al., 2021; Lund, 2021; Schiamberg et al., 2012). Other factors discussed in connection with staff-to-resident abuse include the institutional context and facility characteristics, such as workloads, support from managers, level of teamwork, and size of the facility (Botngard et al., 2021; Hirt et al., 2022). A recent systematic review found that staff believe abuse is best handled internally and, though it is seen as morally wrong, many cases are tolerated and underreported to protect staff (Hirt et al., 2022).
Resident-to-resident abuse has been identified as more common than physical abuse by staff in long-term care units (Gimm et al., 2018; Hirst, 2015; Lachs & Pillemer, 2015). A study of nursing homes showed that aggression by residents was often considered inevitable in elder care facilities, physicians were rarely consulted and there was little involvement by the criminal justice system (Snellgrove et al., 2013). Additionally, nurses did not report abuse between residents, and most strategies employed by staff were reactive, alleviating abusive situations rather than preventing future events (Rosen et al., 2015). Furthermore, residents suffering from dementia seemed to be more exposed to physical violence by co-residents (Snellgrove et al., 2013). In the later stages of dementia, cognitive and language abilities decline, leading to disruptive behaviors; this may include aggressive outbursts that prompt other residents to act aggressively (Rosen et al., 2015). Research on resident-to-resident abuse in group homes or supported accommodation for people with intellectual disabilities is limited (Nankervis et al., 2020). Much of the literature on abuse in the field of intellectual disabilities has focused on sexual abuse (Beadle-Brown et al., 2010). However, similar factors concerning abuse in care for older people and people with disabilities have been identified (Halladay & Harrington, 2015).
Labeling the seriousness of physical abuse in care settings
The meaning of violence and its different levels of seriousness is determined socially and culturally (Loseke, 2017). To count as a social problem, a condition must cause harm, and the harm must be specified by the person making the claim (Loseke, 2017). How harm is defined is crucial for all social problems and their solutions. Social workers investigating incidents of physical abuse must give meaning to the facts they gather, and investigators’ judgments of seriousness include a labeling process. Similar to framing a social problem, investigators construct the meaning of a condition by attributing blame and responsibility, explaining why the condition is intolerable, and presenting solutions to the problem. An effective strategy in complex cases is to construct simplistic diagnostic frames, which tend to offer an easy resolution to a problem. However, a simplistic diagnostic frame may fail to capture the complexity of the harm that violence against older people and people with disabilities causes.
When defining the seriousness of cases of violence, the literature focuses on several important factors (Brennan, 2016; De Haan, 2008; Tolan, 2007), three of which are of interest in the context of care provision. These factors relate to the perpetrator, the victim, and the institutional setting. The perpetrator's intention to harm themself or another is a central factor in defining violence, and how serious the violence is judged to depend on the interpretation of the motivation to harm (Tolan, 2007). In care facilities, residents should be protected from harm as they may have difficulty protecting themselves. However, as Tolan (2007) states, the question of motivation is controversial and has led to two countervailing views that promote different responses. The first is to see violence through the lens of personal responsibility and promote the application of legal methods in response. The other is to view violence as an issue of behavioral health that warrants changes in environment and risk-reducing strategies, for example, moving aggressive or victimized residents. Another important factor for judging the seriousness of cases of violence is the victim's perception of harm and the extent of any injury experienced (Tolan, 2007). The latter also corresponds to the definition of mistreatment in Swedish law, in which the consequences of mistreatment for an individual's life and physical or psychological well-being are central in determining the degree of seriousness. The likelihood of an incident being labeled as serious should correspond to the degree of harm suffered by the afflicted service user. The third factor in defining the seriousness of cases of violence has to do with the institutional setting (Tolan, 2007), specifically the notion that institutional practices, such as rigid regulations or inadequate staffing, inhibit the provision of care.
Method and material
This study was part of a larger study investigating all mandatory reports in one region over 1 year in Sweden (Kjellberg et al., 2023). In total, 1,105 reports were coded in a database. The material for this analysis includes reports of physical abuse in care for older people and care for people with intellectual disabilities. Both authors coded and set up the database and were familiar with the reports, which consisted of 1–2 pages of the initial report written by staff and an investigation written and conducted by an investigator, including a description of the incident, interviews, facts about staff and their competence, information about the care facility and finally a judgment of seriousness. The quality of the investigations varied widely. Each report included an investigation 5–15 pages in length. We refer to the report and the investigation as the same document, all included. IK conducted the preliminary screening and analysis. KB was involved in the latter stages of the analysis and write-up.
