
Abstract
This article studies the use of positive assessments in interaction in Swedish residential care in Finland. The data consisted of four video recordings of baking activities involving professional caregivers and residents with dementia. The method used was conversation analysis. In these activities, caregivers used positive assessments to facilitate the residents’ performance of the task, either by providing them with the resources needed to perform the task or by performing things for the residents. Assessments were used to encourage the residents in attempting to perform the task, making progress in the task, and achieving autonomous activity in the task. The study demonstrated how residents’ reduced functional capacity makes also minor success worth praising, without an undertone of infantilization.
Keywords
Introduction
This study examines how professional caregivers use positive assessments to facilitate how residents with dementia perform manual tasks and what the role of positive assessments is in managing the residents’ independence and assisting them in task performance. The empirical data consist of videotaped baking sessions involving caregivers and residents and the method used is conversation analysis (CA). The studied assessments are analyzed sequentially to determine their placement in relation to the ongoing task.
Food-related activities such as cooking and baking together constitute meaningful activities in residential care. Meaningful activities are defined as “enjoyable activities that engage the nursing home resident to an extent that they improve either their emotional wellbeing, cognitive status, physical function, or reduce problematic behaviors” (Morley et al., 2014). There is a vast amount of literature on how engagement in meaningful activities can have a positive influence on residents’ quality of life (e.g., Cooney et al., 2009; Schenk et al., 2013; Shryock and Meeks, 2022) and reduce neuropsychiatric symptoms such as agitation and passivity (e.g., Kolanowski et al., 2005).
Thus, it is a well-known fact that residents’ engagement in meaningful activities support their thriving in residential care (Björk et al., 2017). However, residents’ capacity to engage in such activities efficiently can be challenged because of dementia leading to deterioration in executive functioning skills, such as the ability to plan, organize, and carry out activities efficiently (Evans et al., 2021; Voss and Bullock, 2004; Wherton and Monk, 2010). As the ability to function independently decreases, individuals with dementia increasingly become dependent on others to participate in everyday activities (Eriksen et al., 2016; Vikström et al., 2008). However, co-participants may experience dilemmas in managing how persons with dementia engage in activities. Co-participants can use seemingly contrasting approaches such as supporting persons with dementia to perform tasks independently or taking over tasks (e.g., Johansson et al., 2011; Vikström et al., 2008), demonstrating a perceived dilemma between encouraging initiative or providing help.
The dilemma between supporting independence and helping residents can result in different interactional strategies, especially when the aim of the activity is not learning but maintaining residents’ skills or supporting their wellbeing. This study explores the interactional behavior of several caregivers employed by the same health care organization with a particular focus on positive assessments. In all studied conversations, both the material environment and the overall turn-taking pattern in the interaction were adapted to facilitate the performance of residents with dementia. Arrangements of the material environment involved placing artifacts in the immediate physical environment and, thus, making them available to residents (Majlesi et al., 2019). The adaptation of the turn-taking pattern involved caregivers taking on the role of producing directives, “utterances designed to get someone to do something” (Goodwin, 2006: 517), that created an interactional environment in which individuals with dementia were able to participate efficiently in an ongoing activity (cf. Majlesi and Ekström, 2016). Even though the material and interactional environment was arranged to facilitate resident performance, the details of interaction demonstrated a variety in how this was accomplished.
In studying positive assessments in dementia care interaction, this study draws on the theoretical and conceptual framework of conversation analysis. Conversation analysis, originally a method for empirical study of naturally occurring social interaction (Heritage, 1984), has over time developed towards a theory with the aims to uncover the structural organizations of practice that participants in a social interaction draw upon (Stivers, 2013). The application of conversation analysis to research on complex communication needs provides a perspective focused on interaction and meaning created as the product of participants’ collaborative work. Further, the conversation analytic perspective enables analysis of how complex communication needs become evident in interaction and how the participants deal with these challenges. (Wilkinson et al., 2020: 26–27.) This study contributes to a growing body of research on dementia and interaction (e.g., Guendouzi and Müller, 2006; Jansson and Plejert, 2014; Lindholm and Stevanovic, 2022; Mikesell, 2016; Rasmussen et al., 2019) as well as to the research on assessments in institutional interaction and dementia care (see section “Assessments in institutional interaction and dementia care”). In the following, I give an overview of previous research on assessments from an interactional perspective and the special take on assessments I adapt in this study.
