
Abstract
Introduction:
Management of mutilated cases is challenging, and adult patients often require orthodontic correction of occlusion before prosthetic replacement of missing teeth.
Objective:
To highlight the novel, simple, hygienic, and efficient miniscrew-supported Beta titanium molybdenum alloy (TMA) cantilever spring for uprighting severe mesially tipped molars for interdisciplinary treatment.
Diagnosis and Treatment:
A 23-year-old male patient presented with skeletal Class I relation, average growth pattern, Class II Division 1 malocclusion with dentoalveolar collapse, crowding, multiple missing, supraerupted teeth, and severe mesially tipped mandibular third molars. MBT appliance with 0.022˝ slot was used to achieve the objectives. 38 and 48 were uprighted and protracted with miniscrew implant-supported TMA cantilever springs to substitute 37 and 47. Mild intrusion of maxillary posterior teeth was done with acrylic bite blocks and transpalatal arch (TPA), followed by prosthetic replacement of missing teeth.
Results:
The patient had a consonant smile arc and a pleasing soft tissue profile. 38 and 48 were uprighted and protracted with good vertical control, and the mesial pockets were eliminated. 17 and 27 were intruded, and group function occlusion was established. Class I canine relationship, normal overjet, and overbite were achieved.
Conclusion:
Miniscrew supported TMA cantilevers are efficient for uprighting of severely tipped 38 and 48 without extrusion, unlike the conventional mechanics. 18, 28, 38 and 48 with good root forms can be protracted and substituted as 17, 27, 37 and 47 respectively to minimize or eliminate prosthetic rehabilitation.
Keywords
Introduction
The management of mutilated cases is challenging for orthodontists. They usually include adult patients with missing teeth, periodontal lesions, fractured teeth, functional shifts, temporomandibular joint disorders, etc.1, 2 Most of them require orthodontic correction before prosthetic replacement of missing teeth. 3 This includes correcting unfavorable sequelae of long-term missing teeth such as the tipping of teeth adjacent to extraction space, supraeruption of opposing teeth, and periodontal pockets. 4
The common orthodontic correction is the uprighting of tipped abutment teeth. The challenges faced during uprighting are lack of adequate anchor units, anchorage loss like proclination of anterior teeth, or mesial movement of posterior teeth. 5 The skeletal anchorage systems provide good support and eliminate the adverse effects of orthodontic forces on anchor units. Miniscrew implants provide a wide range of options in mutilated cases. 6
Apart from the mechanical considerations, the management of interdisciplinary cases require utmost attention.7, 8 Treatment plan must be meticulous and correlated with other involved departments for timely follow-up appointments. Patients usually are misled because of a lack of communication between clinicians of other disciplines. Hence, scheduling plays an important role in gaining the confidence of patients and efficient rehabilitation of function and occlusion.
The purpose of this case report is to highlight a novel, simple, hygienic, and efficient miniscrew-supported TMA spring for orthodontic treatment of dentoalveolar collapse and interdisciplinary treatment. To our knowledge, there is no case report in the literature using an implant-supported TMA cantilever spring without any loop or helix that is efficient and simplifies maintenance of hygiene in periodontally compromised cases.
