
Abstract
Background and significance
Social Determinants of Health (SDOH) encompass a multitude of non-clinical factors influencing health, such as financial status, nutritional status, education level, and social support. They are defined as “the conditions in which people are born, grow, live, work and age” by the World Health Organization (WHO). 1 These social determinants are often distributed inequitably across the population, leading to inequitable health outcomes known as health disparities.2,3 These factors have significant implications for both short- and long-term health outcomes.
For example, 10.5% of families in the United States experience food insecurity, which has been shown to predispose patients to obesity, cardiovascular disease, diabetes, and childhood developmental disorders, among other chronic conditions.4,5 Additionally, financial resource strain or poverty may predispose children to develop developmental delays, mental illness, chronic disease, and poverty in adulthood.6,7 In order to determine if these social risk factors affect their patients, health care providers (HCPs) can employ questionnaires and/or advanced history taking during clinical encounters. 8 Knowledge of specific risk factors such as a patient not being able to afford a prescription or trouble getting to multiple office visits may help HCP’s tailor care plans specific to their patient needs. Aside from patient care, SDOH also have ramifications for billing and reimbursement—the collection of SDOH through medical records has been used to reflect care complexity in billing and has been incentivized to better connect at-risk populations with appropriate resources.9,10 The timely and accurate collection of SDOH using validated questionnaires, however, poses a challenge. Questionnaires can be time-consuming, may frustrate both patients and HCPs, and can disrupt the flow of clinic.11–13 Furthermore, patients may choose to withhold information out of embarrassment, lack of understanding of how information recorded in SDOH screening will be used, mistrust of healthcare, or fear of legal consequences, among other reasons. 14 Patients may also be unable to recall aspects of their past social history or be unable to understand the questionnaires due to low health literacy, educational level, or neurodivergence. 14 To circumvent these issues, SDOH screening tools must be easy to administer, provide minimal discomfort to the patient, and exhibit high sensitivity with reasonable specificity to efficiently detect risk while capturing a high percentage of at-risk individuals.12,13
To help with the identification and screening of patients with social risk factors, certain electronic medical records (EMRs) have created tools within the patient chart to document these attributes. For example, Epic® has created a SDOH “wheel” that helps clinicians collect information on transportation needs, social connections, financial resource strain, housing stability, and food insecurity, among other factors. 15 Through this “wheel,” Epic creates a snapshot of each patient’s social risk factors by risk stratifying each patient based on answers to a series of questions in each SDOH domain. Because the EMRs can be integrated across multiple geographic healthcare systems, they can play a pivotal role in advancing the medical field in the collection of SDOH for point of care utilization and potentially for reimbursement.
Objective
Although EMRs are employing tools to identify social risk factors, it is unclear how these tools, such as the Epic SDOH “wheel” questions, were developed, and there is no evidence that they were validated. A previous study identified Epic’s poor sensitivity and specificity in the domains of financial strain, transportation, food insecurity, and housing instability in a small safety-net population. 16 Our study, however, sought to build upon these results in a larger sample at an urban-tertiary care center, the University of Chicago Medical Center. We compared the Epic SDOH “wheel” domains of transportation security and financial toxicity to the domains of transportation security and financial toxicity from previously validated questionnaires to determine the accuracy of the “wheel” in risk stratifying patients in these two specific domains of SDOH.
Materials and methods
Study design, setting, and participants
This was a cross-sectional study that was approved by our Institutional Review Board (IRB23-0306). The inclusion criteria were English-speaking patients aged 18 years or older who presented to a single, urban, tertiary academic level 1 center, the University of Chicago Medical Center, and were seen in orthopaedic hand surgery or foot and ankle surgery between June 12, 2023 and October 31, 2023. All eligible patients were approached in-person, and those who agreed to participate were consented and provided with questionnaires on an iPad. We have previously shown high completion rates with our PROs collected on iPads in our patient population. 17 Patients were asked to completed both the Epic SDOH domain questions of transportation needs and financial resources strain as well as a set of validated questionnaires for these domains. There was no incentive for participation in the study. There was no survey logic to ensure all questions were answered in order to maintain the voluntary aspect of participation, so participants were allowed to leave survey questions blank and were excluded from the subsequent analysis. To determine the rate of enrollment, we recorded the number of patients approached and the number who declined to participate from July 11, 2023 onwards.