Assessments in institutional interaction and dementia care
Assessments are typically performed through utterances that contain a positive or negative prediction of either a referent or something that can be inferred from the context (Goodwin and Goodwin, 1987; Pomerantz, 1984; Sorjonen and Hakulinen, 2009). They are related to knowledge—by producing an assessment, a speaker claims knowledge of the referent he/she is assessing, and claiming insufficient knowledge counts as a valid reason for being unable to produce an assessment (Pomerantz, 1984: 57, 58). Sequentially, assessments typically make relevant responses constituting of subsequent assessments. These subsequent assessments may either agree or disagree with the first assessment. Agreeing subsequent assessments are constructed as preferred, and they can be either upgraded or downgraded (Pomerantz, 1984).
Assessments involve lexical, vocal and embodied resources that are combined to perform evaluations (Goodwin and Goodwin, 1987; Pomerantz, 1984; Sorjonen and Hakulinen, 2009). Assessments are complex and their form can vary (Potter and Edwards, 2013: 715). Sometimes they include moral or evaluative terms (good, poor), but on other occasions, they are built using descriptions. The present study included both minimal evaluative terms (explicit positive assessments; Waring, 2008) and more elaborate descriptions (see section “Data and methods”).
Assessments have different functions in various forms of natural interaction. This study investigated the use of positive assessments in the institutional context of dementia care. In institutional contexts, the activity has a clear overall goal and participants have complementary roles connected to certain rights and duties (Drew and Heritage, 1992; Heritage, 1997; Linell, 1998). Typically, professionals are responsible for institutional activities, and laypersons are supposed to act in a manner expected by the institution. In institutional interaction, professionals typically use positive assessments to maintain institutional routines, such as managing transitions between activities. How positive assessments are used to segment the flow of interaction has been demonstrated for various institutional contexts, such as interviews (Antaki et al., 2000), service encounters (Lindström et al., 2019), classroom conversations (Waring, 2008), personal training (Huhtamäki and Grahn, 2022), and task-guidance by job coaches (Leskelä, 2023). Huhtamäki and Grahn (2022: 126), for example, demonstrated how the placement of assessments created an interpretative framework for the action—assessments produced during an ongoing exercise were interpreted differently from those produced near closure.
While most CA studies on assessments have addressed contexts involving neurotypical participants, a few exceptions are, however, worth noting. In their study of positive assessments in interviews, Antaki et al. (2000) showed that assessments were used to signal the completion of both individual question-response pairs and whole series of questions. Although the researchers (Antaki et al., 2000: 260) noted that most of their examples included data on participants with learning disabilities, they did not present a direct causal relationship between the participants’ mental capacity and the use of positive assessments. In contrast, they discussed whether it could be participants’ underlying expectations that caused them orient to possible trouble and see a stronger need for encouragement than in other contexts. Leskelä (2023) also examined positive assessments in interaction involving persons with learning disabilities. More precisely, the context involved job coaches guiding workers with intellectual disabilities in performing manual tasks. She demonstrated that positive assessments often targeted either the progress and success of a task or a worker’s general skills and learning process. Leskelä did not draw any conclusions regarding the use of positive assessments and the participants’ mental capacity. However, she stated that persons with learning disabilities are often the target of assessments, which indirectly indicates that the use of positive assessments in these contexts would differ from assessments in conversations with neurotypical participants.
In the context of caregiving for older adults, the earliest studies discussed assessments as an aspect of communication without delving deeper into this area. These primarily sociolinguistic studies demonstrated how caregivers used positive assessments to overcome potentially commanding caregiving situations (e.g., Backhaus, 2009; Grainger, 1993; Makoni and Grainger, 2002). These studies defined the exaggerated use of positive assessments, such as praising an older person’s performance in an ordinary task, as a patronizing feature of elderspeak (Backhaus, 2009; Grainger, 1993; Sachweh, 1998; Shaw and Gordon, 2021). Elderspeak, a simplified speech register based on the systematic accommodation of speech toward older adults (Kemper, 1994), has been criticized for being infantilizing and dependency-inducing (e.g., Caporael, 1981; Kemper and Harden, 1999; Marsden and Holmes, 2014; Williams et al., 2009). Thus, these early studies primarily reported the negative aspects of positive assessments in older adult care and must be followed up by more detailed studies on the use of positive assessments in interaction, such as the current one.