Diagnosis and Etiology
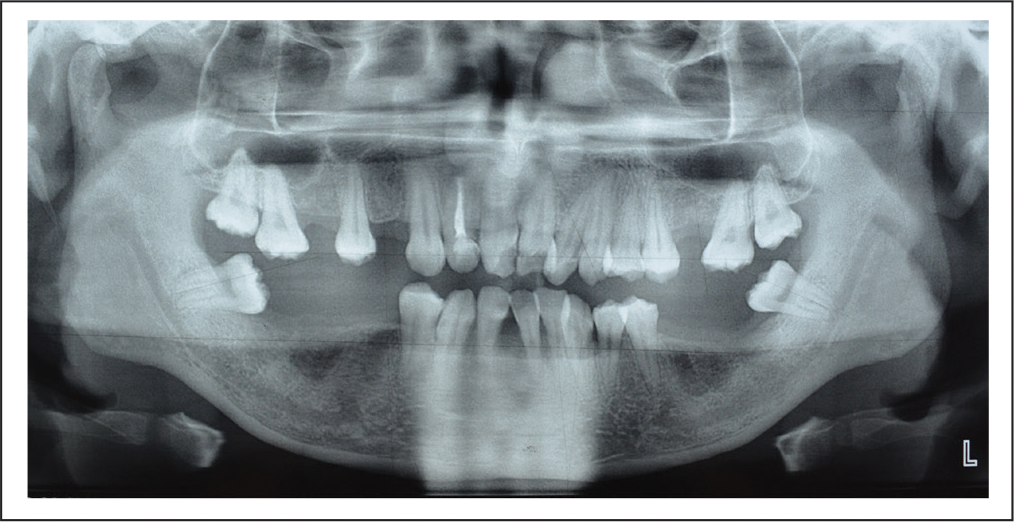
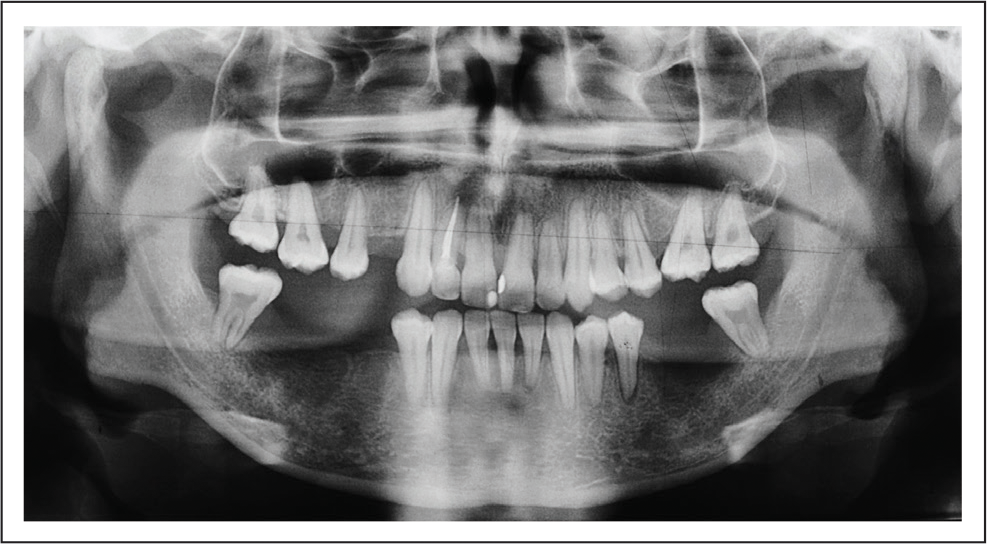
A 23-year-old male patient came to the department with the chief complaint of inability to chew food properly and crowding of upper anterior teeth. He was mesoprosopic with a straight profile and competent lips. The smile arc was nonconsonant. The maxillary midline was shifted to the right in relation to the facial midline. There was no functional shift or temporomandibular disorder. Intraorally, moderate crowding in the maxillary and mandibular anterior teeth was observed. He had 9 missing permanent teeth—14, 16, 26, 36, 37, 41, 45, 46, and 47. 17, 27, 38 and 48 were mesially tipped into the extraction spaces. Supraeruption of 15, 17, 25, and 27 was observed (Figure 1). The orthopantomogram showed a fair periodontal status and endodontically treated 12 (Figure 2). The cephalometric analysis revealed a Class I skeletal relationship and average growth pattern with proclined maxillary incisors (Figure 3). The diagnosis was skeletal Class I with average growth pattern, dental Class II Div 1 malocclusion with dentoalveolar collapse, multiple missing teeth, supraerupted teeth, severe mesially tipped 38 and 48 and Miller’s Class III gingival recession in relation to 31. Etiology: Dentoalveolar collapse resulting from extraction of grossly destructed posterior teeth because of caries and periodontitis.
Pretreatment Photographs.

Pretreatment Orthopantomogram.
