
Abstract
As opportunities for social interactions proliferate online, questions arise as to how engagement in such activities may relate to mental health. Given older adults’ shrinking networks and increasing use of information and communication technologies (ICTs), online interactions could offer alternatives for connections that could ultimately benefit older users’ mental health. This article examines associations between older adults’ online social engagement and their mental health. Using data from an online survey of older adults ages 60+, we find positive and negative associations between different forms of online social engagement and anxiety. In terms of depression, two forms of online social engagement showed positive associations with this mental health indicator. Our results can help explain inconclusive findings of previous research on ICT use and mental health by looking at how specific online social activities relate to mental health.
Introduction
Virtually, all societies are being challenged with the following two broad trends: (1) The rapid dissemination of information and communication technologies (ICTs) and (2) the rapid growth in the number and proportion of older persons (60+ years) in their populations (Charness, 2019; Czaja et al., 2019; United Nations, 2019; World Health Organization, 2015). Accordingly, there is also a growth of older adults using ICTs (Hunsaker and Hargittai, 2018). Central to these societal developments is the question of how the older population’s use of ICTs is related to their mental health, as retirement age and the concomitant potential decrease in regular social contacts are potential risk factors for poor mental health in terms of loneliness, depression, and anxiety (Curran et al., 2020; Fernández-Niño et al., 2018). On one hand, ICT use (both the use of devices, such as smartphones or tablets, and of services such as social network sites, SNSs, or information sites on the Internet) can reduce loneliness and enhance older users’ mental health (e.g. Forsman and Nordmyr, 2017; Schlomann et al., 2020). On the other hand, other research has found detrimental effects of ICT use on mental health outcomes—especially if ICTs are used in a problematic fashion (e.g. Meshi et al., 2020). This question about the association between older adults’ ICT use and mental health is also relevant because a digital inequality exists between younger and older seniors in terms of adoption of specific services, the use of ICTs, and in terms of the skills to use these technologies in a personally beneficial way (e.g. Hargittai et al., 2018; Hofer et al., 2019; Wu et al., 2015). Thus, examining the link between mental health and ICT use seems especially relevant among older adults.
Research suggests that using the Internet might serve as a remedy for depressive symptoms or anxiety (Cotten et al., 2014; Francis et al., 2019; Wade, 2010). Khosravi et al. (2016), for instance, found that ICTs, and especially socially relevant ICTs such as social management systems (special software designed for older adults), can be used to reduce loneliness and (perceived) social isolation―a central predictor for depression and anxiety―among older adults. In addition, research suggests that older adults carefully manage their interactions within the digital environment in order to improve the quality of their lives (Sinclair and Grieve, 2017). Thus, the use of ICTs could help against mental health issues such as anxiety and depression. However, other studies suggest negative links between older adults’ mental health and their use of the Internet (Hunsaker et al., 2020; Kraut et al., 1998) resulting in inconclusive findings in the literature.
Among the myriad of different things a person can do online, one group of behaviors relevant for older adults’ mental health in general, and depression and anxiety in particular, is the social use of ICTs (Chang et al., 2015b; Seabrook et al., 2016). We refer to this kind of ICT use as online social engagement (Burke et al., 2010, 2011; Nguyen et al., 2020). Online social engagement can take many different forms, such as participation in online forums or discussions by asking questions or giving answers, looking at photos of family and friends whether found on a site or received directly. In short, it is a form of online behavior that involves others. Social network sites (e.g. Facebook and Instagram) are one prominent example of services that facilitate these kinds of behaviors. However, online social engagement is not limited to such sites, it can happen in other online contexts as well, such as direct interpersonal communication through messaging or on mailing lists and various forums.
On the one hand, socially engaging online can help users affirm and express their identity and emotions, and socially interact with others to counteract loneliness and ensuing depression and anxiety. The mechanism between social connectedness and mental health, or the lack thereof, is well documented in research. Santini et al. (2020), for instance, found lower social connectedness (i.e. social network size and range, frequency of social interactions) to be associated with perceived isolation, which in turn was linked to depression and anxiety. Using longitudinal data (five waves, 5 years apart), Cacioppo et al. (2010) showed that loneliness predicted depressive symptoms after 5 years. Thus, social connectedness seems to be a key factor in a person’s mental health (see also Baumeister and Leary, 1995). The deeply engrained need to feel connected with people and the concomitant maintenance or improvement of mental health can, at least in part, be satisfied by socially engaging online (for a review, see Forsman and Nordmyr, 2017). On the other hand, using ICTs in a social manner can also have dysfunctional effects on older adults’ mental health, for instance, if usage patterns are problematic, result in negative social comparisons, or when ICT use is a replacement of or a compensation for other social interactions (Hofer and Eden, 2020; Kraut et al., 1998; Meshi et al., 2020; Schlomann et al., 2020; Seabrook et al., 2016). In this study, we examine the relationship between different forms of online social engagement and older adults’ depression and anxiety.
Literature review
Depression and anxiety are often regarded as crucial determinants of a person’s mental health and his or her well-being. Keeping these two mental health issues at bay is critical in the process of healthy or successful aging that is defined as “the maximization of gains and the minimization of losses” (Freund and Riediger, 2003: 612; Urtamo et al., 2019). In the context of this study, gains and losses can be regarded as suffering from the least amount of depressive and anxiety symptoms (gain) or becoming anxious and depressive (loss). As people age, the ratio of gains and losses in general tends to become smaller (Freund and Riediger, 2003). To manage gains and losses people rely on resources—both tangible (e.g. money) and intangible ones (e.g., social interactions; Freund and Riediger, 2003). Engaging socially online can be regarded as an intangible resource to manage mental health (Hofer, 2016). In addition, resources have to be used prudently in order to achieve gains and avoid losses. That is, online social engagement might not be beneficial per se. In order to have positive effects, this resource needs to be utilized pragmatically (Freund, 2008). In addition, different forms of online social engagement might have different effects in the process of successful aging.
