
Abstract
While the free movement of people is one of the cornerstones of the European integration project, a pressing question remains whether public support depends on who is moving. Against the backdrop of increasing debates on the development of a European Health Union, this study focuses on the case of patient mobility and compares support levels to those of student and worker mobility rights. To this end, the study draws on an original survey conducted among 6000 respondents in Germany. The results reveal that patients are less supported than students and workers, both for incoming and outgoing mobility. We also find evidence of differentiated drivers of free movement attitudes, as a higher socio-economic status increases support for student and worker mobility but not for patient mobility.
Introduction
The free movement of people represents one of the fundamental freedoms of the internal market of the European Union (EU; Bauböck, 2019; Carrera, 2005; Delhey et al., 2019 ; Favell, 2008; Recchi, 2015). This principle allows citizens of EU member states to move freely across borders for various purposes, for example, work, leisure, studying, and medical treatment and healthcare services. While extensive research has focussed on labour mobility (Galgoczi et al., 2013; Martinsen and Pons Rotger, 2017; Ruhs and Palme, 2018 ) and student mobility (Felder and Tamtik, 2023; Gordon and Jallade, 1996; Mitchell, 2012), the phenomenon of patient mobility received far less attention in the literature so far. This is a significant research gap because patients can make use of their mobility rights to access core social services of the welfare state, contributing to the fact that patient mobility has been in the political spotlight several times over the past years. For example, the Brexit campaign has framed medical tourism in the EU as a threat to the public National Health Service (NHS) in the UK. Furthermore, the COVID-19 pandemic has sparked calls for the creation of a ‘European Health Union’. 1 This can be seen as a starting point towards more EU integration in health (Brooks and Geyer, 2020; Mary, 2020; Nabbe and Brand, 2021) and raised questions of transnational solidarity in the case of medical support (Baute and De Ruijter, 2022; Heermann et al., 2023). These events highlight that debates about the future of national healthcare systems can no longer neglect the European dimension, despite the relatively small share of European citizens who effectively engage in cross-border healthcare. According to Eurobarometer data, about 5% of people living in the EU received medical treatment in another EU country in the last 12 months (European Commission, 2015), but for this group of people, it remains unclear whether seeking medical treatment was the prime motivation for border crossing or not. 2 Comparatively speaking, the share of mobile EU workers comprises 4% of total employment in the EU (Eurostat, 2020), while the share of mobile EU students enrolled in tertiary education in the EU amounts to 2.3% (Eurostat, 2024).
Against this background, a pressing question is whether patient mobility enjoys similar levels of public support compared to more established types of intra-EU mobility, such as worker and student mobility. This question touches on different subfields, such as welfare attitudes, welfare chauvinism (i.e., the opposition towards social rights for immigrants) and EU support. However, most related studies have predominantly focused on support for the general principle of the free movement of people (Karstens, 2020a; Lind and Meltzer, 2021; Lutz and Karstens, 2021; Vasilopoulou and Talving, 2018). Some studies exclusively focus on worker mobility (Ferrera and Pellegata, 2018; Karstens, 2020b; Mårtensson et al., 2023); only a few studies directly compare different mobile groups that can exercise their right to free movement (Sojka et al., 2023), but still do not include patients in this comparison. In addition, past studies often focus on the perspective of incoming mobility (Ferrera and Pellegata, 2018; Gerhards, Lengfeld and Dilger, 2021; Mårtensson et al., 2023), thereby ignoring that the free movement of people comprises both incoming and outgoing mobility rights (Lind and Meltzer, 2020; Lutz, 2020; Sojka et al., 2023). The absence of more systematic comparisons across mobile groups is a significant research gap, since it is well-established in the literature that support for (social) EU policies is multi-dimensional and depends on the policy at stake (Baute et al., 2018; Beetsma et al., 2022; Gerhards et al., 2019). In summary, it remains unclear to what extent public support for the free movement of people depends on who is moving as well as the direction of mobility (incoming or outgoing). In order to arrive at a comprehensive understanding of public support for the development of a more integrated European (Health) Union, it is imperative to broaden the scope of analysis.
In order to do so, this article addresses the following research question: (1) How does support for patient mobility compare to support for student and worker mobility? (2) Does support differ for incoming and outgoing patient mobility? and (3) Which factors determine support for patient mobility? The contribution of this article to the existing literature is threefold: First, our study clarifies to what extent support for the free movement of people depends on the group of ‘movers’ by providing for the first time a direct comparison of public support for patient, student and worker mobility rights. These three groups hold very different and specific motivations for taking up mobility – namely for the purpose of medical treatment (patients), education (students) and employment (workers). Hence, their mobility provides them access to core social services of national welfare states such as healthcare, the education system or labour market policies. However, we argue that these three mobile groups fundamentally differ in their reciprocal relationship with the welfare state of the destination country. Accordingly, this study analyses to what extent public support for freedom of movement varies across these three mobile groups. Second, the study takes into account the dual nature of free movement rights by integrating the perspective of incoming and outgoing mobility as two sides of the same coin. By doing so, our study recognises that patterns of public support could differ between the two as outgoing mobility can be thought of as social rights for natives, whereas incoming mobility refers to rights for citizens from other EU countries. Third, the study identifies whether the determinants of support for patient mobility are domain-specific or similar to student and worker mobility. Hereby, we focus on the role of objective indicators of socio-economic status as well as perceptions of relative deprivation of opportunities to valuable resources in society (i.e., medical treatment, education and employment).
To test our hypotheses, novel survey data were collected in January 2023 among a sample of 6000 respondents in Germany. To briefly foreshadow our main findings, we show that patient mobility is less supported than student and worker mobility, both when we look at incoming and outgoing mobility. Even though outgoing mobility is generally more supported than incoming mobility, the differences are relatively small. Social-structural variables such as education, income and employment status matter to a lesser extent in shaping support for patient mobility than for student and worker mobility. Overall, these findings demonstrate that patient mobility deserves more attention in current academic debates.
Patients on the move: Patient mobility in the EU
The Treaty of Rome of 1957 laid the groundwork for the free movement of people, goods, services and capital. As such, patient mobility was conceptually present in the early principles of the free movement of people within the European Union and its institutional predecessors. Overall, there are three different ways of accessing cross-border patient mobility for EU citizens (Berki, 2018): First, it includes access to healthcare in the member state of origin when residing in another member state. Second, it includes access to necessary healthcare during a temporary stay outside the member state of residence. 3 Third, it includes access to planned healthcare outside the member state of residence. We focus in this article on the third type of patient mobility, namely those instances whereby EU citizens employ their mobility rights only to intentionally seek and obtain medical treatment in another member state while being aware of the fact that the first two types of mobility also play a significant role in cross-border patient mobility. EU regulations ensure that patients travelling to another EU country for medical care will enjoy equal treatment with the citizens of the country in which they are treated. However, free movement rights have a dual nature – including the right to exit and the right to entry – and thus do not only involve rights in the destination country. The set of social rights permits patients to have their medical expenses reimbursed when having been treated in another member state (Börner, 2020). If they are entitled to that healthcare at home, then they will be reimbursed by their home country. Their reimbursement will be up to the cost of that treatment at home. Thus, EU citizens have the right to receive healthcare in any EU country and to be partially or fully reimbursed by their home country. To guarantee this fundamental right, the EU utilises different legislative instruments, including Directive 2011/24/EU and the Social Security Regulations (EC) 883/2004 and 987/2009, which provide the legal framework for the operation of reimbursements of the costs of cross-border healthcare in the EU. In some cases, patients may need to seek authorization before travelling for treatment, which indicates that national governments can exert some control over patients’ right to exit (Finotelli, 2021).