Pretreatment Lateral Cephalogram.

Treatment Objectives
The treatment objectives were decrowding, uprighting, and protraction of 17, 27,18, 28, 38 and 48 intrusion of supraerupted 15, 17, 25, 27, to achieve Class I canine relationship, normal overjet and overbite, group function occlusion, and prosthetic replacement of 14, 36, 45, and 46.
Treatment Plan
A nonextraction line of treatment with preadjusted edgewise appliance using miniscrews as direct anchorage for uprighting and protraction of 38 and 48 with a segmental approach.
Oral prophylaxis was planned once in three months during the treatment. Free gingival graft for covering the gingival recession of 31 was planned. Prosthetic replacement of 14, 36, 45, and 46 was planned after orthodontic treatment.
Treatment Alternatives
The first treatment option was uprighting and protraction of 38 and 48 with the microimplants-supported TMA cantilever mechanics to substitute 37 and 47 as they had good root form, sectional arch mechanics in the mandibular anterior teeth, continuous arch mechanics in the maxillary arch, protraction 17, 27 to substitute as 16 and 26 and 18 and 28 as 17 and 27, intrusion of 15, 17, 25, 27, and prosthetic replacement of 14, 36, 45, and 46.
The second option was the same as above but with continuous arch mechanics in the mandibular arch, without miniscrew implants for third molar uprighting and protraction.
The third option was autotransplantation of 38 and 48 as 37 and 47, followed by orthodontic treatment to achieve the objectives and prosthetic replacement with implants for other missing teeth.
The first option was the finalized treatment plan as that would provide the best biomechanical advantages. The miniscrew-supported cantilevers produce sufficient moments for uprighting and effectively suppress the extrusive forces on the molars as they are upright. The restraining tie from the miniscrew does not allow distal displacement of the crown, leading to relatively fail-safe molar root movement. 9 The sectional wire in the anterior segment would prevent undesirable side effects because of molar uprighting.
The second option was not considered as the continuous arch mechanics would extrude 38 and 48 during uprighting with undesirable side effects on the premolars and proclination and intrusion of anterior teeth.5, 7 The third option was not selected as the patient did not want to undergo surgery for autotransplantation.
