
Abstract
This study aimed to examine whether depression mediated the association between successful aging (SA) and death anxiety (DA) in middle-aged and older people with hypertension. A survey design (N = 298) assessed demographic variables associated with participants (sex, age, place of residence, cigarette smoking, alcohol habits, physical activity, social activity, chronic medical illness burden), the Successful Aging Inventory (SAI), and the Patient Health Questionnaire (PHQ-9), the Templer Death Anxiety Scale (T-DAS). Pearson Correlation Analysis and Regression analysis were performed in the data analysis. In addition, AMOS was used to analyze the mediator variable effects. Results indicated a negative correlation between SA and depression (r = −.199, p < .01), while a positive correlation was observed between depression and DA (r = .277, p < .01). Regression analysis reported that SA and depression significantly positively predicted DA (F = 4.013, R2 = .111, p < .01). the structural equation model showed that depression mediated the effect of SA on DA (χ2/df = 3.055, p < .01, RMSEA = 0.083, CFI = 0.960, IFI = 0.961, GFI = 0.952, PGFI = 0.508, PNFI = 0.628, PCFI = 0.640). It was determined that depression mediated the association between SA and DA. The study suggests that prevention and control of depression can decrease death anxiety in middle-aged and older people with hypertension.
Introduction
Death is a fact anybody is unable inescapable at one point in life. Death anxiety (DA) is defined as fearful feelings and unpleasing thoughts about death and dying, DA is a universal instinct and defensive reaction to protecting oneself when someone feels threatened by death (Lehto & Stein, 2009). Although DA is a general phenomenon in all societies, lasts from birth to the end of one’s life, and causes aversive emotional reactions in people, older people and the sick may be more prone to DA when they encounter death-related events or extreme psychological stress compared to younger people (Missler et al., 2011). As a significant stressor, chronic disease can instill patients with the fear of death, and experience various forms of psychological distress in addition to physical health problems, including depression, anxiety, and disappointment (Bailey et al., 2019; Gulbahar Eren et al., 2023; Khodarahimi et al., 2021). DA is one of the most prevalent psychological states in patients with chronic disease, which can bring about adverse consequences and compromise the quality of life (Gulbahar Eren et al., 2023; Khodarahimi et al., 2021; Wu et al., 2002). The mental health status of middle-aged and older people in China is not optimistic, and they undertake heavy responsibility and pressure in society and families (Cavusoglu et al., 2020; The, 2016; Wu et al., 2002). Middle-aged and older people with hypertension suffer a variety of physiological and psychosocial functions impaired, resulting in a decline of labor capacity and activities of daily living, frailty, and worthlessness, and are prone to negative emotions, such as DA (Li et al., 2020; Pettey et al., 2016; Segel-Karpas & Bergman, 2022; Shen et al., 2022; Y. Zhang et al., 2018; Zhou et al., 2021). DA is higher in middle-aged adults than in the elderly (Barnett et al., 2018). A study in China reported that almost 17% of adults suffer at least moderate DA (Tang et al., 2021), and at least moderate DA was reported by 32% to 43% of patients with cancers (Eggen et al., 2020), and 70% of patients with cardiovascular disease (Gulbahar Eren et al., 2023; Valikhani, 2015). However, there is no literature reporting the level of DA in hypertension patients.
In the prior literature, DA has been researched to be associated with many variables, such as age, gender, education, religion, culture, illness, mental health, self-esteem, personality traits, purpose in life, social support, life expectancy, et al (Feng et al., 2021; Jung, 2018; Kahraman & Erkent, 2022; Khodarahimi et al., 2021; Oker et al., 2021; Özdemir et al., 2021; Rashedi et al., 2020; Soleimani et al., 2016). Depression as a mental health problem, is an important factor in DA (Gundogan & Arpaci, 2022). Successful aging (SA) indicates a positive aging experience, entailing the preservation of life quality and the reduction of health burdens associated with aging (Chen et al., 2022; M. Choi et al., 2017; Lin et al., 2020). However, none of the studies investigated the mediating role of depression in the relationship between SA and DA. This study aimed to investigate the mediation impact of depression between successful aging and DA in middle-aged and older people with hypertension in China.
As the population aging in China, SA is receiving increasing attention. SA is a multi-aspect concept, including the physical, cognitive, psychosocial, and spiritual aspects (Depp & Jeste, 2006; Ji et al., 2015; Phelan & Larson, 2002; Rowe & Kahn, 1997). Some scholars interpret it as a dynamic diversification process, decreasing incidence of disease and disability, high cognitive, the ability to participate in activities of social and productive, and meaning and purpose in life, it’s a crucial factor affecting the quality of life (M. Choi et al., 2017; Drevenhorn, 2018). In mid-range nursing theory (McCarthy & Bockweg, 2013), the construct of SA can be elucidated by examining two closely related concepts (adaptation and transcendence). SA is not a static state, but rather an ongoing process of adaptation and development in both psychosocial and physical domains to address challenges related to aging (Kusumastuti et al., 2016). SA is applied to middle-aged and elderly and has been widely studied, such as the China Health and Retirement Longitudinal Study (CHARLS; Lin et al., 2020; Nari et al., 2021). In China, the average prevalence of SA was 17.6% (Nakagawa et al., 2021). SA has been researched to be associated with a series of variables, such as age, sex, education, place of residence, economic status, social support, lifestyle habits, et al (M. Choi et al., 2017; Depp & Jeste, 2006; Ding et al., 2020; Gu et al., 2016; Kusumastuti et al., 2016; Lin et al., 2020; Sun-Suslow et al., 2020).