Variables and demographics
We chose two validated questionnaires matching the Epic “wheel” domains: the COmprehensive Score for financial Toxicity (COST) questionnaire and the Transportation Security Index (TSI) questionnaire. These validated questionnaires (2) plus the Epic equivalents composed the four total questionnaires completed by all participants.
Other domains in the Epic “wheel” that were not assessed in this study include food insecurity, alcohol use, physical activity, intimate partner violence, depression, tobacco use, housing stability, utilities, stress, and social connections. While the above domains are all important to patient care, we decided to select two domains to avoid excessive survey burden on clinic patients and so surveys could be completed in a timely fashion. We started with transportation security and financial toxicity given the availability of validated questionnaires (namely, the TSI and the COST) corresponding to these SDOH and the relevance of these SDOH to medical and surgical care.18,19 Furthermore, given Epic’s food insecurity questions are the same as the validated two-question food insecurity survey, we did not include food insecurity in this manuscript despite it being among the most common health-related social needs. 20
Financial toxicity was measured by the COmprehensive Score for financial Toxicity (COST), a 12-question validated questionnaire. A lower score on COST indicates a higher level of financial toxicity.19,21 To determine specificity and sensitivity, COST was dichotomized with a score of below 17.5 indicating high toxicity and a score above 17.5 indicating low toxicity in accordance with previous studies. 22 We chose the COST survey as it was most prominently-utilized validated measurement of financial toxicity that included measures of impact on patient medical expenses, rendering it the gold standard.23,24 Other questionnaires such as the recently-developed Economic Strain and Resilience in Cancer (ENRICh) measure, utilized the COST survey in their validation.25,26
The Epic SDOH wheel financial toxicity risk assessment consisted of a one-question, five-item Likert scale. Based on the answer to this one question, Epic labeled patients as “Low Risk,” “Medium Risk,” and “High Risk” for financial toxicity. For comparison purposes, we group the medium and high risk patients together into an “at-risk” group. These questionnaires can be found in the Supplementary Materials as “Material A” and “Material B”. 15
Transportation security was determined by the Transportation Security Index (TSI), which is comprised of an 11-question set and 16-question set that are scored numerically, while the Epic SDOH wheel transportation security questionnaire consisted of two dichotomous questions.27–29 A lower score on the TSI indicates a higher level of transportation security. 30 We chose TSI because it is the most prominently-used transportation security measure on a national level across multiple fields. 18 Murphy et al. (2022) and Vallas et al. (2022) used the TSI to create national economic models of transportation insecurity in Americans facing poverty and disability, respectively.28,31
Epic describes patients as transportation insecure if a patient answered “yes” on either Epic SDOH transportation security question. 15 Numerical TSI scores were dichotomized, with a score below 10.5 indicating low insecurity and a score above 10.5 indicating high insecurity. 30 These questionnaires can be found in the Supplementary Materials as “Material C” and “Material D”. 15
Between June 12, 2023 and October 31, 2023, a total of 229 patients agreed to participate in the study. Of the 229 patients who participated in the study, 203 participants fully completed both the COST and EPIC financial toxicity survey and 199 participants fully completed both the TSI and EPIC transportation needs survey. Participation rates were not recorded until July 11, 2023. From that date onwards, 302 patients were approached to participate in the study, 172 were consented into the study, and 130 declined to participate or withdrew after signing consent, yielding a participation rate of 57.0% (n = 172/302). While the participation rate over the first month of the study is unknown, the data from that time was still included in the results. To encourage participation, the surveys were anonymous, and no protected health information was collected on patients.
