
Abstract
Introduction
The shift toward an aging society and the increasing prevalence of chronic diseases have prompted a transition from hospital-based care to home-based care.1,2 This shift has increased the demand for home nursing healthcare services as patients are now required to manage their medical devices, wounds, and nutrition independently at home.3,4 The COVID-19 pandemic further highlighted the feasibility of managing various symptoms at home. Consequently, the responsibility and burden placed on informal caregivers without professional training has been increasing, and the need for accessible home-based support have increased.5–7
Studies on the characteristics of patients or caregivers receiving home-based care services have reported difficulties in managing indwelling medical devices (e.g., central venous catheter, urinary catheter, tracheostomy tube) or addressing urgent situations.8–11 Patients and caregivers reported that they were not fully prepared to provide home-based care and experienced difficulties due to changes in lifestyle, family relationships, etc.9,10 Home-based care services to support them are provided by home health nurses who visit according to an established schedule. Thus, the role of the patients themselves or their caregivers remains important in critical care activities, such as medical devices management, drug administration, and wound dressing change. However, most perform various care activities without formal training.12–15
Performing patient care activities at home without formal and sufficient training can cause serious problems. Infections account for the largest proportion of unexpected hospitalizations among patients receiving home care.16,17 One of the factors that increases the risk of infections is the presence of indwelling medical devices (e.g., central venous catheters, urinary catheters, tracheostomy tubes, etc.) inserted into the body and exposed to the outside.18–21 Furthermore, household infections are a particularly important problem as they are difficult to detect early and can have serious consequences for patients. 19 To prevent such infections, it is critical to improve patients’ and caregivers’ management skills and abilities through sufficient training and education is critical.19,22
Training and education are essential for patients and caregivers to improve their management skills and abilities by increasing self-efficacy. 23 Studies have supported significant correlations between self-efficacy and caregivers’ management skills and abilities.24,25 Caregivers with high self-efficacy exhibit high caregiving readiness, including physical and psychological preparation alongside knowledge and skills.26,27 These findings indicate that targeted interventions to enhance self-efficacy are needed to improve patients’ and caregivers’ management skills and abilities. Self-efficacy refers to an individual’s confidence and belief in their ability to perform a specific task and has four elements: performance accomplishment, vicarious experience, verbal persuasion, and emotional arousal. 28 When developing interventions aimed at self-efficacy enhancement, incorporating these core elements is imperative. For example, interventions could include helping individuals to gain successful experiences (performance accomplishment), observing others (vicarious experience), receiving positive reinforcement (verbal persuasion), and effectively managing emotional stress (emotional arousal). 28
Considering the effectiveness and accessibility of the intervention methods for patients and caregivers is also crucial. Among various strategies, access via mobile applications plays a pivotal role in improving users’ self-efficacy and promoting self-management activities.29,30 Recent technological innovations have facilitated active interventions targeting patients and caregivers through mobile applications. This approach represents a significant advancement from one-way information transfer to interaction promoting user participation and positively affecting education and psychological support.31,32 These mobile applications facilitate community formation,33–35 provide users with information in various formats,36,37 and enable communication with healthcare providers. 38 Such features reduce the psychological burden on users, enabling them to independently manage their conditions and cope with various challenges.34,39,40 However, to date, most mobile applications aimed at helping patients or caregivers manage home-based care are designed for users with specific diseases, such as cancer, stroke, or heart failure33,36,41 or those using specific indwelling medical devices, such as ostomy or enteral nutrition tube.35,42 While addressing specific diseases or indwelling medical devices may provide specialized information, it is difficult for patients and caregivers managing multiple diseases or devices to effectively utilize them. Users who have experienced using mobile application interventions for specific indwelling medical devices have reported the need for features that integrate and manage multiple treatment routines. 42 Thus, it is necessary to develop comprehensive mobile applications for managing various indwelling medical devices.
This study describes the development of a mobile application protocol designed for patients and caregivers managing indwelling medical devices at home based on Bandura’s self-efficacy theory. 28 This mobile application is aimed at helping patients and caregivers effectively and safely manage their medical devices and symptoms to reduce unnecessary hospital visits and lower the risk of infection. Ultimately, it is expected to positively affect the healthcare system by improving healthcare quality, reducing costs, and increasing patient satisfaction through more efficient utilization of healthcare resources.
Methods
The development of the mobile application was systematically guided by the Analysis, Design, Development, Implementation, Evaluation (ADDIE) model (Figure 1). This model is actively used in developing traditional education methods and in mobile application training.43–45 Mobile application development phases (ADDIE model).