Only a few CA studies on positive assessments in caregiving situations have been conducted among older adults. Lindström and Heinemann (2009) studied assessments in Danish and Swedish home help situations. They showed that low-grade assessments (such as “good”) were used for task completion, whereas high-grade assessments (such as “brilliant”) were used to treat senior citizens’ performance of tasks as an achievement. Thus, on one hand, high-grade versus low-grade assessments were used to treat tasks performed by caregivers as routine tasks, and, on the other hand, senior citizens’ tasks as something out of the ordinary. Jansson (2016) examined praise in Swedish caregiving settings with staff assisting residents with personal hygiene. She observed that encouraging residents to perform certain tasks involved the repeated use of positive assessments. She also pointed out that residents did not usually respond to praise, but any sign of response was used by caregivers as an opportunity to intensify contact with residents. In a study on assessments in assisted eating activities, Majlesi et al. (2020) demonstrated that assessments were used to build joint attention in the activity of assisted eating and to encourage assisted persons to submit to or continue with the activity of eating.
In sum, a large body of CA-research has investigated assessments in interaction. According to previous studies on institutional interaction, positive assessments are used to indicate transitions between activities, provide encouragement and positive evaluations. The present study focused on how positive assessments are used by caregivers to facilitate residents’ performance in the activity of baking. It demonstrates how caregivers use positive assessments to facilitate resident performance and manage the dilemma between encouraging resident initiative and helping them out in the performance of manual tasks.
Data and methods
The data consisted of four video recordings (approximately 2 h and 20 min) of baking activities with the overall aim of providing recreation for residents with dementia. The data were collected in Swedish-language care facilities in Finland and involved seven residents with dementia and five professional caregivers. 1 At the request of the caregivers, all recordings involved two caregivers working with a pair of residents. Both pairs of participants were present on site in the conversations from which the analyzed extracts were drawn. However, the analyses in this article focus on dyads involving one resident and one caregiver. The data were augmented through two researchers’ direct observations (one of which was the author of this article) and interviews with the caregivers conducted on other occasions. The interviews cast light on the overall results on the research project in which the data were collected (see Footnote 1), that is, adaptation of language, by demonstrating caregivers’ understanding of the need to adapt communication when persons with dementia are involved. The interview data are, however, analyzed elsewhere, and this study focuses solely on interactional data.
The analysis section of this article features examples from three conversations. The method used, conversation analysis (CA), has been successfully applied since the 1990s to the analysis of the interaction of persons with communication impairment (Wilkinson, 2019). In CA, the analyst approaches the data without hypotheses. Specific points of interest emerge when the data are analyzed. Because these data were collected in a project of Easy Language, the researchers originally approached the data with an interest in studying linguistic adaptation. However, in the initial phase of analysis, both verbal and embodied strategies used by caregivers to facilitate the performance of manual tasks were identified. Verbal strategies involved dividing directives into fragments and using positive assessments, whereas embodied strategies involved changing the caregiver’s posture by leaning forward, manipulating artifacts, and touching the resident.
Positive assessments used to facilitate the performance of manual tasks were chosen as the focus of the current study. A total of 57 positive assessments used in this manner were identified and analyzed. This collection primarily involved 37 lexical turns and 20 clausal turns. The sequences analyzed in this study are representative of the whole data set, with Extracts (1) and (2) containing mostly lexical turns and Extract (3) both lexical and clausal turns. A sequential analysis of the positive assessments was performed to establish the functions of the assessments and to determine where they were placed in relation to the ongoing task. The data extracts were transcribed following conversation analytic conventions (Ochs et al., 1996). The multimodal features were transcribed using Mondada’s (2019) transcription conventions.
Analysis
I will now proceed to an empirical account of positive assessments produced by caregivers. The data provide an illustration of how caregivers’ positive assessments are related to the dimensions of taking over tasks and supporting independent performance. The presentation of extracts proceeds from (1) taking over the task via (2) encouraging attempts to perform the task to (3) encouraging autonomous activity.
Taking over the task—mitigating caregivers’ input
When persons with dementia become increasingly passive in engaging in activities, one strategy used by co-participants is to take over tasks. There are various reasons for taking over tasks, such as saving time for having more free time together with the person with dementia (Vikström et al., 2008: 269), or, in professional contexts, simply to get the job done (Brown Wilson and Davies, 2009).
Extract (1) features an example of caregiver C taking the main responsibility for moving the task forward, providing directives simultaneously with the embodied activity of cutting dough, without waiting for resident A to perform the activity independently.
