
Abstract
The interoperable exchange of social-behavioral determinants of health data is challenging due to complex factors including multiple recommendations, multiple tools with varying domains, scoring, and cutpoints, and lack of terminology code sets for storing assessments and findings. This article describes a strategy that permits scoring by social-behavioral determinants of health domain to create interoperability and equivalency across tools, settings, and populations. The three-tier scoring strategy converts social-behavioral determinants of health data to (1) be used immediately at point of care by identifying social needs or social risk factors, (2) be consumed within analytics and algorithms and for secondary analysis, and (3) produce total scores that reflect social determinant burden and behavioral determinant burden across populations and settings within a healthcare system. The strategy supports the six uses recommended by the National Academy of Medicine, provides flexibility in choice of social-behavioral determinants of health tool, and leverages the power of social-behavioral determinants of health data in healthcare delivery.
Keywords
Background
Social determinants, the circumstances in which people live and work, have a strong effect on health and are linked with the development of chronic conditions and their management.1,2 Many factors, including genetics, lifestyle behaviors, environment, healthcare, and social determinants, influence population health. 3 According to Garg and Dworkin, 4 social and environmental factors likely have twice the impact on the overall health of an individual compared to quality health care. Deficits in education, housing, transportation, and income influence health behaviors, such as nutritional habits and physical exercise patterns, and are interwoven in the web of causation for disease. 5 The Institute of Medicine (IOM), 6 now National Academy of Medicine, calls for clinicians to focus on these factors within their care delivery processes. Reimbursement policies that incentivize population health management and value-based purchasing encourage attention to modifiable determinants of health. 7
Adler and Stead 7 describe six uses of social-behavioral determinants of health (SBDH) delineated by the IOM which include the following: diagnosis and treatment, care coordination, risk assessment and stratification, appropriate referrals, patient experience, and research. 1 Uniform use of electronic health records (EHRs) that incorporate SBDH domains could influence population health measurement, population health management, patient care delivery, and secondary uses of SBDH data in health-related research, performance improvement initiatives, population segmentation, and risk identification algorithms.
Complexities to assess, capture, exchange, and use SBDH data
A proliferation of publications with recommendations for the assessment of SBDH, both voluntary and mandated, have arisen since 2014 including the IOM phase I and II reports, Meaningful Use 3, Healthy People 2020, Medicare Social Risk, CMS Accountable Health Communities, and National Quality Forum.1,2,8–12 The wide range of recommendations and use cases include varying and inconsistent SBDH domains. In addition, the cacophony of recommendations for the use of SBDH has led to a lack of holistic vision and contributed significantly to confusion for healthcare systems, providers, and EHR suppliers.
Variation in SBDH assessment
In addition to a lack of holistic vision, there is variation in SBDH assessment. Assessment instruments vary by population and discipline with as many as 8 adult SBDH tools/instruments and 16 pediatric instruments.13,14 SBDH assessment tools/instruments vary by researchers’ training, which influences their approach to the design of instrument items and the number of items developed to measure a construct. 15 The importance, or weight, of SBDH varies according to outcome (health status, missed work/school days, mortality, encounters, and costs) and disease. There is little established reliability and validity for tools in the public domain, with only one adult SBDH instrument with established reliability. 16 In addition, scoring scales and cutpoints are dissimilar or non-existent across tools. These differences introduce variability to the assessment and measurement of SBDH domains and decrease the precision of SBDH measurement across populations.
Standardizing SBDH data collected by different instruments
The measurement of SBDH is particularly important in vulnerable populations, which include women, children, elders, minority races or ethnicities, lower socioeconomic status, immigrants, gay men or lesbians, and the homeless. 17 Stewart and Napoles-Springer 18 suggest that measurement of phenomena in diverse populations requires comparable measures to ensure that data can be used for multiple uses (e.g. comparative effectiveness studies, reimbursement policies, and practice guideline development). Therefore, consistency of measurement will increase precision and reduce bias in the interpretation of assessment results across populations and settings.
