
Abstract
This paper describes the orthodontic treatment of two cases that were successful in winning the British Orthodontic Society (BOS) Membership in Orthodontics (MOrth) Cases Prize in 2019. The first case describes the management of a 12-year-old girl with a Class II division 2 malocclusion complicated by moderate upper and lower arch crowding, multiple unerupted teeth, restored lower first permanent molars, pseudo-transposition of the lower left lateral incisor and canine, and diminutive upper lateral incisors. Treatment involved a combination of an upper removable appliance followed by upper and lower preadjusted edgewise fixed appliances. Anteroposterior correction and overbite reduction was achieved with triangular Class II elastics with posterior occlusal disengagement. Both upper permanent canines were exposed and aligned, and the diminutive upper incisors built up with resin-based composite. Treatment was completed over a period of 23 months. The second case describes the management of a 13-year-old boy with a Class II division 2 malocclusion complicated by severe upper and lower arch crowding with unerupted UR5, UL4, LR3, rotated LR5, an increased overbite complete to tooth, buccally displaced upper canines and hypoplastic upper first premolars. Treatment involved a first phase of functional appliance therapy, followed by the extraction of UR4, UL4, LL5, LR4 and upper and lower preadjusted edgewise fixed appliances over a 28-month period.
Introduction
The British Orthodontic Society (BOS) Membership in Orthodontics (MOrth) Cases Prize is a national award presented annually. It is in recognition of the two best treated MOrth cases displayed at the BOS Conference. Two cases are presented that were treated during specialist orthodontic training at the Leeds Dental Institute.
Case 1
A fit and healthy 12-year five-month old girl was referred by her general dental practitioner concerned about her ‘crooked and missing teeth’. She presented clinically with a Class II division 2 incisor relationship on a moderate Class II skeletal base with reduced vertical proportions and an increased labio-mental fold and nasolabial angle. Her malocclusion was complicated by moderate crowding in both arches, multiple unerupted teeth, restored lower first permanent molars, pseudo-transposition of the lower left lateral incisor and canine, and diminutive upper lateral incisors. The overbite was increased and complete to tooth.
Extra-oral examination
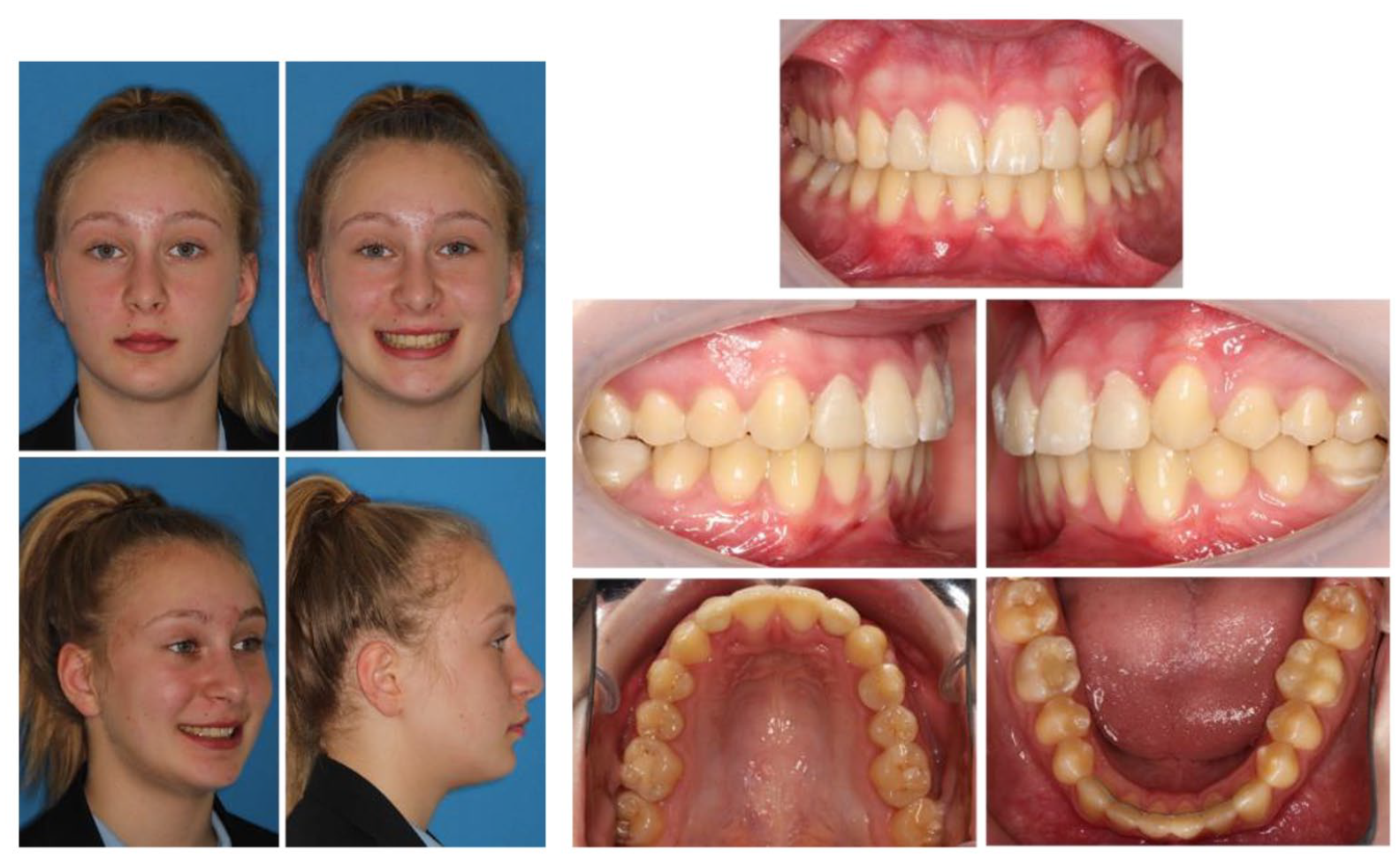
Clinical examination in the anteroposterior (AP) dimension revealed a moderate Class II skeletal base relationship (Figure 1). The profile was convex, with soft tissue A point lying on Zero Meridian and soft tissue pogonion behind it (González-Ulloa, 1962). Vertically, the Frankfort-mandibular planes angle was average and the anterior lower face height reduced. Transverse examination using vertical fifths revealed no significant facial asymmetry. The upper dental centreline was coincident with the midfacial axis.

Case 1 - Pre-treatment extra-oral photographs.
Soft tissue assessment revealed an increased nasolabial angle and increased labio-mental fold. Both upper and lower lips were retrusive in relation to Ricketts’ E-plane (Ricketts, 1981). The lips were competent at rest and there was reduced maxillary incisor show on full smile.
The temporomandibular joint examination was normal with a 1.5 mm mandibular displacement to the left between the retruded contact and intercuspal positions.
Intra-oral examination
The patient was in the mixed dentition with retained maxillary primary canines (Figure 2). Generalised plaque induced gingivitis was noted. There was buccal caries in the upper left primary canine, occlusal caries in the upper right first permanent molar and occlusal caries in the lower left first permanent molar. The lower right first permanent molar was restored and had a history of vital pulpotomy. There were hypoplastic enamel patches on the buccal and palatal aspects of the upper left first premolar. The following teeth were erupted:


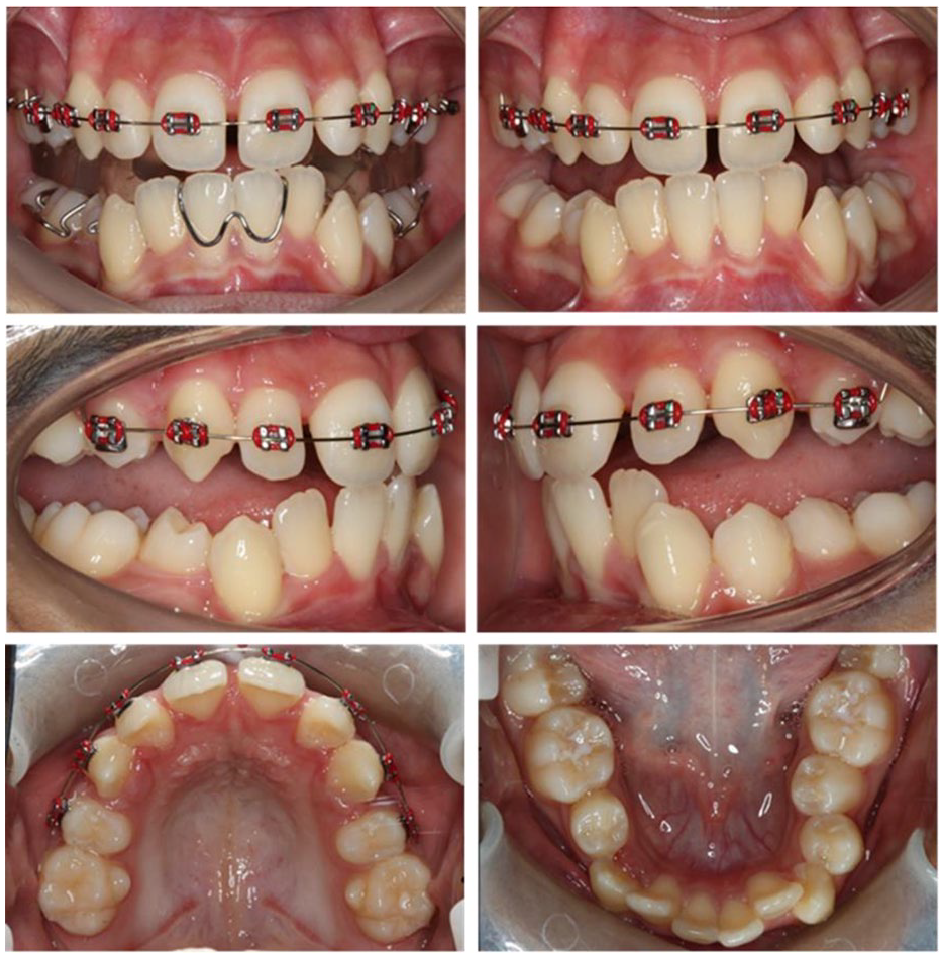
Case 1 - Pre-treatment intra-oral photographs.
