
Abstract
We explored the potential of asthma apps to support self-management and identified preferred features that enable users to live with asthma. We recruited patients from five UK practices and social media; observed their usage of our app, administered a questionnaire and interviewed a purposive sample of patients and professionals to explore preferred features. Thematic analysis of interview was synthesised with quantitative data. A total of 111 patients used our app for 3 months. We interviewed 15 patients and 16 professionals. Participants were interested in a broad range of self-management support strategies, including action plans, monitoring with feedback, allergy/weather warnings and tailor-made running coaching. Professionals wanted to integrate patients’ logs with practice records, though were concerned about data overload and risk of patient dependency. We propose a paradigm shift - from apps developed to provide features that are easy to implement technologically, to an approach in which apps are designed to deliver theoretically grounded preferred components.
Introduction
Asthma is a chronic disease affecting over 230 million people worldwide 1 and 4.3 million adults in the United Kingdom. 2 There is overwhelming evidence that supported self-management of asthma improves control and reduces attacks.3–6 British Thoracic Society/Scottish Intercollegiate Guidelines Network (BTS/SIGN) 3 describes the core components for self-management as ‘education, action plan and professional support’. However, this is a medical model of self-management. The definition of self-management is broader than this, for example, also including coping with emotional and role challenges of living with asthma. 7
The Practical Review in Self-Management Support (PRISMS) taxonomy, derived from a systematic meta-review of 969 unique randomised controlled trials (RCTs) of supported self-management in 14 conditions, offers a pick list of support strategies that healthcare systems should consider when developing services to support self-management for long-term conditions. 8 These include information (about the condition and/or its management), information about available resources, agreement on specific clinical action plans, regular clinical review, monitoring of the condition with feedback, support with adherence, provision of equipment, easy access to advice when needed, training to communicate with healthcare professionals, training for everyday activities, training for practical self-management activities, rehearsal for psychological strategies, social support and lifestyle advice.
Digital technology has the potential to contribute to many of these components. 9 However, today’s apps typically only focus on logging data.10,11 Therefore, we aimed to explore the features that patients and healthcare professionals utilised and wanted in a self-management app with reference to the theoretically grounded broader approach of the PRISMS framework.
Methods
Ethical approval
The study commenced in September 2016 and ended in July 2017, with the approval of the NHS South East Scotland REC 02 and NHS HRA (ref: 16/SS/0101). All participants provided their fully informed consent.
Design
We used mixed methods including user feedback on a prototype app, questionnaire surveys about preferences and qualitative interviews exploring patients and professional perspectives on self-management features. Building on frameworks described by Creswell et al., the qualitative analysis is the major component of the study; we included some observational quantitative data to enrich the description of the ‘wanted’ features.
Practice and patient recruitment
Practice recruitment
We recruited five primary care practices meeting our eligibility criterion (an asthma trained nurse willing to participate in the study) in Lothian (Scotland) and Oxford (England). The Scottish Primary Care Research Network (SPCRN) invited potential practices from diverse demographic areas: rural village, suburban, town and city, representing different populations with respect to deprivation and age. We also approached a practice from Oxford, operating within the English healthcare system.
Patient recruitment for piloting prototype ‘app’
We recruited patients through their primary care practices and through social media to use the prototype app and provide quantitative usage and questionnaire data. We aimed to recruit adult asthma patients who could manage their own asthma independently:
Recruitment through their practice. We included patients (aged 16 years old or over) with active asthma, 12 identified from the practice register. Patients were invited by letter from their family doctor. Patients who had annual asthma reviews within our study period were invited to participate by their asthma nurse during the consultation.
Recruitment through social media. We posted advertisements on Facebook and Twitter accounts of Asthma UK and the Asthma UK Centre for Applied Research. Patients who were interested in trying our app were asked to confirm their eligibility by answering the eligibility questions (adults with asthma registered with a UK general practitioner (GP)). Eligible patients were automatically directed to the information leaflet on our project website and read the information before giving consent, registering and using the app.