Methods
This article describes a strategy that permits scoring SBDH tools by domain to create equivalency across instruments, settings, and populations, which in turn supports interoperability of EHR data, regardless of the SBDH tool used, with the goal of promoting the use of standardly measured SBDH data as described by Adler and Stead. 7 To create this strategy, a critical appraisal of the scientific literature for evidence-based strategies to achieve equivalency between SBDH instruments was completed. Psychometric and EHR methods to achieve equivalence between SBDH instruments/tools were reviewed and applied to the PRAPARE (Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences) tool and IOM instrument.16,19
Psychometric methods to achieve equivalence
From a psychometric perspective, to simultaneously analyze data from multiple sources, measures must be available from each source which represent the same construct, the construct must represent the same theoretical meaning, and the scores for the construct must be scaled similarly. 20 To achieve the six uses of SBDH data, as suggested by Adler and Stead, 7 equivalency across instrument domains is essential so that a common meaning is represented. Standardization, normalization, and harmonization are three central concepts that support equivalency of meaning. Instruments that have been standardized through validation and reliability analyses perform consistently across time and populations and, therefore, represent similar meaning across populations and time. Normalization, as it relates to psychometrics, means that values measured on different scales are adjusted to a notionally common scale, while harmonization refers to the recoding of variables so that they are scored with identical values.20,21 Data harmonization refers to all efforts to combine data from different sources and provide users with a comparable view of data from different studies. 20
Health information technology methods to achieve equivalence
Interoperability is central to enhancing the functionality of the EHR. The Office of the National Coordinator for Health Information Technology (ONC) and Healthcare Information and Management Systems Society (HIMSS) offer parallel definitions of interoperability, the extent to which systems and devices can securely exchange data and interpret that shared data across disparate healthcare settings, regardless of the application or vendor.22,23 As previously described, there is great variability in how SBDH domains are measured and stored in the EHR, which presents a challenge to interoperability of SBDH information and, subsequently, equivalency of meaning. Therefore, methods for achieving equivalency of meaning are needed.
The concepts of standardization, normalization, and harmonization are common to psychometrics and the health information technology (IT) standard development community, but the definitions are quite different. The ONC Interoperability Standards Advisory recognizes four types of standards: (1) vocabulary/code sets/terminology (semantics), (2) content/structure (syntax), (3) services, and (4) administrative and non-clinical. 24 This article will focus on the first two standards, semantics and structure (syntax). Semantic interoperability takes advantage of both the structuring of the data exchange and the encoding of the data to a standard vocabulary (terminology), so that the receiving information management systems can interpret the data. 24
In addition, we introduce the concept of terminology binding, which “is a link between a terminology component (semantic) and an information model artifact (structure).” 25 Standardizing with terminology binding is accomplished by encoding clinical data with a code from a standard vocabulary or code system, such as Systematized Nomenclature of Medicine—Clinical Terms (SNOMED CT), Logical Observation Identifiers Names and Codes (LOINC), or International Classification of Diseases (ICD)-10. Normalization of the encoded data is accomplished by associating (curating) the codes into groups (value sets) of semantically similar meaning, while harmonization refers to storing and displaying the encoded data from different sources in a meaningful way 26 and provides actionable knowledge for clinical decision support to the user. Actionable knowledge using SBDH data collected by disparate tools requires standardization, normalization, harmonization, and equivalency scoring by the SBDH domain.
The complexities of SBDH assessment, storage, exchange, and use create challenges in four ways. The first challenge is to electronically store the assessment of various instruments/tools. The second challenge is semantic standardization of the stored data (terminology binding). The third challenge arises when standard codes are not available in shared code systems for encoding. Finally, the fourth challenge, the focus of this article, is to create equivalency of meaning of the data associated with SBDH domains collected in different ways by different tools. Currently, there are no evidence-based guidelines for achieving equivalence in data collected from different SBDH instruments/tools and stored in the EHR. Table 1 summarizes psychometric and health IT methods to achieve equivalence.
Comparison of psychometric versus health IT terms.