Treatment Progress
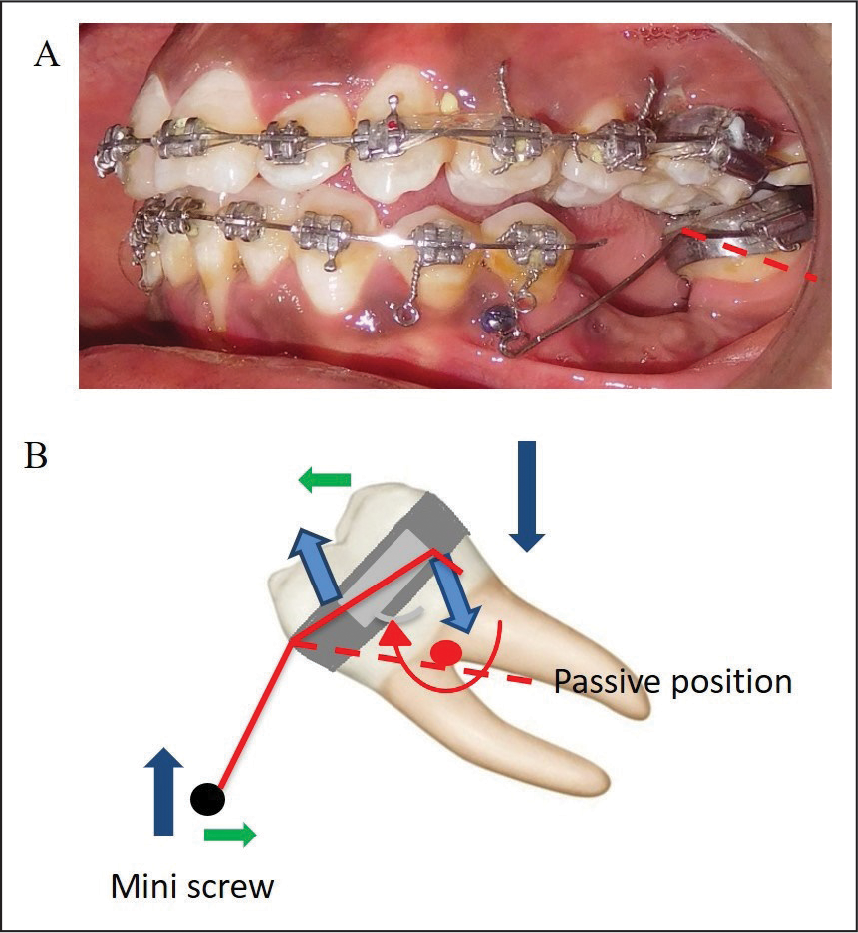
Maxillary and mandibular arches were banded and bonded with MBT appliance (0.022″ slot). Initial alignment and leveling was done using 0.014″ nickel titanium (NiTi), 0.016″ NiTi, and 0.018″ AJ Wilcock archwires with the continuous arch in the maxillary and sectional in the mandibular arch. A removable posterior bite plane was used in the mandibular edentulous region to intrude mildly supraerupted 15, 17, 25, 27 (Figure 4). It was advised to be worn full time, during meals also. Miniscrew implants were placed in the mandibular arch in the edentulous area on both sides (Self-drilling titanium screws: 1.5 mm × 8 mm) and 0.017″ × 0.025″ TMA cantilever uprighting springs with gable bends were engaged to upright 38 and 48 initially, followed by 0.019″ × 0.025″ TMA springs (Figure 5). The left side miniscrew failed twice, and the right side once as the bone density was very low in the edentulous regions. Therefore, the left miniscrew was reinserted in the interradicular area between the premolars to continue the segmental arch mechanics.
Posterior Acrylic Bite Blocks for Intrusion of Maxillary Posterior Teeth.

Miniscrew Implants and TMA Cantilever Springs.

TPA with soldered arms and elastic chains were engaged for the intrusion of the overhanging palatal cusps and palatal tipping of maxillary molars (Figure 6). 38 and 48 were uprighted with the implant-supported TMA cantilever springs (Figure 7). The removable mandibular posterior bite plane was trimmed to accommodate the miniscrew implants. After uprighting 38 and 48, they were protracted on 0.019″ × 0.025″ stainless steel cantilevers with gable bends using active tiebacks from the molars to the miniscrews for three months. Micro-osteoperforations were done mesial to 38 and 48 to accelerate protraction. The bite plane was also trimmed from the posterior end sequentially to allow protraction of the 38 and 48 to the region of 37 and 47. The space closure progressed smoothly. The advantage of the active tiebacks for retraction is optimal low force and good moment to force ratio for favorable translation.
TMA Uprighting Springs and Modified TPA with Soldered Arms.

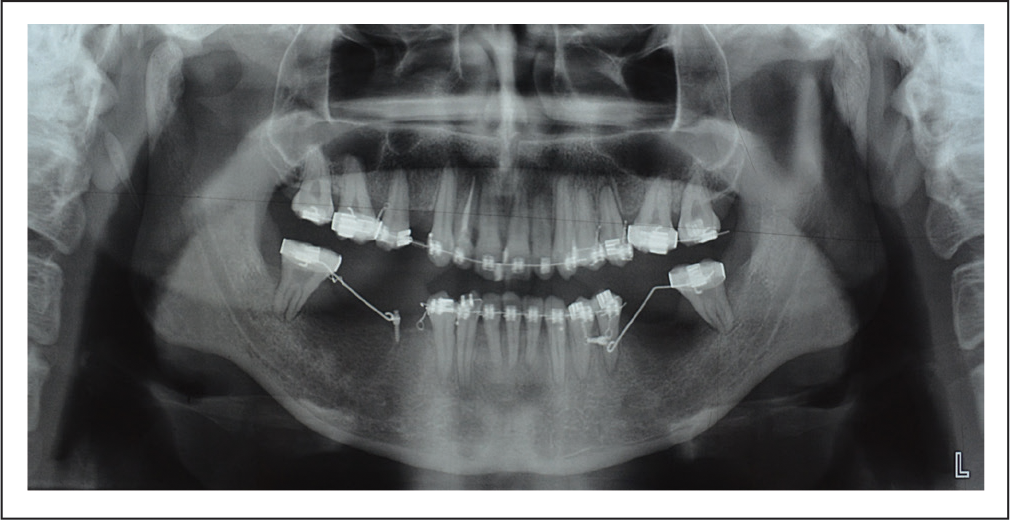
Post Molar Uprighting Orthopantomogram.