Sampling for qualitative interviews
We used purposive sampling, from among those invited by their practice for individual interviews, to achieve a maximum variation sample. Sampling was based on age: young adults (16–25 years), adults (26–60 years) and older adults (60+ years); ownership (or not) of an asthma action plan; and previous user (or not) of healthcare apps. We sampled 15 patients, a number likely to achieve data saturation and practical within our resources, for individual interviews. We also requested interviews from the healthcare professionals involved in asthma care.
App prototype
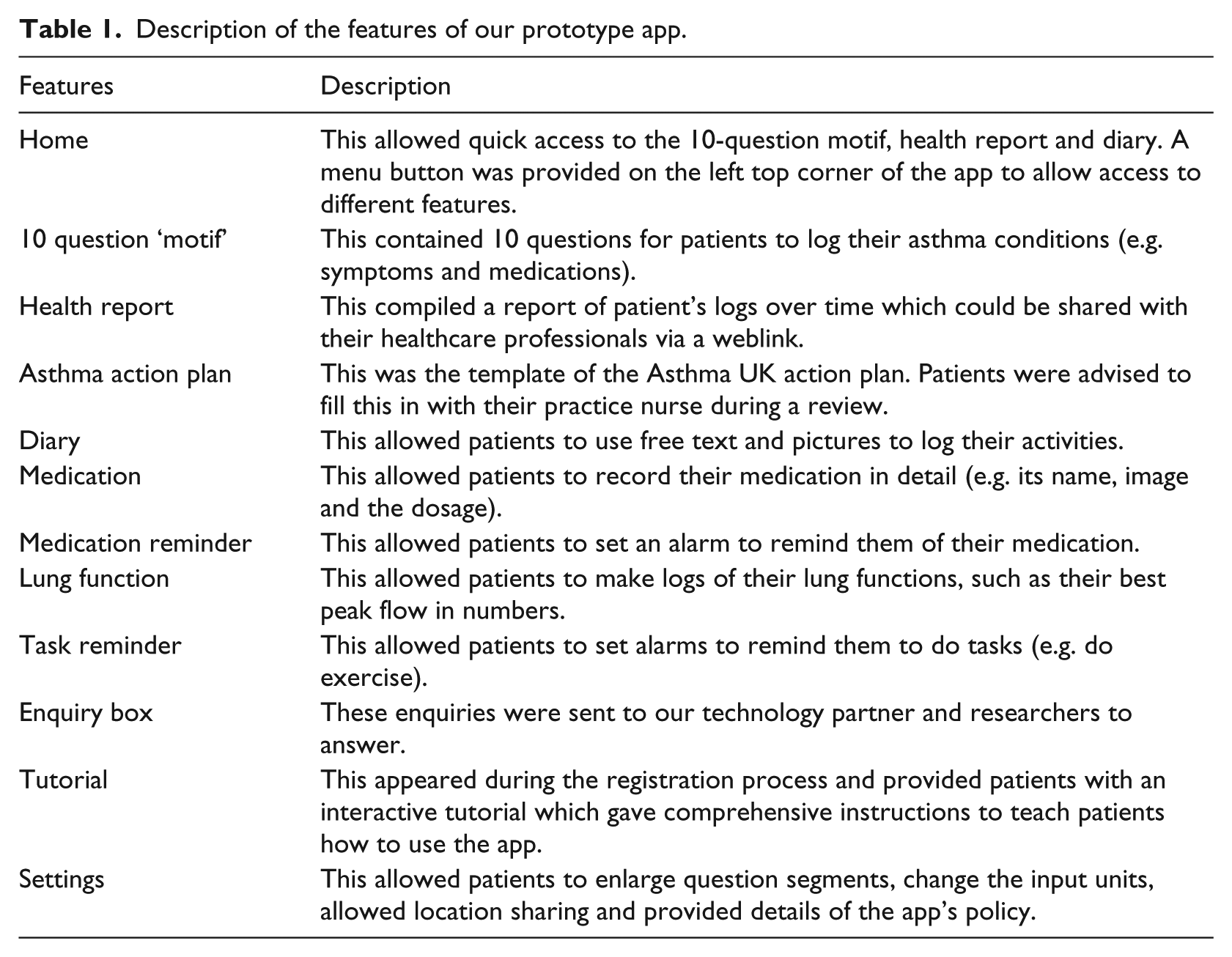
Our prototype app was built on the uMotif 13 platform and provided self-management support features to patients. We chose the app’s features with reference to the comments from our lay and professional advisory groups (four asthma patients invited from the Patient and Public Involvement group in the Asthma UK for Centre for Applied Research, five GPs and two asthma nurses). Some screenshots are shown in Figure 1 and the features are described in Table 1. Participants used the app for up to 3 months. Patients who did not have an asthma action plan were advised to arrange a consultation with their GP/asthma nurses to complete an action plan on the app.