Statistical analysis – Tools & methodology
Statistical analyses were completed using the RStudio program. Patients with missing values in any survey were excluded from the sub-analysis of the respective survey. The level of significance for all tests was set at p < 0.05 and all p-values were reported unadjusted and interpreted descriptively unless otherwise stated.
Tests were used to compare the Epic SDOH risks with the validated risks in both domains. Shapiro-wilk tests for normality were completed on each category of data to determine whether data was parametric and inform subsequent statistical testing. Non-parametric Fisher’s Exact Tests were utilized to compare the Epic financial toxicity risk with the COST-defined financial toxicity risk categories and the Epic transportation insecurity risk with the TSI-defined transportation insecurity risk categories. We then calculated the sensitivity and specificity of each Epic domain. True positives and true negatives were defined when both the EPIC questionnaire and the validated questionnaire were in both positive or negative. False positives were noted when the EPIC questionnaires had a positive screen when the validated questionnaire was negative. False Negatives were noted when EPIC questionnaires had a negative screen when the validated questionnaire was positive.
Results
Number of patients with financial toxicity according to Epic questionnaire and COST survey.
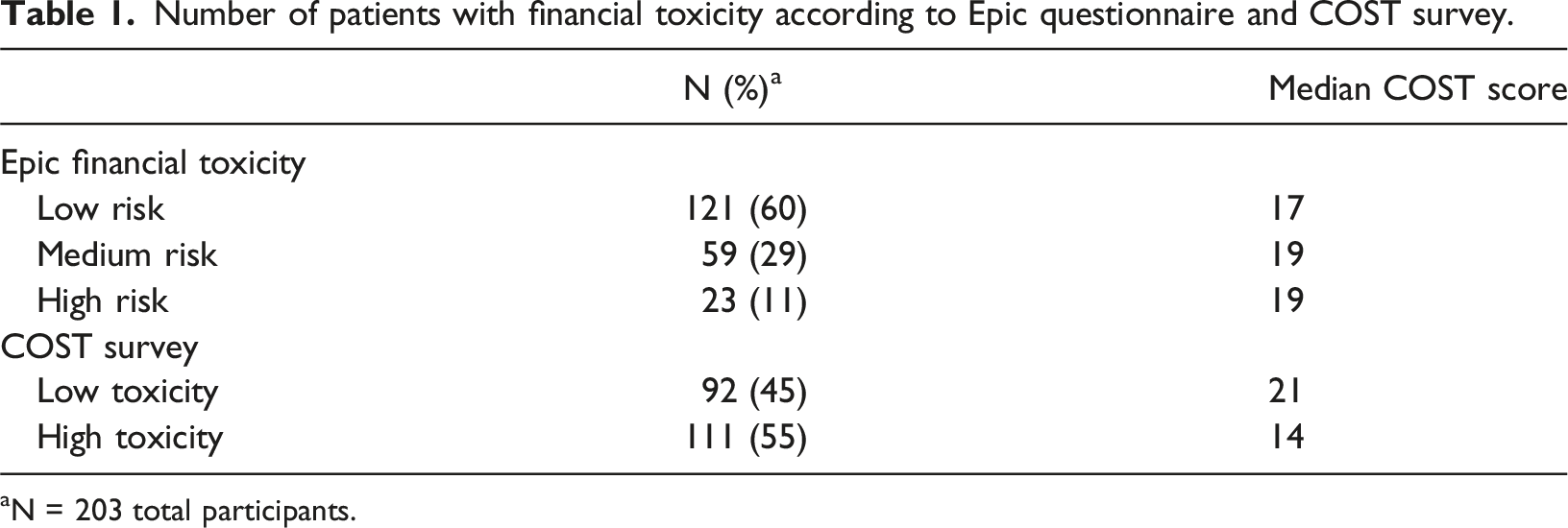
aN = 203 total participants.

Epic financial toxicity risk totals compared with COST financial impact category totals.
Number of patients with transportation insecurity according to Epic questionnaire and TSI survey.

aN = 199 total participants.
