
Abstract
Ectopic eruption of the first permanent molar is prevalent in children, with a reported prevalence of up to 6%. Treatment options usually range from passive observation to active correction with orthodontic appliances like separators or distalising devices. This study outlines the step-by-step procedure for creating a ‘pistol spring’ system, which delivers a consistent, sustained force, reducing the need for frequent reactivation. The system is easy to fabricate, well-tolerated and enhances treatment efficiency, improving patient compliance and reducing chair-side time. The ‘pistol spring’ offers a cost-effective, time-efficient solution for managing ectopic first molars, particularly in paediatric patients with limited appointment availability.
Plain language summary
Sometimes, children’s first permanent molars do not come in properly, which happens in up to 6 out of 100 kids. This can cause problems if not treated. Dentists usually watch and wait or use devices to fix it. This study explains how to make and use a new tool called the ‘pistol spring’. It gently moves the molar into the right place and does not need to be adjusted often. The spring is easy to make, comfortable for kids, saves time at the dentist’s office and is affordable—making it a helpful option for busy families.
Introduction
Ectopic eruption of the first permanent molar is a developmental anomaly in which the first molar erupts in an abnormal path, often leading to impaction against the distal surface of the primary second molar (Hsiao and Boynton, 2016). The reported prevalence is in the range of 1%–6%, with a significantly higher incidence in the maxilla (Alfuriji et al., 2023; Caliskan et al., 2021). This condition is commonly observed in children and, if left untreated, may result in resorption and premature exfoliation of the primary molar, with subsequent space loss, and creation of, or worsening of, a malocclusion (Hsiao and Boynton, 2016; Seehra et al., 2011). Early diagnosis and timely intervention are crucial to prevent long-term orthodontic complications.
Several treatment modalities exist for managing ectopic first molars, ranging from passive monitoring to active mechanical correction using separators, distalising appliances or surgical intervention (McFarlane, 2004; Seehra et al., 2011). Previous studies have reported the Piston Elastic using power chains (Kim et al., 2021; Wangsrimongkol, 2023); however, the power chains tend to lose force rapidly due to material fatigue and intraoral environmental factors, thus often requiring multiple follow-up appointments for replacement or tightening to maintain adequate force levels.
This paper presents a clinical pearl on making a ‘pistol spring’ system with a molar buccal tube and closed coil spring for uprighting and distalising the ectopic first molars. This ‘pistol spring’ system provides a superior force consistency and reduced need for frequent reactivation. It is a cost-effective and time-efficient solution for ectopic first molars.
Methods
The step-by-step process for forming the ‘pistol spring’ system is listed below.
Materials: rectangular stainless-steel wire and second molar buccal tube
Use rectangular stainless-steel (SS) wire, preferably 0.018 × 0.025 inches for 0.022-inch slot systems, or 0.016 × 0.022 inches for 0.018-inch slot systems. Rectangular wire offers improved rotational control and reduced mucosal irritation compared to round wire.
A second molar buccal tube is recommended over the first molar tube due to its smaller size and lower profile, which minimises occlusal interference from opposing mandibular molars.
Wire bending
Create a C-shaped loop on the mesial side of the buccal tube to serve as a hook for the closed coil spring (Figure 1). At the distal end of the tube, form an L-shaped bend designed to rest against the distal surface of the primary second molar (tooth E). This design prevents the wire from sliding into the primary molar, especially in cases where distal root resorption is present.
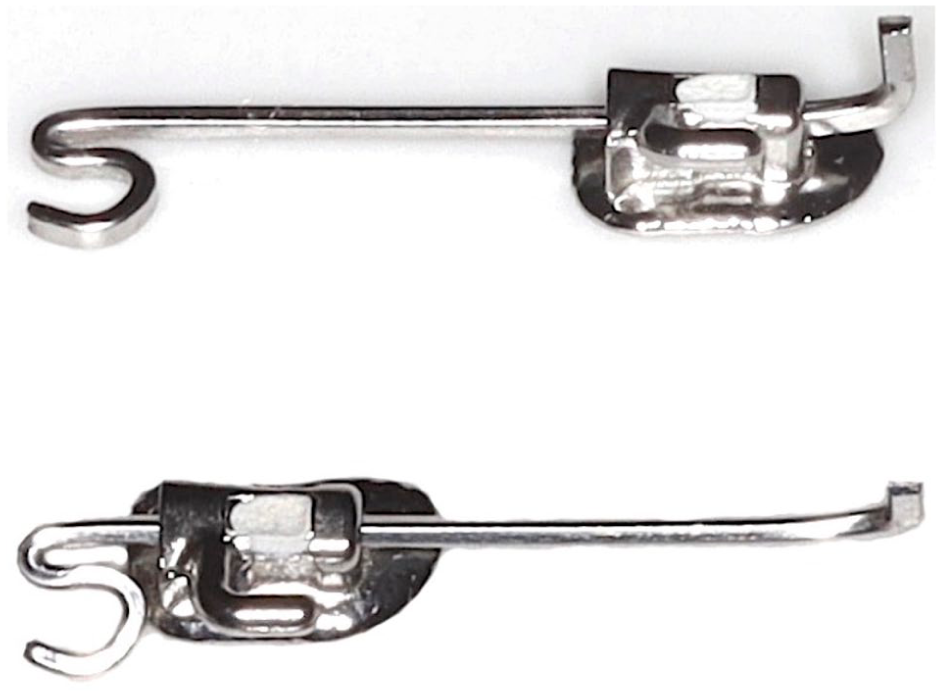
Components used to create the pistol spring, including a rectangular stainless-steel wire and a molar buccal tube.