While there is a lack of accurate data on patient mobility in the European Union, healthcare expenditure for treatments abroad in relation to total health expenditure is currently relatively small (European Commission, 2024a). In spite of so far limited actual patient mobility, indicative evidence from the Eurobarometer shows that Europeans are quite divided on their cross-border healthcare rights. In a survey from 2014 (European Commission, 2015), 33% of the respondents in the EU28 replied that they would be willing to travel to another EU member state to receive medical treatment, with a further 16% spontaneously stating that it depends on the EU country or on the type of medical treatment.
Various motivations exist for why patients travel abroad for healthcare, including perceived quality, affordability, availability – both in terms of quantity and type of treatment – and familiarity (Glinos et al., 2010). However, many obstacles may be in place for patients seeking treatment in another EU country, including language barriers and a lack of reliable information on cross-border healthcare rights among patients. According to Eurobarometer data, about half of Europeans feel informed about their reimbursement rights for domestic healthcare, while only 17% feel knowledgeable about rights for cross-border healthcare (European Commission, 2015). This significant knowledge gap may prevent European citizens from using the rights which they are entitled to under EU law. Moreover, these insights suggest that misperceptions exist about the rights of EU patients travelling for medical treatment, potentially with many wrongly assuming that EU mobile patients exploit the domestic healthcare system by receiving free care.
Patient mobility and the limits of solidarity
This article aims to dive deeper into the public opinion on patient mobility and how it compares to public opinion towards student and worker mobility. The issue of patient mobility and solidarity can be approached from various perspectives within the field. Such attitudes are related to different welfare states and welfare policies, to welfare policies towards different immigrant groups and to attitudes towards immigrants in the EU. A useful starting point to dive into this literature is the deservingness theory (Van Oorschot, 2006). According to this theory, along with related empirical studies, the sick and disabled are typically considered the most deserving group in terms of government support (Jensen and Petersen, 2017). This is because they are seen as having less control over their situation – unlike other groups such as the unemployed. The argument is supported by studies that find strong support for healthcare policies on the national level (Busemeyer, 2023; Jensen and Petersen, 2017; Missinne et al., 2013) as well as high levels of public support for healthcare solidarity in the EU (Baute and De Ruijter, 2022; Heermann et al., 2023). Research focusing on public attitudes towards different social rights of mobile EU workers demonstrates that providing access to healthcare is more widely supported compared to access to many other social policies, including education, childcare, social housing or unemployment benefits (Eick and Larsen, 2022). This finding is remarkable as studies on social rights for immigrants more generally usually show significant levels of opposition, in the literature known as welfare chauvinism (Van der Waal et al., 2013). However, the study by Eick and Larsen (2022) was not focused on patients per se and also did not examine outgoing mobility, which this article addresses.
Based on the significant evidence showing the high level of support for healthcare, rights for patient mobility may also be strongly supported by the public. However, there are good reasons to expect patient mobility to be less supported compared to student and worker mobility. Here we are moving more to the studies on the European Union, where the free movement of patients is considered to be a manifestation of deeper integration and solidarity among EU member states (Béland and Zarzeczny, 2018). Therefore, patient mobility has implications for national solidarity as national healthcare systems can come under pressure in case of high inflows and outflows of patients (Vollaard, 2004: 292), such that citizens may want to avoid exploitation of health services and increasing health expenditures for the reimbursement of treatments abroad. Focussing on the economic perspective, we argue that citizens may be less supportive of the notion of freedom of movement for patients compared to workers and students because of the lack of a reciprocal relationship between mobile patients and the host country for their medical treatment. 4 If foreign patients obtain healthcare, the question of financing instantly arises. While the costs of medical treatment of foreign patients are indeed financed by the health insurance of their home country and/or out-of-pocket payments, 5 mobile patients do not contribute directly to the broader ‘health infrastructure’ of the host country and they typically leave after they receive the medical treatment. In other words, mobile patients consume valuable healthcare resources without participating in the risk- and cost-sharing arrangements that underlie the host country's healthcare system, which is typically funded through general taxation or insurance contributions. Given that financial, technical and human resources in the healthcare sector are often limited, satisfying increasing needs for healthcare resulting from patient inflows may be perceived as a welfare burden rather than as a market opportunity.
As a result, patient mobility may be perceived as primarily benefiting the patient, who gains access to a wider range of treatment options, with little contribution to the host country. Such concerns align with broader debates on ‘medical tourism,’ a global phenomenon in which individuals travel to other countries specifically to obtain medical care. The underlying image of medical tourism is one of patients behaving like consumers seeking the best medical treatment at the most favourable reimbursement rate.
By contrast, the mobility of workers and students may receive more support because these groups contribute something to the host country (in line with the reciprocity criterion in the deservingness literature, cf. Van Oorschot [2006]). With regard to labour mobility, workers contribute to the economy and pay into the national tax system of the host country. Such a reciprocal relationship between mobile workers and the host country may be perceived in a positive light, boosting support for worker mobility (Mewes and Mau, 2013; Van der Waal et al., 2013). Student mobility, in turn, provides access to a broader range of study programs, including those of potentially higher quality that may not be available in one's home country. Both patient and student mobility provide access to services, rather than in-cash benefits or jobs. Therefore, delivery depends on the country of destination and its (by nature limited) capacity. However, beyond individual benefits, student mobility in particular can be seen as a type of mobility that may generate economic benefits for the broader society. More specifically, students may stay in the country after graduation, contributing to the workforce in the host country, further strengthening the reciprocal relationship between mobile students and national institutions.
The literature demonstrates that reciprocity is a cornerstone in the European solidarity debate. For example, empirical studies have shown that reciprocity is an important driver in support of European unemployment risk-sharing (Baute et al., 2022 ). The fact that workers and student mobility are characterised by a strong reciprocal nature may also explain why student and work-related immigration are supported more strongly than immigration linked to family reunification or war (Boomgaarden and Meltzer, 2021). Other studies showing that deservingness perceptions in healthcare depend on the identity (migrant status) of the recipient suggest that citizens are sensitive to reciprocity in healthcare systems, too (Eick and Larsen, 2022; Gandenberger et al., 2023 ; Hrast et al., 2018; Knotz et al., 2021). Finally, Sojka et al. (2023) found among respondents in the UK that support for welfare rights is significantly lower, both for incoming and outgoing mobility, than support for the right to work. Although patients do not take up welfare benefits, they may, similarly, be perceived as needy and reciprocating to a lower degree compared to workers and students.