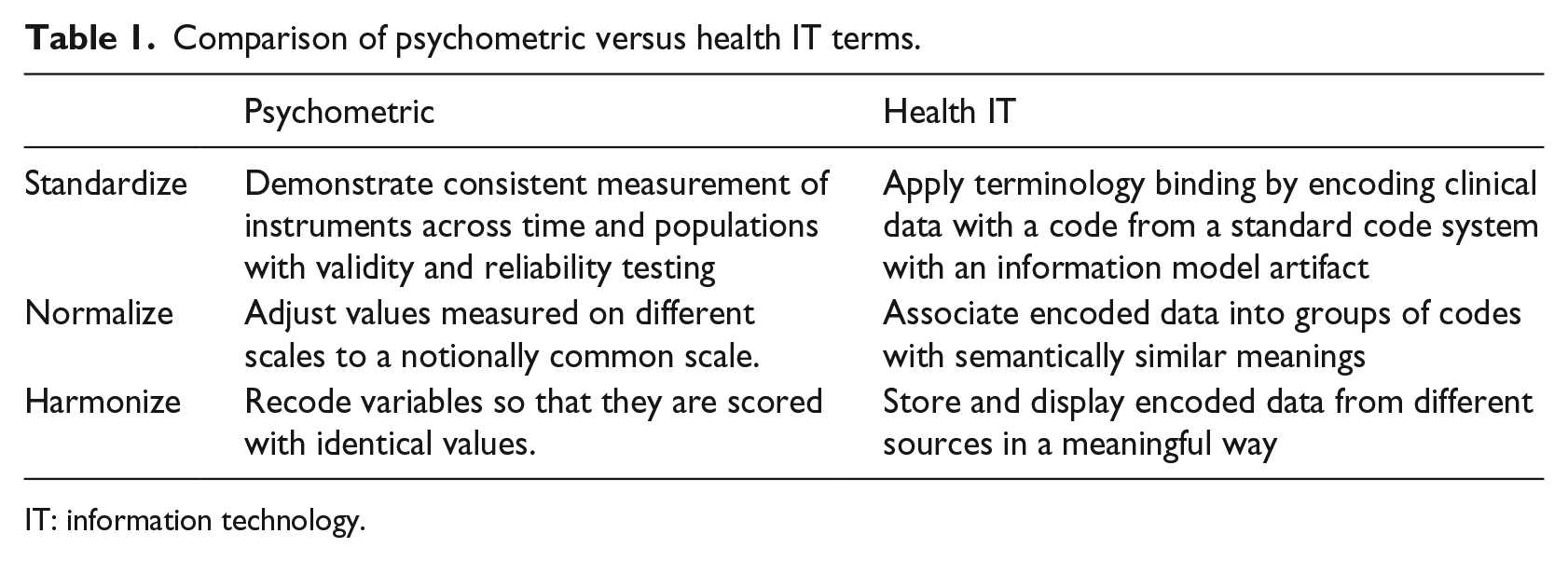
IT: information technology.
In conclusion, only one of the eight SBDH tools evaluated has established validity and reliability; thus, standardizing data collected from different SBDH tools is not possible using psychometric methods. Moreover, generally held practices recommended by the healthcare IT standard development community for standardizing EHR data will not achieve equivalency across SBDH tools. For this reason, the scoring strategy is needed to establish equivalency.
Achieving equivalency
Stewart and Napoles-Springer describe six types of equivalence including conceptual, semantic, operational, psychometric or measurement, item, and criterion equivalence. Conceptual equivalence of constructs and items is realized when the constructs exist, are applicable, suitable, and measured across cultures. 18 In addition, the value or emphasis of each measured domain is similar, and the items represent the definition of the constructs. Semantic equivalence is attained when items have similar meanings to members of different groups in the target and source language. Operational equivalence ensures that uniform methods of survey administration are suitable for the targeted group’s culture, and the respondent groups across cultures are identified using a standard method. Psychometric or measurement equivalence is achieved when comparable psychometric properties are embedded in the source and target measures. Item equivalence is shown when (1) items retain the same measurement level (e.g. biased) in the target and original culture, (2) item weights represent a similar level of importance for items in all groups, and (3) the meaning of and distance between response choices is comparable across cultures. Criterion equivalence is achieved when the interpretation of scores is (1) the same across groups and (2) the same when compared with norms for each group. 21 For classification measures, criterion equivalence means that the phenomenon exists in both cultures. Conceptual and criterion equivalence are applicable to this article.
Results
Strategy to address data capture and storage issues
The critical appraisal of the scientific literature followed a process that
Identified, assembled, reviewed, and critiqued adult instruments that assess SBDH.
Derived a three-tier scoring procedure.