Screening procedure
There were 35 reports related to care for older people that included incidents of physical violence, and coincidentally there were also 35 such reports related to care for people with disabilities. Few of the cases were deemed serious by the investigator: five in care for older people and eight in care for people with disabilities. IK started carefully reading all 13 serious reports about physical abuse to find incidents that were sufficiently similar to compare. Three reports were excluded because they pertained to incomparable and unique incidents, leaving 10 serious reports remaining. Two different categories of violence were identified: (1) staff-to-resident abuse and (2) resident-to-resident abuse.
The remaining non-serious reports were then read, with 19 similar reports identified. Altogether, 29 comparable reports were included in the analysis: 18 from care for older people and 11 from care for people with disabilities. In care for older people, five incidents were reported from nursing homes, 10 from specific wards for older people with a dementia diagnosis, and three from home care, that is, a service user living in ordinary housing who receives assistance from staff at regular times. In care for people with disabilities, services are provided for people in need of various forms of support of all ages, including children. Nine incidents were reported in group homes, in which service users have their own flats but share common areas. One incident was reported from a group home for children (D43:5): accommodation for children with extensive needs that cannot be met in ordinary housing. One incident was reported in relation to a service user living in ordinary housing with the help of Personal Assistants (D55:7).
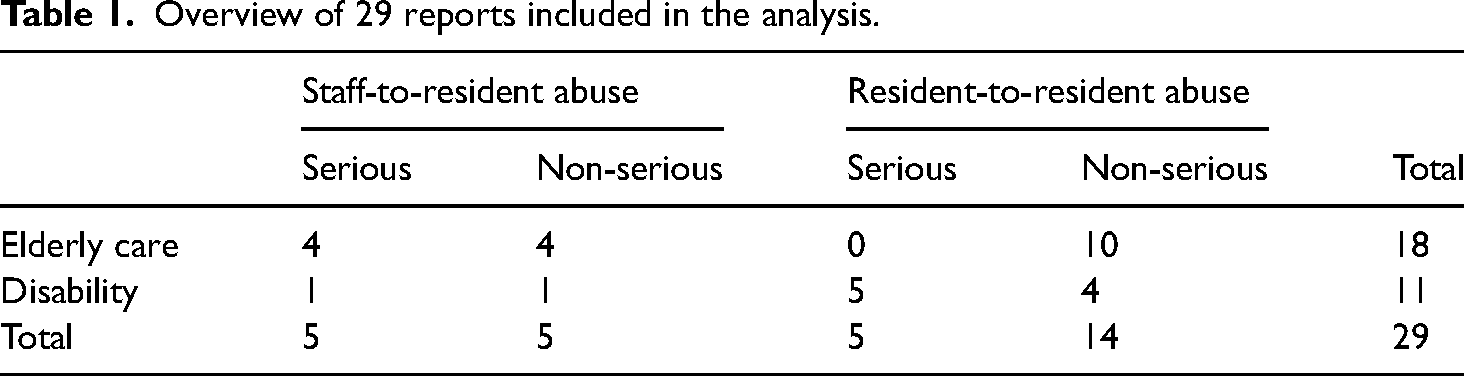
In care for older people, eight reports concerned staff-to-resident abuse and 10 concerned resident-to-resident abuse (see Table 1). Within disability care, two reports concerned staff-to-resident abuse, and nine concerned resident-to-resident abuse. The events reported were almost identical for both serious and non-serious incidents, but the judgments differed.
Overview of 29 reports included in the analysis.
Analysis
Initially, each report was coded using interpretative content analysis (Drisko & Maschi, 2015). Four main categories that comprised the judgments were identified: the incident, the perpetrator (staff or co-resident), the victim, and organizational issues. For the first category, descriptions from staff and the investigator were compiled and studied. The next three categories relate to the most important factors for determining the seriousness of cases of violence: characteristics and descriptions of the perpetrator, the victim, and finally organizational issues. We kept the analysis within the scope of the reports, taking care to provide summaries from divergent reports. After the initial coding, comparisons were drawn between care areas and serious/non-serious reports. Notes were written by the authors, including comments, ideas, similar cases in previous research, etc., throughout the coding process.