There was 6 mm of potential crowding in the lower arch. The upper central incisors were retroclined and the lower lateral incisors were tipped distally and mesio-lingually rotated. At this point the lower left permanent canine crown could be palpated within the buccal sulcus in an anterior position to the lower left lateral incisor. The lower molars were lingually tipped.
There was 5 mm of potential crowding in the upper arch. The upper central incisors were retroclined and the upper lateral incisors diminutive. The maxillary buccal segments were inclined palatally and the upper right permanent canine palpable buccally. The curve of Spee was within normal limits and both arches were U-shaped.
In occlusion, there was an overjet of 3 mm with an overbite that was increased and complete to tooth. The molar relationship was ¼ unit Class II on both sides. The lower dental centreline was 1.5 mm to the right of the upper in intercuspal position. The diminutive upper lateral incisors both had a mesiodistal width of 4 mm.
The dental health component (DHC) of the Index of Orthodontic Treatment Need (IOTN) was 5i and the aesthetic component (AC) was 9 (Brook and Shaw, 1989).
Special tests
Sensibility testing using ethyl chloride and electric pulp testing were carried out on both lower first permanent molars. A reproducible positive response suggested both these teeth were vital. This was repeated throughout the treatment with a normal positive response.
Radiographic examination
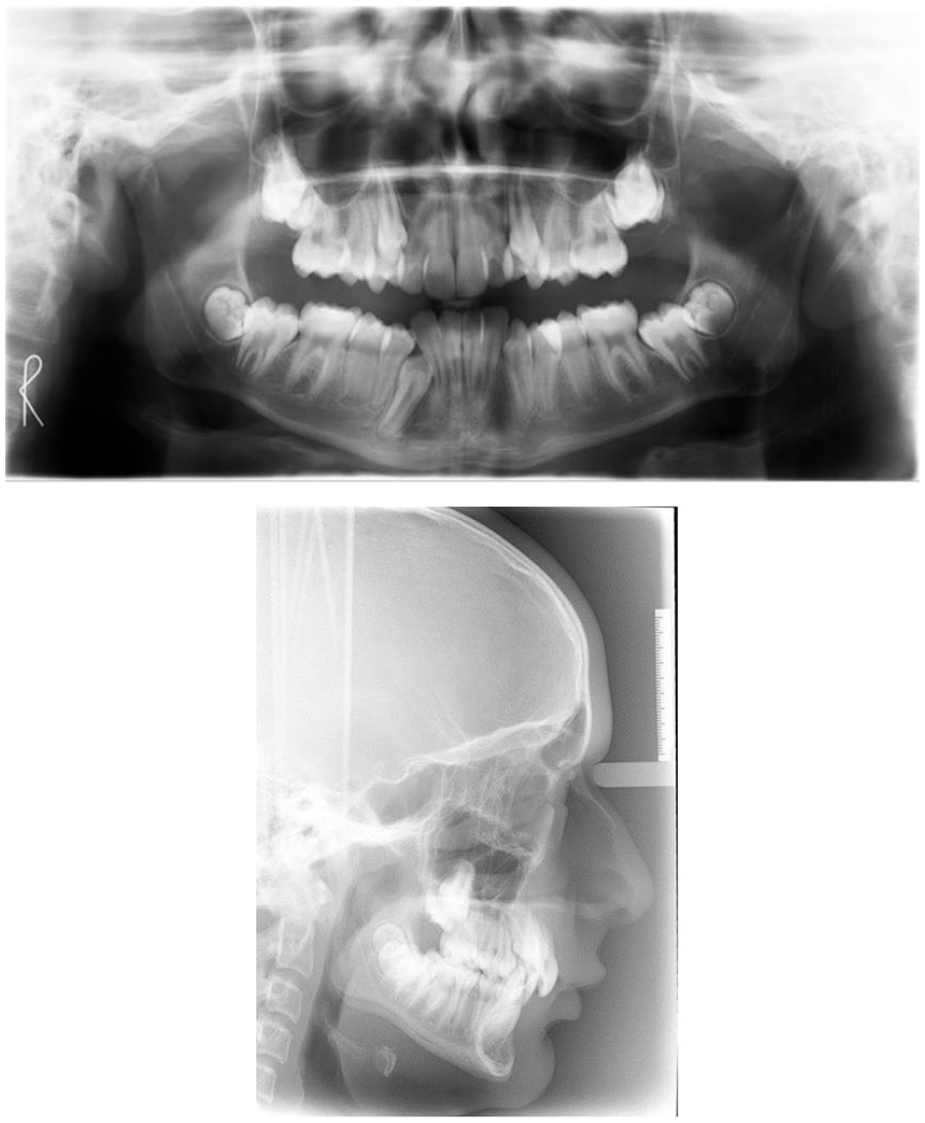
The dental panoramic tomograph (DPT) revealed caries in the lower left first permanent molar and a large restoration in the lower right first permanent molar (Figure 3). The DPT confirmed the presence of multiple unerupted teeth including ectopic position of both maxillary permanent canines. The presence of the upper left, lower left and lower right wisdom teeth could not be confirmed.
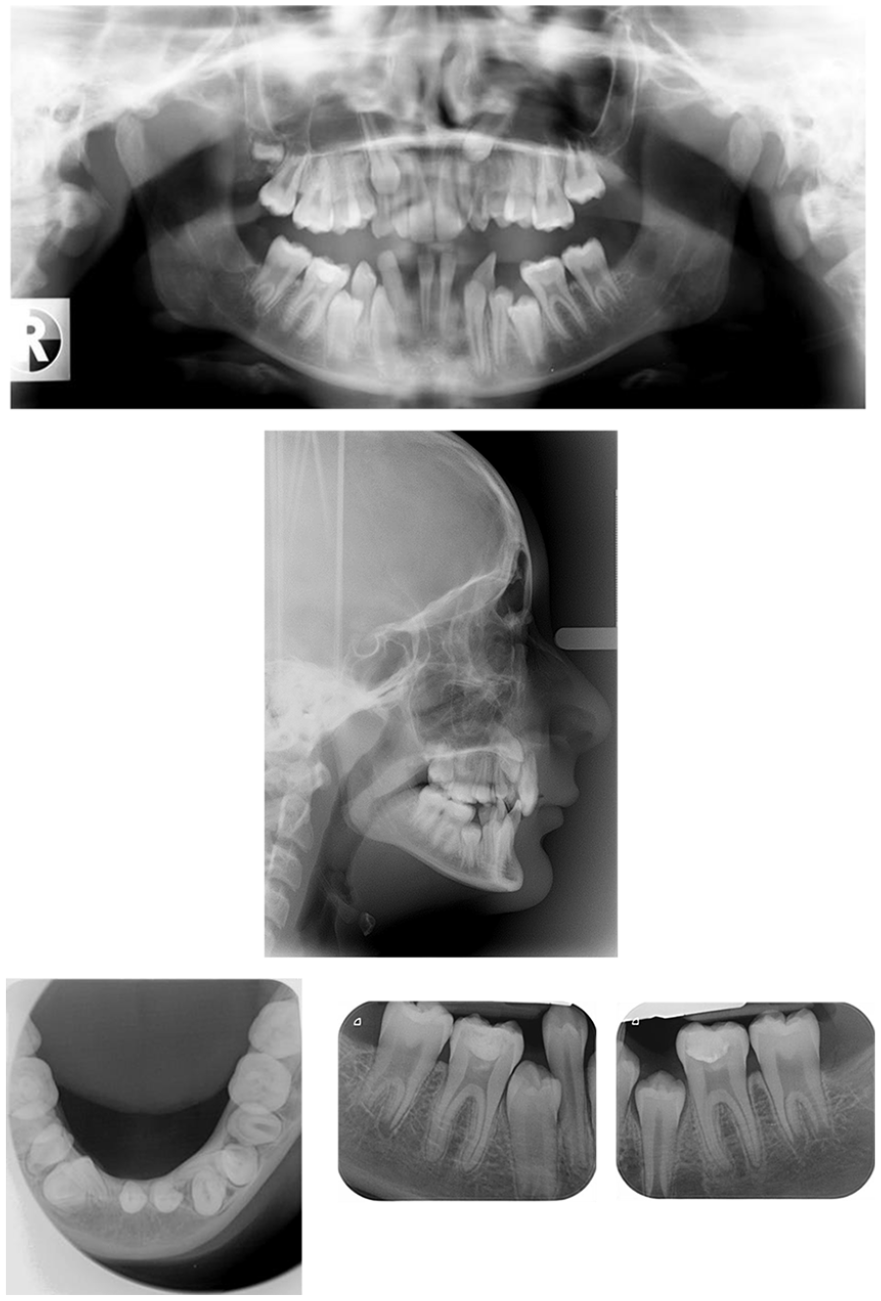
Case 1 - Pre-treatment radiographs.