Developed a scoring strategy to create equivalency by the SBDH domain across instruments, settings, and populations.
The three-tier scoring strategy permits SBDH data to (1) be used immediately at point of care (POC) by identifying social needs or social risk factors 3 and an actionable interpretation that links to patient goals and interventions, (2) be consumed within analytics and algorithms and for secondary analysis, and (3) produce a score that reflects total social determinant burden and behavioral burden across settings within a healthcare system. This strategy is an extension of the process reported by Wetta et al. 27
The IOM published evidence-based recommendations suggesting SBDH that should be incorporated into the EHR 1 and, therefore, provided the foundation for the strategy to assess and store SBDH data for (1) diagnosis and treatment, (2) social needs and social risk factor referrals, (3) care coordination, (4) patient experience, (5) risk assessment, and (6) secondary uses for research. Figure 1 lists the SBDH domains and underlying factors associated with the IOM instrument (in blue), the PRAPARE instrument (in green), and both instruments (in gray).1,16,19
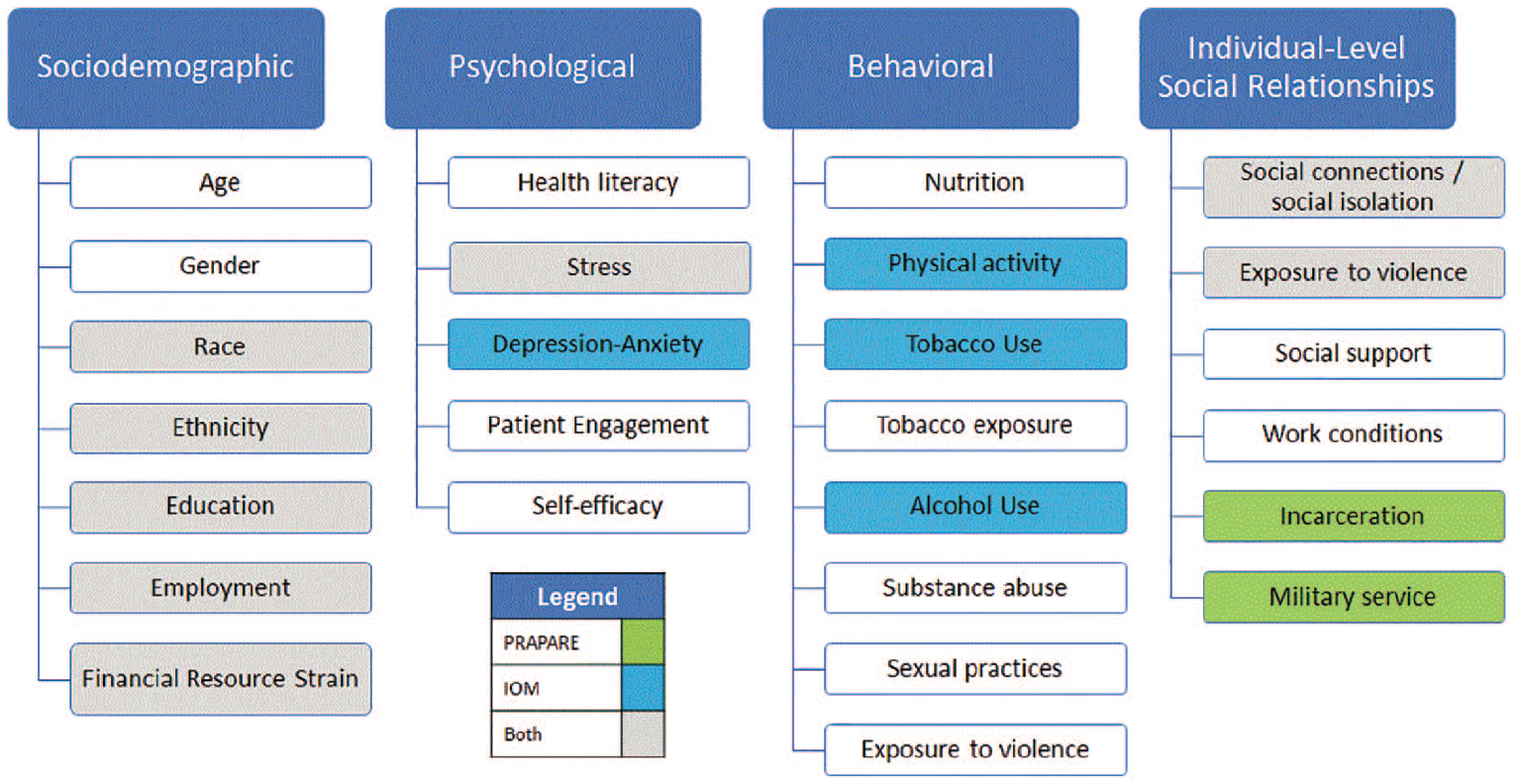
IOM categories of SBDH domains and underlying constructs.