In the later stage of the analysis, we were inspired by the analytic induction approach (Katz, 2001) to develop assertions on what led to an incident being defined as serious. In analytic induction, phenomena are redefined as new explanatory factors are encountered (Katz, 2001). As new data are examined, initial assertions may be contradicted, and explanations reworked to validify the analysis. In our analysis, we were looking to define what investigators judge as serious in similar incidents of physical abuse. For example, an initial assertion was that to judge an incident as serious an investigator must identify harm to the victim, such as pain, distress or, in some cases, a medical examination proving serious injury. However, we soon encountered judgments of seriousness that did not meet this criterion. Thus, we reworked our assertion according to the new cases encountered. We regularly referred back to our notes, testing different assumptions and modifying our assertions. However, these assertions are exploratory rather than confirmatory.
Findings
The findings are structured according to the four main categories: incident, perpetrator (staff or resident), victim, and organizational issues. For each category, similarities and differences between serious/non-serious reports, care areas, and the two types of abuse are clarified. Assertions are made about what seemed to be important in the investigator's judgment of seriousness. Reports from care for older people are marked with an “O” in parenthesis and reports from disability care are marked with a “D.”
The incidents
Ten reports were included relating to staff-to-resident abuse, eight in care for older people, and two in care of people with disabilities. Half of these were deemed serious. In care for older people, all but one of the incidents involved service users with dementia.
There were 19 reports included related to resident-to-resident abuse: 10 in care for older people and nine in care for people with disabilities. Five reports from group homes for people with intellectual disabilities were deemed serious, one of them occurred in a group home for children. None of the reports in care for older people were considered serious, and all of them occurred in care homes for people with dementia.
Incidents in staff-to-resident abuse
In relation to staff-to-resident abuse, acts described included slaps to the face or body, pinching, pushing, forced increase in movement speed, dragging, and hard grabbing. Overall, staff were characterized as hard-handed and described as using raised voices. Incidents typically included at least two staff members, with one being aggressive and physically abusing a service user and others protesting and, sometimes, attempting to intervene. In many reports, staff reported witnessing recurrent incidents involving the same staff members abusing service users. One investigation contained four different occasions of reported physical abuse involving the same staff member, and other reports mentioned previous incidents of abuse, although not always with the same staff members involved. The situations were generally described as stressful, including one staff member losing their temper and screaming at a service user “What the hell are you doing” (D19:56) or “Here, this is how it feels” (O18:150) while pinching or slapping them. In some cases, verbal threats were made if the service user did not obey or behaved in a certain way. None of the investigators labeled the abuse as “violence.” Although physical abuse is a crime, only two incidents from all 10 reports were reported to the police (D55:7, O18:212).
Some incidents deemed non-serious also included cases of severe abuse, with one report mentioning verbal threats, bruises and a service user being struck with a bunch of keys and “pressed down in bed while the staff held a hand over her nose and mouth” (O18:51). Some cases deemed serious included incidents that seemed comparatively less so, for example, two light slaps on the buttocks (D55:7). That is not to say that such incidents are acceptable, but comparatively the abuse was described as less severe and a one-time occurrence.
Incidents in resident-to-resident abuse
In resident-to-resident abuse, cases of abuse were generally described as more severe than in staff-to-resident abuse and included beatings to the face and body, slaps, strangleholds, hard punches with fists, hair-pulling, pushing, and objects being thrown near and at people. In one case a resident put their arm around the neck of another and pressed their palm against their larynx (D19:84). Another walked into a co-resident's room and the staff discovered that he leant over the bed, where the resident was sleeping, and the visiting resident held his hand over the sleeping resident's mouth and nose (O50:64). The investigator deemed this to be mistreatment, but not serious mistreatment, because the actions “belonged to the picture of the disease” (O50:64). The situation was considered resolved when the agitated service user calmed down under the influence of new medication.
There were also verbal threats reported, including death threats: “R1 threatened to slit the throat of R2” (D19:85). One incident involved two teenagers: “R1 was frightened by R2 and started crying, then R2 hits R1 on the head. R1 was sad for the rest of the day” (D43:5). This case was deemed serious, despite more severe abuse being reported in other incidents deemed non-serious. However, a minor was involved in this case, which may be a reason for the investigators regarding it as serious.