Analysis of the lateral cephalogram showed that the SNA and SNB values were within normal Caucasian values at 81° and 75°, respectively (Figure 9). The ANB angle of 6° and Wits appraisal of 3.6 mm backed up the clinical findings of a Class II skeletal relationship. The maxillary-mandibular planes angle of 29° was within normal limits and the lower anterior face height proportion was 52%.
The upper central incisors were significantly retroclined at 77° to the maxillary plane. The lower incisors were inclined at 87° to the mandibular plane and the interincisal angle was increased at 168°. The tip of the lower incisor was 4.8 mm behind A-Pogonion and 4.2 mm behind the upper incisor edge-centroid.
The upper and lower lips were both 4.1 mm behind Ricketts E-Plane. This suggested that the lower lip sat behind the most aesthetic position relative to the nose and chin.
A lower standard occlusal radiograph showed a pseudo-transposition of the lower left lateral incisor and unerupted lower left canine with the apex of the lateral incisor mesial to the canine tooth. The root apex of the lower left lateral incisor was lingually positioned and in close proximity to the lingual cortex of the mandible. The lower right lateral incisor was distally tipped with no evidence of transposition.
Two periapical radiographs were taken of the lower first permanent molars to assess for periapical pathology. Both these teeth had large radiopaque coronal restorations with no evidence of periapical pathology.
Problem list
The list of problems was as follows: (1) occlusal caries LL6 and generalised plaque induced gingivitis; (2) multiple unerupted teeth including ectopic UR3 and UL3 and pseudo-transposition of LL3 and LL2; (3) Class II skeletal base relationship; (4) Class II division 2 incisor relationship; (5) moderate lower arch crowding with unerupted LL5, LL4, LL3, LR3 and LR5; (6) moderate upper arch crowding with diminutive UR2 and UL2; (7) increased overbite; and (8) lower centreline 1.5 mm to the right in intercuspal position with 1.5 mm mandibular displacement to the right on closure.
Aims and objectives of treatment
The aims and objects of treatment were as follows: (1) address caries and improve oral hygiene; (2) address ectopic upper permanent canines and pseudo-transposition LL2 and LL3; (3) camouflage the Class II skeletal base relationship; (4) relieve crowding through controlled increase of the arch length; (5) level and align both arches with overbite reduction; (6) obtain Class I incisor, canine and molar relationships; (7) build up diminutive upper lateral incisors; and (8) retain the result.
Treatment plan
The treatment plan was as follows: (1) intensive oral hygiene instruction and diet advice, prescription of 2800 ppm fluoride toothpaste; (2) restoration of caries LL6; (3) extraction of URC and ULC; (4) fitting of upper removable appliance (URA) with flat anterior bite plane and lower preadjusted edgewise fixed appliance (0.022” × 0.028” slot, MBT prescription); (5) fitting of upper fixed appliance; (6) space creation for unerupted maxillary canines alongside triangular Class II elastics with posterior occlusal disengagement; (7) closed exposure maxillary permanent canines; (8) alignment of unerupted teeth; (9) space creation for resin-based composite build-up of UR2 and UL2; (10) finishing and detailing; and (11) retention with mandibular bonded retainer and upper and lower vacuum formed retainers.
Treatment progression
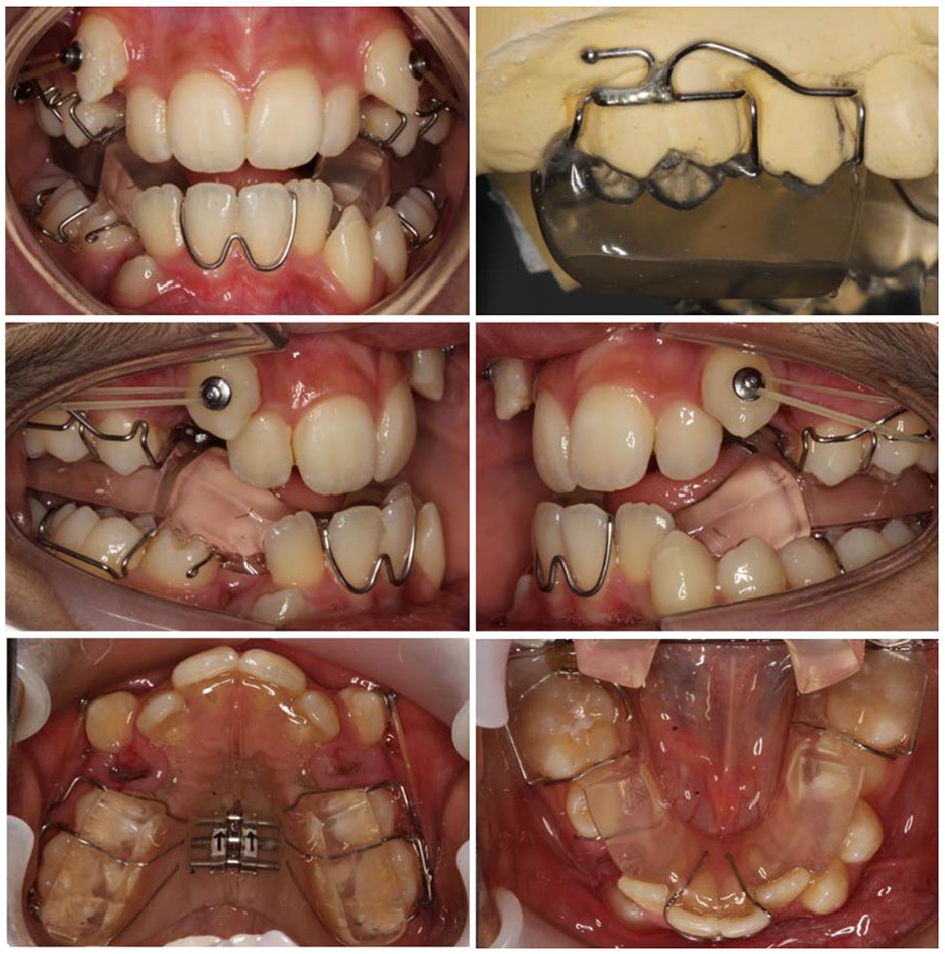
Extraction of both upper primary canines was followed by fitting of an upper removable flat anterior bite plane and bonding of the erupted lower teeth (Figure 4). The arch was bonded with MBT prescription preadjusted edgewise brackets with a 0.022” × 0.028” slot. Stainless-steel closed coil was placed distal to the LL2 on a 0.014” super-elastic nickel-titanium (NiTi) archwire. This helped strengthen the large span of unsupported archwire and helped prevent movement of the lateral incisor into the unerupted LL3. Following improvement in the position of the lower lateral incisors, the upper arch was bonded with careful bracket positioning to prevent unwanted tipping of teeth into the unerupted upper canines. Where teeth had not erupted fully, lower incisor brackets with their smaller base were fitted temporarily and later replaced.

Case 1 - Upper removable appliance flat anterior bite plane. Lower pre-adjusted edgewise fixed appliance. 0.014” super-elastic NiTi. Stainless steel closed coil LL3, LL4 and LL5 area.
The archwires progressed through 0.018” NiTi to a 0.018” and 0.020” A.J. Wilcock Australian wire (Special+) stainless-steel archwire. Glass-ionomer cement was placed on the UR7 and UL7 to disengage the occlusion, push coil was placed in the upper canine positions and Kobayashi ligatures placed on the upper premolars (Figure 5). The patient was instructed to wear triangular Class II elastics (1/4” 4.5 oz). These mechanics provided an anterior and vertical vector of force to correct the buccal segment relationship through tipping of the teeth and correcting the vertical discrepancy through extrusion of the lower molars and alteration of the occlusal place.

Case 1 - GIC UR7 and UL7 to disengage the occlusion. 0.020” stainless steel archwires. Open stainless-steel coil UR3, UL3, LR5. Closed stainless-steel coil LL3, LL4, LL5, LR3.