The PRAPARE tool is intended to assess SBDH, which implies the evaluation or estimation of the nature or quality of their influence on health outcomes. Operational definitions of SBDH domains are accomplished by defining how each construct will be measured, in this case, the PRAPARE items. Measurement is the assignment of numbers to units of analysis, but currently, the PRAPARE tool does not assign numerals, nor is it scored or weighted. The PRAPARE tool poses questions with responses that reflect dichotomous and ordinal scales. Thus, a simple scoring strategy was employed to operationalize the measures using the following guidelines: dichotomous measurement (yes = 1, no = 0; present = 1, not present = 0) and ordinal measurement (rank ordered categories assigned numerical values in the ascending order). Items were associated with their respective domain, and each domain was scored separately.
Tier-1: POC scoring
POC scores were achieved by summing response(s) to each domain item(s). For example, “What language are you most comfortable speaking?” is intended to screen for potential language barriers. Responses for various languages are listed. If a respondent lists English as the language they are most comfortable speaking, it was scored 0; any other language received a 1. To derive a domain composite score, the responses were summed and assigned a health concern for language barrier or a risk (e.g. 0 = no risk for language barrier, 1 = at risk for language barrier).
Tier-2: domain equivalency score
The POC scoring varies between tools/instruments as the items assess the constructs differently and responses are captured in dissimilar ways. For example, the IOM instrument uses the Humiliation, Afraid, Rape, Kick instrument (HARK) to assess intimate partner violence, which uses four items with yes/no responses. 16 Any positive (yes) response receives a point; therefore, the composite score for this assessment ranges from 0 to 4, with 1 or more indicating a positive screening for intimate partner violence. For the PRAPARE instrument, there is one item that assesses intimate partner violence, and a positive response indicates a positive screening for intimate partner violence. 14
To create equivalency between the PRAPARE tool and IOM instruments for domestic violence assessment, the domain equivalency score was derived by collapsing the score into two categories as 0 = negative intimate partner violence screening and 1 = positive intimate partner violence screening. No manipulation was needed for the PRAPARE item, but the IOM HARK score would be collapsed to 0/1 rather than 1–4.
Figure 2 provides a visual description of the three-tier scoring strategy as applied to the Financial Resource Constraint domain. For the PRAPARE instrument, there are seven subdomains assessed, including childcare, clothing, food, medications or health care, phone, utilities, and transportation (medically and non-medically related). Responses receive a score of either 0 or 1 depending upon whether the constraint is reported by the individual patient. The range of scores for this domain is from 1 to 9 points.