Continuous arch mechanics was followed in the maxillary arch. The lacebacks on Niti archwires and active tiebacks from second molars on 0.018″ AJ Wilcock Premium plus archwire and 0.019″ × 0.025″ stainless steel wires were used to gain space for decrowding and retraction of maxillary anterior teeth.
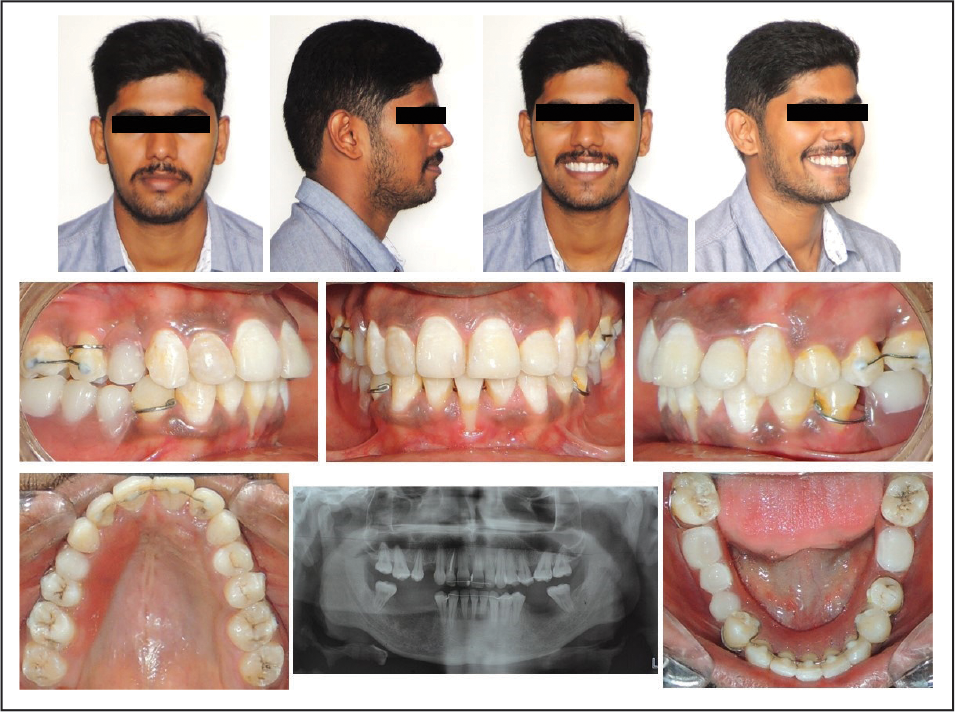
Settling of occlusion was done with 3/16″ elastics on 0.016″ AJ Wilcock Premium plus archwires followed by debonding (Figure 8). Maxillary and mandibular fixed retainers were bonded. The prosthetic replacement with implants was advised. The patient chose the option of removable partial dentures for a short term. The free gingival graft was carried out in relation to 31 posttreatment (Figure 9).
Posttreatment Photographs.

Free Gingival Graft in Relation to 31.