Sensitivity and specificity of Epic Financial Resource Strain and Transportation Needs surveys.

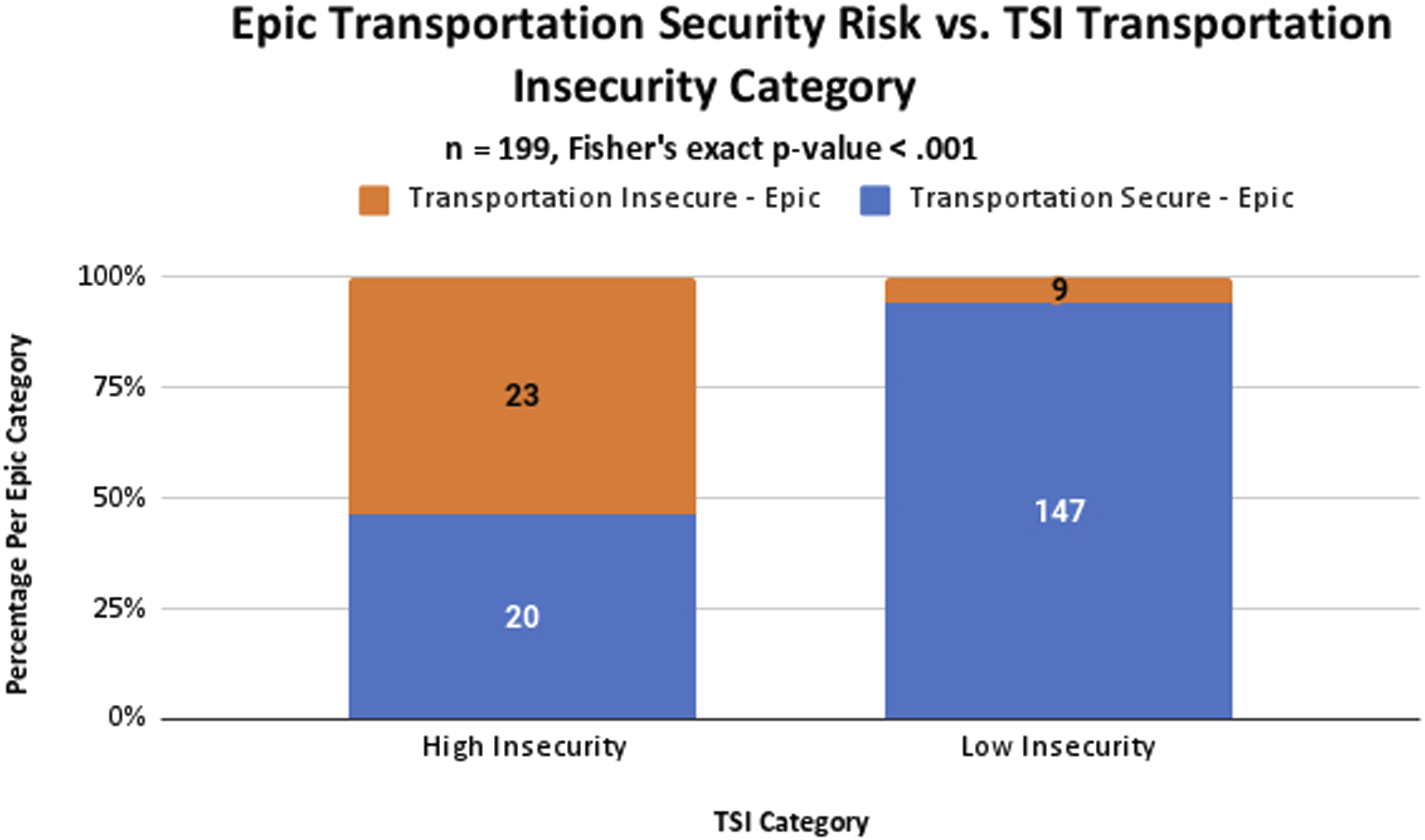
Epic Transportation Security Survey totals by TSI survey category.