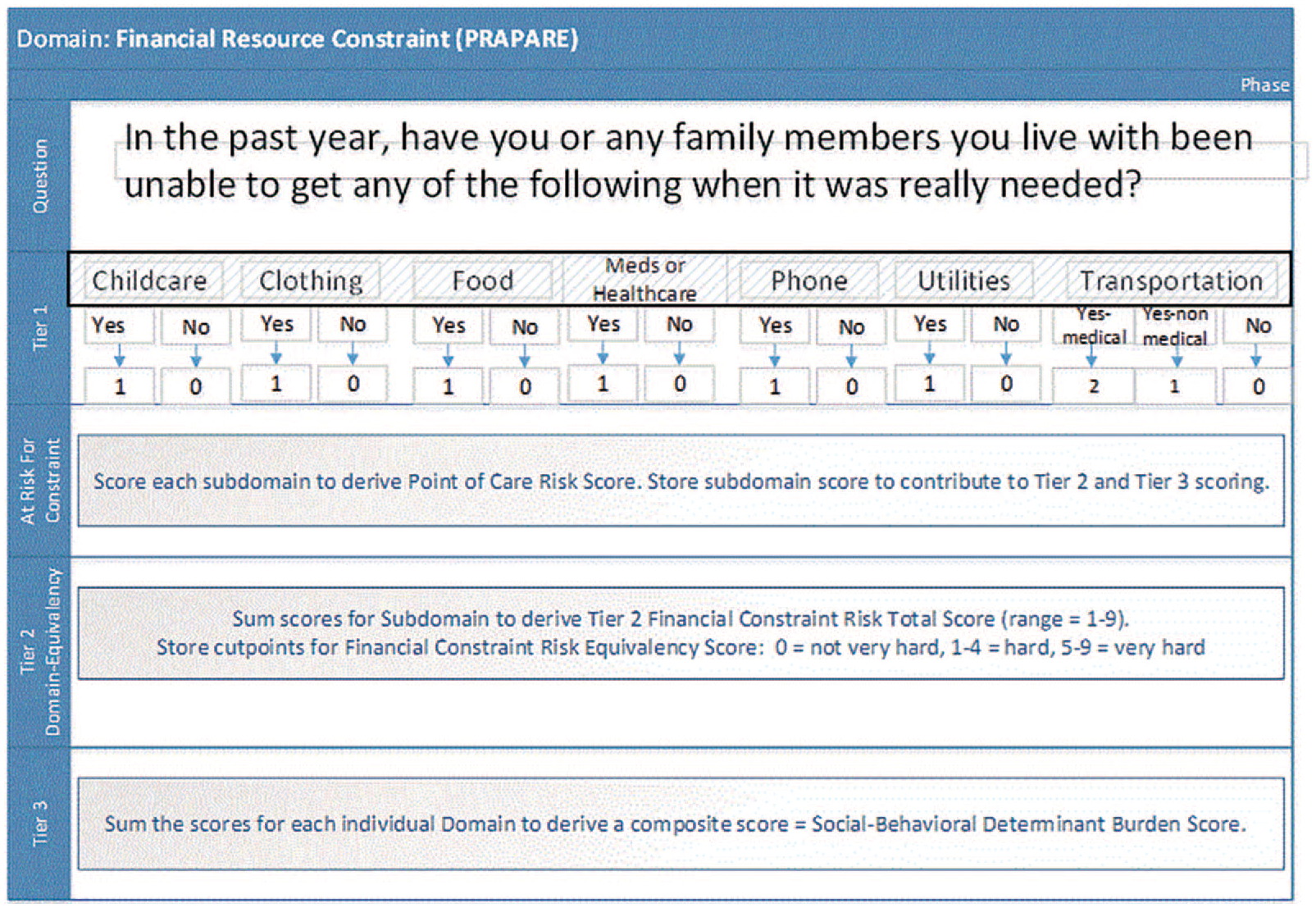
Visualization of the three-tier scoring strategy.
For the IOM instrument, one question is posed, “How hard is it for you to pay for the very basics like food, housing, medical care, and heating? Would you say it is, not very hard, somewhat hard, hard or very hard?” This item provides a potential range of scores from 0 to 3 points. Because the IOM instrument has established validity, reliability, and scoring, the categories of financial resource constraint were adopted: not very hard, somewhat hard, hard, or very hard. Equivalency across instruments was achieved by summing the scores and applying the cutpoints, 0 = not very hard, 1–2 = somewhat hard (at low risk for financial constraint), 3–4 = hard (at moderate risk for financial constraint), and 5–9 = very hard (at high risk for financial constraint).
Likewise, the Social Isolation/Social Connection construct was assessed differently between the IOM instrument and PRAPARE tool. In addition, the scales are inversely scored, which required correction to derive the equivalency score. For the PRAPARE tool, “How often do you see or talk to people that you care about and feel close to? (For example: talking to friends on the phone, visiting friends or family, going to church or club meetings).” Responses are less than once a week (4 points), one time or two times a week (3 points), three to five times a week (2 points), and more than five times a week (1 point). The interpretation of the scores is 4 = at high risk for social isolation, 3 = at moderate risk for social isolation, 2 = at low risk for social isolation, and 1 = no risk for social isolation.