Treatment Results
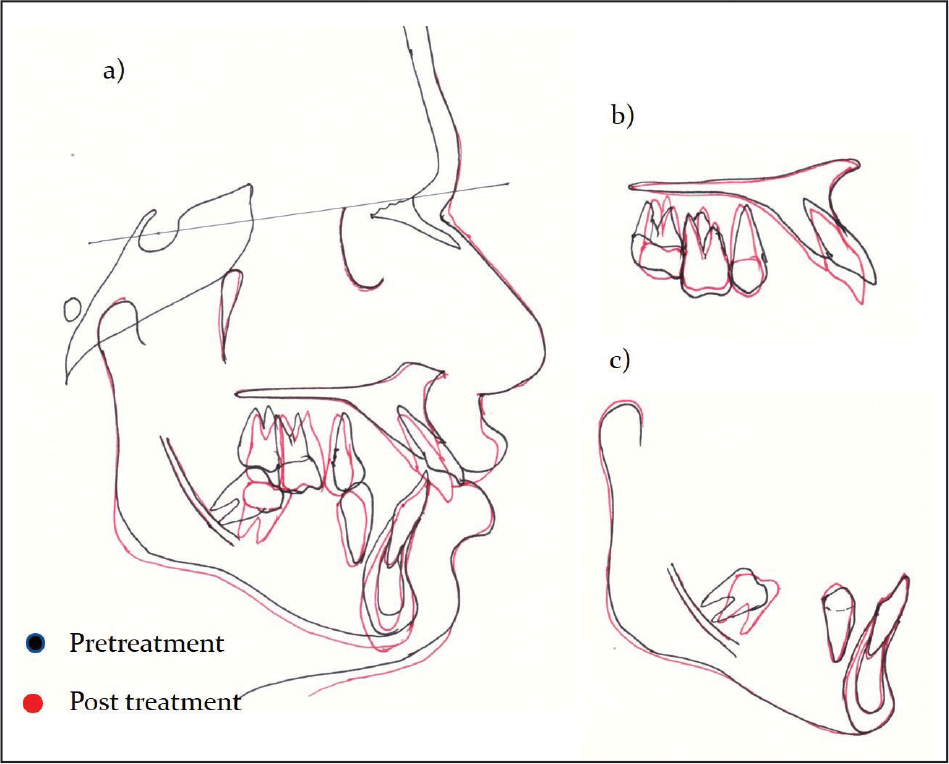
At the end of treatment, the anterior teeth were well aligned, and the patient had a consonant smile arc. 38 and 48 were uprighted and protracted. 38 was uprighted by 39° (pretreatment: 158° long axis to the occlusal plane, post: 119°) and protracted by 5 mm. 48 was uprighted by 55° (pretreatment: 165°, long axis to the occlusal plane, post: 110°). There was good vertical control during treatment. 38 and 48 intruded by 2 mm at the distal cusps and extruded by 3 mm at the mesial cusps. 17 and 27 were intruded by 1 mm. (Table 1, Figures 10 and 11). 38 was protracted by 5 mm, and 48 was protracted by 2 mm. Further protraction had to be stopped because of the patient’s request to complete the treatment at the earliest. Planned incisor position was achieved. The lower incisors did not procline. Class I canine relationship, normal overjet, and overbite were achieved. The pseudopockets in relation to 38 and 48 were eliminated. There was no evidence of root resorption or bone resorption around 38 and 48 because of light forces (Figure 12). The overall treatment duration was 25 months.
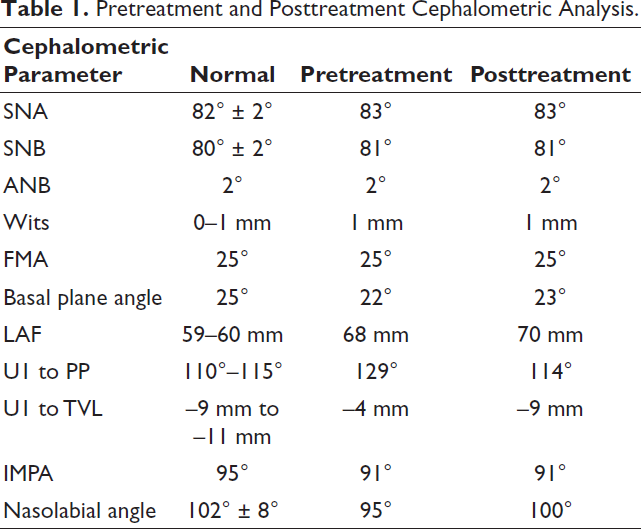
Pretreatment and Posttreatment Cephalometric Analysis
Posttreatment Lateral Cephalogram.