The investigator labeled incidents of abuse as “violence” in four reports (of 19), of which three were deemed serious. In some incidents, the abusive resident directed aggression toward a specific resident who seemed to irritate the aggressor. It was also common for abuse to start when a specific resident moved into the care facility. Most of the incidents occurred in common areas of the care facility. Guards were called in two cases (D19:85, O50:60), the police were alerted in one case (D23:3) and a police report was filed by a next of kin in another (D19:85). However, whether police reports were filed in the remaining cases was unclear; next of kin were asked to file a report in two cases but did not do so. In one incident, relatives of a resident indicated that they would not file a police report, but it was not clear from the investigation whether they did so ultimately. According to legislation, a victim of abuse should file a police report, but if there is no next of kin to help or the service user is afraid of retaliation, abuse is often not reported to the police.
Similarities, differences, and assertions in the incidents
There were more incidents reported concerning resident-to-resident abuse than staff-to-resident abuse, however, resident-to-resident abuse was considered serious in fewer cases than staff-to-resident abuse, despite incidents including more serious cases of violence. Physical abuse between co-residents in dementia care was not considered serious mistreatment. Older people with dementia seem to be at higher risk than other groups.
One difference between the care areas was that more incidents of resident-to-resident abuse occurred in care for people with intellectual disabilities.
Incidents included similar descriptions of physical violence in serious and non-serious reports, suggesting that it is not the incidents as such that determine investigators’ judgments of seriousness. In conclusion, we suggest that for both types of abuse, similar situations are judged differently; it is not the severity of abuse or a particular situation that forms investigators’ decisions of degree of seriousness.
The perpetrator
The main objective of the reporting procedure is to prevent something similar from happening again, and to understand why the misconduct occurred (NBHW, 2014).
Staff as perpetrators
In all five reports deemed serious incidents of staff-to-resident abuse, staff denied abusing the service user. Those accused had another view of the event than the one reported. The allegations were not proven but the accused staff were still dismissed. In one report the investigator concluded that there was an ongoing conflict in the work team (O35:11). The only serious incident from the disability area involved a personal assistant slapping a service user twice on the buttocks. They denied the accusation but were dismissed.
The remaining non-serious reports followed the same pattern: all staff denied the accusations, but three out of five staff members were dismissed. In one report (O18:150) the accused staff member admitted to the violence and claimed that it was a result of stress resulting from private problems. The employee was also well liked, and the investigator recommended a warning instead of dismissal. In another report (O18:22) the accused staff member had previously been redeployed for inappropriate behavior. It was unclear what steps the organization had taken to ensure the safety of service users, and misconduct had occurred on several occasions over 2 years. Still, this was not considered to be serious mistreatment.
Investigators’ views of the reasonings for staff acting violently appeared inconsistent. In one report the underlying reason was explicitly stated as “staff with inappropriate behavior were hired” (D55:7). However, further safety measures when hiring staff were absent from the recommended actions. Another report stated the opposite that the underlying reasons were deemed to be of a temporary personnel nature, and there was no indication that the incident was due to structural problems within the organization (O18:212). The conclusion was that the situation would be under control once the specific staff member was dismissed. The organization was not to blame; this was one unsuitable employee. It can be argued that the staff member in question exhibited a pattern of inappropriate behavior prior to being hired, but the investigator judged the incident to be linked to a specific employee and that therefore the matter should be handled under employment law.
Residents as perpetrators
Five cases were deemed serious in resident-to-resident abuse, all of which occurred in care for people with disabilities. In the reports, there were few descriptions of the abusive resident. One resident was said to be acting out because of sound sensitivity (D43:5). In two cases, aggressive residents had recently moved into the care facility, of which there was a general lack of knowledge among staff (D19:85, D23:3). The reasons for the incident were not primarily attributed to the abusive resident. Instead, it was emphasized that low-affective treatment was necessary when working with the target group and a general statement was made, with no further details given, explaining that extensive work was underway concerning the resident (D43:9).
Descriptions of aggressive residents in reports of non-serious incidents were also rare. One report stated that the group home was strongly influenced by one resident's behavior (D37:2). In reference to an incident that occurred during daily activities, it was stated that a resident had a difficult home situation which was reflected in the daily activities (D50:54), and sound sensitivity was again mentioned as a triggering factor (D9:11).
In dementia care homes (10 non-serious reports), abuse between residents was mostly explained as a symptom of dementia “the reason the resident is agitated is due to the onset of the disease, which can be difficult to divert despite action plans and routines, and that these two residents do not always get along” (O50:57). Similar statements appeared in several reports, with a few adding that it was difficult to guarantee that a similar situation would not arise again (O27:16). Abusive residents were described as “acting out,” “aggressive,” or “agitated”; however, in one report, an investigator labeled abuse and its perpetrator as violent (O18:139).