We enter the conversation at a point where C is verbalizing the target of the coming action, simultaneously making a sweeping gesture with his hand (l. 01). In Line 04, C announces that he will visa modell (“show you how to do it”). Using the terminology of Evans and Lindwall (2020), C seems to be verbally announcing a directive with the form of demonstration as performance, in which the instructed person is treated as a passive learner and recipient. However, C then places his hands on A’s hands. This embodied action indicates that A is not supposed to watch a demonstration of how to perform the action, but that they, rather, will do the action together. During the action of cutting dough, A is moving along with C, who holds on to the knife (l. 09-17).
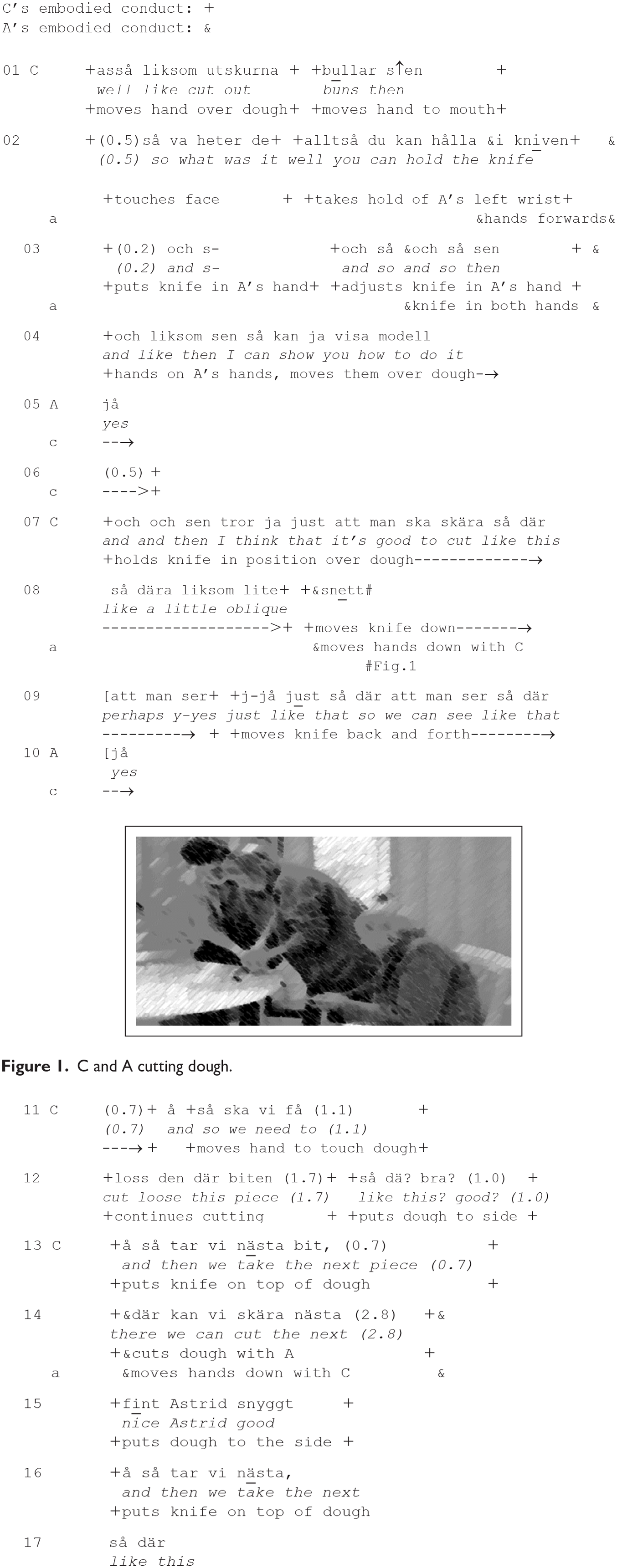
Extract (1) contains two instances of positive assessments, så dä? bra? (“like this? good?,” l. 12) and bra Astrid snyggt (“nice Astrid good,” l. 15). The first of these instances is produced with rising intonation. Both instances indicate transitions between phases in the activity, cutting pieces of dough. Both assessments are produced simultaneously as C puts a piece of dough to the side, indicating the end of one phase of the activity, and followed by C producing a meta-comment (l. 13, 16) and placing the knife in a position ready for cutting the next piece of dough. The assessments seem to signal that the activity is moving in a preferred direction.