Discussion
The purpose of this study was to assess the performance of Epic’s SDOH wheel as a screening tool when compared to validated surveys in two specific domains. SDOH are important contributors to clinical outcomes, and an understanding of each patient’s social risk factors is critical to providing patient-centered care.18,32 We found that the Epic SDOH wheel demonstrated low sensitivity and specificity in the domain of financial toxicity and low sensitivity and high specificity in the domain of transportation security. The understanding of patients’ risk in these domains may be relevant to effectively identify barriers to successful treatment and recovery. 32
The importance and the benefits of SDOH screening tools in EHR have been clearly established by previous authors. Berkowitz et al. noted that their screening process in their clinics was feasible and important to staff and patients alike. 33 Rogers et al. utilized EPIC to screen patients utilizing the SDOH wheel and then refer high-risk patients to appropriate community resources within EPIC. 15 When patients tested positive for deficiency in one or more SDOH, they were presented with a list of community resources tailored to their respective deficient SDOH(s) and the list was also added to their medical record for future communication about the list between providers and patients as well as for social workers to connect the patients with their resources. 15 While utilizing the EMR in this manner is a step forward in automating and providing appropriate resources for our patients, we must ensure the validity of the data we are collecting.
Other than the current study, two additional studies have found that the EPIC SDOH wheel does not perform well in certain domains when compared to existing questionnaires. Our study’s findings were most similar to a study by Vest, Wu, and Mendoca (2021), who also investigated screening tools for social risk factors. 16 This study found that the Epic financial resource strain and transportation needs screening tools had low sensitivity (28.0% and 50.0%, respectively) and high specificity (93.8% and 90.7%, respectively) 16 ; our findings regarding the sensitivity and specificity of the transportation needs questionnaires were similar, despite utilizing a different validated transportation security survey. Regarding the financial resource strain questionnaire, we similarly found low sensitivity—however, we found the Epic tool also had poor specificity at 53%. Harle et al. (2023) also investigated Epic SDOH but instead evaluated the food security, housing instability, and financial resource strain modalities. They also similarly found low sensitivity (27.1%) for financial resource strain despite finding high specificity (98.1%). 34 Our study expands on the Vest et al. (2021) results with a larger patient sample and different patient population; Vest et al. (2021) sampled patients from a safety-net provider, while we recruited patients from an urban tertiary care orthopaedic surgery office. Additionally, while Vest et al. (2021) and Harle et al. (2023) utilized email for some of their data collection, all our survey data was collected in person as to avoid ehealth literacy and technological barriers as potential confounding factors. Despite these differences, all three studies found the Epic tools to have low sensitivities in the domain of financial toxicity, and our study along with Vest et al. additionally found low sensitivities in transportation security. If utilized as a screening tool in a clinical setting, the Epic tool would not appropriately identify many at-risk patients with high financial toxicity and transportation insecurity.
Current literature on financial toxicity underscores its considerable impact on patient outcomes including worse psychological and physical outcomes, and increased mortality.35,36 Notably, patients at high risk of financial toxicity are also less likely to fill their medications, undergo recommended testing, and attend medical appointments.35,37 Financial toxicity has become an increasingly important consideration in treatment planning, as direct costs associated with novel medications and surgeries are frequently more than patients are able to pay out-of-pocket.36,38 As a result, there remains a need for practical tools to screen patients for financial toxicity risk—without effective screening, patients may not be provided the resources and support required to help complete necessary treatments that may otherwise be unaffordable. Past studies have also implemented various screening tools but largely have not directly compared such tools to validated assessments of financial toxicity37,39; future research must therefore identify a more effective screening tool to allow for practical, quick, and sensitive assessment of risk.