After this, closed exposure of the upper permanent canines was undertaken and gentle vertical traction was applied via a piggy-back archwire (Figure 6). Following eruption of the unerupted lower canines and premolars, the remaining teeth were bonded (including the second permanent molars). Space was created around the upper lateral incisors to facilitate later build-ups. Eighteen months into treatment, upper and lower 0.019” × 0.025” stainless-steel archwires were placed and Class II intermaxillary elastics (1/4” 3.5 oz) used to complete the Class II correction. A near end of treatment lateral cephalogram taken at this point confirmed acceptable incisor inclination, interincisal angle and edge-centroid relationships accepting that the lower incisors had been proclined to help camouflage the Class II skeletal relationship.
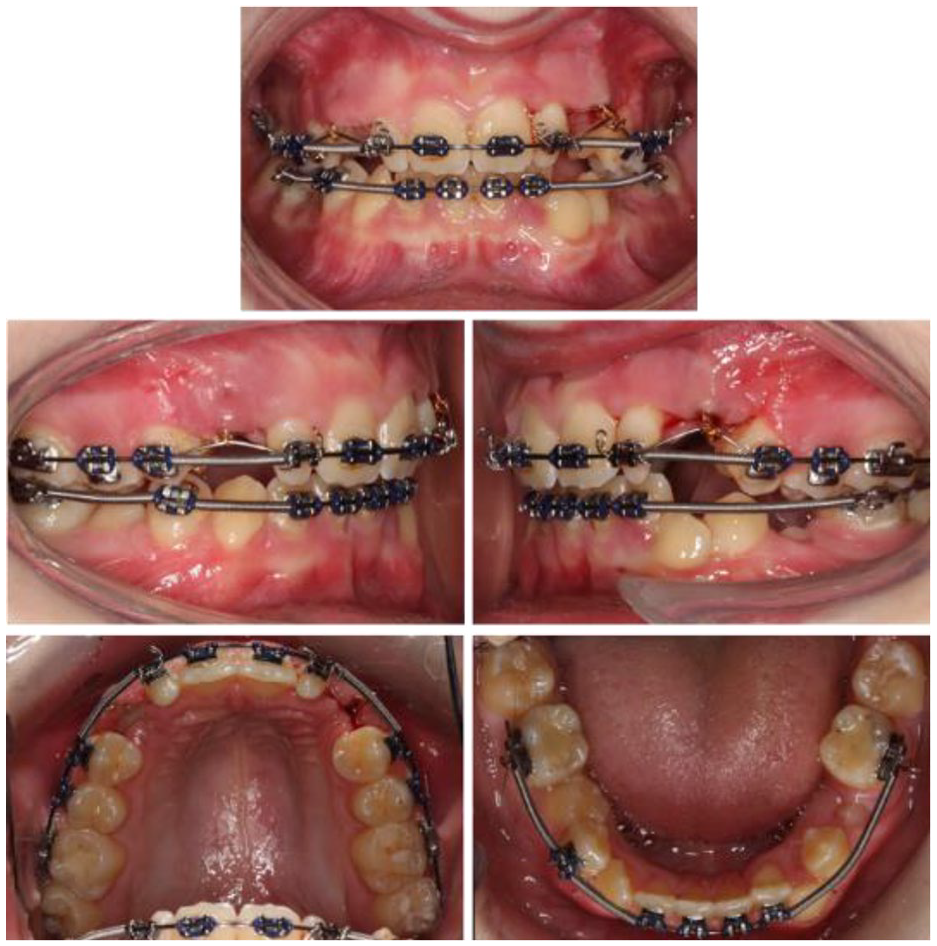
Case 1 - Closed exposure UR3/UL3 and gentle traction with an 0.014” nickel-titanium piggyback archwire. Class II elastics to maintain antero-posterior correction.
Finishing and detailing of the occlusion involved placing third order bends to express torque in individual teeth. Vertical settling elastics were used on a lower 0.018” × 0.025” NiTi archwire to improve interdigitation (Figure 7). Near end of treatment radiographs were taken at 19 months (Figures 8 and 9), and after 23 months of treatment, the appliances were debonded, resin-based composite build-ups of the upper lateral incisors carried out and restoration of the lower left first permanent molar completed (Figure 10).
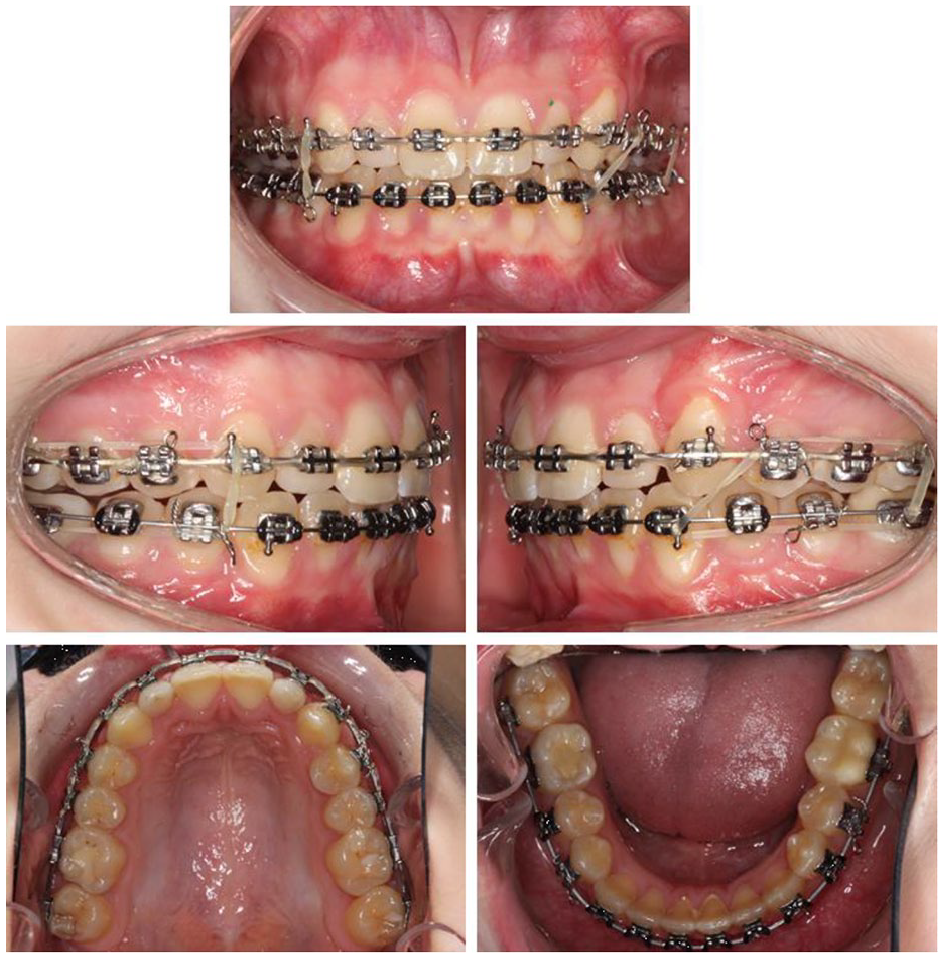
Case 1 - Near end of treatment photographs.