SA could be interpreted partly as proactive engagement and positive spirit (Tong et al., 2022), which are affected by the attitude toward aging and old age, moreover, that attitude is perceived as the influence factor of DA (Depaola et al., 2003). Studies have shown that there was a significant positive correlation between attitude toward aging and elderliness and DA (Depaola et al., 2003; Francalancia et al., 2021; Kahraman & Erkent, 2022), those with a higher negative attitude toward aging and old age had greater DA. The extant research has not yet better understood SA, including the way it can cover death and dying (Martin et al., 2015). According to the terror management theory (TMT; Cicirelli, 2002), DA is considered a fundamental fear that underlies the development and perpetuation of various forms of psychological distress (Lester, 2015), and can influence the quality of life and promotion behavior (Jaberi et al., 2022; Rashedi et al., 2020). Based on this theory, meaning and purpose in life were suggested to be integrated into DA management, extensive studies have indicated that meaning in life is significantly and negatively correlated with DA (Kahraman & Erkent, 2022; J. Zhang et al., 2019). But another article stated meaning in life served as a risk factor, rather than a protective factor for anxiety when people experienced boredom (Chao et al., 2020). In addition, scholars have stated that meaning and purpose in life is a connotation of SA (Kozar-Westman et al., 2013; Y. Yu, 2022), however, the two cannot be regarded as the same concept, the association between SA and DA has not been examined.
One variable related to DA is depression. Depression is characterized by persistent feelings of sadness, emptiness, or irritability (Battle, 2013), is the predominant psychological problem in middle-aged and older adults (Corrêa et al., 2020; Jin et al., 2019), and it’s on the rise (Charlson et al., 2019; X. Yu & Liu, 2021). Usually, the lack of interest in the usual activity is the first manifestation of depression among the aging population (Alexopoulos, 2005), which is universally viewed as a normal part of the aging process, causing it to be easily ignored (Segel-Karpas et al., 2017; Wilkinson et al., 2018). Depression affects their mental condition negatively and causes a low quality of life. Besides, chronic diseases cause feelings of worthlessness and anxiety, eventually resulting in depression (Crestani et al., 2019).
The literature is replete with evidence that SA serves as a buffer against Depression (Nari et al., 2021). In the context of the successful aging theory, older adults who get SA are less likely to have depressive symptoms if they are effectively using harmonious coping mechanisms including higher levels of personal control, creativity, and positive affectivity (Kozar-Westman et al., 2013). A study reported that depression was significantly negatively associated with all dimensions of SA (Lee et al., 2017). According to a subjective report on SA, self-rated depression emerged was most strongly associated with SA (Golja et al., 2020), and depression interfered with nearly all determinants of SA (Jeste et al., 2010). Based on the study of a longitudinal sample of older people aged 45 years and over in Korean adults, the results indicated that people who continuously failed to achieve or maintain SA status had a higher risk of depression (Nari et al., 2021). Several studies in China have also indicated a significant correlation between SA and depression (Sun et al., 2022; Y. Yu, 2022).
Depression as a mental health problem, is an important factor in DA (Gundogan & Arpaci, 2022). Existing studies indicated that individuals with depression showed a markedly higher risk of death anxiety compared to individuals without depression (Eggen et al., 2020; Erbesler & Demir, 2022; J. Zhang et al., 2019), stronger DA increases the risk of reduced quality of life and more likely bring depression. A study reported that depression was a positive significant predictor of DA during the COVID-19 pandemic (Gundogan & Arpaci, 2022). Another study among older adults reported that depression was positively related to anxiety about death (Woo & Bae, 2022), with different studies about chronic patients suggest DA was related to depression in both patients and caregivers (Eggen et al., 2020; Grabler et al., 2018). However, an article about multiple sclerosis sample indicated depression was significantly correlated with disability, but not with DA (Francalancia et al., 2021). Literature review reveals that a high proportion of patients in medical institutions are expected to suffer from physical and/or mental illness, stimulate thoughts about death, which is associated with high levels of DA (Abdel-Khalek, 2005; Missler et al., 2011; Soleimani et al., 2020). Therefore, the sample of this study was from hospitalized patients.
Given the above, Studies have reported a significantly positive correlation between attitude toward aging and elderliness and DA (Depaola et al., 2003; Kahraman & Erkent, 2022), however, the association between SA and DA has not been fully examined. Studies have reported a significant negative correlation between SA and depression (Nari et al., 2021; Sun et al., 2022; Y. Yu, 2022). Previous literature indicated a positive correlation between depression and DA (Eggen et al., 2020; Erbesler & Demir, 2022; Gundogan & Arpaci, 2022; J. Zhang et al., 2019). Research on the mediating role of depression between SA and DA was limited. Accordingly, we aimed to examine the mediation impact of depression between SA and DA among middle-aged and older people with hypertension in China.
We hypothesized that depression might act as a mediating role between SA and DA. The present study proposes a mediator model to analyze the relationships among SA, depression, and DA, focusing on the mediating role of depression, thereby, providing evidence for reducing DA among middle-aged and older people with hypertension. Alternative hypotheses are presented below, and the hypothesized mediator model is displayed in Figure 1.