Transportation insecurity is closely tied to financial toxicity, with high rates of transportation insecurity among patients living below the poverty line. 18 Recent literature on transportation insecurity also relates high levels of insecurity to delays in seeking care, poor treatment adherence, and higher mortality, as well as worse psychological outcomes and quality of life.18,40 Unfortunately, practical and brief screening measures for transportation insecurity are currently unstandardized or poorly studied, and our current investigation revealed a sensitivity of just 53% for Epic’s transportation insecurity screening tool.40,41 While the tool performed well in identifying those not at risk, further research will be vital to developing appropriate screening modalities to more fully capture patients suffering from transportation insecurity. High-risk patients may be eligible for valuable resources, such as hospital-based transportation services, transportation-assistance programs, flexible follow-up options, and telemedicine-based care.40,42
Ultimately, SDOH such as transportation security and financial toxicity are closely interrelated with financial constraints potentially affecting ability to obtain transportation. Therefore, a comprehensive understanding of these patient risk factors is required for healthcare providers to meaningfully engage patients in shared decision-making and avoid preventable hardship for patients. 43 EHRs can easily fill this void through documenting different social risk factors a patient may have that is accessible to all treating physicians. EHRs can automate the referral pathways and alert HCPs to individuals with social risk factors similar to Rogers et al. 15 First, however, accurate screening tools must be developed with the EHRs.
Notably, minimum cutoffs for sensitivity and specificity for screening tools are not well-established, and these measures may vary across clinical settings. In theory, an ideal screening test would exhibit a sensitivity and specificity of 100%, capturing all at-risk patients while omitting those not at risk 44 ; while this is generally unachievable in real-world settings, many routinely-administered clinical screening tools, such as colonoscopy (up to 95% sensitivity, 85% specificity in detecting adenomas >10 mm), mammography (roughly 80% sensitivity, 90% specificity in detecting breast cancer), and the Patient Health Questionnaire-9 (88% sensitivity, 88% specificity in detecting Major Depressive Disorder), exhibit both high sensitivity and specificity.45–47 However, sensitivity is often optimized at the expense of specificity in settings where the benefits of capturing high-risk individuals greatly outweigh the risks associated with false positives, as is the case with the identification of SDOH.44,48 It is thus reasonable for screening tools for other SDOH to similarly prioritize achieving a sensitivity of over 90% while maintaining a practical specificity of at least 70%–80%. Other conventional medical resources also state that a combined specificity and sensitivity of 150% is an acceptable benchmark.49,50 The Epic SDOH wheel surveys, however, did not consistently exhibit such performance in our study or in prior research.16,34
There are numerous reasons that may explain the inherent discrepancy of the Epic SDOH wheel and the validated questionnaires.15,32,51 The Epic screening tools we used, Epic Financial Toxicity (1 question) and Transportation Security survey (2 questions)), were brief in comparison to the COST survey (12 questions) and the TSI survey (27 questions). The longer lengths of the validated questionnaires may allow them to address additional concerns and detect smaller differences, but they may also make them less practical in a clinic setting. While screening tools should be brief, they must balance brevity with accuracy and high sensitivity as to allow for further screening if necessary.