Conclusions and assertions about the role of perpetrators in both cases
In conclusion, there was seemingly no discernible pattern to investigators’ judgments of inappropriate and aggressive behavior by staff, and differences between the two care areas were not evident. In most cases, abusive staff were dismissed, which seemed to solve the problem. Employers are mandated to check the police register before hiring staff in social care, but this only provides information on those who have previously been convicted of a crime. Although one investigator highlighted the hiring of unsuitable staff as a problem, it did not lead to further safeguards in the employment process. If staff admitted to acts of violence and showed remorse, in combination with referencing private problems, cases were sometimes attributed to mitigating circumstances. Apparently, investigators assessed unsuitable staff inconsistently.
The reasons for abusive residents being agitated in cases of resident-to-resident abuse was explained differently across the two care areas. In care for people with disabilities, aggression was attributed to personal dislike of a certain resident or an aggressor being a new arrival in the group home. This was also occasionally given as an explanation in care for older people, but most physical abuse was explained as a symptom of dementia. One assertion is that in dementia care the safety of the residents cannot be guaranteed due to the nature of their condition. In some cases, the disease made residents behave violently. Such an assertion may result in older people and people with disabilities being characterized by their impairment, illness, or physical needs. Here, violence appeared to be part of a physical and/or a mental condition rather than a social phenomenon.
The victim
The core criteria for defining mistreatment in the SSA (2001) are the consequences of mistreatment for a service user. If an incident of mistreatment has negative consequences for the life, safety, or physical or psychological health of an individual, staff are obliged to report it and the incident must be investigated. If a service user suffers any harm it is defined as mistreatment, but there is not much guidance for investigators in judging severity. The regulation for mandatory reporting should contribute to ensuring that the individual receives good-quality interventions. It must also protect the individual from abuse (NBHW, 2014).
The victim in staff-to-resident abuse
In staff-to-resident abuse, the consequences for service users in serious and non-serious reports were contradictory. In the serious reports, consequences were described in vague terms, such as feelings of violation, or not described at all. However, in all non-serious reports, the consequences for service users were referenced in the judgments. In some reports, it was obvious that service users had difficulties communicating, and investigators gathered information about staff apprehension over changes in the mood of service users. Sometimes, bruises or bleeding were described, but mostly the consequences described included fear, insecurity, and feelings of being violated; as one service user said, “I feel belittled” (O48:9). In one case the service user was able to express herself and said she suffered from “increased anxiety … constantly afraid … must have the lights on at night, the desire for death has increased,” but she was also afraid of causing trouble (O18:51). She was abused during the nightshift, which made her feel even more exposed. These consequences were not enough for the investigator to judge the mistreatment as serious. The incidents were deemed to be mistreatments, but not serious mistreatment. The investigator concluded that issues that should be considered in particular were treatment issues, and “how to deal with the service user's emotional experiences, where to draw the line between violence and harassment” (O18:51). However, it is unclear how this line was drawn in this case, although the investigator pointed out that the service user was trustworthy. In contrast, three serious reports included a standard formulation “the reported events refer to actions and the omission of actions that could have or have had consequences for service users’ physical and psychological health” (O34:19, O18:22, O18:150). These investigations did not contain any more information about the consequences for the service users, but they were deemed serious mistreatments.
The victim in resident-to-resident abuse
All reports in resident-to-resident abuse included consequences for the abused resident. Of the serious incidents, there were reports of bruises, a concussion, fear, anxiety, sadness, etc. The non-serious reports included reports of bruises, pain, fear, anxiety, feelings of being locked in, and sadness. One report also referred to a hip fracture, of which the investigator stated that the incident “has had serious consequence for the resident … a hip fracture with several days of concomitant hospitalization. The need for care has also increased after the incident” (D19:42). The consequences were serious, but the overall assessment was not of serious mistreatment. In one group home, an abused resident had to move to another facility, and several other residents moved or threatened to move because of an abusive resident (D37:2).
Assertion regarding consequences for victims in all reports
The threshold for what was considered serious with regard to service users’ experiences of harm seemed very high in some cases and low in others. Although the definition of mistreatment leans on service users’ experience of harm, the extent of the consequences for the life, safety, and physical or psychological health of an individual was not always used as a main criterion for judgments of seriousness, as is required by legislation.