Support for patient mobility is lower than support for student (H1a) and worker (H1b) mobility.
This article also aims to highlight the dual nature of freedom of movement rights in the EU, consisting of ingoing and outgoing mobility rights. The right to exit (outgoing mobility) enables individuals from a given host country to take up opportunities for work, study or seek medical treatment in other EU member states. At the same time, the right to entry (incoming mobility) ensures that access to employment, education and medical care is granted to citizens from other EU countries and can no longer be restricted to the national community. Due to the reciprocity of mobility rights between EU member states, the free movement can thus be studied from a dual perspective of outgoing and incoming mobility.
There are good reasons to expect that outgoing and incoming patient mobility rights enjoy different levels of public support. More specifically, we expect that citizens are generally more supportive of outgoing mobility rights compared to incoming mobility rights. This is because, from a self-interest perspective, outgoing mobility rights enlarge citizens’ opportunities to profit from foreign healthcare systems, labour markets and education systems, amongst others. In the healthcare area, free movement rights benefited COVID-19 patients who needed critical support and were transported to other EU member states for medical treatment (Medeiros et al., 2021 ). Similarly, during the Eurozone crisis, migration flows from South to North Europe significantly increased, as unemployment rates peaked in the South and many were seeking employment opportunities in countries that were less adversely affected by the financial crisis (Lafleur and Stanek, 2017). Furthermore, students across the EU can benefit from educational programs abroad, which significantly increases the range of higher education programs they have at their disposal. By contrast, the incoming mobility perspective may trigger perceptions of increased competition for scarce resources that societies provide and which determine one's life chances. This argument is based on the vast literature on anti-immigrant and welfare chauvinist attitudes in the EU (e.g., Hainmueller and Hiscox, 2006; Lutz, 2020; Van der Waal et al., 2013). The argument is particularly relevant related to healthcare, as during the COVID-19 crisis shortages in medical equipment, hospital beds and health workers threatened the lives of European patients. To the extent that access to employment as well as social benefits and services can no longer be restricted to the national community, incoming mobility of students, workers and patients could be perceived as a threat rather than an opportunity to the economy and national welfare states. In summary, European citizens may consider outgoing mobility as an opportunity, while incoming mobility may be perceived as a threat. Therefore, from a self-interest perspective, support for outgoing mobility rights should generally be higher than support for incoming mobility rights.
A few attitudinal studies explored this double nature of the freedom of movement. First, Sojka et al. (2023) studied public support for the right to live, work, do business and access welfare in the UK/EU for EU citizens on the one hand and UK citizens on the other hand as part of the Brexit deal. They find that the levels of support for UK citizens’ rights in the EU are slightly lower on all four rights (between 1.3 and 4.4 percentage points), although the authors interpret these differences as evidence of a high degree of congruence. Second, Lutz (2020) studied the tension between citizens’ own mobility rights and the mobility rights of citizens from other EU countries using both observational data and a survey experiment across the EU28. The observational data from the Eurobarometer 2016 shows that support for free movement in general is slightly higher (3 to 5 percentage points) compared to support for incoming mobility rights of EU citizens in respondents’ country. However, in a survey experiment, Lutz applied a split sample for an outgoing and incoming mobility treatment. 6 This design is less prone to social desirability bias compared to observational survey items and revealed a much larger gap (of 14.4 percentage points) in support between incoming and outgoing mobility rights. Third, Lind and Meltzer (2021), drawing on a six-country panel study (Germany, Hungary, Poland, Spain, Sweden, United Kingdom), also find stronger support for outgoing than for incoming mobility in all countries. 7 More generally, literature on welfare chauvinism would also strongly support the argument that social rights for immigrants are much more contested than social rights for natives (Eick and Larsen, 2022; Mewes and Mau, 2013; Reeskens and Van der Meer, 2019; Van der Waal et al., 2013).
Altogether, these findings suggest that citizens value their own mobility rights more than the mobility rights of citizens from other EU countries of EU citizens in their country. We expect this to hold true for all types of mobility and this argument can be extended to the case of patient mobility.
Support for outgoing patient mobility is stronger than support for incoming patient mobility.
Determinants of support for patient mobility
Besides looking at overall differences in support for the mobility of patients, workers and students, this article also explores the determinants of support for mobility rights and whether they are similar or domain-specific across these different groups of movers. From a theoretical perspective, our framework is mostly based on self-interest-related accounts, while we also acknowledge the relevance of identity-centred explanations and include some related variables as controls in the analysis below. The utilitarian, self-interest-based model of public support for European integration (Brinegar et al., 2004; De Vries, 2018; Gabel, 1998) as applied to freedom of movement rights suggests that those who benefit (or expect to benefit) more from mobility rights are more supportive of these rights. Following this logic, previous research found that lower socio-economic status groups – measured by education and employment status – are indeed less supportive of free movement in general (Lutz, 2020; Vasilopoulou and Talving, 2018), intra-EU labour mobility (Ferrera and Pellegata, 2018; Mårtensson et al., 2023) as well as granting social rights to EU migrants (Sojka et al., 2023). This is because, theoretically, these groups feel more threatened and are less equipped to take advantage of mobility rights.
From the viewpoint of objective self-interest, patient mobility can be seen as an ‘elitist practice’ whereby those with more financial resources are more likely to take up their mobility rights to seek higher quality or less expensive healthcare abroad – including treatment that might not be available in their home country – or avoid domestic waiting lists. Only those with sufficient financial resources to travel and to get informed about cross-border healthcare rights will be able to benefit from patient mobility. In addition, there is no absolute guarantee that cross-border healthcare expenses are fully covered and reimbursed by citizens’ domestic health insurance, which could pose an additional obstacle to the cross-border mobility of poorer citizens. Taking advantage of these prospects is often determined by and differentiated along the lines of access to information and individual ability to pay (Österle, 2007). Furthermore, data from the Eurobarometer shows that those with more years of completed schooling are indeed more knowledgeable of rights related to healthcare received in another EU country and are more willing to travel to another EU country to receive medical treatment (European Commission, 2015). If mobility rights are used and exercised by the better off (because they know about these rights and have the means to travel to other countries), the better off get better treatment abroad, leaving the poor behind to receive worse treatment. This may further increase inequalities in health outcomes and access to specialised medical care.
From the viewpoint of subjective self-interest, perceptions of relative deprivation may also matter for attitudes towards patient mobility. Basically, citizens may feel that they do not have equal opportunities to meet their healthcare needs. We expect such feelings of relative deprivation in the medical era to be detrimental to their support for patient mobility, in particular regarding incoming patient mobility, since an increase of patients from other EU member states may pose a threat to the already perceived scarcity of medical resources. While no previous research has looked into this linkage explicitly, Ferrera and Pellegata (2018) find that perceptions of intertemporal material deprivation – i.e., a decrease in one's household financial situation in the last five years – go hand in hand with opposition towards intra-EU worker mobility in several member states including Germany. In a similar vein, individuals who perceive that they do not have equal opportunities when it comes to medical treatment in their country may fear that patient mobility further increases inequalities in access to and affordability of medical care for local residents. This could make them overall less supportive of patient mobility.