Additionally, the overall development process of the mobile application considered the elements outlined in the Healthcare App Quality Guidelines provided by the Korean Health Industry Development Institute (KHIDI). 46 These guidelines offer direction across multiple dimensions, including effectiveness, reliability, usability, sustainability, design, technological soundness, privacy and data security.
Analysis phase
In the analysis phase, a literature review was conducted to identify the characteristics and needs of patients with indwelling medical devices and their caregivers. We reviewed studies that provided mobile application-based interventions for such patients and caregivers. We searched studies published until October 2024 using databases, including PubMed, CINAHL, and Scopus. A combination of terms was used for the search, including “medical,” “device,” “tube,” “mobile,” “home care,” “self-care,” and “management.” In the literature review, we examined the impact of mobile application interventions on the home management of indwelling medical devices. Through a literature review, we sought to provide clinical evidence demonstrating with effectiveness, a key requirement outlined in the Healthcare App Quality Guidelines. 46
Design phase
Based on the results obtained in the analysis phase, we structured the core components of the mobile application in the design phase to address the key elements of the self-efficacy theory (Figure 2). To implement the components in practice, we selected evidence- and theory-based methods of behavior change techniques (BCTs) suggested by the behavior change wheel, a theoretical framework designed to systematically facilitate individual and group behavioral change to obtain the intended intervention effects.47,48 Behavior change techniques (BCTs) serve as a motivational system designed to help users sustain ongoing engagement, in accordance with the recommendations of the Healthcare App Quality Guidelines.
46
Theoretical framework (Bandura’s self-efficacy theory).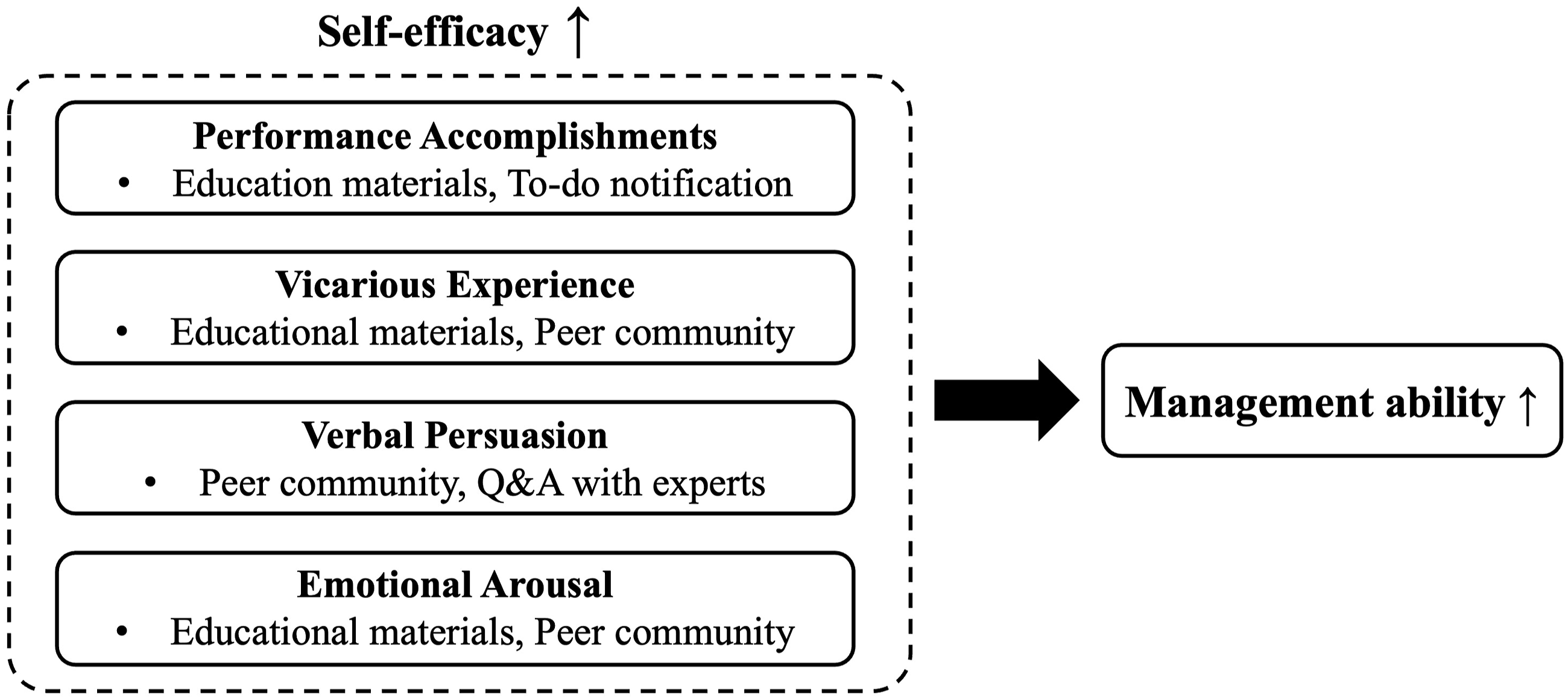
Development phase
In the development phase, a prototype has been created using the Figma Inc., San Francisco, California, USA, software. A prototype is a tool that visually represents the user interface (UI) and user experience (UX). It was used to visualize the mobile application components identified in the previous phase. Based on the developed mobile application prototype, we plan to collaborate with IT professionals to implement it into an actual mobile application. This process adheres to the ease-of-use dimension specified under the usability standards in the Healthcare App Quality Guidelines. 46
Implementation phase
In the implementation phase, we plan to conduct a pilot study to evaluate the self-efficacy, management ability, and feasibility of the developed mobile application. The pilot study will include 12 patients or caregivers managing indwelling medical devices at home in South Korea based on the recommended sample size guidelines for pilot studies.
49
The Participants will use the mobile application for 1 month, and we will measure changes in their self-efficacy, management ability, and feasibility in mobile application use. To measure the self-efficacy levels of the patients and caregivers, we will use the Korean version of the General Self-Efficacy Scale.
50
This scale consists of ten items on a 4-point scale, with a higher score indicating a higher level of self-efficacy.
51
The Cronbach’s