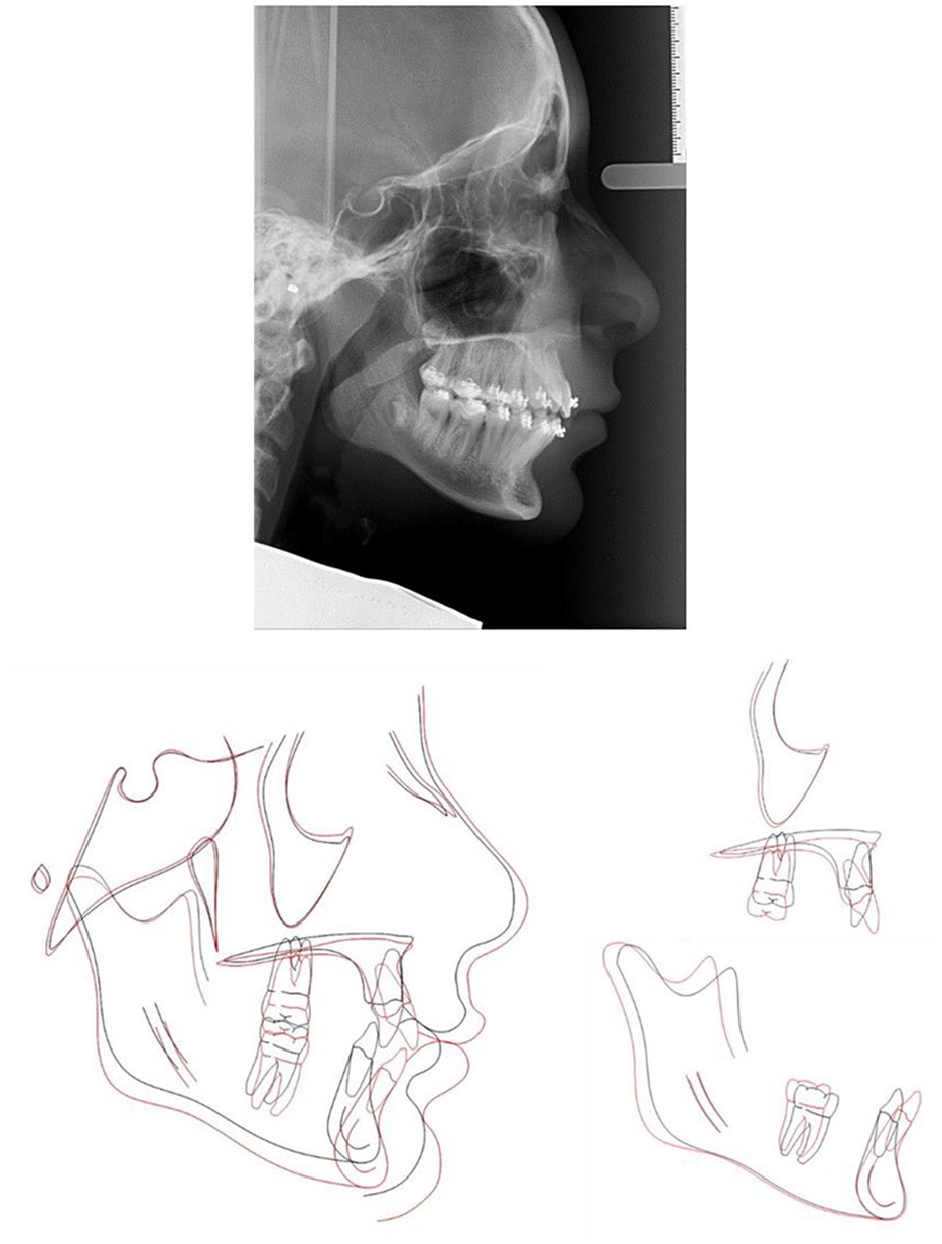
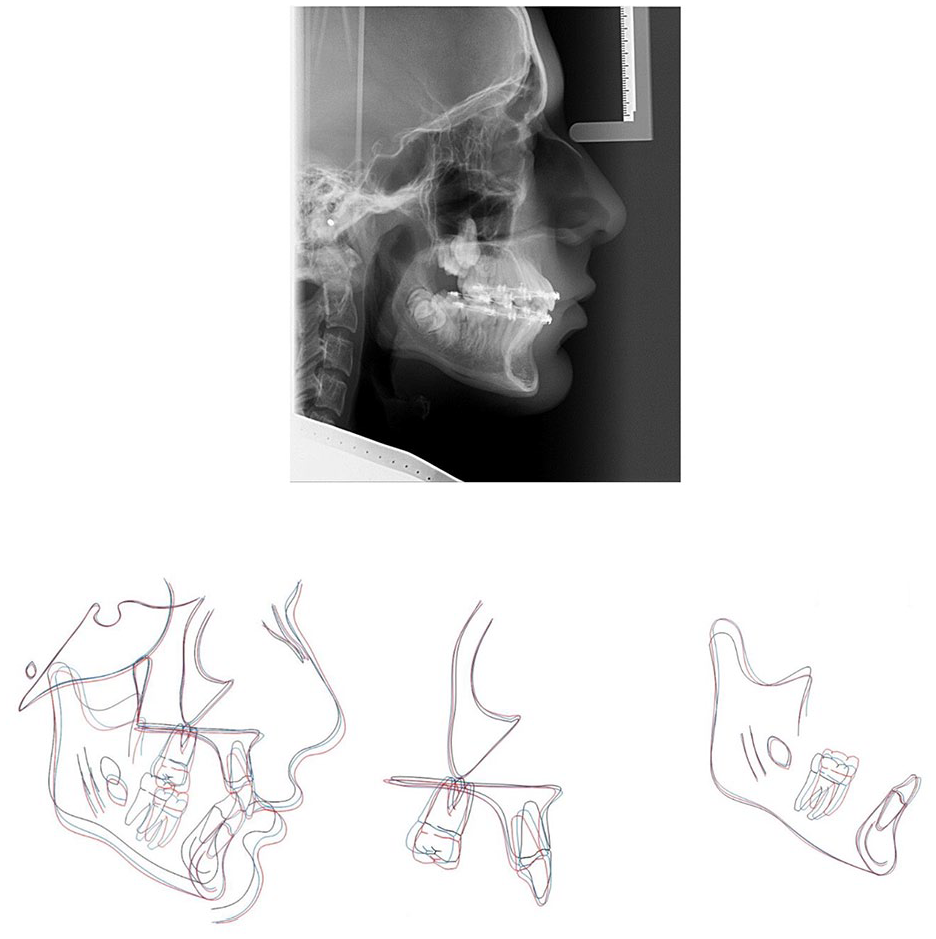
Case 1 - Near end of treatment lateral cephalogram radiograph and cephalometric superimpositions on Bjork’s stable structures (Skieller et al., 1984). Key: Pre-treatment in black and near end of treatment in red.
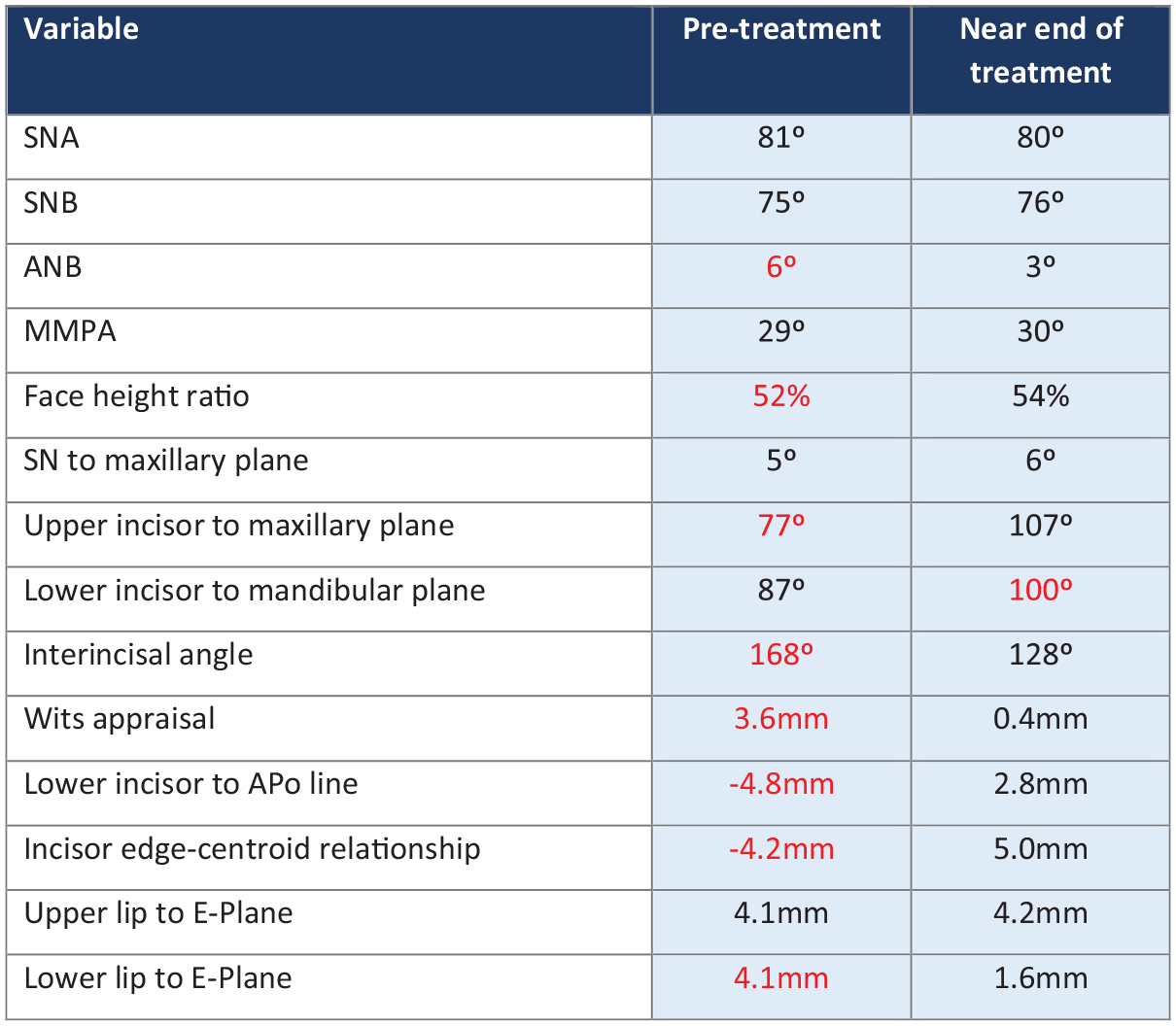
Case 1 - Table showing pre-treatment and near end of treatment lateral cephalogram values. Key: red indicates value outside normal range.