Organizational issues
Mandatory reporting is part of systematic quality assurance work, and all reports of serious mistreatments must be sent to the HSCI for control and approval. One aim for the organization is to develop, and improve, to correct mistreatments and to prevent similar incidents from occurring again. The purpose is to understand why the mistreatment did occur (NBHW, 2014). Questions the investigator asks regarding the role of the organization when incidents have occurred include, for example: Do staff have the right competence for their tasks? Is there good supervision and coaching? Did staff receive enough information about the individual's needs before the arrival to the care facility? (NBHW, 2014). These questions are generally considered in investigations.
Staff-to-resident abuse
The seriousness of an incident was highlighted by referring to organizational issues in all serious reports in staff-to-resident abuse. There were statements on lack of leadership (O34:25), lack of trust in managers as a result of frequent changes and a “long lasting destructive culture … the systematic quality assurance work has not worked out well” (O34:19), underlying conflicts between staff (O35:11), lack of documentation and that the organization had not managed to anchor value-based work in the right way in all employees (O48:9). The only serious report in care for people with disabilities (D55:7) concluded that staff who exhibited inappropriate behavior had been employed, but this was not pursued on a systematic level.
Some of the same arguments were found in the non-serious reports but to a much lesser degree.
Resident-to-resident abuse
In most serious reports, the lack of organizational control, supervision, pedagogical support, and a lack of documentation and competent staff were used as evidence to support the judgment of an incident as serious. There were examples of organizational issues overriding a resident's suffering stating that the main deficiency in the organization was not that a resident had been hit and pinched in the arm by another resident, but that the manager did not follow the routines of mandatory reporting, and promptly documented immediately taken measures (D43:9). The one report that concerned a child stood out as an exception, with organizational issues not mentioned.
In the non-serious reports, for both care areas, organizational issues were underemphasized or absent. Instead, there were statements of action plans working and in support of staff, they did what they were supposed to do, and there were no deficiencies on a systematic level (O18:139). When organizational problems were mentioned, it was usually an observation without clearly stated actions. There were also some reports that stated that described measures were adequate for preventing similar events in the future or that an action taken was enough to remedy the mistreatment. If mistreatment was interrupted or ameliorated, seriousness seemed to no longer be of concern and control and approval from the HSCI were deemed unnecessary.
Conclusion and assertion of organizational issues in all reports
In cases of staff abusing service users, the causes were commonly attributed to abusing staff. Overall, organizational faults and a lack of quality assurance work were accentuated in most serious reports and de-emphasized or absent in non-serious reports. Police reports were rarely filed. In no cases did the organization take responsibility for filing police reports, and it was expected that this be done by the victim of abuse. If there was no next of kin to help, or the service user was afraid of retaliation, abuse was not reported to the police.
The assertion regarding the importance of organizational issues was that the seriousness of abuse was accentuated if there were organizational issues highlighted by the investigator. One report in resident-to-resident abuse concerned a child, and when a child was involved, organizational issues did not seem necessary for an incident to be judged as serious.
Discussion and implications
Physical abuse in care settings is detrimental for service users and care organizations. In Sweden, the designated officials who investigate mandatory reports of mistreatment are mostly social workers. Their judgments have an immediate impact on service users’ lives, safety, and health. Previous research has shown physical abuse to be relatively common in care settings (Burns et al., 2013; Collins & Murphy, 2022). The threshold for seriousness is blurred and boundaries are hard to set (Keddell & Hyslop, 2020). The comparison of judgments of seriousness in staff-to-resident abuse and resident-to-resident abuse in care for older people and care for people with intellectual disabilities showed that investigators judged similar types and situations of abuse differently, depending on whether the perpetrator was a staff member or co-resident. In staff-to-resident abuse, individual staff were singled out as scapegoats, with emphasis put on individual responsibility. In resident-to-resident abuse, violence was interpreted as a behavioral health issue, particularly in dementia care. When a violent perpetrator acted out it was viewed as a symptom of disease, because the presence of dementia resulted in the motivation to harm being judged as absent. Thus, the motivation to harm (De Haan, 2008; Tolan, 2007) seemed crucial for investigators’ judgments. As a result of social workers’ judgments, there is a risk of physical abuse being normalized, which may result in continued physical violence.