Prior work has repeatedly shown positive social connectedness as a resource to manage depression and anxiety (e.g. Baltes and Lang, 1997; Cacioppo et al., 2010; Steger and Kashdan, 2009). Social connectedness can also be pursued using ICTs and research shows that these technologies are a feasible tool to enhance social connectedness (Barbosa Neves et al., 2019). However, research on the link between depression and anxiety and socially engaging online (e.g. through SNSs) provides an unclear picture. In their review of related work, Pantic et al. (2012) found a positive association between depressive symptoms and SNS use. That is, the more a person spends time on an SNS, the more likely he or she shows depressive symptoms. Similarly, Tandoc et al. (2015) found Facebook use to be related to higher levels of depression. However, other studies found no relationship (Bessière et al., 2008; Jelenchick et al., 2013).
This lack of consistency in findings could be due to the age of participants. Pantic (2014) argues that different age groups may use SNSs differently and react differently to the content on and challenges posed by such sites. Older adults often use SNSs for social purposes (e.g. Chang et al., 2015a). However, difficulties using this technology could lead to less positive or negative effects, such as frustration or even anxiety (Ballantyne et al., 2010; Chang et al., 2015a). In terms of social online engagement being a resource in the process of successful aging, we could argue that it has to be used in a conscious way in order to have positive effects on a person’s mental health (Hofer, 2016).
Another reason for varied outcomes could be linked to different purposes of use; Shaw et al. (2015), for instance, found no connection between passive use of Facebook and anxiety, but did find a positive relationship between its communicative and social use and anxiety. In terms of using ICTs as a resource in the process of successful aging, we could argue that a more active social use of ICTs might have a positive effect on older adults’ mental health, whereas a more passive use of this resource may have negative effects. More recent research has taken these age- and use-related considerations into account. Analyzing the online experiences of older adults in particular, Hunsaker et al. (2020) found that belonging to certain online communities and engaging in meaningful online discussions about some topics were related to higher levels of anxiety. Choi and DiNitto (2013) show that email and texting linked to higher anxiety levels. These studies are examples of how helpful it can be to disaggregate types of online engagement. Similarly, applying a functional approach by differentiating between four types of Internet use, Lifshitz et al. (2018) found that using the Internet for leisure activities and task performance is negatively related to depressive symptoms. Communication online, however, was not related to depression in either positive or negative ways.
Nguyen et al. (2020) also go beyond the basic concept of (frequency of) social media use to look at active online social engagement, such as looking at photos or clicking on links. Their study examines how such activities relate to social capital and find a positive association with online bridging social capital. In this study, we follow Nguyen et al. (2020) by examining the hitherto unclear connection between online social engagement and depression as well as anxiety.
Research questions
Previous findings point to positive associations between online social engagement and anxiety among older adults (Choi and DiNitto, 2013; Hunsaker et al., 2020). That is, the more people socially engage online, the higher their anxiety. For instance, false expectations, social comparison processes, or even negative feedback by other users could increase anxiety levels. However, based on past work on the association between social media use and anxiety (Cauberghe et al., 2021), one could also argue that online social engagement is related to decreases in anxiety when people use it as a way to connect with others, to improve their social connections, and to find humor. Specifically, positive social interactions and relationships could act as a form of coping and enhance self-esteem, happiness, or life satisfaction, which could counteract feelings of anxiety (Cauberghe et al., 2021; Seabrook et al., 2016). The same arguments apply to associations between online social engagement and depression. That is, online social engagement could either be associated with increases or decreases in depression. Because research on the relationship of online social engagement and mental health is limited instead of constructing hypotheses, we pose the following research questions (RQ1 and RQ2):
RQ1. Are different forms of online social engagement related to higher or lower levels of anxiety among older adults?
RQ2. Are different forms of online social engagement related to higher or lower levels of depression among older adults?