To measure management ability, we will use the Patient Activation Measure (PAM)13-K, which was translated into Korean by Ahn et al.,52,53 and the CG-PAM, which was converted into a caregiver version of the PAM.
54
The PAM13-K and CG-PAM consist of 13 items on a 4-point scale, with a higher score indicating a higher activation state for health management. Cronbach’s
To measure feasibility in mobile application use, we will use the Korean version of the Health-ITUES of Lee and Schnall.56,57 It consists of 20 items divided into four subscales, impact, perceived usefulness, perceived ease of use, and user control, each rated on a 5-point scale. A higher score indicates a more positive outcome on each subscale. Cronbach’s
Evaluation phase
In the evaluation phase, the pilot study results will be analyzed to measure the participants’ feasibility in mobile application use, self-efficacy, and management ability. The results of the pilot study will serve as a foundation for assessing the suitability of the effectiveness items outlined in the Healthcare App Quality Guidelines. 46
Results
Analysis phase
The electronic literature search on the characteristics and needs of patients with indwelling medical devices and their caregivers yielded 525 studies. Among these, 23 studies specifically identified mobile application-based interventions for patients and caregivers. After removing duplicates, ten relevant studies were included. These studies focused on the specific types of indwelling medical devices, including ostomy (n = 6), enteral feeding tubes (n = 3), and urinary catheters (n = 1).
The results of the literature review were analyzed based on the four elements of Bandura’s self-efficacy theory. To achieve performance accomplishment, more than half of the studies provided education on management methods and complications and various health-related information.35,38,58–62 In addition, a systematic and effective guidance was provided to perform tasks through step-by-step instructions,42,63,64 or using the smartphone alarm function.42,58,60,62
To enable the participants to gain vicarious experience, some studies shared educational materials outlining their successful experiences in mobile communities,35,60,64 and users could gain competence and motivation by imitating such successful behaviors. 61 Verbal persuasion was achieved through social opportunities, such as positive communication in a community35,60,64 or obtaining feedback by communicating with experts through mobile applications.38,59,63,64 Furthermore, emotional arousal was also achieved through social opportunities, such as access to various educational materials, community,35,60,64 and expert advice,38,59,63,64 allowing participants to believe that they can overcome stress and fear.
These mobile interventions exerted positive effects on several aspects of home-based management in addition to Bandura’s four elements. They provided continuity and accuracy of care, reducing the psychological burden on patients and caregivers.42,60,63 Facilitating remote interaction with healthcare professionals contributes to psychological stability and improved quality of life.35,64 Moreover, the accessibility of educational resources through mobile applications leads to higher satisfaction than that of traditional methods, such as brochures,38,61,62 and promotes self-management of indwelling medical devices.58,59 These effects guide users in utilizing the mobile application to induce changes in appropriate caregiving behaviors, thereby enhancing their self-efficacy.