H1: SA is statistically significantly associated with DA in middle-aged and older people with hypertension.
H2: SA is statistically significantly and negatively associated with depression in middle-aged and older people with hypertension.
H3: Depression is statistically significantly and positively associated with DA in middle-aged and older people with hypertension.
H4: Depression is a statistically significant mediator in the relationship between SA and DA in middle-aged and older people with hypertension.

The hypothesized structural equation modeling.
Methods
Participants
A total of 315 hypertension hospitalized patients were recruited by multi-stage sampling method and random number table method in the anonymized District of anonymized City, anonymized Province, from October 2021 to February 2022. Firstly, a third-class hospital of the Second Affiliated Hospital of the anonymized University School of Medicine was randomly selected. Secondly, dermatology, endocrinology, and traditional Chinese Medicine departments were selected from the hospital. Thirdly, hypertension patients were selected for questionnaire surveys at each survey point according to the inclusion criteria. The criteria for participant inclusion are as follows: (i) aged ≥ 45 years old; (ii) consent to participate; (iii) no cognitive impairment; and (iv) clear consciousness and barrier-free communication. We also excluded patients in case they were reluctant to answer study questions during data collection. Following the criteria proposed by Kendall, the sample size should be 10 to 20 fold of the number of items and expanded by 10% and over to ensure an adequate sample size. As the number of items in this study was 16 (seven in demographic characteristics, four in SAI, one in PHQ-9, and four in T-DAS), the calculated sample size was at least 176 (Malone et al., 2016). Finally, we enrolled 315 patients in our study. The data were gathered from the patients during their first week of hospital admission. The study distributed 315 questionnaires and received 298 valid responses, resulting in an effective response rate of 94.6%. Participant characteristics are described in Table 1. Participants are predominantly male (n = 190; 63.8%), aged 45 to 96 years (M = 64.0).
Frequency Distribution of Demographic Characteristics (N = 298).

Procedure
After the medical ethics committee of anonymized approved this research, the researchers contacted 17 investigators. To ensure that participants would be recruited in a standardized way, investigators received standardized training that covered research purposes, survey methods, communication skills, and scoring criteria. Finally, uniformly trained investigators conducted face-to-face interviews with the participants, with each interview lasting about 10 to 20 minutes. After a brief description of the research and informed consent, the participants provided written informed consent to investigators. The investigators asked the participants questions and then filled in the questionnaire on their behalf. The study was conducted in compliance with the principles of the Declaration of Helsinki. The collected data were kept confidential and used only for the purpose of this study. The study involving human participants was reviewed and approved by the Medical Ethical Board of anonymized (approval number 2021-3).
Measures
Demographics
A standardized questionnaire assessed participants’ sex, age, place of residence, cigarette smoking, alcohol habits, physical activity, and social activity. Age was categorized as 45 to 54, 55 to 64, 65 to 74, 75 to 84, and ≥85 years old. Sex was categorized as either male or female. The place of residence was classified as city, suburban, and countryside. Cigarette smoking included no smoking, ever smoking (smoking cessation for at least 1 year), and current smoking. Alcohol habits included no drinking, ever drinking (temperance for at least 1 year), and current drinking. Physical activity was divided into three groups: no physical activity, irregular physical activity, and regular physical activity (exercising at least 3 days/week and more than 30 minutes/day, including moderate to vigorous physical activity and walking). Social activity (including interacting with friends, providing help to friends/family/neighbors, doing voluntary or charity work, caring for a disabled or sick adult who does not pay you for the help and does not live with you, doing a social/sport/other types of club, going to the community club, playing cards/chess/mahjong, attending a training or educational course, taking part in a community-related organization, using the Internet, stock investment) was grouped as no social activity, irregular social activity, regular social activity (at least once a week).
Chronic Medical Illness Burden
The Cumulative Illness Rating Scale-Geriatrics (CIRS-G) is an organ-system-based rating scale that assesses the most severe condition presenting in each of 14 organ systems. It is a 14-item instrument, scored on a Likert-type scale ranging from 0 (no problem) to 4 (extremely severe), and total scores range from 0 to 56 (Miller et al., 1992). The CIRS-G Severity Index providing an estimation of the overall severity of dysfunction, is derived by dividing the total CIRS-G score by the number of organ systems recognized in CIRS-G. The CIRS-G has been translated into a Chinese version with high reliability and validity (Wang et al., 2020), and the Cronbach Alpha value was found to be .81 in this study.