The positive assessments in (1) are not only related to signaling transition, but also to how C deals with the dilemma of supporting A’s independence and taking on the responsibility for the task. The extract demonstrates diversity in how participants’ agency is expressed and enacted. As mentioned earlier, C starts by positioning Astrid as the one who holds the knife (l. 02) and himself as the one showing her how to do it (l. 04). Here, he uses the first person (du, “you,” l. 02) and second person (ja, “I,” l. 04) singular pronoun to refer to them as actors. Later, he, however, changes to impersonal constructions with the generic third person man (“one,” l. 07, 09), when he initiates the following action and produces online commentary of the cutting action. From line 11 onwards, there is a change in pronouns; C uses the first plural pronoun vi (“we,” l. 11, 13, 14, and 16) to present the ongoing and following action as joint action performed mutually by him and Astrid. On the other hand, his positive assessments, particularly the one in line 15, seem to be addressed to Astrid. Here, he uses Astrid’s first name in the positive assessment. Using a person’s first name in interaction typically has the function of addressing the turn to this person (Lerner, 2003), whereas, here, the use of Astrid’s first name also seems to underline her performance and tone down C’s own role in cutting the dough. Previous research on positive assessments in care has demonstrated how positive assessments can be used to mitigate the institutional representative’s role and construct the care recipient as capable and autonomous (Jansson, 2016; Lindström and Heinemann, 2009). This is also the case in Extract (1). However, the underlying asymmetric relationship between participants remains unchanged because the caregiver acts as having the right to assign responsibility to the resident (cf. Magnusson, 2022).
In Extract (1), caregiver C and resident A cut dough into pieces, making progress with the activity of baking buns one piece at a time. Even though C announced the activity as a demonstration performed by him, he turned out to facilitate A’s performance by taking on the main responsibility for the task. This illustrates a difference between the context of caregiving and educational contexts (e.g., Lindwall and Ekström, 2012). In educational contexts, the overall aim manifests, for example, that the teacher cannot complete the assignment for the student (Lindwall and Ekström, 2012: 35). Here, the main aim is not to teach Astrid how to bake but to engage her in a meaningful activity. Therefore, C does not wait for Astrid to perform the activity but intervenes to make it easier for her to perform it. Positive assessments were used to give Astrid credit for her performance and seemed to mitigate the caregiver taking over the task and the resident sticking to a more passive role.
Encouraging resident’s attempts to perform the task
Extract (1) demonstrated how positive assessments were used to assess the resident’s performance in a context where the caregiver, in fact, was the primary actor of the task. Another strategy used by caregivers in the data to manage residents’ performance involved carefully constructing opportunities for the resident to perform the task and producing positive assessments that encourage the resident’s attempts. This was the case in Extract (2) that features a lengthy sequence in which caregiver C helps resident Susanne in pressing doughballs with a fork to make cookies.
This sequence demonstrates how C incrementally adjusts her support to Susanne’s needs and constructs affordances for Susanne to participate. She first uses verbal resources and pointing gestures to initiate participation (l. 01-02) and then touches (l. 03) and adjusts the available artifacts (l. 06, 07). The demonstrated order of the resources is in line with the findings of Marstrand and Svennevig (2018), who showed that touch was used to facilitate interaction between residents and caregivers only when verbal resources and gestures failed. Extract (2) illustrates yet another dimension, with touch being followed by the handling of artifacts.