Method
Data collection
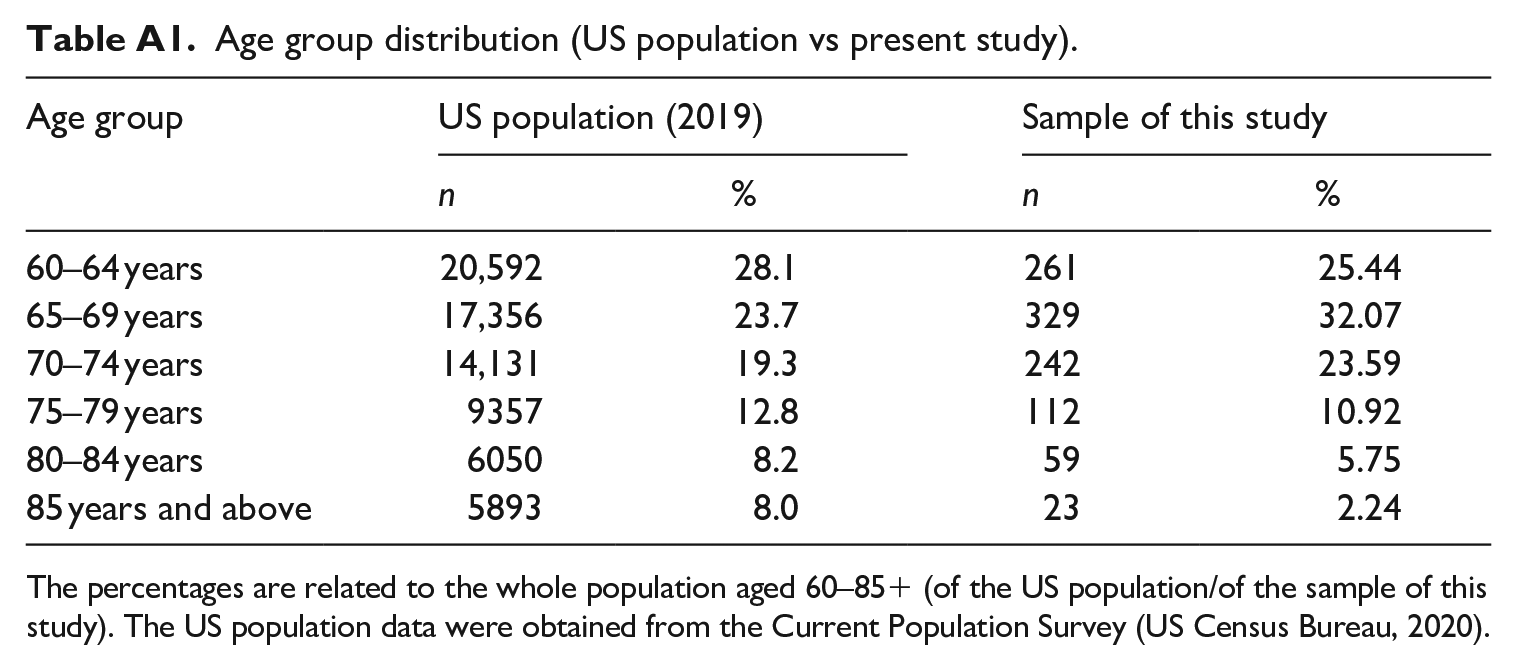
We surveyed 1026 older adults in the United States aged 60 and above in July 2018. The age cutoff follows the definition of old age by the World Health Organization (2015). We contracted with the online research firm Cint to administer our study to a diverse group of older adults. Cint uses a double opt-in procedure to recruit respondents to its panels. To achieve a diverse sample, we quota sampled on various older age groups, gender, race and ethnicity, and education based on US Census figures. Age quotas ensured that our sample did not simply include younger-aged older adults allowing us to compare people of different ages across this population (see Table A1 for a comparison of the US population and the sample of this study). We included the other quotas to make sure we had a diverse sample given findings in digital inequality scholarship about variations in Internet use by sociodemographic factors (e.g. Hargittai and Hsieh, 2013). Respondents were sent an invitation to participate in the survey and received compensation for it. They were allowed to skip any questions they did not want to answer. The study complied with the ethical requirements of the research institution.
Measures: dependent variables
Anxiety
We measured anxiety symptoms using the Beck Anxiety Inventory (Beck et al., 1988), which has been shown to be suitable for older adult populations (Wetherell and Areán, 1997). The scale asks respondents about the occurrence of five different anxiety symptoms over the past week (e.g. “I had fear of the worst happening,” “I was nervous”). Response items included 1 = never, 2 = hardly ever, 3 = some of the time, and 4 = most of the time. We averaged the responses over the five items so that possible scores ranged from 1 to 4, and higher scores indicated more anxiety symptoms. The mean anxiety score was 1.5 (SD = 0.5, Cronbach’s α = .78) and scores ranged from 1.0 to 3.8.
Depression
We relied on the widely used Center for Epidemiologic Studies Depression Scale (CES-D Scale) to assess depression (McDowell, 2006; Radloff, 1977), a measure included on the US Health and Retirement Study and one that other researchers studying Internet uses have also utilized (Cotten et al., 2014). The question asks respondents about the frequency with which they had experienced eight feelings in the past week (e.g. “I felt depressed,” “I felt lonely,” “I felt sad”) with the following answer options: “rarely or none of the time (less than 1 day)”; “some or a little of the time (1–2 days)”; “occasionally or a moderate amount of time (3–4 days)”; more or all of the time (5–7 days).” After reverse coding two of the items (“I was happy,” “I enjoyed life”), we averaged these scores. The mean depression score was 1.6 (SD = 0.6, Cronbach’s α = .87) and scores ranged from 1.0 to 4.0.
Measures: independent variables
Sociodemographics
We asked about year of birth to measure age (M = 69.3 years, SD = 6.2). We asked gender giving the following options: (a) male, (b) female, and (c) other, please specify. Over half the sample (57%) responded female; no one chose “other.” To measure race and ethnicity, following US Census conventions, we first asked whether the respondent was of Hispanic or Latino origin and then about race using the following categories: White, Black or African American, Asian, American Indian or Alaska Native, Native Hawaiian or Pacific Islander, and/or Other, please specify. The sample is 82% White (the base in the models), 9% Black, 6% Hispanic, and 3% Asian.
Respondents provided their highest level of school completed or highest degree received using the categories: less than a high school degree, high school graduate (high school diploma or equivalent including GED), some college but no degree, associate’s degree, bachelor’s degree, and advanced degree (e.g. master’s, doctorate). We recoded these into the following three categories: 23% completed high school or less (the base in the models), 40% completed some college, and 37% completed college or more. We asked about household income through 12 categories, which we then recoded into a continuous variable using midpoint values (M = US$60,042, SD = US$45,161). To determine household size, we asked for the total number of people currently living in the respondent’s household, including themselves; 33% of the sample lived alone, 52% lived with one other person, 9% lived with two people, and 6% lived with three or more people (M = 1.9, SD = 1.0). In regression analyses, we logged the value of household size to address the diminishing returns of having more individuals in a household. Table 1 summarizes the characteristics of our sample.