The wire and molar tube together form a plunger-type mechanism, allowing smooth mesiodistal sliding within the tube (Figure 1).
The total wire length after bends is approximately 20 mm—approximately double the mesiodistal width of the first permanent molar—to allow for adequate activation and force delivery.
Placement of the closed coil spring
Use a 5-mm segment of closed coil spring. Hook approximately 1.5 mm of the spring onto the molar tube hook and 1.5 mm onto the mesial C-loop of the SS wire. The remaining 2 mm of the spring is the active portion that delivers the force needed to upright and distalise the first permanent molar (Figure 2).
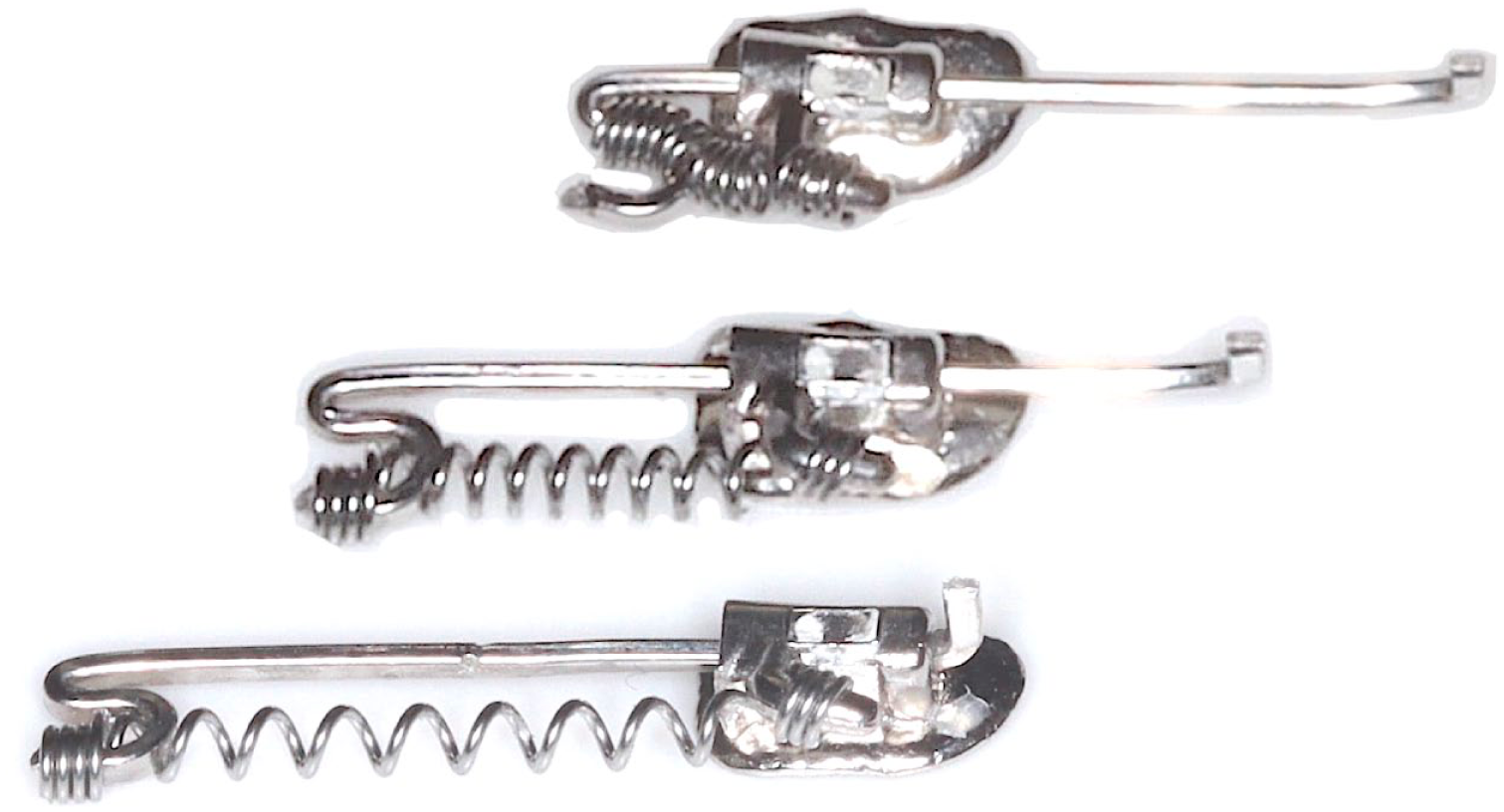
Closed coil spring generates continuous force for correcting an ectopic molar.