Successful Aging
The Successful Aging Inventory (SAI) contains 16 items (Lee et al., 2017). Each item is succinct, positively phrased, and assessed using a Likert-type scale ranging from 1 (not at all) to 4 (very important). Respondents express their agreement with statements or the degree to which they perceive the applicability of the statement. There are four components: proactive engagement, positive spirit, wellness resources, and valued relationship (Tong et al., 2022). The SAI is scored from 16 to 64, with higher scores indicating more SA. We translated the SAI into the Chinese version (C-SAI) and assessed the validity and reliability of the C-SAI. Firstly, the SAI was translated into C-SAI by two English-Chinese bilingual professional translators. Then, another two translators translated the C-SAI back into English version. Secondly, a bilingual expert panel of two psychology experts and four gerontology experts assessed each item for cultural and linguistic equivalence. Thirdly, a preliminary field test was conducted on 30 older adults using C-SAI. The C-SAI was revised based on their feedback. The content validity index (CVI) of the C-SAI was 0.948, and the CVI of the items ranged from 0.833 to 1. A Kaiser–Meyer–Olkin (KMO) value of 0.923 and a Bartlett spherical test value of 2583.148 (df = 120, p < .001) in an exploratory factor analysis of C-SAI indicated that the factor analysis was suitable. The four-factors model explained 62.906% of the total variance. With confirmatory factor analysis (CFA), the fit indices were chi-square/degree of freedom (CMIN/df) = 3.42, root mean-square error of approximation (RMSEA) = 0.09, goodness of fit index (GFI) = 0.90, adjusted goodness of fit index (AGFI) = 0.82, incremental fit index (IFI) = 0.91, tucker lewis index (TLI) = 0.90, comparative fit index (CFI) = 0.91. The Cronbach Alpha value of the C-SAI was .909. The split-half reliability was 0.841 (Supplemental File 1).
Depression
The Patient Health Questionnaire-9 (PHQ-9), was designed based on the diagnostic criteria for depression from the Diagnostic and Statistical Manual of Mental Disorders, fourth Edition (DSM-IV; Kroenke et al., 2001). PHQ-9 is increasingly being used in research and clinical practice as a dependable and efficient self-report tool (Y. Yang et al., 2021). The questionnaire consists of 9 items, examples of the items are “feeling down, hopeless, or depressed,” and “having little interest or pleasure in doing things.” Each item is rated on a scale from 0 (not at all) to 3 (nearly every day). Scoring of the PHQ-9 ranges from 0 to 27, the higher scores indicate greater self-reported depressive symptoms (E. P. H. Choi et al., 2020). The PHQ-9 has been translated into a Chinese version with high reliability and validity, and the Cronbach Alpha value was found to be .76 (X. Yu et al., 2012).
Death Anxiety
The Templer’s Death Anxiety Scale (T-DAS), developed by Donald Templer in 1970 (Templer, 1970), has been widely utilized as one of the predominant questionnaires for assessing DA (Feng et al., 2021; Oker et al., 2021). It consists of 15 items, originally in a true/false format, and later developed into a 5-point Likert type, with each item scoring ranging from 1 (greatly disagree) to 5 (greatly agree; Royal & Elahi, 2011). The total scoring of the T-DAS ranges from 15 to 75, the scores for items 2, 3, 5, 6, 7, and 15 are reversed, and lower total scores represent lower levels of DA. There are four components: conscious about the passing of time, concern for somatic changes, fear of intellectual and emotional reactions caused by death, and concern for tension and pain accompanying death. A cross-cultural adaptation was completed in 2010, and the scale was translated into a Chinese version (C-TDAS) with high reliability and validity (H. Yang et al., 2016). The C-TDAS was used in our study. The Cronbach Alpha value was found to be .86 in this study.
Statistical Analysis
Data input and statistical analysis were conducted by SPSS Statistics (version 26.0). Descriptive statistics (frequency, percentage, means, and standard deviations) were performed to summarize the demographics of participants and scores on the questionnaires. One-way analysis of variance (ANOVA) and T-test were used to test differences of between-groups. Continuous variables (SA, PHQ-9, T-DAS) were calculated by Pearson correlation analysis. Regression was conducted to calculate whether SAI and PHQ-9 were significantly associated with T-DAS after input characteristics (sex, age, place of residence, cigarette smoking, alcohol habits, physical activity, and social activity). Then we used AMOS software to measure the mediation model. For the current study, the statistical significance level was set at p < .05 two-sided.
Results
Sample Characteristics and Descriptive Statistics
The frequency and rate of the characteristics were reported in Table 1. Participants were mostly aged 55 to 64 (30.2%) and 65 to 74 (36.6%), mostly living in the city (48.3%) and countryside (41.3%). Participants mostly had no cigarette smoking (53.7%) and no alcohol habits (56.0%), mostly had irregular physical activity (58.7%) and irregular social activity (59.7%).