There were more commonalities than differences between care for older people and care for people with intellectual disabilities. However, one difference was the greater number of reports of resident-to-resident abuse than staff-to-resident abuse in care for people with disabilities. There is a growing awareness of resident-to-resident abuse being more common than other forms of abuse in institutional settings (Lachs & Pillemer, 2015). Overall, there were more incidents and, based on the descriptions of the violent acts, more severe incidents, of resident-to-resident abuse. However, investigators generally considered these incidents to be less serious than cases of staff-to-resident abuse. In line with previous studies, older people with dementia seemed to be particularly at risk of physical abuse by co-residents (Snellgrove et al., 2013). There was evidence of the normalization of violence in dementia care, stemming from assumptions of the disease making residents aggressive. Despite the descriptions of incidents including serious and repeated violence and severe injuries, in most cases, they were not defined as “violence.” When framed as a behavioral health issue, violence was regarded as “normal” in dementia care, leading to no action being taken. How acts of force are defined, whether as violence, abuse, aggression, or assault, affects reactions and responses to them (Triplett et al., 2016). The descriptions of incidents include various judgments on the degree of seriousness; for example, there are distinctions drawn between slapping, pushing, and hitting. The judgments of investigators supported various interventions that can be tied to whether they defined incidents as violent or not. Violence demands action, and physical interpersonal violence calls for criminal justice in many cases (Triplett et al., 2016). However, in the care context, Åkerstrom (2002) showed that violence by residents is rarely defined as such and downplayed by nurses in an attempt to normalize older peoples’ aggression. In this way, acts of violence are portrayed as less serious and can remain within the context of care provision. Similar tendencies to normalize violence were identified in investigators’ judgments, particularly in resident-to-resident violence. We do not advocate for service users in care facilities to be criminalized or disease-related aggression to be completely removed as a diagnostic framework. However, investigations also need to address the social dimensions of interpersonal violence and recognize helpful specialist support linked to this, for example, sufficient emotional support, and the acute prevention of future violence (Lonbay & Southall, 2024). The same tendency toward a narrow understanding of violence was shown in relation to resident-to-resident violence in disability care, and the social context seemed to shape the way violence was interpreted, that is, as a behavioral issue linked to impairment. More research on the latter is greatly needed (Nankervis et al., 2020).
Surprisingly, there were no differences between serious and non-serious incidents. The incidents included similar descriptions of physical violence and it was not the severity of the violence that guided threshold decisions for seriousness. Similarly, victims’ perceptions of potential harm and the extent of the injuries they experienced were not used as the main criteria for seriousness, as should be the case according to the legislation (NBHW, 2014). Instead, the threshold for what was deemed serious relied on investigators accentuating organizational issues, such as a lack of supervision, documentation, or competent staff. However, as research demonstrates, commonly suggested interventions for organizational issues, including more rules, policies, and administrative measures, rarely make a difference (Trainor, 2015). The way the mandatory reporting system is processed in Sweden seems inadequate to protect service users from physical violence. Interventions appeared slow and insufficient, particularly in dementia care but also in care for people with intellectual disabilities where residents were at risk of violence from co-residents. It may be time to change reporting procedures and let service users and their advocates have a greater say in investigations of alleged abuse in Sweden. It seems that more training is required in assessing violence for the Swedish social workers investigating reports.
Limitations of the study
It was not possible to analyze gender differences because names and genders were anonymized in the reports used. We do believe gender is important, however, our request that gender data not be anonymized was not granted.
Conclusion
Physical abuse by staff and co-residents of older people and people with intellectual disabilities in care settings is not uncommon. Based on the descriptions of the violent acts in reports of mistreatment, this study showed that resident-to-resident abuse was more likely to be reported than staff-to-resident abuse. Service users in dementia care seemed to be most at risk, and in this context, violence was regarded as a behavioral health issue resulting from insufficient measures taken and with a risk of continued violence. Similar and severe acts of violence were judged differently, showing inconsistency in investigators’ judgments. Investigating reports of physical abuse is a complex and delicate matter, and more safeguarding guidance for investigators seems to be necessary. Methods to investigate abuse by listening to service users and their advocates are needed.
Footnotes
Ethical approval
The study was approved by the Swedish Ethical Review Authority (approval number 2020-05817).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Swedish Research Council for Health, Working Life and Welfare (FORTE; grant number 2020-00195). The funding source had no role in the collection, analysis, and interpretation of data, in the writing of the report or in the decision to submit the paper for publication.
Declarations of conflict of interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.