Overall, we can derive the following hypotheses from this section:
Individuals with higher socio-economic status are more in favour of patient mobility.
Individuals with stronger perceptions of relative deprivation within the healthcare system are less in favour of patient mobility rights.
Data and methods
Data
In order to test our theoretical expectations, we rely on original survey data collected between 11 January and 30 January 2023 for 6000 respondents in Germany. Data collection was conducted by the survey company IPSOS based on their online access panel. Quotas for age, gender, education and regional distribution were applied (with cross-quotas between age and gender) to ensure that the sample was representative of the demography of the general population aged 18–75 years. Informed consent was obtained from all participants. Respondents who did not pass the IPSOS quality checks were excluded from the sample. We additionally excluded respondents with item nonresponse on at least 30% of the questionnaire, those who participated in the pre-test and those with missing values on the dependent variables to facilitate comparison of effect sizes. This resulted in a net sample of 5750 respondents.
Germany is a highly relevant case when it comes to freedom of movement in the EU. As one of the founding countries of the EU, Germany has a long institutional history of European integration, which may have normalised the appreciation of the free movement of patients, students and workers among its population. First, Germany is the most popular destination country when it comes to intra-EU worker mobility and also has the largest outflow of workers in absolute numbers (European Commission, 2023). Second, Germany is among the top three countries for both inbound and outbound mobility of the Erasmus + program (European Commission, 2024b). Third, Germany has particular relevance as a country for outgoing as well as incoming patient mobility in the EU. While detailed EU-wide data on patient mobility is lacking, Germany alone represented 32.2% of the total amount spent among 23 EU countries (for which data is available) to reimburse patients who engaged in cross-border treatment or care not requiring prior authorisation in 2022 (European Commission, 2024a). At the same time, the enhancement of patient mobility rights through the introduction of Directive 2011/24/EU – which came into effect in 2013 in Germany – did not trigger any noticeable contentious debates in the German public (Haufe Online Redaktion, 2013). Overall, Germany ranks highest in the EU for healthcare spending, which amounted to 11.8% of its GDP in 2023, of which the largest share comes from public sources (85.9% of total expenditure) (OECD, 2024). Even though a high level of spending and resources in the healthcare system do not automatically translate into quality of provision (Reibling et al., 2019), the (perceived) quality of the German healthcare system is relatively high (Busemeyer, 2022), making it plausible to assume that there is considerable demand from EU patients to make use of the German healthcare system. Furthermore, patients may move to Germany from other countries for other reasons such as availability of care (shorter waiting lists), affordability and familiarity (Burge et al., 2005; Palm & Glinos, 2010). Therefore, we argue that Germany is a suitable test case for our hypotheses given its prominent position in the European debate about healthcare mobility.
Nevertheless, it is important to note that healthcare organisation and financing structures vary greatly across EU countries, which warrants caution in generalising the findings of this study to other EU member states. The German healthcare system operates on the principle of social insurance and is largely financed through contributions from individuals and companies to statutory health insurance funds. 8 Since the link between people's contributions and access to healthcare is stronger in the contribution-based systems compared to the tax-financed systems, this could imply that patient mobility is less likely to be perceived as a violation of the reciprocity norms among the German population as compared to populations in tax-financed systems, particularly if individuals are aware that incoming patients pay for healthcare in their home countries. On the other hand, the insurance logic could also lead to the opposite dynamic, with individuals who pay contributions being more inclined to support access only to those who directly pay into the system. In this regard, previous research indicates that reciprocity within welfare state institutions shields free movement from opposition, at least among vulnerable groups (Mårtensson et al., 2023). Although our case study cannot empirically test such claims, we consider the cross-national variation in healthcare systems when interpreting our findings and discussing their implications for broader generalisation (see conclusion).
Variables
The dependent variables, support for mobility rights of patients, students and workers, are measured by six items in total. Since free movement is characterised by a double nature, we incorporate both the outgoing and incoming mobility perspectives in our measurement of support for free movement rights. Firstly, respondents were asked about their support for outgoing mobility rights by means of the following survey items: ‘There are Germans who would like to go to other countries in the European Union for various reasons. To what extent do you agree or disagree with the following statements?’
9
Germans should be able to go to any other country in the European Union to work. Germans should be able to go to any other country in the European Union to study. Germans should be able to go to any other country in the European Union to receive medical treatment.
Subsequently, respondents were asked about their support for incoming mobility rights by means of the following survey items: ‘There are citizens from other European Union countries who would like to come to Germany for various reasons. To what extent do you agree or disagree with the following statements?’
Citizens from other European Union countries should be able to come to Germany to work. Citizens from other European Union countries should be able to come to Germany to study. Citizens from other European Union countries should be able to come to Germany to receive medical treatment.
Responses were measured on a 5-point Likert scale ranging from strongly agree (=1) to strongly disagree (=5) and recoded in a way that higher scores indicate higher levels of support. While all respondents were first presented with the items on support for outgoing mobility and then for incoming mobility, the order in which the different groups of movers were presented to the respondents (i.e., workers, students, and patients) was randomised in the survey. A confirmatory factor analysis reported in the Online appendix generates relatively weaker factor loadings of the items on patient mobility, suggesting that attitudes towards the free movement are not unidimensional and that patient mobility rights should be treated as a distinct type of free movement. We acknowledge that the formulation of the items on patient mobility allows for different interpretations since medical treatment covers a wide variety of healthcare services. However, since our aim was to tap into general attitudes towards patient mobility in a way that is comparable to the items on worker and student mobility, we believe that the generalised phrasing is a suitable measurement of our research question.
The socio-economic status is measured using three variables. First, we include education by distinguishing lower secondary or less, upper-secondary and post-secondary non-tertiary, and tertiary education based on the ISCED classification. Second, we include the net equivalised household income of the respondents categorised in quartiles. To calculate the equivalised income, we gave each household member an equivalent value: 1 for the first adult, 0.5 for the second and each subsequent adult, and 0.3 for each child under 18. Third, we include dummies for employment status, distinguishing the employed, unemployed, students, retired and a rest category for others. Generally speaking, we expect a positive association between the different indicators of socio-economic status and support for mobility rights as hypothesised above.
To measure perceptions of relative deprivation, the survey included detailed measurements of deprivation in the healthcare system, education system and labour market. For medical treatment opportunities, respondents were asked ‘Imagine you were to seek medical treatment today. Compared to other people in Germany, would you say that you personally would have more or fewer opportunities of receiving the medical treatment you want?’. For education opportunities, respondents were asked ‘When you compare yourself with other people in Germany, do you have the feeling that you personally had more or fewer opportunities of achieving the educational qualification you want?’. For job opportunities, respondents were asked ‘Imagine you are currently looking for a job. Compared to other people in Germany, would you say that you personally would have more or fewer opportunities of getting the job you want?’. Responses were measured on 5-point scales ranging from ‘far more opportunities’ (=1) to ‘far fewer opportunities’ (=5) and recorded in a way so that higher scores indicate higher levels of deprivation.