Disease Status of the Patient
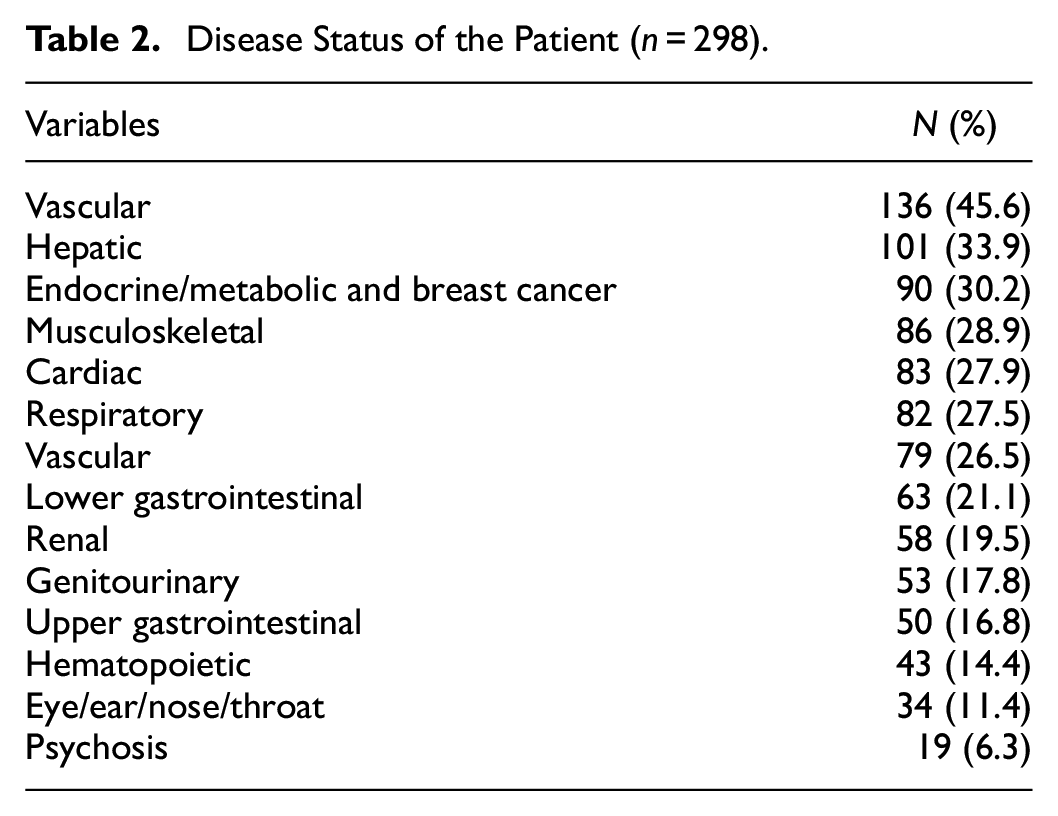
The scores for CIRS-G were 4.61 ± 3.12. As shown in Table 2, the five most prevalent disease types were vascular (45.6%), hepatic (33.9%), endocrine/metabolic and breast cancer (30.2%), musculoskeletal (28.9%), and cardiac (27.9%).
Disease Status of the Patient (n = 298).
Comparison in Different Social-Demographic Subgroups
In the present research, the mean SAI, T-DAS, and PHQ-9 scores of participants were 51.22 ± 7.63, 46.67 ± 9.03, and 7.16 ± 4.60 respectively.
Table 3 displayed the means and SD of the PHQ-9, SAI, and T-DAS with different variables. After analyzing data with independent t-test and ANOVA, the results showed that the mean PHQ-9 score differed by cigarette smoking (F = 3.761, p < .05), alcohol habits (F = 7.457, p < .01), and physical activity (F = 12.504, p < .001). The mean SAI score differed by age (F = 2.869, p < .05), and residence (F = 4.116, p < .05). Furthermore, the mean T-DAS score differed by physical activity (F = 3.856, p < .05).
Comparison of PHQ-9, SAI, and T-DAS in Different Social-Demographic Subgroups (N = 298).

Note. PHQ-9 = Patient Health Questionnaire-9; T-DAS = Templer-Death Anxiety Scale; SAI = Successful Age Inventory.
Preliminary Exploratory Bivariate Correlation Analyses
The correlation was assessed to bivariate associations between variables. The correlation matrix in Table 4 displays that there is a significantly negative correlation between PHQ-9 and SAI (r = −.199, p < .01), a significantly positive correlation between PHQ-9 and T-DAS (r = .277, p < .01), a significant positively correlation between SAI and the component (fear of emotional and intellectual reactions caused by death) of T-DAS (r = .177, p < .01), and a significant positively correlation between T-DAS and the component (positive spirit) of SAI (r = .130, p < .05).
Correlation Among the Study Variables (N = 298).

Note. PHQ-9 = Patient Health Questionnaire-9; T-DAS = Templer-Death Anxiety Scale; SAI = Successful Age Inventory.
p < .05. **p < .01.
Multiple Regression Analyses
Table 5 reported the detailed results of the multiple regression, the established model was statistically significant. The mediating role of PHQ-9 in the effect of SAI on T-DAS was significant. This was the case after inputting account demographics (sex, age, place of residence, cigarette smoking, alcohol habits, physical activity, and social activity).
Multiple Regressions of Hypothesized Relationships (N = 298).

Note. PHQ-9 = Patient Health Questionnaire-9; T-DAS = Templer-Death Anxiety Scale; SAI = Successful Age Inventory.
PHQ-9 was the dependent variable in the first regression model, demographics were entered into the first stage, then SAI was entered into the next stage, explaining an additional 3.3% (F = 6.320, R2 = .149, R2change = .033, p < .001) of the variance in PHQ-9 scores. The SAI significantly negatively predicted the PHQ-9 (β = −.183, p < .01, 95% CI [−0.176, −0.045]).
T-DAS was the dependent variable in the second regression model, and PHQ-9 was entered into behind SAI, explaining an additional 7.1% (F = 4.013, R2 = .111, R2 change = .071, p < .001) of the variance in T-DAS scores. The SAI significantly positively predicted the T-DAS (β = .142, p < .05, 95% CI = 0.034, 0.301), the PHQ-9 significantly positively predicted the T-DAS (β = .289, p < .001, 95% CI [0.335, 0.800]).