For the IOM instrument, the Social Isolation-Connection score was obtained by summing the points for 4, ordinal scale items that assess the frequency of (1) interaction with friends and family by phone, (2) interaction with friends and family in person (3) religious service attendance, (4) attendance of club/organization meetings, and 1 additional point was assigned for being married or living in a marital-like relationship. Respondents receive 1 point for averaging three or more interactions per week (based on the average of the first two questions), 1 point for attending church services four times per year or more, 1 point for attending club and organization meetings, and 1 point for being married or living in a marital-like relationship. Questions left blank are excluded from the calculation. The instrument scoring was categorized as follows: Most isolated: 0–1 point, Very isolated: 2 points, Somewhat isolated: 3 points, and Not isolated: 4 points. 16 To achieve equivalency, the interpretation of the scores are 0–1 = at high risk for social isolation, 2 = at moderate risk for social isolation, 3 = at low risk for social isolation, and 4 = no risk for social isolation.
Tier-3: social determinant burden score and behavioral determinant burden score
Chronic disease burden is an important global metric used to estimate the burden of illness from chronic disease and injury. 28 Tracking chronic disease prevalence, healthy life years, or disability-adjusted life years supports population health measurement in public health. 29 Similarly, a measure of social determinant burden and behavioral determinant burden will be important to population health management within a healthcare context. The tier-3 scoring sums the domain equivalency scores to provide overall burden scores that measure total social determinant burden and total behavioral burden for a person. These burden scores may be used to document the social and behavioral burden by clinic, hospital, or health system and can be leveraged for planning purposes within an organization or as an indicator of burden at the community level.
Discussion
The IOM calls for clinicians to focus on SBDH factors within their care delivery process, 1 but the complexity of assessment, data storage, and use introduce hurdles to implementation. By incorporating SBDH equivalency scoring with uniformly defined SBDH domains using patient-level data stored in the EHR, comparable interpretation of the information and data interoperability are possible across patient groups and settings. Population health measurement, population health management, patient care delivery, and secondary uses of SBDH data in health-related research or performance improvement initiatives would be optimized. Application of standard measures introduces the prospect for efficient detection of factors that may influence diagnoses, treatment, and referrals and makes the data functional for various systems and purposes. 7 Moreover, it is consistent with the goal of the Gravity Project to support documentation for screening, diagnosis, treatment/intervention, and planning activities within EHR and related systems. 30 The urgent demand for capturing SBDH data, related to growing pressures on providers and systems moving toward value-based care, is driving the speedy adoption of SBDH instruments. However, many instruments have not been assessed for reliability, scoring, or derived cutpoints that support actionable intervention at the POC. In addition, the variation in recommended domains for assessment, numerous use cases, and multiple instruments create difficulty in aligning data gathered with different SBDH instruments/tools. When standard measures are applied in diverse groups, the instrument is generally assessed for conceptual and psychometric equivalence across groups, but these methods are less feasible in a real-world setting. As only one of the eight tools has established validity and reliability, standardizing data collected from different SBDH tools is not possible. Moreover, generally held practices for standardizing EHR data will not achieve the need for establishing equivalency of SBDH data across tools. Current science is not keeping pace with the current need for application in the practice setting.
The strategy described in this article addresses the complexities associated with a lack of national strategy for the assessment, storage, and use of SBDH to promote population health. 7 The tier-1 scoring promotes clinical decision support during a healthcare encounter for identifying social needs or risk factors and prescribing more appropriate referrals that enhance the probability and speed of recovery. The tier-2 scoring supports clinical decision support through artificial intelligence and algorithms and automates potential interventions to address social needs and risk factors. 31 Furthermore, the strategy supports planning for care coordination so that patient’s SBDH complexity is revealed. Care manager workloads can be more equally distributed based upon social and behavioral burden. The tier-1 and tier-2 scoring can inform the healthcare delivery system about ways to tailor care delivery to enhance the patient’s experience based upon their SBDH. Moreover, EHRs are increasingly used for research and performance improvement activities. The merging of equivalent SBDH data with conventional clinical, laboratory, radiology data enhances the potential for comparative effectiveness research.