Design phase
Among the BCTs, “Information about antecedent” and “instruction on how to perform the behavior” have been employed to enhance performance accomplishment. 48 The proposed mobile application provides education on various diseases and indwelling medical devices to improve the users’ physical and psychological capabilities. This education enables users to acquire the necessary information and the ability to effectively manage medical indwelling devices. Furthermore, the educational materials integrate voice-based artificial intelligence (AI) to help users utilize them usefully. For example, if users have questions regarding the antecedent procedure while disinfecting a patient’s skin, they can request guidance through voice commands and receive the corresponding assistance. The mobile application has an alarm function for tasks set up by users, thereby reducing the psychological burden associated with indwelling medical devices management. This alarm function facilitates the timely completion of necessary actions by users and contributes to the enhancement of their psychological capabilities. Users are automatically motivated by setting their own alarms and creating management records.
The BCTs for achieving a vicarious experience include “self-monitoring” and “demonstration of the behavior.” 48 The mobile application users will monitor and imitate an educator’s successful behavior through educational materials. The mobile application will also include a peer community function to achieve behavior change through the BCT “social support.” 48 It provides users with social opportunities through active participation, and users gain reflective motivation by observing others and sharing their experiences.
Achieving verbal persuasion can be realized by utilizing the BCT “information about health consequences.” 48 Providing information on care-related items can facilitate the management of indwelling medical devices and contribute to the creation of a home-based care environment. This facilitation can also be achieved by obtaining social opportunities through behavior changes resulting from “social support”, 48 such as peer communities and Q&A with medical experts.
The BCTs “instruction on how to perform the behavior,” “information about antecedent,” and “social support” can be employed to induce behavioral change to achieve emotional arousal. 48 Specific strategies include providing social opportunities to transform stress into confidence through various educational materials and providing emotional support through peer communities.
Development phase
Figure 3 presents the prototype, including the interface of the mobile application. This mobile application was designed with UI and UX in mind, emphasizing user convenience through an intuitive interface that enables users to manage the elements of the indwelling medical device on a single screen. Figure 3(a) shows an alarm function for a schedule to be done in the locked screen state. Figure 3(b) depicts a screen showing registered indwelling medical devices and an example of when only one central venous catheter is registered. Figure 3(c) shows a settings screen for registering management schedules and information related to registered medical devices. Figures 3(d)-(e) show detailed management screens for registered medical devices, particularly screens for to-do tasks, educational materials, diary, and product quantity management. Mobile application prototype (a) Mobile application alarm function; (b) Main screen (when the registered indwelling medical device is a central catheter only); (c) Indwelling medical device registration and management schedule, information registration screen; (d–e) Detailed management screen for indwelling medical devices.
The mobile application will be developed in collaboration with IT and nursing professionals, reflecting the prototype above. The validity of the mobile application components will be verified by at least three nursing professionals. Nursing professionals will ensure that the UI and UX of the mobile application are designed to reflect the needs and expectations of actual users. For the pilot study, this mobile application will be developed primarily for Android users and will be produced in “Android application package (APK)” format. After verification through the pilot study is completed, the mobile application will be developed and expanded with the iOS operating system, enhancing our offerings in the mobile market.
Implementation and evaluation phase
The pilot study is scheduled to be conducted following the completion of the mobile application development. Based on the results of the one-month-long project, we plan to conduct the main study after supplementing the mobile application functions.
Discussion
This protocol study addresses the importance of developing the need for new mobile applications tailored to the needs of patients and caregivers managing one or more indwelling medical devices at home. A notable strength of this mobile application is that its content was developed based on a well-established theoretical framework, and the development process was guided by the ADDIE model, which is recognized as a valuable guideline for effective interventions. In addition, we have established a strong foundation for delivering high-quality services by incorporating the Healthcare App Quality Guidelines set forth by the KHIDI throughout every phase of mobile application development. 46
Although AI-based medical devices and digital therapeutics are assuming an increasingly pivotal role in clinical practice, their safety and efficacy cannot be adequately ensured without a clear regulatory framework, which had remained insufficiently addressed in South Korea until the enactment of the Digital Medical Products Act in January 2025. The Act comprehensively governs the manufacturing, importation, clinical trial design, and evaluation of digital medical products, aiming to enhance national health and promote the development of high-quality, safe, and effective digital medical products. 65
The Act classifies these products into three categories: (1) digital medical devices, (2) digital combination pharmaceuticals, and (3) digital medical and health support devices. The mobile application developed in this study is expected to fall under the third category. Digital medical and health support devices employ digital technology to monitor, measure, collect, and analyze biosignals for the purpose of supporting healthcare or maintaining and improving overall health. These low-risk devices contribute to health promotion by promoting healthy behaviors, analyzing lifestyle data, and reducing the risk of chronic diseases.