Cephalometric Superimpositions.
Posttreatment Orthopantomogram.
Discussion
The major consideration in managing interdisciplinary cases is treatment planning in conjunction with other specialties. Treatment must be planned with minimal appointments. The adjunct procedures in other disciplines must be combined with orthodontic appointments to reduce patient fatigue. The patient must be provided with all the details of treatment stages and the approximate cost. This will avoid confusion and uncertainty in the patient and ensure better compliance. 10 The patient was informed about the schedule of periodontal and prosthetic procedures.
The unfavorable sequelae of long-standing extraction spaces in adults include tipping adjacent teeth into these spaces. This results in the formation of periodontal pockets, and masticatory forces are not directed along the long axis. 4 To avoid these unfavorable sequelae, the involved teeth must be orthodontically corrected into the right position and inclination.11, 12 Molar uprighting can be done in 2 ways. Uprighting a tipped molar by a distal crown movement leads to increased space for a bridge pontic or implant, whereas uprighting the molar by mesial root movement reduces space and might eliminate the need for a prosthesis. However, this tooth movement can be very difficult and time-consuming to accomplish, especially if the alveolar bone has resorbed in the area where a first molar was extracted many years previously. 13 In the present case, 38 and 48 uprighted by mesial root movement and protracted later (Figure 13).
Biomechanics of Molar Uprighting with TMA Cantilever Spring.
The conventional uprighting mechanics have inadvertent effects of molar extrusion and proclination and intrusion of anterior anchor units. This may worsen the existing periodontal problems like gingival recession and bone resorption. In mutilated cases with multiple missing teeth, the anchorage units are small posing limitations for force levels and biomechanics. The contemporary alternative is miniscrew implants. The miniscrews success rates were good when used as anchorage for molar uprighting.14, 15 The miniscrews can be used as direct and indirect anchorage units for molar uprighting. The biomechanics involved in direct anchorage is simpler compared to indirect anchorage. It also requires less chairside time, only one MI per quadrant, and is more comfortable for the patient. 16 There is extrusion of the molars as they are upright if continuous arch mechanics is followed. The extrusion and other side effects of continuous arch mechanics can be minimized by using direct anchorage from miniscrews. 13
The force levels during orthodontic treatment play a major role, especially in adult patients with periodontal lesions. Melsen et al, 17 stated that the optimum force had not been scientifically defined yet, and higher force levels do not necessarily gain tooth movement. Hence, light orthodontic forces should be applied to teeth to avoid ischemia and local necrosis of the tissues. The magnitude of a moment to upright a molar varies around 1000 g.mm to 1500 g.mm.18 Another study suggests that 1200 g mm is appropriate for molar uprighting. 19
As mentioned above, the type of uprighting spring and wire material play an important part in maintaining optimal force levels. A simple cantilever with a gable bend made of 0.017″ × 0.025″ TMA wire was used to upright 38 and 48 in the present case, as it is very easy to maintain hygiene with this, unlike with the T spring (Figure 13). TMA has higher spring back properties compared to stainless steel and can be deflected twice as much without permanent deformation. Additionally, it releases forces that correspond approximately to half of the forces released by steel alloys under similar activation. 20 In the present case, to maintain low and efficient force levels, the first spring was made with 0.017″ × 0.025″ TMA wire with gable bend followed by 0.019″ × 0.025″ TMA and stainless steel. After treatment, root length was well-preserved and bone resorption was not evident in relation to 38 and 48 because of the low force levels used. The bone density was low pretreatment in relation to the edentulous areas.
The mandibular removable posterior bite plane was used to intrude the supraerupted 15, 17, 25, 27 with the natural masticatory forces. 21 Modified TPA can be used for the intrusion of maxillary molars in adult and mutilated orthodontic patients.22, 23 TPA was activated to achieve the buccal root torque of 17 and 27 in the present case. A very light elastic force from TPA was used to eliminate overhanging palatal cusps of 17 and 27.