The IOM’s phase II report, Finding 7–1, suggests that EHR suppliers lack harmonized standards to capture SBDH in a way to promote the exchange of data. 1 Furthermore, the IOM’s Recommendation 7–1 (page 16) is “The Office of the National Coordinator for Health Information Technology’s electronic health record certification process should be expanded to include appraisal of a vendor or product’s ability to acquire, store, transmit, and download self-reported data germane to the social and behavioral determinants of health.” This recommendation for EHR certification requires that the storage of the data supports interoperability. However, the concept of interoperability and equivalency are not interchangeable. Unless the data captured by SBDH tools are stored in a manner to support equivalency, interoperability cannot truly be accomplished.
The equivalency scoring strategy described in this article achieves both equivalency and interoperability. The domain equivalency scoring creates equivalency among tools/instruments, and by encoding the domain equivalency score with a standard code system, interoperability is achieved. This strategy addresses the complexity inherent in applying SBDH in healthcare settings. Using this strategy, health systems can select the tools/instruments that best fit the patient populations served and permits use of data across healthcare systems, regardless of the population or setting.
Additional uses of the equivalency scoring strategy are possible. For example, the strategy could contribute to health system planning using the social and behavioral burden equivalency scores, by domain and overall. In addition, the strategy would permit organizations and health systems to identify community-based partners needed to address social needs and risk factors that interfere with care delivery and disease self-management. Healthcare administrators could use the social and behavioral burden data to plan the distribution of healthcare team members, such as social workers or community health workers, needed to support ambulatory and community settings with the greatest SBDH need. The strategy could also support healthcare systems anticipating Centers for Medicare and Medicaid (CMS) SBDH-based reimbursement policy by documenting the SBDH burden by the provider, organization, health system, regionally, and nationally. Furthermore, the strategy supports research and performance improvement by storing SBDH data with equivalent meaning. Finally, this strategy may help to support the creation of a more holistic vision of SBDH application within health policy circles and within the healthcare industry.
Only one of the four complexities associated with SBDH assessment, storage, exchange, and use was addressed by this article, specifically, to create equivalency of meaning of the data associated with SBDH domains collected in different ways by different tools. But work has begun on the third challenge (e.g. standard codes are not available in shared code systems for encoding). The HL7 Gravity Project, led by the Social Interventions Research and Evaluation Network (SIREN) in partnership with EMI Advisors, LLC, has convened a national public collaborative to identify and harmonize social risk and protective factor data for interoperable electronic health information exchange. 30 Between April and December 2019, food security, housing stability and quality, and transportation access will be addressed, which supports the third challenge to create codes to store social determinants of health. Additional efforts will be needed to address other challenges.
Limitations
Despite following an evidence-based search strategy, relevant literature may have been missed that excluded national organizations that are salient to SBDH policy implications. Likewise, additional SBDH assessment instruments may have been excluded unintentionally. Furthermore, SBDH assessment instruments that may be used in other countries were not included in the critical appraisal. Ongoing monitoring of national organizations, federal websites, and published literature should be maintained to incorporate new SBDH tools/instruments. Finally, the strategy has been applied to the IOM SBDH, PRAPARE, Accountable Health Communities, WellRx, and Health Leads instruments without issue thus far.11,16,19,32,33 Future testing to verify equivalency is planned.
Conclusion
The implementation of standard screening tools/instruments and use of domain equivalency scoring strategy will increase interoperability, reduce hurdles to information exchange within and across organizations, and decrease redundant data capture. 1 As the healthcare industry moves to leverage SBDH data, novel approaches will be needed that permit SBDH data to be applied to the six uses advocated by Adler and Stead. 7 The strategy described in this article supports the six uses recommended by the National Academy of Medicine and addresses the complexities associated with a lack of national strategy for the assessment, storage, and use of SBDH.
Footnotes
Acknowledgements
The authors would like to thank their colleagues at Cerner who provided insight and expertise that greatly assisted with the project. The authors extend their appreciation to Jeff Orndoff and Nate Lewis for their insights.
Author contributions
R.E.W. helped in strategy design, data collection, psychometric data analysis and interpretation, writing, and manuscript editing; R.D.S. helped in strategy design, data collection, terminology data analysis and interpretation, writing, and manuscript editing; and H.G. helped in writing and manuscript editing.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.E.W. and R.D.S. are employed by Cerner Corporation, an EHR supplier.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.