Bonding the ‘pistol spring’ system
Bond the entire assembly onto the occlusal surface of the ectopically erupting permanent first molar using light-cured composite resin (Figure 3).

The pistol spring is bonded on the permanent first molar.
It is recommended to cover the exposed wire ends with flowable composite resin to prevent soft tissue irritation and dislodgement of the coil spring due to mechanical forces such as toothbrushing.
Correction of the ectopic first molar
The coil spring generates a distalising force by pushing the wire against the primary molar (tooth E). This creates a reaction force that acts on the first permanent molar, leading to uprighting and distal movement of the tooth. In the presented case, successful correction of the ectopic eruption was observed in 2 months (Figure 4). It is recommended to achieve at least 1 mm of space between the distal surface of the primary molar E and the mesial surface of the permanent first molar. This clearance helps facilitate natural eruption past the point of impaction.
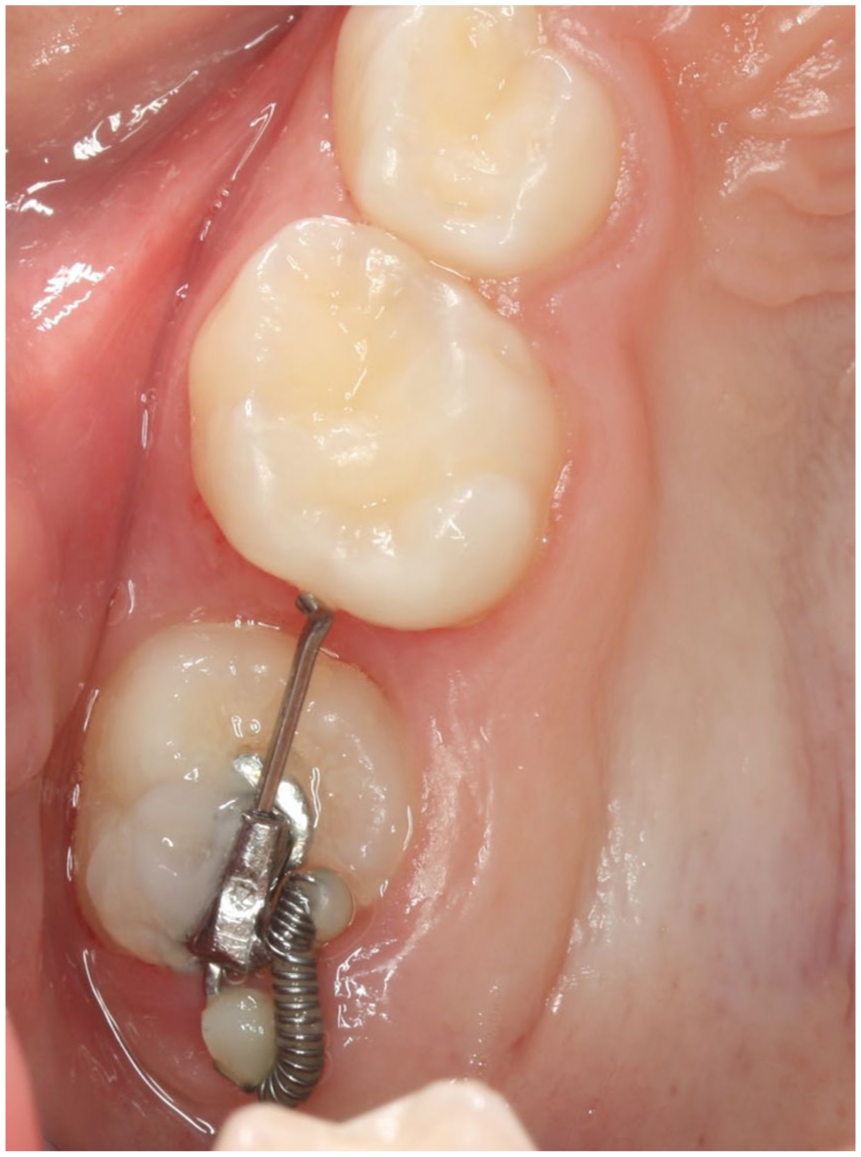
Reaction force on the first molar induces uprighting and distal movement, with successful ectopic eruption correction in 2 months.
Although the ‘pistol spring’ has demonstrated clinical effectiveness, regular clinical supervision remains essential. Due to its small size, there is a potential risk of accidental breakage and unnoticed inhalation between appointments, which must be carefully monitored. In addition, timely removal of the appliance once the desired treatment outcome is achieved is crucial to avoid unnecessary complications.
Conclusions
The ‘pistol spring’ is easy to fabricate and is well-tolerated by patients. It provides a more stable and sustained force over time, allowing for efficient molar movement with fewer clinical visits. This not only potentially improves treatment efficiency but also enhances patient compliance and reduces chair time, making it especially advantageous in paediatric patients or those with limited appointment availability.