Sample characteristics.
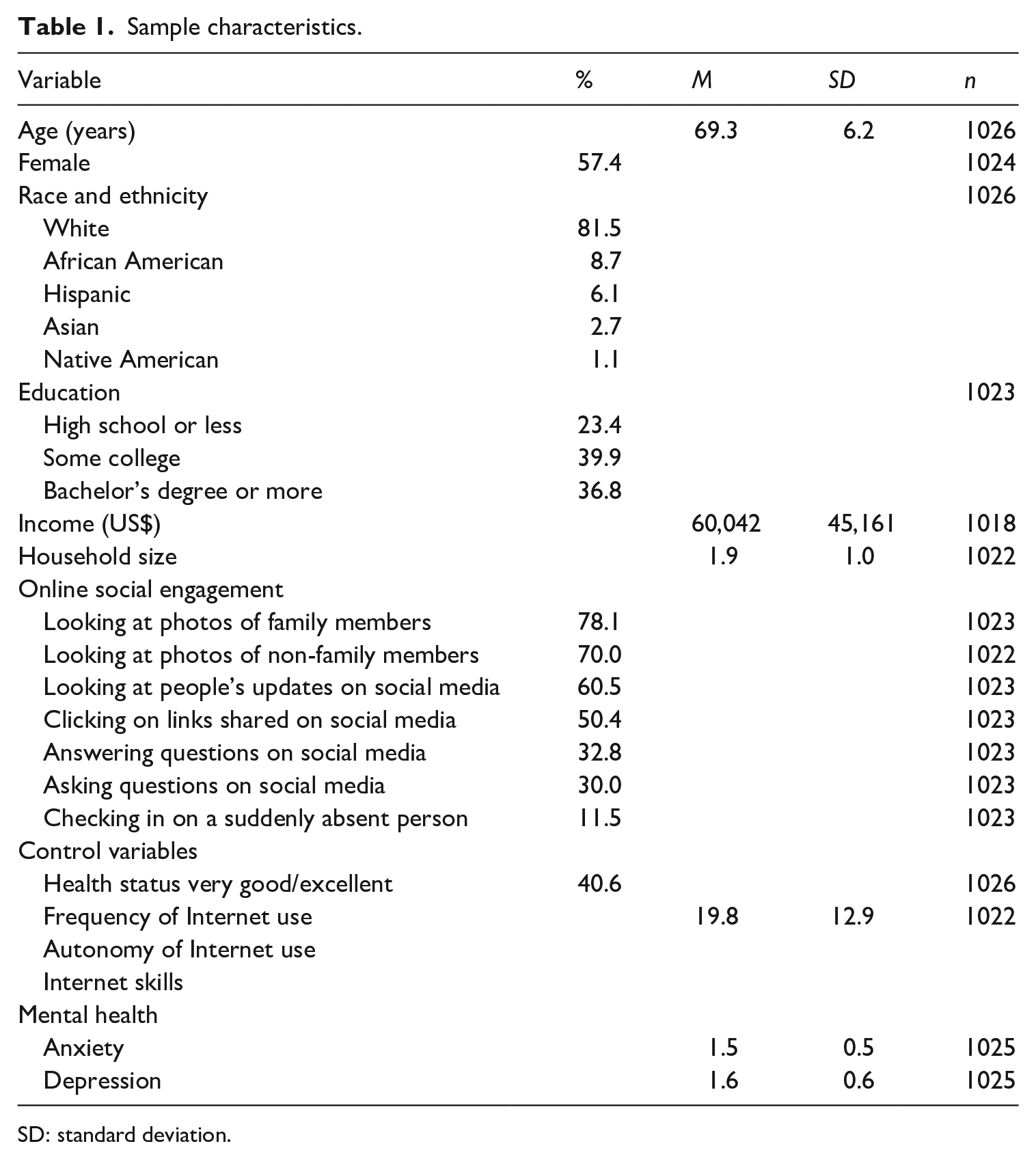
SD: standard deviation.
Online social engagement
Inspired by Burke et al.’s (2011) distinction of different Facebook communication types, we created platform-agnostic social media engagement measures. We focused on specific online activities to move past prior work that tends to consider Internet uses or social media uses more generally than exploring how specific behaviors differ. We asked, “How often, if ever, have you done the following online using a computer, a tablet, or a smartphone?” The seven activities were the following: “looked at the photos of family members,” “looked at the photos of people you care about who are not family members,” “looked at people’s updates on social media,” “clicked on links people shared on social media,” “asked a question in a forum/social media,” “answered a question someone else had asked in a forum/on social media,” and “checked in on a person who was suddenly absent from an online community or group.” Answer options included “never,” “once,” and “two or more times.”
We dichotomized these variables to make a theoretical distinction between the less engaged (0) by collapsing those who indicated “never” or “once,” and the more engaged (1) who indicated “two or more times.” As the figures in Table 1 show, quite a few respondents had experiences with several of these activities. Looking at photos of both family members and others were the most popular at 78% and 70%, respectively. Over half of the sample also reported looking at people’s updates (60%) and clicking on links shared on social media (50%) as things they have done more than once.
Another way to approach these activities is to group together the more passive forms of engagement (looking at photos, checking status updates, clicking on links) versus the more active forms (asking or answering questions, checking in on someone), which not only makes sense conceptually, but which factor analysis also revealed go together well in that way. Due to space constraints, we do not report the outputs of these analyses, but do discuss them below.
Perceived health
Using a widely adopted question to assess self-reported health (Global Programme on Evidence for Health Policy, 2000: 4), we asked, “In general, how is your health?” with the following five answer options: “excellent,” “very good,” “good,” “fair,” “poor.” We created a dummy variable indicating excellent or very good health (=1).