Another key difference between the validated and Epic surveys is that the Epic surveys only ask about the current difficulty patients have in meeting their needs, focusing on immediate social needs. The COST and TSI surveys ask patients about their current situations, past and future exposure to SDOH risk, and their families’ attitudes toward their SDOH situations. The COST and TSI are, therefore, more comprehensive in evaluating patient social risk factors than the Epic SDOH model.24,30
At a larger scale, these findings provide significant context for discussing how information captured in EHRs can be used by HCPs to address health disparities. If data is collected systematically and regularly used as part of a holistic approach to patient care, patients may be helped to connect to social resources in the local community. This approach would also allow healthcare institutions to document the number of high-risk patients in the system, which is becoming increasingly vital as reimbursements become tied to outcome measures. Unfortunately, recent studies have shown that even when HCPs attempt to collect SDOH data, there is often a lack of uniformity and consistency in their approaches, limiting the generalizability and validity of their data collection.52,53 While EHR-integrated screening tools offer a scalable approach to SDoH data collection, their clinical utility depends on data accuracy, interoperability, and integration with decision-support tools. Therefore, prioritization should be made to consider adopting validated screening tools from resources that have produced evidence-based literature using those tools, such as University of California at San Francisco Social Interventions Research and Evaluation (SIREN) database.54,55
Future innovative decision support tools such as machine learning, standardized data frameworks, computer-adaptive questionnaires and artificial intelligence (AI) may be embedded in EHRs to help physicians quickly assess SDOH and potential impacts on care.56,57 Even without these tools, health systems in Denver and Houston are utilizing SDOH tools embedded in their EHRs to better understand how social risk factors affect outcomes on a larger scale, affect policy change, and eventually address health disparities head on.51,58
Our study is not without limitations. iPad use as well as time constraints after finishing a clinic visit were reported barriers to survey completion; these factors may have contributed to lower engagement with survey materials. Despite this, the research coordinator was available to help patients fill out the questionnaires. Additionally, some patients declined participation because they had transportation scheduled with a local patient transportation company, and this may have artificially decreased the number of patients with poor transportation security. Furthermore, we only included patients that appeared in our orthopaedic surgery clinic. This did not include patients without health insurance and includes only patients that were able to make to obtain transportation their clinic appointments. Of note, we also dichotomized the Epic Financial Toxicity scale into high/medium and low risk, which may limit direct comparison with the dichotomized Epic SDOH wheel survey. Epic has additional questions regarding other domains of SDOH, including food insecurity, alcohol use, physical activity, intimate partner violence, depression, tobacco use, housing stability, utilities, stress, and social connections. We did not examine these different domains, and as with the surveys we used, there is no evidence that Epic has validated or tested these domains. Future studies should compare these questionnaires with their validated counterparts and include methods to account for entire hospital systems including patients who do not present to their appointments physically.
Conclusion
Overall, the Epic SDOH wheel demonstrated low sensitivity and specificity in the domain of financial toxicity and low sensitivity and high specificity in the domain of transportation security, suggesting limitations in its ability to serve as an effective screening tool. Our results thus demonstrate that the Epic SDOH wheel requires further evidence-based refinement to more accurately reflect patient risk factors, and future investigations must investigate the other domains of SDOH within Epic to further assess the sensitivity and specificity of the tool, as well as exploring ways to incorporate validated questionnaires into the Epic EHR. EHRs should be transparent on how their screening tools are created or acquire screening tools from validated sources, helping HCPs understand the validity of the screening tools that are being utilized to make treatment decisions. Future efforts should also focus on improving EHR-based SDOH screening through AI-driven risk stratification, standardized data frameworks, and automated clinical decision support systems to address SDOH at scale.
Supplemental Material
Supplemental material - Performance of an EMR screening tool for social determinants of health
Supplemental material for Performance of an EMR screening tool for social determinants of health by Malik Scott, Sarthak Aggarwal, Michael Koch, Jason Strelzow, Kelly Hynes, Jeffrey G. Stepan in Health Informatics Journal
Footnotes
Ethical considerations
This study was conducted according to US and international standards of Good Clinical Practice, applicable government regulations and institutional research policies and procedures.
This protocol and any amendments were submitted to the Institutional Review Board (IRB), in agreement with local legal prescriptions, for formal approval of the study conduct. The decision of the IRB concerning the approval of the study was made in writing to the investigator.
Consent to participate
All subjects for this study were provided a consent form describing this study and providing sufficient information for subjects to make an informed decision about their participation in this study. This consent form was submitted with the protocol for review and approval by the IRB for the study. The formal consent of all subjects, using the IRB-approved consent form, was obtained before chart review. The consent form was be signed by all subjects or (if applicable) legally acceptable surrogate, and the investigator-designated research professional obtained the consent. The original consent document was stored in the research files. A copy of the signed consent was provided to each subject.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article cannot be shared publicly due to the privacy protection requirements of patient healthcare data.
Supplemental Material
Supplementary material is available at Journal of the American Medical Informatics Association online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.