Case 1 - Post-treatment extra- and intra-oral photographs.
Retention involved placement of a lower canine-to-canine coaxial 0.018” × 0.025” stainless-steel bonded retainer with maxillary and mandibular full coverage vacuum-formed retainers.
Critical appraisal
The patient was successfully treated in 23 months. Orthodontic treatment addressed the impacted and unerupted teeth, relieved the crowding and reduced the overbite. The end treatment PAR score of 2 (reduction of 93%) indicated a ‘greatly improved’ occlusal outcome.
Orthodontic treatment was aimed at using an upper removable appliance together with upper and lower preadjusted edgewise fixed appliances on a non-extraction basis to camouflage the Class II skeletal relationship. Use of Class II triangular elastics with posterior occlusal disengagement over a period of approximately six months was used to improve the AP dental relationship. The major benefit of this approach was allowing simultaneous alignment of the teeth, continued eruption of unerupted teeth and reduction of the overbite while maintaining Class II traction. Cephalometric superimposition confirmed favourable skeletal growth during her treatment, which has improved the patient’s profile and has been utilised to correct the patient’s malocclusion.
The post-treatment occlusion is Class I, with acceptable alignment and interdigitation. The patient’s lateral guidance is on the canines without interferences in protrusive or lateral excursions. There has been an improvement in the upper incisor inclination, lower incisor edge-centroid relationship and a reduction in overbite. However, despite placing additional palatal root torque in the archwire, the UL3 remains slightly under-torqued.
There has been recession following proclination of the LL2. This represents a gingival Recession Type 1 (RT1) defect (Cairo et al., 2011). In line with current periodontal guidelines the patient has been instructed to clean with a single tufted brush and will be monitored by the general dental practitioner with repeat measurements and clinical photographs. The mandibular vacuum-formed retainer has also been relieved around the gingival margin in this area.
Both lower first permanent molars are heavily restored but formal discussions with restorative colleagues at the start of treatment suggested a fair prognosis for these teeth. The decision then to maintain these teeth was based on the significant Class II component to the malocclusion, the need to prevent further overbite increase, the need to place a lower fixed appliance early in treatment and the uncertainty of lower third molar presence.
The patient will continue to be reviewed for retainer maintenance and monitored for eventual eruption of the upper right third molar tooth. The resin-based composite build-ups of the upper lateral incisors will require long-term maintenance including smoothing, polishing and repair should the restorations chip. The patient will be reviewed by her general dental practitioner for sensibility testing and radiographic assessment of her lower first permanent molars. If either of these lower first permanent molars lose vitality, then the likely treatment of choice is endodontic treatment followed by cuspal-coverage indirect restoration.
The prognosis for long-term stability of the occlusion is favourable if the suggested retention strategy is followed. The lower incisors have been intentionally proclined through orthodontic treatment and as such there is an increased importance of maintaining the lower bonded retainer.
Case 2
A medically fit and healthy 13-year six-month boy attended in the permanent dentition concerned about his ‘pointy teeth at the sides’. He had a Class II division 2 incisor relationship on a moderate Class II skeletal base with a retrognathic mandible. This was complicated by severe lower arch crowding with unerupted LR3 and rotated LR5, severe upper arch crowding with unerupted upper second permanent molars, buccally displaced upper canines and hypoplastic first premolars.
Extra-oral examination
Clinical examination in the AP dimension revealed a moderate Class II skeletal base relationship (Figure 11). The profile was convex with the soft tissue pogonion lying behind the Zero-Meridian line. Vertically, the Frankfort-mandibular planes angle was reduced and the anterior lower face height was within normal limits. Transverse examination using vertical fifths revealed no significant facial asymmetry.

Case 2 - Pre-treatment extra-oral photographs.
Soft tissue assessment revealed a mildly increased nasolabial angle and marked labio-mental fold. The lips were competent at rest with the lower lip retruded in relation to Ricketts’ E-plane. There was a high lower lip line with partial coverage of the upper central incisors on smiling. The upper incisor show on smiling was reduced due to some natural asymmetry of the lower margin of the patient’s upper lip. A full smile showed adequate width with the second premolars visible. The temporomandibular joint examination was normal.
Intra-oral examination
The patient was in the permanent dentition. Oral hygiene was adequate with no evidence of caries and the soft tissues were healthy (Figure 12). There was 12 mm of crowding in the lower arch. The LR3 was unerupted but palpable in the buccal sulcus and the LR5 was mesiobuccally rotated by 90°. The LR7 had started to erupt.

Case 2 - Pre-treatment intra-oral photographs.
The following teeth were erupted:

There was 17 mm of crowding in the upper arch. Both upper permanent canines were erupting, positioned buccally and excluded from the arch with the UR2 and UR4 in contact. Both upper first premolars had hypoplastic defects. The central incisors were square-shaped and both upper lateral incisors had a reduced mesiodistal width. Despite this, the anterior and overall Bolton ratio was within normal limits at 77.7% and 89.6%, respectively, likely as a result of the large upper central incisors (Bolton, 1958). The curve of Spee was increased and both archforms were U-shaped.
In occlusion, there was a 4-mm overjet with an overbite that was increased and complete to tooth. The molar relationship was ¾ unit Class II on the right and a full-unit Class II on the left. The dental centrelines were coincident with each other. There was a buccal crossbite that affected the UL4.
The DHC of the IOTN was 5i with AC 9.
Radiographic examination
The DPT revealed the presence of all teeth including all four third permanent molars (Figure 13). The LR3 was vertically impacted and there was overlap of the upper second and third molars. There was no obvious caries or other pathology present.
Case 2 - Pre-treatment radiographs.
Analysis of the lateral cephalogram showed an average SNA angle of 78° and a reduced SNB angle of 73° (Figure 19). The ANB angle was 5° suggesting a borderline Class I skeletal relationship. Applying the Eastman correction, the ANB angle increased to 6.5° (Mills, 1987), which along with the Wits appraisal value of 3.3 mm, supported the clinical findings of a Class II AP relationship (Jacobson, 2003).
The maxillary-mandibular planes angle of 25° and lower anterior face height proportion of 55% were within normal limits. The upper incisors were retroclined at 98° and there was an exaggerated upper central incisor collum angle (Woodhouse, 1983). The lower incisor to mandibular plane angle was within normal limits at 96°. The lower incisors were lying 1.2 mm behind the A-Pogonion line and the lower incisor tip was estimated to be behind the upper incisor centroid by 0.5 mm.
Partway through treatment, a cone beam computed tomography (CBCT) scan was carried out to assess the position of the unerupted maxillary second molars. The scan showed vertical impaction of the UR7 and UL7 against the UR8 and UL8, respectively, preventing their eruption.
Problem list
The list of problems is as follows: (1) Class II skeletal base relationship; (2) Class II(2) incisor relationship; (3) increased overbite; (4) severe lower arch crowding with unerupted LR3; (5) severe upper arch crowding; (6) impacted and ectopic UR7 and UL7; and (7) hypoplastic UR4 and UL4.
Aims of treatment
The aims of treatment were as follows: (1) use of a functional appliance to correct the buccal segment relationship, reduce the overbite and increase anchorage during the retraction of the upper permanent canine teeth; (2) relieve crowding through extractions; (3) procline the upper and lower incisors; (4) level and align arches with overbite correction; (5) obtain Class I incisor, canine and molar relationships; (6) monitor unerupted and ectopic UR7 and UL7; and (7) retain the result.
Treatment plan
The treatment plan was as follows: (1) referral to the joint orthodontic-oral surgery multidisciplinary clinic to assess the unerupted maxillary second permanent molars; (2) growth modification with Modified Clark’s Twin Block functional appliance; (3) extraction of UR4, UL4 and LR4; (4) upper sectional preadjusted edgewise fixed appliance (0.022” × 0.028” slot, MBT prescription); (5) extraction of LL5; (6) fitting of full arch upper and lower fixed appliances; (7) supracrestal fiberotomy LR5; (8) finishing and detailing; and (9) dual retention with maxillary and mandibular bonded retainers and upper and lower vacuum formed retainers.
Treatment progression
Treatment was initiated with a modified Clark’s Twin Block functional appliance (Figure 14). The patient was instructed to wear the appliance full time including at mealtimes.
Case 2 - Two months into treatment with the functional appliance in situ and extraction UR4, UL4, LR4 completed.
Once there was clinical evidence of good appliance wear, extraction of the UR4, UL4 and LR4 was requested. The patient was instructed to wear an elastic extending from hooks on the Adams cribs, to buttons bonded to the buccal aspects of both maxillary canines. A gentle force of 70 g per side was used and the elastics changed at least once per day. The patient was instructed to turn the midline expansion screw once per week until horizontal expansion of 3 mm had been achieved.