Internet experiences
To avoid reporting spurious associations between online social engagement and mental health, we included the following three control measures of Internet experiences: frequency of Internet use, autonomy of use, and Internet skills. To assess time spent online, we asked, “On an average weekday, how many hours do you spend visiting Web sites including social media (but not counting e-mail)?” Response options included none (coded as 0), more than zero, but less than 1 hour per day (0.5), 1 hour (1), 2 hours (2), 3 hours (3), 4 hours (4), 5 hours (5), and 6 hours or more (7). We asked the same question about the average weekend. We recoded responses by multiplying the weekday values by 5 and the weekend values by 2, then summing these for a possible range of 0–42 hours. The sample reported using the Internet an average of 20 hours per week (SD = 12.9). We logged this final number of hours in the regression analyses to account for diminishing returns of additional time spent online.
Autonomy of use is a measure of the extent to which a person can use the Internet when and where he or she wants and has been shown in the literature to be an important correlate of various online experiences (e.g. Hassani, 2006; Schradie, 2011). To gauge autonomy of use, we asked at which of nine locations (e.g. own home, family member’s home, community center, on-the-go) respondents could use the Internet if they wanted to and aggregated these into a summary score, which averages 2.8 locations (SD = 1.9). To assess Internet skills, we relied on a widely used measure (Hargittai and Hsieh, 2012) that asked respondents their level of understanding of several Internet-related terms (e.g. jpg, spyware, advanced search) on a 1–5 scale and creates a mean score of them, which was 2.9 (SD = 1.1, Cronbach’s α = .94).
Results
Bivariate results
We first turn to bivariate results. As displayed in Table 2, both depression and anxiety are related to some forms of online social engagement, but not others. Checking in on a person who was suddenly absent from an online community—something 12% of respondents reported having done more than once—correlates positively with both depression and anxiety. In addition, anxiety positively correlates with answering questions online (something 33% had done) and looking at photos of others (70% occurrence).
Zero-order correlations between study variables.
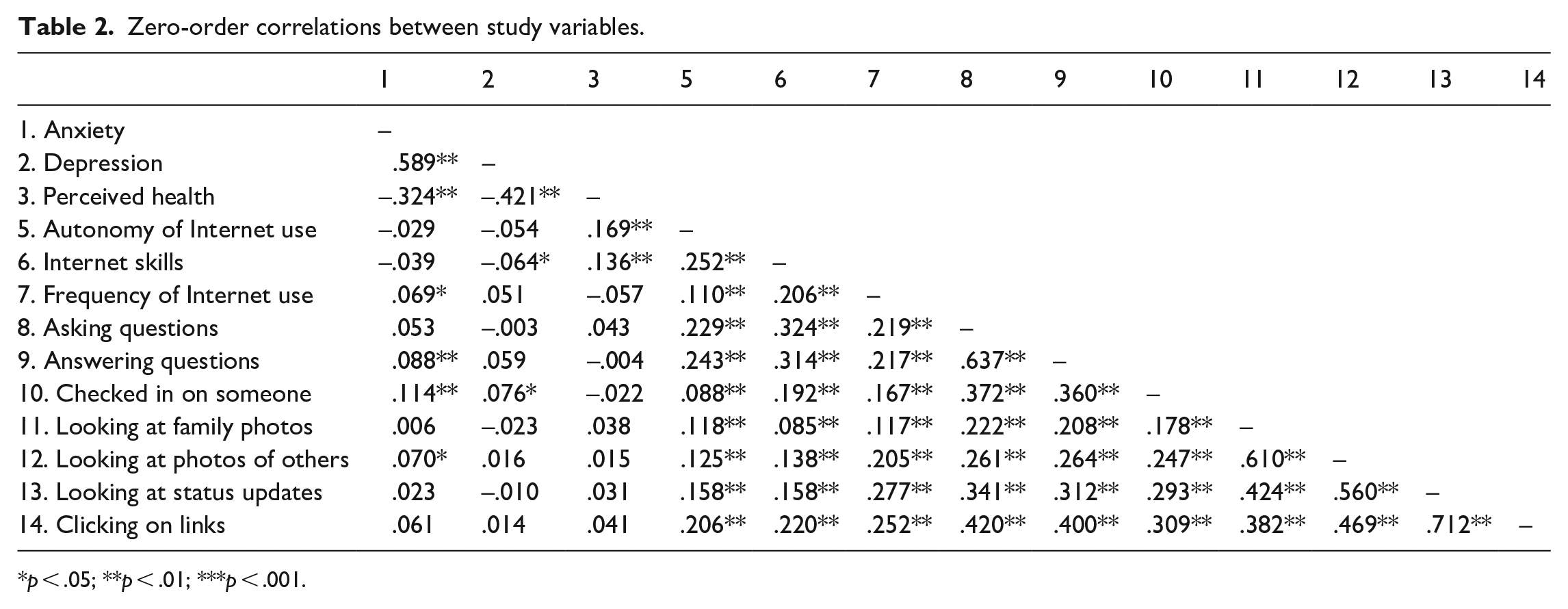
p < .05; **p < .01; ***p < .001.
Multivariate results
We conducted ordinary least squares (OLS) regression models in which we controlled for sociodemographic variables, perceived health, and general Internet experiences (i.e. frequency of use, autonomy of use, and Internet skills). Among the sociodemographic variables, being female was associated with anxiety (β = .08, p = .010). By far, the strongest association was the one between perceived health and anxiety (β = −.32, p < .001). The general Internet experience variables were not related to anxiety.