Mediation Analyses
AMOS 23.0 software was used to construct the structural equation model (SEM), SAI as the exogenous unobserved variable, PHQ-9 as the endogenous observed variable, T-DAS as the endogenous unobserved variable, examined the model by the method of maximum likelihood (see Figure 2). Then the model was modified once according to the modification indices (see Figure 3), and the results proved that the adjusted model had a good fit (see Table 6), χ2/df: 3.055, RMSEA: 0.083, GFI: 0.952, PGFI: 0.508, IFI: 0.961, CFI: 0.960, PCFI: 0.640, PNFI: 0.628.

The original mediation model.

The adjusted mediation model.
Measurement Model Fit Set (N = 298).

Note. χ2 = Chi-square; χ2/df = chi-square divided by degree of freedom ratio; RMSEA = root mean square error for approximation; GFI = goodness of fit index; PGFI = parsimony goodness of fit index; IFI = incremental fit index; CFI = comparative fit index; PCFI = parsimony comparative fit index; PNFI = parsimonious normed fit index.
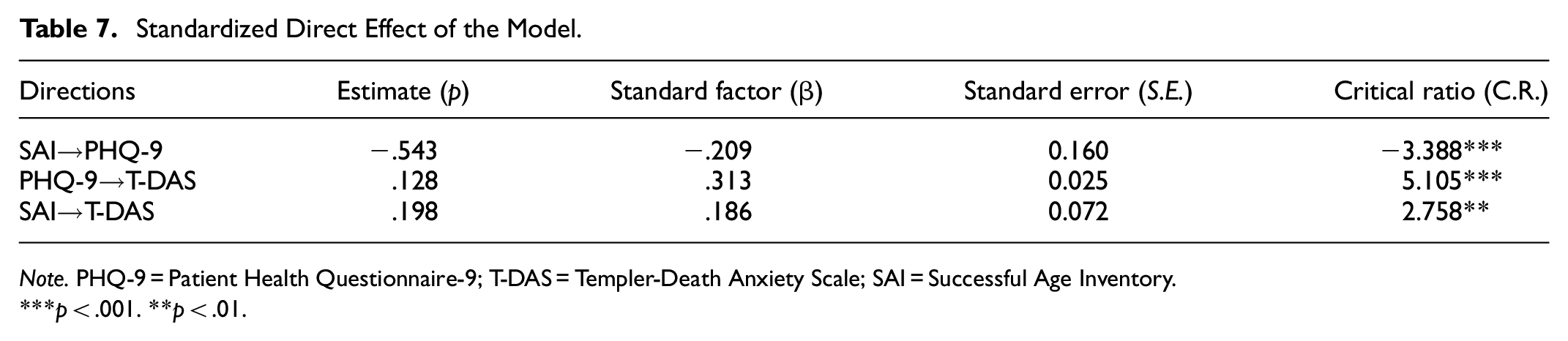
Table 7 reported the parameter estimate for the direct effects of the adjusted model, the direct effect of SAI on PHQ-9 was significant (β = −.209, p < .001), the direct effect of PHQ-9 on T-DAS was significant (β = .313, p < .001), the direct effect of SAI on T-DAS was significant (β = .186, p < .01). Combined with the results of the multiple regression results, it can be summarized that the mediating role of SAI in the effect of SAI on T-DAS was significant.
Standardized Direct Effect of the Model.
Note. PHQ-9 = Patient Health Questionnaire-9; T-DAS = Templer-Death Anxiety Scale; SAI = Successful Age Inventory.
p < .001. **p < .01.
Discussion
The present study examined whether depression mediated the relationship between SA and DA, and explored the relationships among SA, depression, and DA via a mediator model. The results indicated that SA and depression were all significantly correlated to DA, but the effects of these factors were different. Depression significantly mediated the association of SA and DA. Moreover, depression was correlated with DA positively and correlated with SA negatively. SA was correlated with DA positively.
Status Analyses of Death Anxiety
In the present study, the mean score (SD) of DA is 46.67 (9.03), this is consistent with a study about cardiovascular diseases in hospitalized patients 45.15 (8.44; Soleimani et al., 2020), but higher than the study using the original Templer’s Death Anxiety Scale instrument among elderly Chinese community people (3.54 out of 15; Wu et al., 2002), and also higher than other studies in the middle-aged and elderly people too (Barnett et al., 2018; Portal Moreno et al., 2008; Segel-Karpas & Bergman, 2022; van der Kaap-Deeder et al., 2020). This may relate to that hypertension poses great challenges to older living quality owing to the related cardiovascular diseases (Shen et al., 2022), the patients may have multiple chronic diseases as shown in Table 2. All these situations make those people feel a strong menace of death, and cause anxiety about dying and death (Hou et al., 2020), especially in inpatient. Other studies (Azaiza et al., 2010; Missler et al., 2011) reported that elderly people in care institutions would expect high proportions to suffer physical and/or mental poor health, and they would not have enough energy to deal with the changes in the process of the disease (Beydag, 2012). The anxiety of hospitalization and condition aggravation may increase the perception of death threaten, thus resulting in increased DA.