We control for a number of socio-demographic variables, including age, gender, migration background (being born or having at least one parent being born outside of Germany) and region (former East/West Germany). Furthermore, we also control for anti-immigrant attitudes and support for egalitarianism via an index (see the Online appendix for operationalisations) to isolate the effects of socio-economic status and relative deprivation. Since EU mobility is a specific type of migration, citizens’ generalised attitudes towards immigrants partly explain their support for free movement (Lutz, 2020; Sojka et al., 2023). Similarly, since political ideology shapes one's support for free movement rights, with left-wing citizens being more in favour (Ferrera and Pellegata, 2018; Gerhards et al., 2021; Vasilopoulou and Talving, 2018), we expect individuals with stronger egalitarian values to be more supportive of patient, student and worker mobility rights. The Online appendix provides descriptive statistics of all variables and correlation coefficients.
Statistical modelling and robustness checks
We perform ordinary least square (OLS) regression analysis using support for outgoing and incoming mobility for the three mobility groups of theoretical interest – patients, students, workers – as the dependent variables in our models. All continuous independent variables (i.e., relative deprivation, egalitarianism, anti-immigrant attitudes, age) have been standardised with a mean of zero and a standard deviation of one. Weights are applied in all analyses to correct for potential non-response bias. To gain a more nuanced understanding of the factors shaping free movement attitudes, we provide models including and excluding control variables. Furthermore, we report a series of robustness checks in the Online appendix: (1) using ordered logit modelling, (2) logistic regression modelling, (3) multilevel modelling, 10 excluding respondents without German nationality and (4) including political interest as a proxy for knowledge about mobility rights. These additional analyses provide very similar results, providing further evidence for the robustness of our findings.
Support for patient, student and worker mobility (N = 5750).
Results
Descriptive analysis
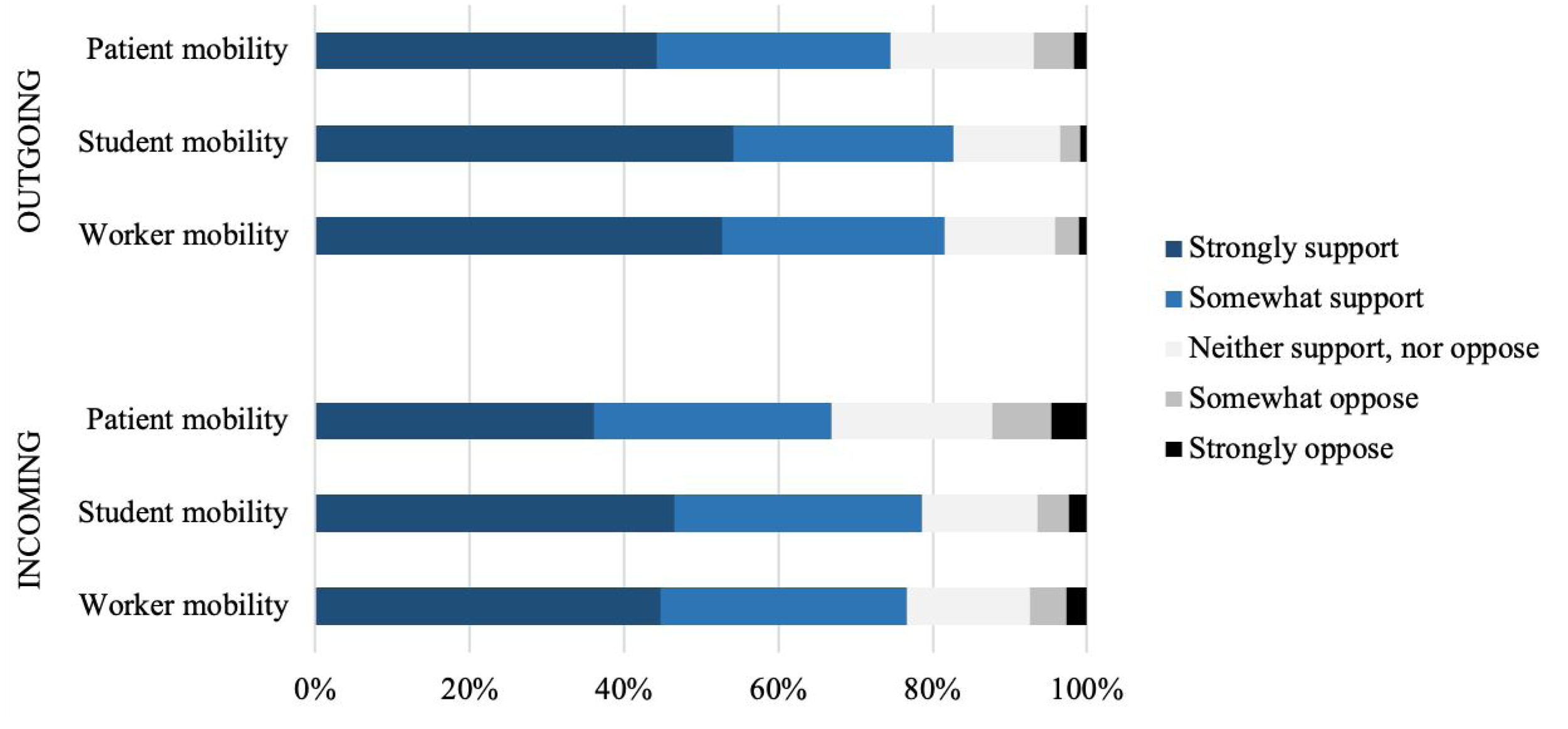
We are interested in whether there is a universal ranking order of support for different mobile groups. Figure 1 displays the weighted support levels in the sample and illustrates that support levels indeed vary across the three groups of interest and that the ranking order is similar for outgoing and incoming mobility, with student mobility being most supported and patient mobility least supported. Considering outgoing mobility, Figure 1 shows that patient mobility is less supported than worker mobility and student mobility. Specifically, 82.7% of the respondents somewhat or strongly support outgoing student mobility rights, while 81.5% support worker mobility and 74.6% support patient mobility rights for German citizens. To test whether these differences are statistically significant, the Online Appendix presents the mean values and 95% confidence intervals. It confirms that the difference in support between patients, on the one hand, and workers and students, on the other hand, is statistically significant (p < .001), while the support levels for worker and student mobility do not differ significantly from one another. Turning to incoming mobility rights, we similarly observe that support for patient mobility is significantly weaker than support for student and worker mobility (p < 0.001). Differences in support between incoming worker and student mobility are again insignificant (see the Online Appendix). These findings support Hypothesis 1 from above, suggesting that the principle of reciprocity trumps that of (medical) need in the context of EU freedom of movement.