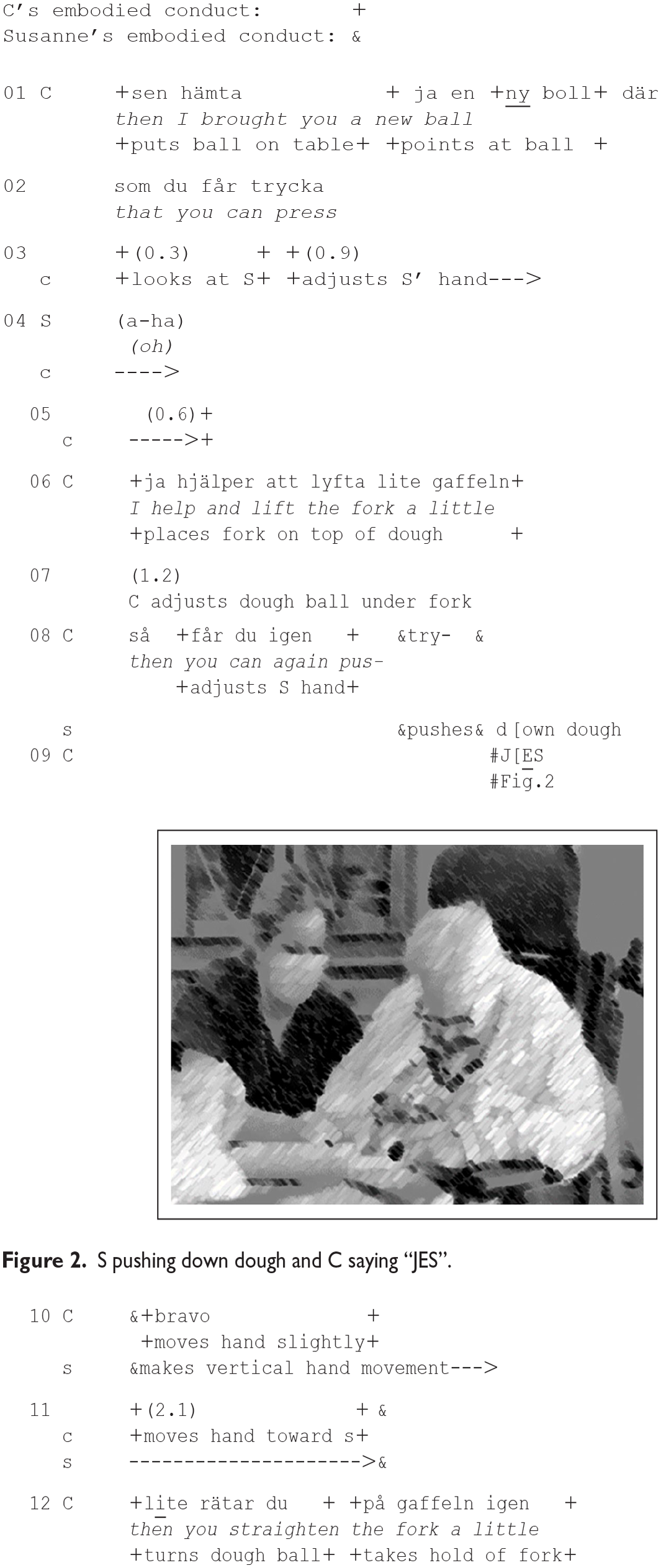
In Line 08, C produces a new directive that focuses solely on the proposed next action: the pressing down on the fork. Simultaneously with the verbal directive, C adjusts the position of Susanne’s hand, which has slid down to the side of the doughball. The adjustment places Susanne’s hand on the top of the doughball, in a better position for performing the next action. The directive in Line 08 is not syntactically complete, because C self-interrupts her utterance when Susanne starts pressing down the fork. She watches Susanne’s pressing down of the fork for as short while before she reacts to it with the positive assessment token J
Extract (2) exemplifies how caregivers can acknowledge residents’ attempts to perform a task by producing positive assessment tokens. The first positive assessment token was produced immediately after the resident had initiated her action, and the second when the activity had proceeded a little further. It is worth noting that the assessment tokens were accompanied by the caregiver first demonstrating readiness to intervene and then intervening by taking hold of the fork. Thus, it seemed to be the resident’s onset of the action and her attempt to perform the task, rather than a successful outcome, that were positively assessed, even though it is impossible to discern whether the assessment targets the actor’s abilities or her conduct.
Extracts (1) and (2) have demonstrated different strategies used by the caregivers to manage the resident’s performance of a task. Whereas the caregiver in (1) announced a demonstration and then took on the responsibility for the task, the caregiver in (2) carefully prepared for the resident’s performance one step at a time by producing verbal directives, touching, and handling the artifacts. Positive assessments were used in both strategies; in (1) to stress the resident’s performance even though the caregiver, in fact, was the primary actor, and in (2) to encourage the resident’s attempts to perform the task, even though these attempts did not seem to be entirely successful. The following extract, (3), exemplifies how positive assessments were used simultaneously with the resident performing manual tasks.
Encouraging autonomous activity
Sometimes, caregivers routinely produced positive assessments in situations where the residents aligned smoothly with the caregivers’ directives to undertake a task and the caregivers were monitoring residents’ performance. Here, positive assessments were used to encourage autonomous activity in situations where caregivers were monitoring residents’ performance. This is the case in Extract (3) in which the resident was the same, but the caregiver different, as in Extract (1).