Moreover, the results also indicated that physical activity was an important protective factor in decreasing DA and depression in middle-aged and older people with hypertension. The results were consistent with previous literature (Fleg, 2012; Lin et al., 2020; Llobet Vila et al., 2020). A possible reason is that physical activity engenders beneficial effects on blood pressure, bone density, lipids, depression, and quality of life, thereby, acting as an indispensable protective factor for improving mental and physical health (Dong et al., 2023; Geneen et al., 2017; Wu et al., 2002) and preventing cardiovascular diseases (Owen et al., 2010). In addition, the mean of DA in females was higher than in males, but this difference was not statistically significant, which was different from previous studies that indicated the female gender was an important risk factor for DA, probably because the samples in these studies were different (Abdel-Khalek, 2005; Alkan et al., 2020; Wu et al., 2002). Females are better at expressing emotions and taking more responsibility in their families and society (Beydag, 2012; H. Yang et al., 2016). During the implementation of the Health Promotion Law (Hou et al., 2020), health management workers should pay more attention to mental health and the promotion of physical activity in middle-aged and old people. The national guideline for hypertension management in China (2019; Bureau of Disease Prevention and Control, 2020) provides health management service guidance, including exercise intervention and psychological counseling, etc., grassroots health workers and the general public should make efforts to improve the mental health level of hypertension individuals based on the guidance.
Analyses Correlation of Depression With Successful Aging and Death Anxiety
This study reveals that SA is negatively correlated with depression among middle-aged and older people with hypertension; higher scores on SA reflect lower depression ratings. This result is consistent with the previous studies. For instance, Nari also found SA to be negatively associated with depression among people aged 45 and older (Nari et al., 2021). A study using active aging (Galli et al., 2016), a concept analogous to SA, having the common characteristic of social activity participation, stated that the prevalence of depression was lower in the elderly with active aging after controlling for multiple confounders. Furthermore, another study stated that self-reported depression was associated with low subjective SA (Golja et al., 2020). Depression affects almost all determinants of SA (Jeste et al., 2010), such as diminished engagement in physical activity and unhealthy eating habits, greater social isolation, and more negative views of oneself and the future. Based on the context of the theory of SA (Kozar-Westman et al., 2013), an older individual with hypertension who is aging successfully is less likely to get depression if she or he is effectively using harmonious coping mechanisms (intrapsychic factors), such as higher level of positive affectivity, creativity, and personal manage. Yet, those who can’t meet the criteria for SA feel discouraged and hopeless (Nari et al., 2021), owing to the accumulation of multiple burdens, such as the functional decline of physical and psychological (Kozar-Westman et al., 2013), and limited social support, thus increasing susceptibility to depression. In other words, when individuals have higher level of SA, they can more effectively adapt to the changes in life and achieve self-acceptance, they can cope with mental issues through psychological adjustment (Davydov, 2014; Drevenhorn, 2018), thus reducing the risk of depression.
This study reveals that depression is positively correlated with DA among middle-aged and older people with hypertension; higher scores on depression reflect higher DA, consistent with prior studies. For instance, a study among Chinese elderly people stated that enhancing elderly people’s mental well-being and diminishing their feelings of depression could conversely help them to accept their death and mortality without excess apprehension (Wu et al., 2002). Therefore, depression displays an establishment of psychological instability and imbalance when older adults are exposed to a death fact or topic that occurs in their lives, the psychological instability and imbalance can aggravate the anxiety about death and dying, thus, these older adults diagnosed for depression score higher DA than the average population (Portal Moreno et al., 2008; Tang et al., 2021). In addition, depression is a significant public health concern and exerts a particularly large influence on health when comorbid with chronic disease. Hypertension is accompanied by a high incidence of depression, which may impede the treatment and reduce the hope for a good prognosis (Y. Zhang et al., 2018), the reduction of hope may increase the perception of death threaten and precipitate the development of DA (Soleimani et al., 2020). Accordingly, diminishing their feelings of depression can help them accept mortality and death without undue DA.
Mediating Role of Depression
This study reveals that SA significantly affects DA in the regression model and mediation model among middle-aged and older people with hypertension; a higher level of SA reflects higher DA, which seems to be at odds with most people’s notions. The positive spirit dimension of SA is positively correlated with DA in correlation analysis. Scholars pointed out that focusing on SA from the perspective of older individuals themselves was essential, and emphasized the importance of cultural differences (Kusumastuti et al., 2016).
According to the traditional Chinese view of family harmony and prosperity (Zhou et al., 2021), a successful state of aging signifies a meaningful older life (Y. Yu, 2022), which mainly derives from health and family members, Chinese older persons tend to consider love and positive fulfillment of family mission as the most important things in their daily life, which will bring them eudemonia and valued relationship (Gu et al., 2017; Tang et al., 2021). Moreover, death as the separation from earthly life is considered not only a personal event (Yin et al., 2022) but also the separation from the family and social mission, this separation causes fear of emotional reactions (Tang et al., 2021). Middle-aged and older people with higher SA appear to be more positively engaged in family missions, they regard having eudemonia and valued relationships as the criteria for SA, and can be reluctant to leave their meaningful life more; therefore, they resist death and death-related events, and experience higher death anxiety. On the other hand, influenced by the culture of filial piety, older parents or seniors usually hold a respected position in both the family and society; and long-lived people are revered and considered a symbol of SA (Gu et al., 2016), these perspectives and environments can help older adults well maintain the positive perception about their usefulness to others. For thousands of years, Confucianism has deeply influenced Chinese life-and-death outlook, and people generally fear annihilation, desire for a longer time left to live, reflect sadness about the passing of time, and show lower acceptance of death (Cicirelli, 2006). An empirical path analysis of a simplified model indicated that if death acceptance was high, DA was generally low (Surall & Steppacher, 2020). Therefore, for older adults, a greater positive perception about themselves as they age can bring out higher SA and exhibit lower death acceptance, aggravating their DA. SA patients have rich resources, positive spirits, and life meaning. When they are isolated from the original familiar rich life after hospitalization, they are easy to feel bored. Research shows that boredom is a risk factor for anxiety and stress, and patients are more prone to anxiety and death anxiety. Furthermore, individuals with higher SA possess positive aging experience and meaning in life, the change in life situation that comes with being hospitalized may lead to boredom, meaning in life serves as a risk factor for stress and anxiety when people experience boredom (Chao et al., 2020), and instead tends to cause greater DA (Oker et al., 2021).