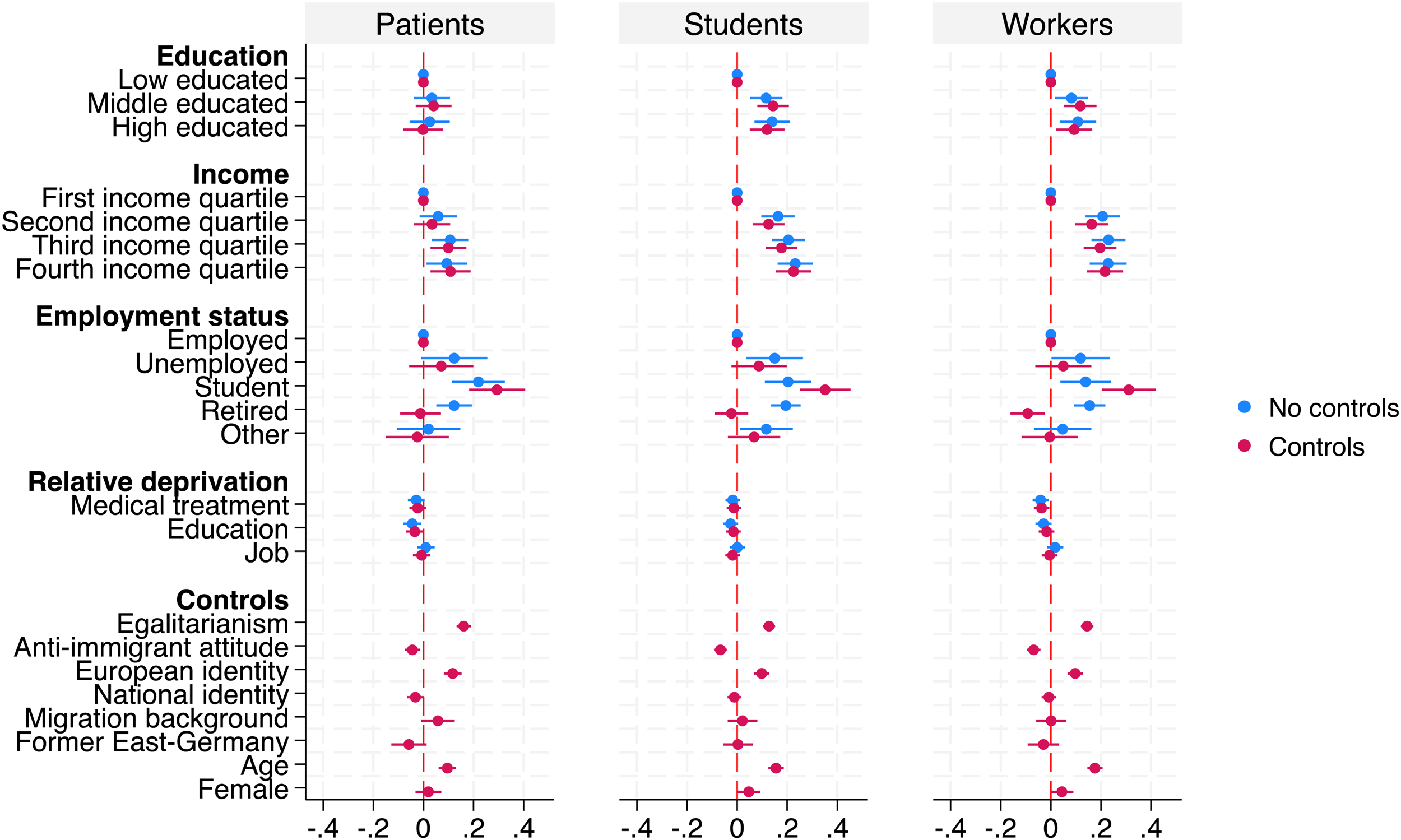
Linear regression models predicting support for outgoing patient, student and worker mobility (N = 5712).
To what extent do support levels for outgoing and incoming mobility rights align? Figure 1 shows that for each of the three respective groups support for outgoing mobility is slightly higher than support for incoming mobility, in line with Hypothesis 2. For example, when one considers worker mobility, we find a gap in support for outgoing and incoming mobility support of 8 percentage points when looking at those most strongly in favour. About 53% of respondents strongly support that Germans should be able to go to any other country in the European Union to work, compared to 45% who strongly agree with the statement that citizens from other EU countries should be able to come to Germany to work. In a similar vein, 54% of respondents strongly agree that Germans should be able to travel to any other country in the European Union to study, while this percentage drops to 46% when it comes to whether citizens from other EU countries should be able to come to Germany to study. Finally, about 44% strongly support outgoing patient mobility, while only 36% strongly support that citizens from other EU countries should be able to come to Germany to receive medical treatment. These differences in support for outgoing and incoming mobility turn out to be statistically significant for each of the three groups. This highlights that support for free movement is conditional on whether one adopts an outgoing or incoming mobility perspective; when respondents are confronted with immigration scenarios (granting rights to citizens from other EU countries), they are somewhat more hesitant to support the principle of free movement than when they are confronted with emigration scenarios (granting rights for nationals). From a broader perspective, the overall high levels of support for all types of mobility rights indicate that the principle of freedom of movement within the EU is well-established and widely supported in German society.
Multivariate analysis
What determines support for patient mobility rights? Figures 2 and 3 display the determinants of support for outgoing and incoming mobility of patients (left panel), along with student (middle panel) and worker mobility (right panel). Regression coefficients are shown for models excluding and including controls. First, we consider the impact of socio-economic status variables. For one, we observe that support for the mobility rights of students and workers is more strongly structured by the socio-economic position than support for the mobility rights of patients. Middle- and higher-educated respondents are more likely to agree that Germans should be able to go to any other EU country to study or work than lower-educated respondents. By contrast, there is no educational divide in support for patient mobility. In a similar vein, higher-income groups are more likely to support worker and student mobility rights. Controlled for other variables, those in the fourth income quartile score about 0.23 and 0.22 points higher on the 5-point scale for outgoing student and worker mobility and 0.19 and 0.17 points higher for incoming students and worker mobility respectively. This pattern is much weaker for patient mobility; those in the highest income quartile are only slightly more in favour of outgoing patient mobility (0.11 points) than those in the lowest quartile. When it comes to incoming patient mobility, the income differences are insignificant. Furthermore, support for free movement rights barely varies with employment status, with the exception of students. Figures 2 and 3 show that students are significantly more supportive of all types of mobility rights than employed individuals. Interestingly, the unemployed do not differ in their free movement attitudes from the employed. Overall, these findings do not provide conclusive evidence in favour of Hypothesis 3 as indicators of socio-economic status seem to be a stronger predictor of attitudes in the case of the other domains compared to patient mobility.