Prior to (3), resident Astrid has agreed on brushing buns. The extract starts with caregiver C removing a spoon from a cup with an egg wash. She expresses completion of this task and orientation to the next phase with the boundary marker så där (“like this”), which marks that the previous phase is completed. The next action is initiated by her first giving the cup to A and pushing the baking sheet toward her. C facilitates Astrid’s performance by handing her artifact needed to perform the next action and pushing the sheet with the buns in the direction of Astrid. The actions are followed by Astrid starting to brush the buns (l. 06).
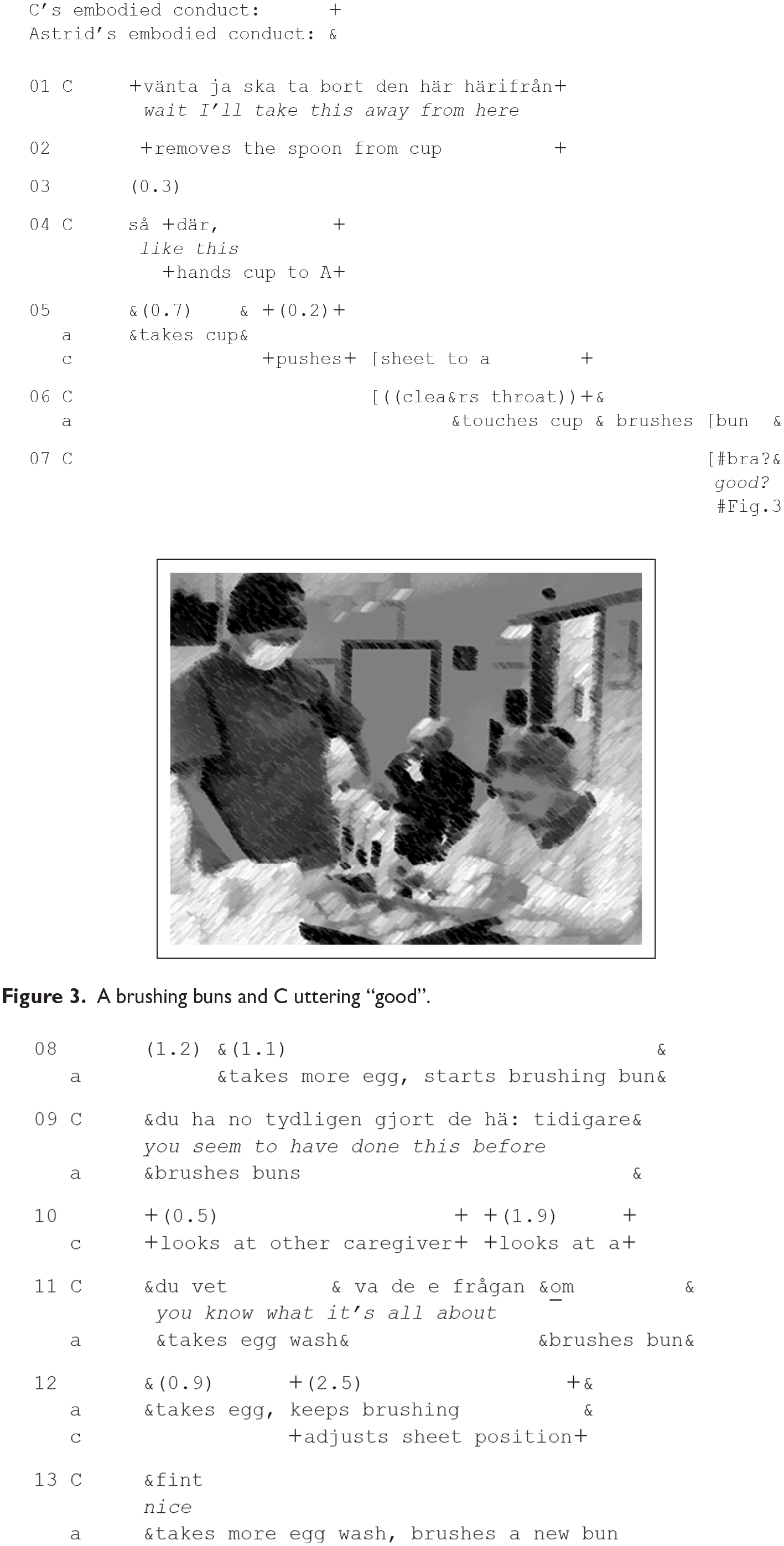
C’s first positive assessment token bra (“good,” l. 07; Figure 3) is uttered with rising intonation and produced simultaneously with Astrid brushing the bun. It can thus be classified as a response to Astrid’s action. When Astrid takes more egg wash and continues to brush another bun, C (l. 09) produces another assessment turn, du ha no tydligen gjort de här tidigare (“you seem to have done this before”). After watching Astrid’s behavior in the current situation, C expresses the conclusion that Astrid has previous experience with brushing buns, and this can be interpreted as an indication of Astrid’s success in performing the task. In Line 11, C produces a new positive assessment turn, which refers to Astrid’s experience and successful performance (du vet va de e frågan om, “you know what it’s all about”). In lines 09 and 11, C ascribes expertise to the person with dementia. Astrid continues brushing buns and C produces another assessment token, fint (“nice,” l. 15) while monitoring Astrid’s performance.