The Act requires developers of such devices to obtain performance certification to ensure product quality and safety, but specific regulations regarding performance certification for digital medical and health support devices are scheduled to take effect in 2026. We are committed to ensuring full compliance with these forthcoming regulatory requirements as they are enacted. In the meantime, our mobile application can be piloted and distributed without undergoing a certification process.
This mobile application incorporates several unique features that enhance its utility for patients and caregivers managing indwelling medical devices at home. First, various indwelling medical devices can be directly registered in the mobile application, and users can set up tasks to be performed and alarms for these tasks; users can also continuously adjust these tasks based on the patient’s condition. Second, by using voice AI, users can obtain the necessary information while performing actions related to managing medical devices or dealing with patients. This supports the continuous and hygienic performance of actions as users do not need to operate the mobile application to obtain information when performing the task. Third, when problems arise during the care of indwelling medical devices, users can verbally describe the situation to an AI chatbot. The AI chatbot analyzes the user’s indwelling medical device information and voice keywords to provide general solutions. The information provided by the AI chatbot will be strictly regulated to offer only general guidance on indwelling medical device management, without extending to medical judgment or diagnosis. We will also adhere to legal regulations in accordance with the Personal Information Protection Act to prevent the unauthorized collection or use of personal information in the context of AI utilization. These unique features can also be useful in the future when individualized information is needed for the patient’s management status, such as when a patient is admitted to a medical institution or a change in caregiver is required.
After the pilot study is completed, the results will be disseminated through peer-reviewed journals and presented at national and international healthcare conferences, such as the Health Information and Management Systems Society Global Health Conference. Additionally, during the mobile application distribution phase, we will prioritize obtaining Korea’s software quality certification—GS (Good Software) certification, administered by the Ministry of Science and ICT. 66 This certificate emphasizes key aspects of software quality, such as functionality, performance, usability, and security. Although software quality certification is currently not mandatory in South Korea, we are committed to delivering highly reliable services to our users through this certification.
Furthermore, we will continuously explore ways to make this high-quality mobile application widely available to individuals, hospitals, and communities. This includes collaborating with hospital systems for pilot implementation, partnering with digital health companies for commercialization, and leveraging mobile application distribution platforms such as Google Play and the App Store. To reach a broader audience, summary reports, including the core findings and benefits of the application, will be distributed through social media platforms and online forums focused on patient care and medical technology.
This study has limitations that should be addressed in future research. First, the literature review conducted in this protocol primarily focused on intervention studies involving mobile applications for patients with ostomies, which limited the analysis of applications targeting other types of indwelling medical devices. Future research should incorporate qualitative data from individuals with various types of indwelling medical devices to provide more comprehensive and context-specific insights for mobile application development. Second, as clinical validation has not yet been conducted, the effectiveness and usability of the mobile application remain to be established. The upcoming pilot study is expected to provide valuable feedback that will inform further revisions prior to broader implementation.
Conclusion
This protocol study addresses the need for novel mobile applications tailored to the needs of patients and caregivers managing one or more indwelling medical devices at home. Research to date indicates a significant demand for such mobile applications; however, none have been developed or implemented thus far. The mobile application designed in this study aims to support patients and caregivers in better managing indwelling medical devices by providing support that enhances self-efficacy in performing care tasks, thereby preventing complications at home, such as infections. Furthermore, if the mobile application is expanded for use in local communities or hospitals, it could facilitate the monitoring of patient management status with indwelling medical devices at home and provide valuable feedback. Ultimately, our mobile application will ensure continuity of care throughout the treatment journey and contribute to improvements in physical and psychological health.
Footnotes
Acknowledgments
The authors express their sincere appreciation to Professor Heejung Kim from the Department of Nursing at Yonsei University for her invaluable guidance and support in conceptualizing the mobile application prototype. We also extend our gratitude to Hyunyoung Lee and Yoojin Jeon for their collaborative efforts in the development and design of the mobile application’s UI and UX.
Authors contributions
Anna Lee contributed to the research by developing the methodology, conceptualizing the study, and writing the review and editing. Dakyung Lee was involved in conceptualization, data curation, formal analysis, visualization, and writing the original draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.