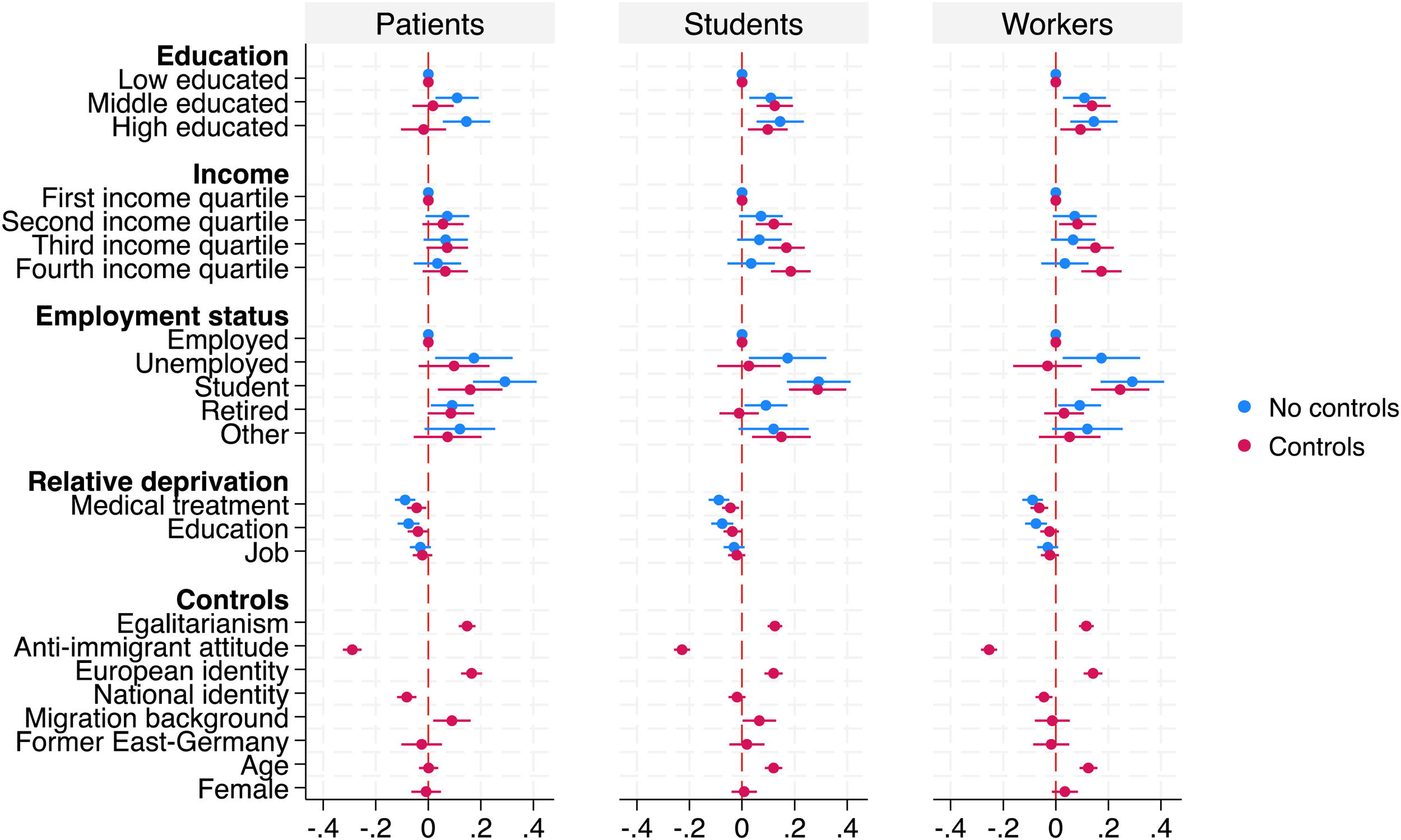
Linear regression models predicting support for incoming patient, student and worker mobility (N = 5712).
Second, Figures 2 and 3 suggest that perceptions of relative deprivation in specific areas slightly erode support for free movement rights for different groups. More specifically, individuals who feel disadvantaged in the healthcare system in comparison with their national fellows are less supportive of incoming patient mobility yet not outgoing patient mobility. An increase of one standard deviation in perceived medical treatment deprivation results in a decrease of 0.045 points on the scale for incoming patient mobility. This finding provides only partial support for Hypothesis 4. Regarding workers and student mobility, the effects of relative deprivation with respect to employment and educational opportunities on support for outgoing and incoming mobility rights all go in the same direction but are statistically insignificant in most cases (see the Online Appendix).
Although not the focus of this article, the control variables further contribute to explaining individual differences in support levels. Figures 2 and 3 show that older respondents are more supportive of all types of mobility rights, with the exception of incoming patient mobility, which could be explained by their higher needs for medical care in old age, thereby fearing competition from mobile patients for timely and high-quality care. Further, those with stronger egalitarian values are significantly more supportive of patient, student and worker mobility. While anti-immigrant attitudes are consistently negatively associated with support for all types of free movement rights, they are particularly relevant in explaining support for incoming mobility, which advances previous research on the link between immigration attitudes and support for free movement (Lind and Meltzer, 2021; Lutz, 2020; Sojka et al., 2023). Finally, a stronger European identity goes hand in hand with higher levels of support for patient mobility, while stronger sentiments of national identity are unrelated or slightly negatively related to support. This pattern is similar across the different domains. Overall, these findings confirm that cultural and ideological attitudes complement self-interest theories (Hainmueller and Hiscox, 2006).
Finally, to gain a more detailed understanding of the similarity or domain-specificity of the drivers of free movement rights for patients, students and workers, we have constructed a differential that measures support for free movement in an alternative way. This measure captures the extent to which respondents are more opposed towards patient mobility relative to student and worker mobility. We constructed a rather conservative measure whereby a value of 1 indicates that respondents expressed higher support for both student and worker mobility compared to patient mobility. A score of 0 captures all other respondents; those giving equal levels of support to all three groups, as well as those with mixed attitudes and those who express higher support for patient mobility than for student and/or worker mobility. With respect to outgoing mobility rights, 17% of the respondents negatively discriminate against patients. This pattern is slightly amplified when we consider incoming mobility, as 21% of the respondents are less supportive of entry rights for EU patients compared to students and workers. The Online Appendix plots the effects of the socio-economic status variables and perceptions of relative deprivation for such differentiated preferences regarding the incoming and outgoing mobility of patients. Interestingly, highly educated respondents are significantly more likely to express disfavour against patients, both when it comes to inflows and outflows of patients. A similar trend is observed for the effect of income, whereby higher income groups disfavour patients more strongly when it comes to their support for outgoing mobility rights, yet not for incoming mobility. Despite the small effect sizes, this finding reveals new and more fine-grained insight into public support for an integrated European Health Union. Not only does it appear that patient mobility is more contested compared to student and worker mobility, but it also appears that different subgroups within the population differentiate to various degrees in their support for different mobile groups.