C produces a series of positive assessments simultaneously as she is monitoring Astrid’s activity and holding onto the baking sheet with the buns. Thus, she is standing by, ready to intervene if trouble occurs. Her positive assessments seem to have the dual function of providing continuous encouragement of the progress of the task and maintaining contact with the resident (cf. Jansson, 2016: 73–74). As noted by Jansson (2016: 81), caregivers can use any sign of response as an opportunity for contact with the resident. Here, the very progress of the task, such as Astrid brushing the buns, can obviously be seen as a source of encouragement and an opportunity for contact.
The series of positive assessments involves both the evaluation of the progress of the task and Astrid’s expertise. The first (l. 07) and the last (l. 13) assessments seemingly orient to the progress of the task, as in Extract (2), while the second (l. 09) and third (l. 11) turns refer to Astrid’s expertise. Here, a connection seems to exist between the syntactic form and the function: minimal tokens relate to the current performance, while syntactic and more elaborate turns orient both to the current task and to the resident’s general skills. This is in line both with the overall findings in the data and those of Leskelä (2023) who discussed minimal positive assessment tokens as a distinct category with the function of indicating transitions between phases in a task.
In Extract (3), Astrid was able to work more independently than the residents in Extracts (1) and (2). As in (2), the caregiver helped her by preparing the setting for a successful performance, for example, by handing her the needed artifacts. However, Astrid also manages to brush the buns independently, which gives the caregiver an opportunity to provide more general assessments of her skills.
Concluding discussion
This article investigated the role of positive assessments in baking sessions involving residents with dementia and professional caregivers. Engaging in meaningful activities, such as baking, can have a positive impact on residents’ quality of life, but their capacity to engage in such activities can be impaired because of dementia. Therefore, residents are dependent on the support of caregivers to carry out such activities. This article demonstrates how caregivers use positive assessments to facilitate residents’ task performance and deal with the dilemma between supporting resident performance and helping them out, resulting in a varying degree of intervention.
We can speculate that the variation in caregiver’s actions depends on the resident’s competence, which is certainly partially true. In Extract (2), the caregiver carefully adjusts the resident’s bodily position and the available artifacts step-by-step to make it possible for the resident to perform the action. The caregiver’s actions seem to be motivated by the residents’ needs. The caregivers’ ways of monitoring the activity also seem to be dependent on the caregivers’ personal preferences. Extracts (1) and (3) feature the same resident, Astrid; however, the caregivers participate in the activity in different ways. In Extract (1), the caregiver performs the activity in collaboration with the resident. Instead of standing by and monitoring the activity, the caregiver provides verbal instructions but holds onto the knife with the resident while they perform the activity together. However, in Extract (3), the caregiver only stands by and watches Astrid’s performance; however, slightly moving the baking sheet to make it easier for Astrid to brush the buns.
Previous research has indicated that positive assessments, especially of everyday tasks, can be patronizing and infantilizing in interaction involving older adults with dementia. However, this study does not provide evidence of a patronizing tone or residents reacting in a negative manner toward the assessments. Instead, we can reflect upon whether residents’ reduced functional capacity makes also minor success worth praising, without an undertone of infantilization. By delving into the details of social interaction, this work demonstrates the potential of positive assessments in managing the performance of older adults with dementia.
Footnotes
Appendix
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research for this study was supported by the Society of Swedish Literature in Finland. The authors declare no conflicts of interest.