The complications encountered during treatment were failure of the miniscrew implants and hindrance to molar protraction because of the knife-edged ridges. The bone density was low, as seen in the pretreatment orthopantomogram. The left side miniscrew failed twice, and the right side once. They were repositioned at new sites, and treatment was continued. The success rate of MI depends on the bone quality, site, and age group of the patient. Park et al 24 reported that the area between the first and second premolars in the mandible of young and adult patients had the highest success rate. There was a significant difference in the success rate of MI and placement site in the mandible. 25 A systematic review conducted by Alharbi et al, 26 showed that the miniscrew diameter, length, design, patient age, and jaw of insertion had minimal effect on the rate of MI failure while the type of gingivae and smoking had a significant effect on failure. In the present case, the patient was periodontally compromised and had resorbed ridges with a low density of the bone that contributed to implant failure. The thin resorbed ridges also hindered the molar protraction. Hence, micro-osteoperforations were done mesial to the 38 and 48 for protraction, as suggested by Alikhani et al, 27 to accelerate tooth movement.
In the present case, 31 was periodontally involved with Miller’s Class III gingival recession pretreatment. Precautions were taken to prevent the worsening of the gingival recession. Very light forces were used. Initially, 0.014″ NiTi archwire was used. The wire was cinched back immediately distal 35 and 44 to prevent proclination. The retraction of 35 and 44 into the edentulous spaces was done by using lacebacks from the miniscrews to gain space for decrowding (Figure 5). To avoid undue stress on 31, the lingually displaced 32 was engaged into the archwire after gaining space by distal movement of 33 and 34. The worsening of the gingival recession started during 0.016” NiTi archwire stage. The patient was advised to maintain good oral hygiene. The lower incisors did not procline posttreatment. In spite of taking the necessary precautions, the worsening of the gingival recession could be because of the distal movement of 31 into the region of the previously extracted periodontally compromised 41.
A free gingival graft was used to cover the defect posttreatment, but there was no significant improvement. This was because of the shrinkage of graft in vertical and horizontal dimensions. A study conducted by Çifcibaşı et al, 28 concluded that the grafts’ shrinkage of vertical and horizontal dimensions was almost equal. They observed that graft shrinkage occurs concurrently in the vertical and horizontal dimensions for 90 days.
Retention after active orthodontic treatment ensures maintenance of correction is achieved. Reorganization of disrupted periodontal tissue takes up to 3 to 4 months until slight mobility observed at appliance removal disappears. 29 In periodontally compromised cases, fixed retainers must be given, which act as splints for stabilization. The retainers must be placed immediately after debonding to avoid relapse. In the present case, fixed retainers were bonded buccally between between 17 and 15, 27 and 25 to avoid opening of the orthodontically closed spaces. The fixed retainers from canine-to-canine were bonded in upper and lower arches. In order to restore the function and maintain spaces until permanent prosthetic replacement with implants, removable partial dentures were given. The overall duration of treatment was 25 months. One-year retention records show that the results are stable (Figure 14). The patient was satisfied with the esthetic and functional rehabilitation.
One Year Retention Photographs.
Conclusion
Miniscrew-supported TMA cantilevers are efficient for uprighting of severely tipped 38 and 48 without extrusion, unlike the conventional mechanics. 18, 28, 38 and 48 with good root forms can be protracted and substituted as 17, 27, 37 and 47 to minimize or eliminate prosthetic rehabilitation.
The keys to ensure efficient restoration of occlusion, function, and esthetics in cases with dentoalveolar collapse are: Appropriate biomechanics to reduce the side effects of uprighting tipped molars, low force levels, appropriate retention, and adjunctive interdisciplinary treatment protocols.
Footnotes
Tooth numbering has been made uniform.
Please see
Acknowledgments
The authors would like to thank their colleagues from departments of Prosthodontics and Periodontics for their help and coordination with multidisciplinary approach to treatment.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.