Once the canines had erupted further and tipped distally, a sectional fixed appliance was fitted to the upper anterior teeth (MBT prescription preadjusted edgewise with 0.022” × 0.028” slot). After approximately seven months, the upper second premolar accessory cribs were removed and the fixed appliance extended further to include these teeth (Figure 15).
Case 2 – Mid-treatment photographs.
A transition phase involved three months of night-only functional appliance wear. A cephalometric radiograph and impressions for study models were taken at this stage.
The transition to upper and lower fixed appliances began at approximately 10 months (Figure 16). Bands were placed on all first permanent molars, the LL5 extracted and carefully selected teeth bonded in the lower arch. An upper 0.017” × 0.025” stainless-steel archwire was used alongside a modified lower 0.018” stainless-steel archwire. This allowed for simultaneous use of de-rotation mechanics around the LR5 and intermaxillary elastics, while reducing potential round-tripping of the lower incisors.
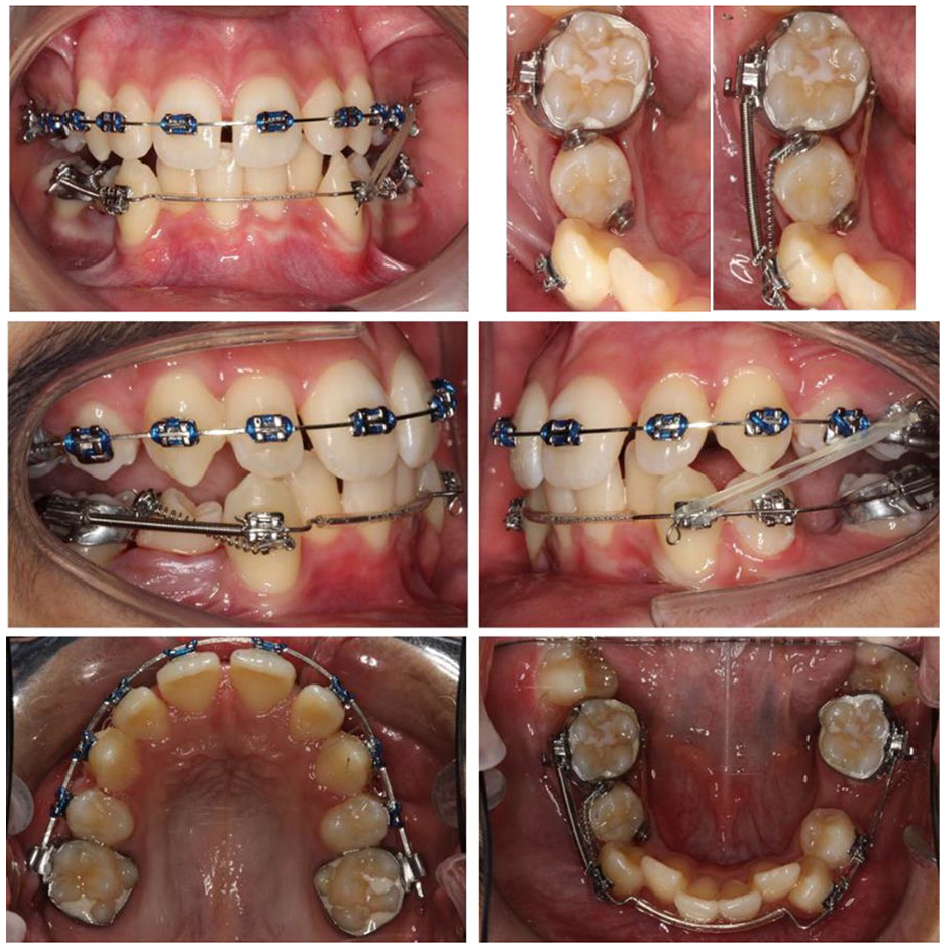
Case 2 – Upper and lower pre-adjusted edgewise fixed appliance. Upper 0.017” x 0.025” and modified lower 0.018” stainless-steel archwires. Pericision LR5. Force couple to de-rotate LR5.
The resulting lateral open bites allowed optimal button positioning on the occluso-buccal and lingual aspects of the LR5 without occlusal interference. A force couple utilising elastic chain and NiTi space closing coil were used along with a soldered lingual cleat on the LR6 and Kobayashi ligature on the LR3 to de-rotate the LR5 (Figure 16, top right). At this same appointment, pericision was carried out under local anaesthetic around the LR5 (Edwards, 1988).
Following de-rotation of the LR5 and relief of lower anterior crowding, the remaining lower teeth were bonded. An initial 0.014” NiTi archwire was followed by 0.018”, 0.017” × 0.025”, 0.018” × 0.025” and 0.019” × 0.025” stainless-steel continuous archwires.
Space closure was completed on an 0.019” × 0.025” stainless-steel archwire using a NiTi space closing coil on the left side, stainless-steel tie-back ligature on the right side, alongside bilateral Class II elastics (5/16”, 4 oz). Individual palatal root torque was placed UR2-UL2 and lingual root torque LL3 (Figure 17).
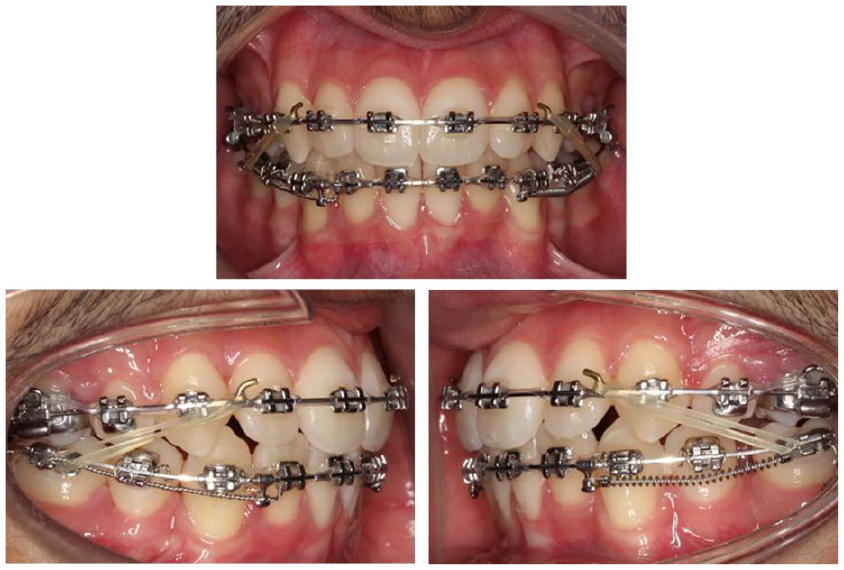
Case 2 - Upper and lower 0.019” x 0.025” stainless steel. Palatal root torque UR2-UL2, lingual root torque LL3. Nickel-titanium spring and tie-back ligature.
Near end of treatment radiographs were taken at 26 months (Figures 18 and 19) and after 28 months of active orthodontic treatment, the appliances were debonded (Figure 20). A Wildcat 0.0195” twistflex bonded retainer was placed with composite resin LL3-LR5 with a view to help resist re-rotation of the LR5. A similar bonded retainer was placed UR2-UL2.
Case 2 - Near end of treatment lateral cephalogram radiograph and cephalometric superimpositions on Bjork’s stable structures (Skieller et al., 1984). Key: Pre-treatment in black, mid-treatment in blue and near end of treatment in red.