In terms of depression, we found a similar pattern. Being female (β = .08, p = .004), lower household income (β = −.09, p = .007), and being African American (β = −.08, p = .006) were associated with depression. Again, perceived health showed a strong relationship with depression (β = −.41, p < .001); general Internet experiences did not. Results are displayed as Model 1 in Tables 3 and 4.
OLS regression model for anxiety.
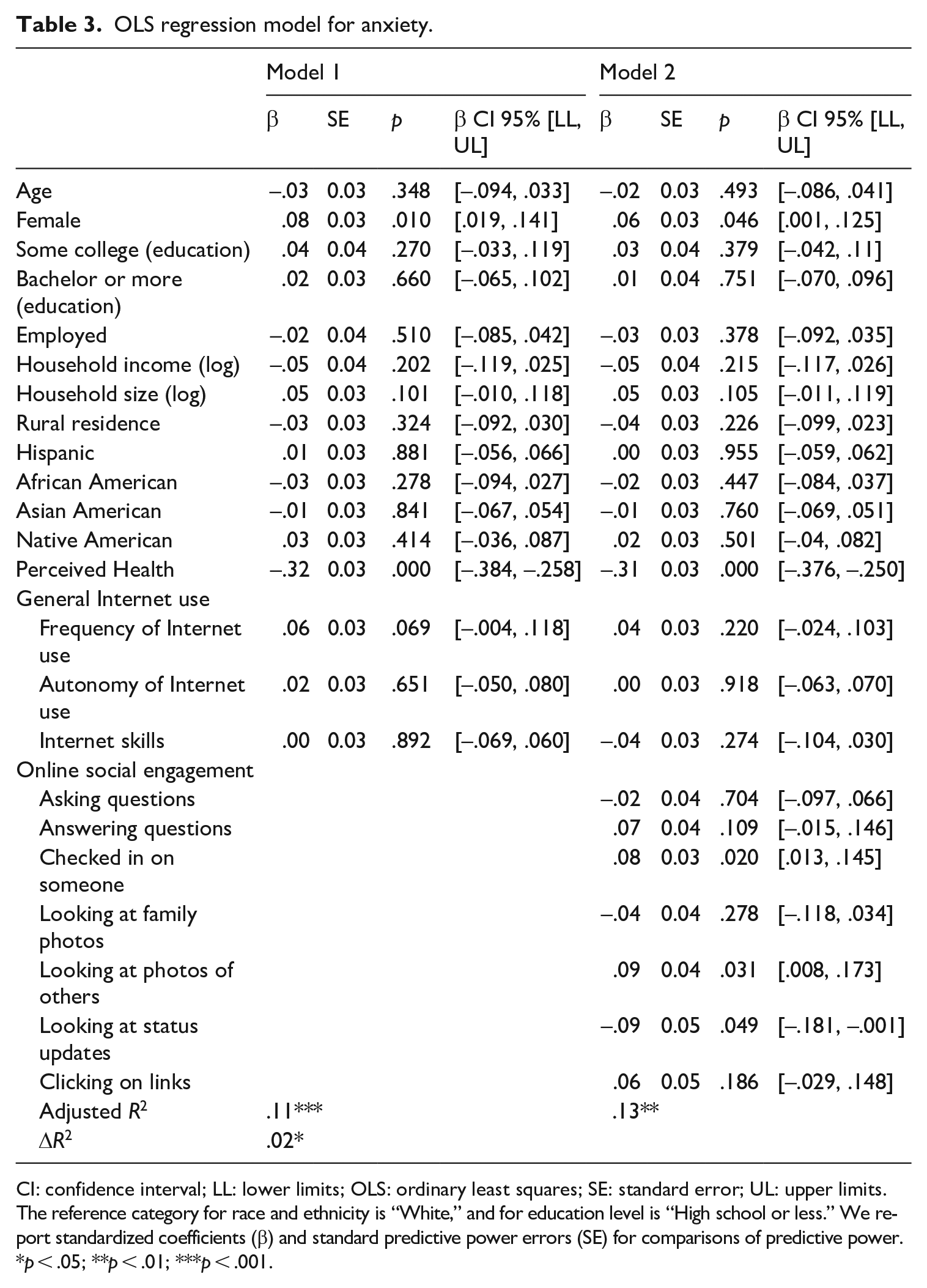
CI: confidence interval; LL: lower limits; OLS: ordinary least squares; SE: standard error; UL: upper limits.
The reference category for race and ethnicity is “White,” and for education level is “High school or less.” We report standardized coefficients (β) and standard predictive power errors (SE) for comparisons of predictive power.
p < .05; **p < .01; ***p < .001.
OLS regression model for depression.