The present study also reports that depression has a significant mediator role in the effect of SA and DA, an increase in SA will cause a decrease in depression, resulting in a decrease in DA. Based on terror management theory (TMT; Cicirelli, 2002, 2006; Greenblatt-Kimron et al., 2021), the pursuit of survival and continued existence are instinctive of all persons but also know mortality is inevitable for all humans. Therefore, middle-aged and older hypertension patients with SA state have the potential to consciously experience DA. Effective psychological measures that aim to enhance patients’ mental well-being and diminish their feelings of depression may in turn help them to accept their mortality and death without undue DA. Health professionals may primarily focus on therapeutic regimen and supportive symptom management, patients may have agonizing DA and depression (Grabler et al., 2018; Soleimani et al., 2016), it is essential to maintain a holistic appraisal of the individual as a bio-psycho-social-spiritual being, alleviate existential concerns in hypertension patients, and palliate mental health distress.
Implications and Limitations
This study is the first to explore the mechanism of SA on DA, clarifies the relationship between SA, depression, and DA, and contributes to the literature by exposing the mediating role of depression in the association between SA and DA in middle-aged and older people with hypertension, and provides theoretical bases and orientations for ameliorating DA. Given that higher SA and depression have been identified as major risk factors for DA among middle-aged and older people with hypertension, we emphasize the clinical importance of providing psychological intervention, emotional guidance, and death education for these people based on improving the level of SA, which should be taken on board by health care professionals. Therefore, it should be Combined with the “Healthy China Initiative (2019−2030)” to develop a multidimensional and systematic program for mental health management for effective intervention with middle-aged and older people with hypertension exposed to depression and DA.
The present study also presents certain limitations. Firstly, this study is limited by the cross-sectional design, the causality between SA, depression, and DA cannot be inferred. Future studies should be designed as a longitudinal study, allowing data to be collected at different time intervals. Secondly, it was conducted in internal medicine inpatients with hypertension in Hangzhou city, which was not representative. These findings may not fully apply to patients in other regions. In future studies, a random sampling method is recommended to recruit larger samples, which includes participants from different groups (living in the community, inpatients, elderly people, etc.). Finally, some other known factors, such as social support, self-esteem, etc. can be introduced to further explore the influencing mechanism of DA and provide a new basis for the development of measures to reduce DA in the future.
Conclusion
Depression plays a mediating role in the association between SA and DA. The available information on middle-aged and older patients with hypertension, especially those with psychological abnormalities, should be thoroughly explored, objecting to find earlier the high-risk psychological abnormalities population, undergoing a psychological intervention to reduce higher levels of DA, and providing criteria for health promotion.
Footnotes
Acknowledgements
We appreciate the contributions of all participants and the cooperation of the research members.
Abbreviation
SA = successful aging; SAI = successful aging inventory; PHQ-9 = patient health questionnaire-9; DA = death anxiety; T-DAS = Templer’s death anxiety scale; C-TDAS = the Chinese version; SEM = structural equation model; TMT = terror management theory; WHO = World Health Organization; B = unstandardized; CI = confidence interval; SD = standard deviation; SE = standard error; R2 = R squared; R2 change = R squared change; ANOVA = analysis of variance; χ2 = Chi-square; χ2/df = Chi-square divided by degree of freedom ratio; IFI = incremental fit index; CFI = comparative fit index; GFI = goodness of fit index; PGFI = parsimony goodness of fit index; PNFI = parsimonious normed fit index; PCFI = parsimony comparative fit index; RMSEA = root mean square error for approximation.
Author Contributions
Conceived and designed the research: LZ. Analyzed the data: X-p L and LZ. Wrote the paper: X-p L. The final manuscript was reviewed and approved by all authors.
Ethics Approval and Consent to Participate
Approval for this study was given by the medical ethics committee of anonymized (approval number 2021-3), All participants provided informed consent. All methods were performed in accordance with the Declaration of Helsinki.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Anhui Provincial Education Department Foundation, PR China (2021jyxm1610); Wannan Medical College Foundation for Teaching Research Project, PR China (2020jyxm27); and the Scientific Research Fund for Young and Middle-aged from the Wannan Medical College (WKS202003).
Data Availability Statement
The datasets used and/or analyzed during this study are not publicly available to preserve anonymity of the respondents but are available from the corresponding author on reasonable request.