Conclusion
This article investigated public attitudes towards mobility rights for patients in comparison with students and workers. This is an important topic, particularly in times of increasingly polarised attitudes on European integration and the European social model. Using novel survey data from Germany, the study comes to a range of conclusions. First, not all mobile groups are perceived equally: Public support for mobility rights for patients in the EU is significantly lower compared to support for student and worker mobility. We explain this finding by pointing to the importance of the reciprocity principle. In the case of healthcare, mobile patients make use of – sometimes scarce – healthcare resources and do not directly contribute to the financing of public healthcare systems in the host country. While mobile students also make use of the host countries’ welfare state institutions and resources, they seem to be perceived as contributing more to society, for instance by staying on for work after their studies. Similarly, mobile workers directly contribute to the financing of the welfare state. Hence, we argue that a stronger reciprocal relationship between mobile EU citizens and the host country fosters support for the free movement of such specific mobile groups.
Second, in relation to the determinants of public support, our most intriguing finding is that socio-economic status increases support for the mobility of students and workers but not for patients. Why is socio-economic status not related to patient mobility support? Potentially, this effect may be related to the particular characteristics of attitudes towards healthcare (Jensen and Petersen, 2017), which are in general not strongly structured by socio-economic status (Azar et al., 2018; Missinne et al., 2013). A further factor could be the institutional set-up of the German healthcare system, in which the delivery of care might be perceived as costless by patients as there are very few co-payments. Consequently, individuals across the income ladder may not see personal financial barriers to seeking treatment abroad and lack awareness about the costs of cross-border healthcare. Overall, these findings further nuance the growing literature on public support for Social Europe by showing that the socio-economic divide in attitudes varies across policy dimensions.
The results of this study also have a few policy implications. While we find some nuances, overall the freedom of movement principles are widely supported by the public, even though their specific implementation may be more contested. In this regard, our research is also connected to the larger literature on the future of social citizenship at the EU level (Bauböck, 2019; Börner, 2020; Ferrera, 2003; Keune et al., 2023). Freedom of movement – including the social rights that are attached to individuals moving across borders – is a central feature of EU social citizenship. So far, much of the literature on EU social citizenship focuses on policies and policy design and less on how citizenship rights are perceived by citizens (Eick et al., 2023). The focus on the individual recipients and their attitudes is of particular importance for the future of the European Health Union where citizens may be somewhat hesitant to support a borderless healthcare system within the EU. Ultimately, patient mobility therefore poses challenges to national governments, in particular as population aging is likely to increase the demand for healthcare services across Europe and further enlargements of the EU have potential implications for the scope of patient mobility.
While this article reveals new insights into the literature, it also comes with some limitations that provide important paths for future research. First of all, the empirical results focus on Germany as a case study. Cross-national data on support for (patient) mobility rights is needed in order to verify our findings, especially in emigration countries such as Eastern Europe (see Bruzelius (2023) and Kyriazi and Visconti (2023) on this point), where shortages in the health workforce may leave citizens with unmet healthcare needs. An interesting question to pursue further in this context is whether the institutional characteristics of healthcare systems influence popular attitudes towards the free movement of patients. As hinted at above, the public may be less supportive of patient mobility in universal healthcare systems that are closely tied to (national) citizenship and residence as in the case of the British NHS, whereas support could be higher in health insurance systems such as Germany, in particular if people are aware of the fact that mobile patients contribute to financing via their home countries. However, the opposite dynamic may also be at work such that individuals in insurance-based systems are more sceptical towards mobility rights as mobile patients do not directly contribute to financing. While previous studies point towards the role of ‘institutional reciprocity’ in welfare states in shaping public support for healthcare solidarity (Hrast et al., 2018) and free movement (Mårtensson et al., 2023; Ruhs and Palme, 2020), this is still to be explored in the area of patient mobility rights. Therefore, future research should investigate cross-national differences in support for patient mobility – in absolute terms and relative to student and worker mobility – and its determinants.
A second limitation of our study is the potential social desirability bias in our survey since all respondents were asked about their support for outgoing mobility and, subsequently, incoming mobility. Participants might have responded more positively to incoming mobility in order not to appear egoistic by supporting outgoing mobility and opposing incoming mobility. One can expect these differences between both perspectives of mobility to be larger when using split-sample designs (Lutz, 2020). However, the fact that we still observe significant differences signals that citizens prioritise their own mobility rights over those of other EU citizens. Finally, our survey does not contain information on specific knowledge about mobility rights, whereas it would be interesting to explore to what extent support for mobility rights is associated with differences in knowledge. For example, respondents could be selectively exposed to information on the costs and benefits of patient mobility in the EU. In addition, it would be valuable to examine support for patient mobility across different types of medical treatment – such as for life-threatening medical conditions, rare diseases, or reproductive and cosmetic surgery – since these may receive varying levels of public support. Furthermore, the supply side is not investigated in our article in terms of the mobility of doctors and nurses, and this would, once again, require a comparative perspective. Hence, in addressing these further issues, we hope that this study will lay the groundwork for future research on the freedom of movement for patients and other underexplored groups.
Supplemental Material
sj-zip-1-eup-10.1177_14651165251341570 - Supplemental material for Equal rights to move? Public attitudes towards the free movement of patients, students and workers in the EU
Supplemental material, sj-zip-1-eup-10.1177_14651165251341570 for Equal rights to move? Public attitudes towards the free movement of patients, students and workers in the EU by Sharon Baute, Marius R. Busemeyer and Gianna Maria Eick in European Union Politics
Supplemental Material
sj-zip-2-eup-10.1177_14651165251341570 - Supplemental material for Equal rights to move? Public attitudes towards the free movement of patients, students and workers in the EU
Supplemental material, sj-zip-2-eup-10.1177_14651165251341570 for Equal rights to move? Public attitudes towards the free movement of patients, students and workers in the EU by Sharon Baute, Marius R. Busemeyer and Gianna Maria Eick in European Union Politics
Supplemental Material
sj-docx-4-eup-10.1177_14651165251341570 - Supplemental material for Equal rights to move? Public attitudes towards the free movement of patients, students and workers in the EU
Supplemental material, sj-docx-4-eup-10.1177_14651165251341570 for Equal rights to move? Public attitudes towards the free movement of patients, students and workers in the EU by Sharon Baute, Marius R. Busemeyer and Gianna Maria Eick in European Union Politics
Footnotes
Acknowledgements
The authors would like to thank the participants of seminars organised at the University of Konstanz, the University of Basel, the Goethe University Frankfurt, and the CES Conference in Lyon 2024 for their valuable feedback.
Author contributions
Sharon Baute contributed to the conceptualisation, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, validation, visualisation and writing of the article. Marius R. Busemeyer contributed to the conceptualisation, data curation, funding acquisition, investigation, methodology, project administration and writing of the article. Gianna Maria Eick contributed to the conceptualisation, data curation, investigation, methodology, project administration and writing of the article.
Funding
This research was supported by the German Research Foundation (DFG) under the Excellence Strategy of the German federal and state governments – EXC-2035/1.
Data availability statement
The data and replication code are available as part of the Supplementary Material at the DOI of the article.
Supplemental material
The data and replication code are available as part of the Supplemental Material.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.