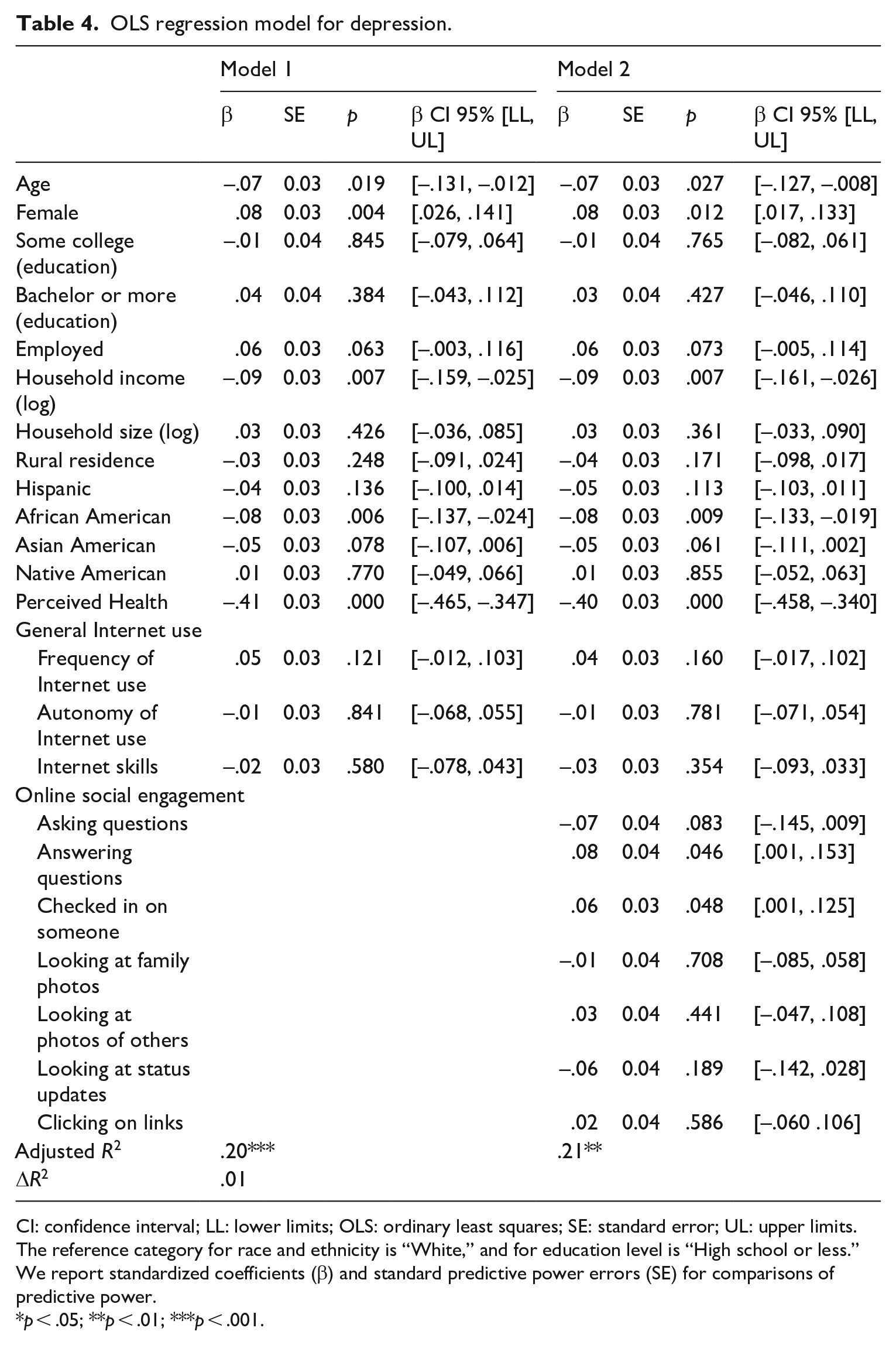
CI: confidence interval; LL: lower limits; OLS: ordinary least squares; SE: standard error; UL: upper limits.
The reference category for race and ethnicity is “White,” and for education level is “High school or less.” We report standardized coefficients (β) and standard predictive power errors (SE) for comparisons of predictive power.
p < .05; **p < .01; ***p < .001.
In Model 2 of these two tables, we added the online social engagement variables. We found two ways of socially engaging online that were related to anxiety; checking in on someone was positively related to anxiety (β = .08, p = .020) while looking at status updates was negatively related to anxiety (β = −.09, p = .049). That is, the more a person in our sample is likely to look at status updates, the lower she or he scores on anxiety. Two forms of online social engagement were related to depression: answering questions (β = .08, p = .046) and checking in on someone (β = .06, p = .048). Both ways of engaging socially online showed a positive relationship with depression, that is, higher likelihood of such engagement was linked to higher depression. When we ran these models with the groupings of passive versus active online engagement, some of these results were robust, but not all. This may be due to some canceling each other out. Below, we reflect on why running the analyses with the individual activities separately is meaningful.
Discussion
We set out to examine the relationship between different forms of online social engagement and anxiety (RQ1) and depression (RQ2). Given varied findings in the literature about the link between social uses of the Internet and mental health, we did not pose specific hypothesizes. Our study joins others that have found a positive relationship between Internet use and both depression and anxiety (Hunsaker et al., 2020; Pantic et al., 2012; Tandoc et al., 2015). However, we focused on specific forms of using the Internet: online social engagement.
As our findings show, specific activities matter. In particular, checking in on someone who was suddenly absent from an online community was positively related to anxiety. Research shows that in the offline world, the sudden loss of a person can increase anxiety (Kendler et al., 2003). While we cannot say for sure that the online activity we described is about the death of someone, it may be that online absence is linked to the loss of someone and such loss has negative mental health associations when experienced in the online environment as well.
Looking at status updates was negatively related to anxiety; older adults who were more likely to have looked at status updates more than once had lower levels of anxiety. Status updates are likely to show a positive image of a person (Krämer and Winter, 2008) and this, in turn, seems to counteract feelings of anxiety in our sample. Taking into account research showing a general tendency to focus on positive aspects of a given object, a person, or a situation and selectively avoiding negative information (a so-called positivity bias; Charles and Carstensen, 2010), this finding seems meaningful. Our result suggests that older adults’ positivity bias also seems to play a role in the online environment. This result, at first sight, seems to go counter to findings about young adults, which suggest that through social comparison they react negatively to other people’s updates (e.g. Tandoc et al., 2015). However, considering the positivity bias that is prevalent among older, but not younger people (Charles and Carstensen, 2010), our finding seems not that contradictory.