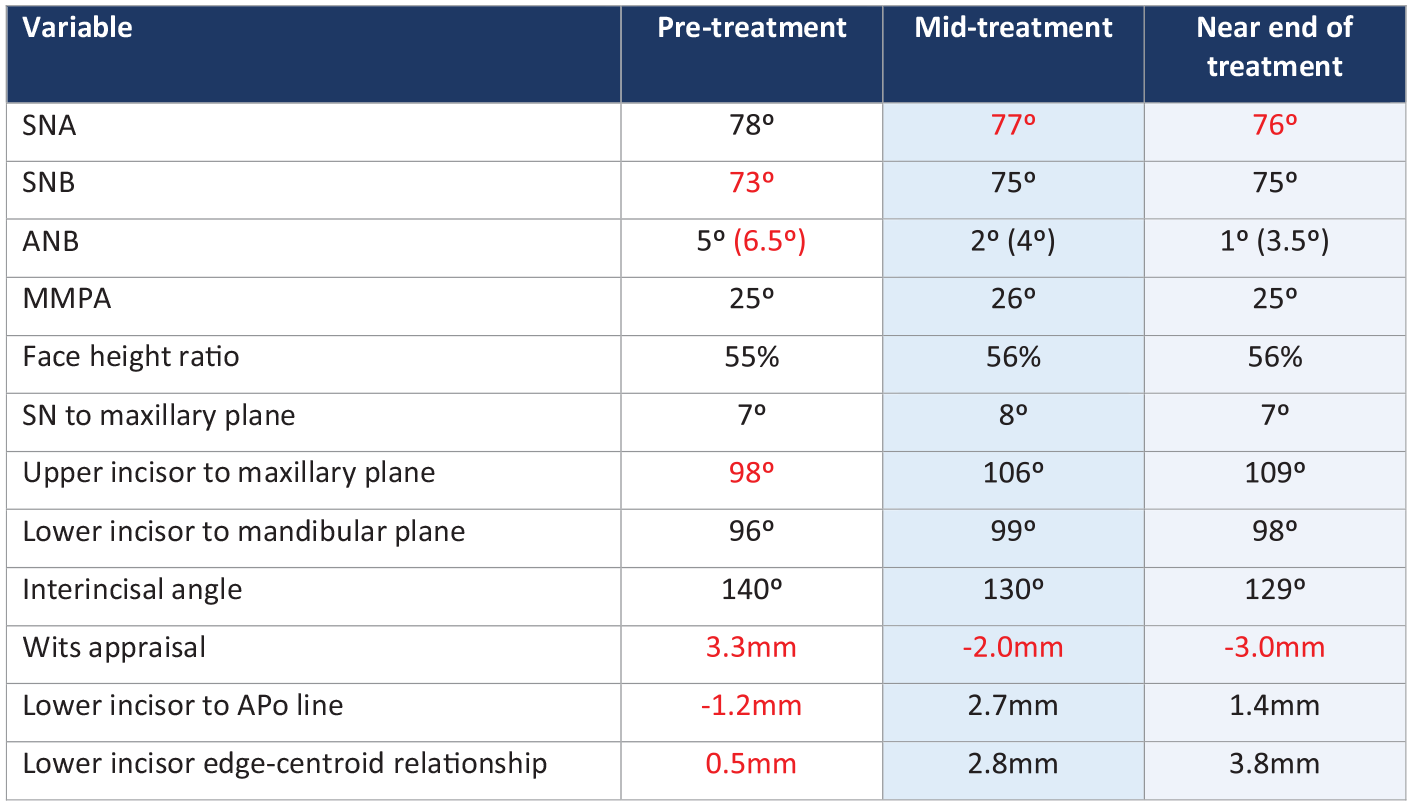
Case 2 - Table showing pre-treatment and near end of treatment lateral cephalogram values. Key: red indicates value outside normal range.
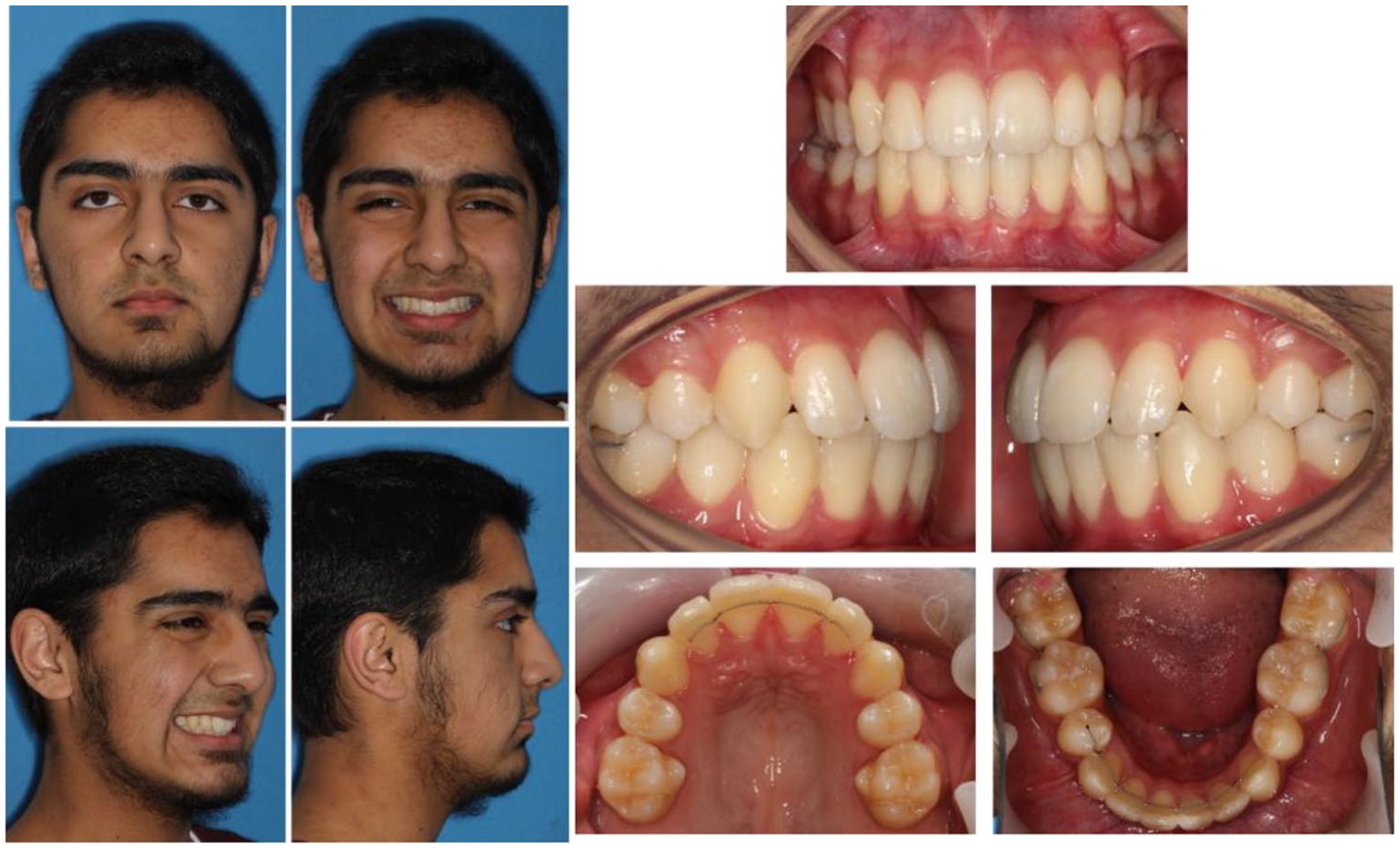
Case 2 - Post-treatment extra- and intra-oral photographs.
Study models taken before debonding showed that both the LL7 and LR7 had no opposing tooth contact. To minimise their potential over-eruption, two short sectional bonded retainers were placed between the LL67 and LR67 and the vacuum-formed retainers were extended to cover these teeth.
These bonded retainers have been reviewed at three months with no issues. The patient will be reviewed again at 12 months, after which the general dental practitioner will be asked to review 12-monthly for debonding, food packing and periodontal pocket formation.
Critical appraisal
This patient was successfully treated in 28 months. Orthodontic treatment relieved the crowding, corrected the buccal segment relationships to Class I and reduced the overbite. The end treatment PAR score of 2 (reduction of 96%) indicates a ‘greatly improved’ treatment outcome. Orthodontic treatment was aimed at optimising potential mandibular growth and correcting the AP relationship using a functional appliance. Cephalometric superimposition suggested some mandibular growth in an AP and vertical direction throughout this phase.
The post-treatment occlusion is Class I with canine guidance bilaterally and no interferences in protrusive or lateral excursions. There is good alignment and interdigitation with minimal change in the mandibular arch width. The centrelines are coincident and correct to the facial midline. There has been an improvement in the upper incisor inclination, lower incisor edge-centroid relationship and a reduction in overbite. The post-treatment extra-oral clinical photographs demonstrate the patient’s improved facial balance and aesthetics, unfurling of the lower lip and appropriate tooth and gingival show.
The patient presented initially with unerupted maxillary second permanent molars. He was seen and discussed on the joint orthodontic-oral surgery multidisciplinary clinic. The CBCT scan report showed vertical impaction of the UR7 against the UR8 and UL7 against the UL8, with both the UR8 and UL8 curving mesio-inferiorly around the UR7 and UL7, respectively, preventing their eruption. Extraction of the unerupted UR8 and UL8 and attempted alignment of the UR7 and UL7 was discussed but declined by the patient.
Alternative extraction patterns were considered including extraction of the upper canines and camouflaging the upper first premolars as canines. The decision to extract the upper first premolars was based on the hypoplastic areas on their buccal aspects and improved overall appearance.
Buccal bonded retainers were placed between the lower first and second molars. This slightly unusual design of bonded retainer was both to help resist relapse of the second molars towards their original lingually tipped position (Figure 16), but also to help resist overeruption. Consideration was given to using a vacuum formed retainer for this purpose; however, it was felt that if may be difficult to achieve sufficient retainer coverage of the second molars, and also even a small amount of relapse may prevent full seating of the removable retainer and result in further relapse.
The patient has been advised to wear his vacuum-formed retainers every night and will continue to be reviewed for eruption of the upper second and all third molar teeth.
Footnotes
Acknowledgements
I would like to thank all my supervisors at the Leeds Dental Institute and at St Lukes Hospital, Bradford for the clinical and academic training I received during my specialist registrar training. In particular, I want to thank Mr Trevor Hodge (Case 1) and Mr David Morris (Case 2) who supervised the management of these two patients at Leeds. Finally, thank you to Align Technology for their generous sponsorship of this prize.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.