Interestingly, looking at photos of others (i.e. not family members) was positively related to anxiety, that is, the higher likelihood of this activity is linked to higher anxiety. This finding could be explained by research about how older people’s social network shrinks with age (Charles and Carstensen, 2010). Older people tend to limit their social network to family and very close friends as they age. Looking at photos of people other than one’s close family might be upsetting because it calls attention to one’s limited social network.
There are other possible explanations for the different findings respecting engagement with status updates versus photographs. People may react differently to textual versus visual cues about others. Alternatively, these types of activities happen in different online environments. Seeing status updates is more likely to happen on social media platforms while seeing photos of others can happen in more varied online environments. Future research can further probe these relationships by (a) focusing more on different messaging modes—textual, visual, animated, vocal and (b) being more explicit about where online social engagement takes place. Given that in recent years, the vast majority of related research has focused on social media, we purposefully wanted to move beyond that one type of online venue. Nonetheless, it seems having more information about the platforms where social interactions take place may be an important part of understanding their implications for well-being.
In terms of depression, we found that checking in a suddenly missing person and answering questions online were positively related to depressive symptoms, that is, likelihood of engaging in these activities is linked to higher depression. This finding also goes along with the above-mentioned research showing detrimental effects of loss. Answering questions could be interpreted as some form of outreach to a community when non-mediated forms of outreach to a community is not possible anymore (for instance, in the case of illness). Research suggests that such compensatory use of (digital) media is related to decreases in well-being (Hofer and Eden, 2020). Hence, such use could also increase depression.
Other forms of social engagement, such as looking at family photos and asking questions, were not related to depression or anxiety. In addition, the explanatory power of the forms of online social engagement in terms of anxiety and depression is marginal. Other variables known for being associated with depression and anxiety (e.g. perceived health) seem to be more important than socially engaging online. So while our study contributes to going deeper in what types of online actions may be related to mental health, it is in line with existing work in showing that in-and-of themselves many such activities do not exhibit strong associations in either direction (see also Büchi, 2020).
The fact that grouping activities into two summary “passive social engagement” and “active social engagement” variables does not reflect the findings of analyses that look at each activity separately reinforces the value in using measures more nuanced than summary indices. It may be that one activity shows a negative relationship with mental health outcomes while another shows a positive one (as is indeed the case here in this study), but collapsing them into one measure then cancels out these findings. As online social engagement options multiply and proliferate across various platforms, the need for differentiating between specific activities will likely grow. There is certainly value in classifying actions by type, but when data sets are able to have more nuance, it can be meaningful to take advantage of them.
Like all papers, ours also has limitations. Our findings are based on cross-sectional data, which do not allow for causal inference, as we are only able to examine undirected associations. There is a good chance that anxiety, depression, and online social engagement reinforce each other over time (see Slater, 2007), but this is not something we can test. Ideally, future studies will be able to examine associations between online social engagement and mental health longitudinally to be able to determine the direction of these associations. For instance, a measurement burst approach (Hofer, 2020) could be applied by which usage patterns (daily or weekly) can be linked with depression and anxiety symptoms over time. Using this approach, short-term developments can be used to explain long-term developments in these two sets of variables. In addition, using a measurement burst approach (and other longitudinal research techniques) enables researchers to disentangle inter- and intraindividual variance and effects (and their direction) over time (e.g. Büchi, 2020).
Conclusion
Analyzing data about a national sample of US adults 60+ years, we show that certain forms of online social engagement are linked to higher levels of anxiety and depression, while other types are related to lower levels. In light of the concept of successful aging, we conceptualized online social engagement as a resource to manage gains and losses in terms of mental health. ICT use, in general, can be conceived of as a resource in the process of successful aging (Hofer, 2016; Hofer and Eden, 2020). However, more specific forms of using ICTs (i.e. online social engagement) can also be used as a resource.
Our results also show that general Internet experiences (frequency of use, autonomy of use, and Internet skills) are neither linked with anxiety nor with depression. Therefore, we believe that our approach of disaggregating online social engagement activities rather than looking at general Internet use measures is important to gain a deeper understanding of what it is about online engagement that may matter for older adults. These findings also help shed light on why certain previous studies have not found a relationship between Internet use and mental health; their measures were too general and by not focusing on specific activities, their overall measures may have masked the effects of specific activities as they may cancel each other out. Given the countless ways in which people can use ICTs nowadays, it is increasingly important to have measures represent specific types of usage rather than grouping them all together. In light of our findings, we encourage future work to employ more specific questions about what it is exactly that older adults are doing online to get a better sense of what types of online actions matter for their mental health.
Footnotes
Appendix 1
Age group distribution (US population vs present study).
| Age group | US population (2019) | Sample of this study | ||
|---|---|---|---|---|
| n | % | n | % | |
| 60–64 years | 20,592 | 28.1 | 261 | 25.44 |
| 65–69 years | 17,356 | 23.7 | 329 | 32.07 |
| 70–74 years | 14,131 | 19.3 | 242 | 23.59 |
| 75–79 years | 9357 | 12.8 | 112 | 10.92 |
| 80–84 years | 6050 | 8.2 | 59 | 5.75 |
| 85 years and above | 5893 | 8.0 | 23 | 2.24 |
The percentages are related to the whole population aged 60–85+ (of the US population/of the sample of this study). The US population data were obtained from the Current Population Survey (US Census Bureau, 2020).
Acknowledgements
The authors are grateful to Amanda Hunsaker for her contributions to data collection.
Author contributions
Matthias Hofer contributed to statistical analyses, writing, and editing and Eszter Hargittai contributed to data collection, writing, and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.