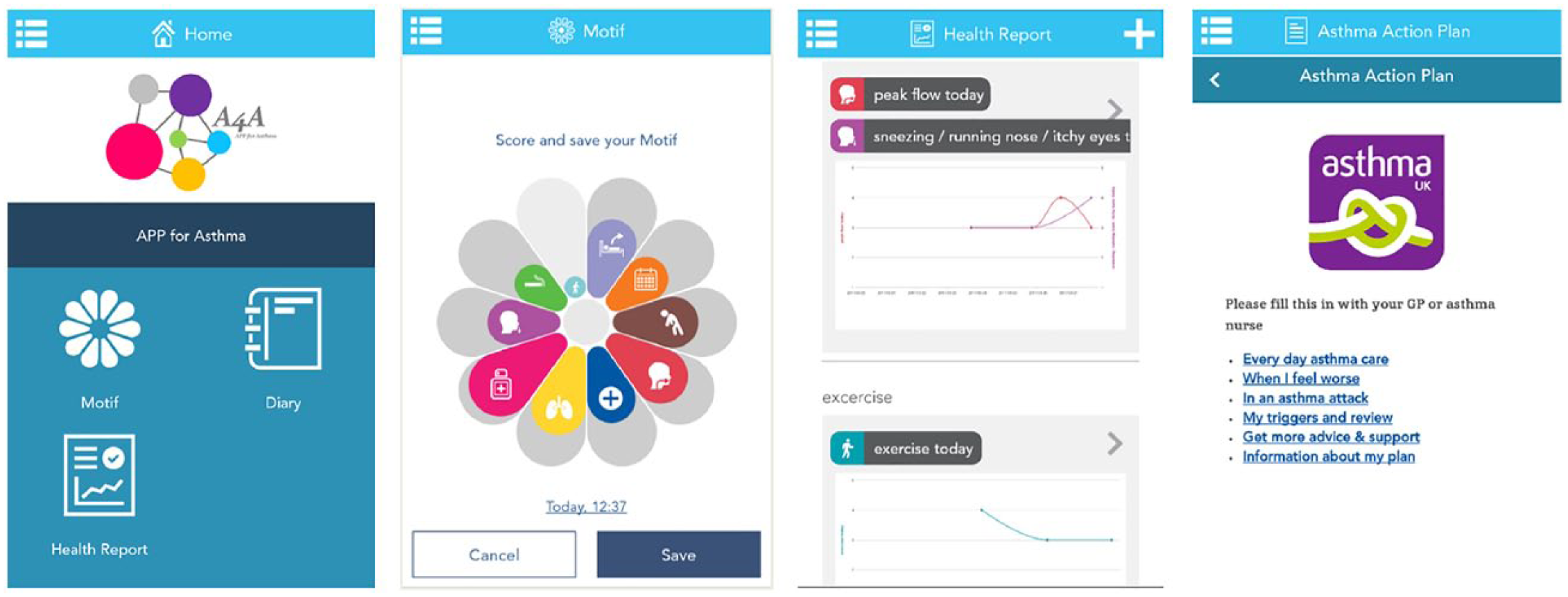
Screen shots of our app: (from left) home, 10 symptom questionnaire, health report and asthma action plan. uMotif configured their app platform for our chosen features.
Description of the features of our prototype app.
Data collection
We collected data in three ways:
Usage data. We collected the patients’ routine app data: weekly usage, usage frequency of each of the features (10-symptom ‘motif’, asthma action plan, diary, medication list, lung function log, medication reminder, task reminder; we could not monitor the use of the shared health report), retention rate and monitoring data at 30, 60 and 90 days.
Questionnaire data. All patients were invited to complete online questionnaires about features they ‘wanted’ to support their self-management before and after using the app. The pre-study questionnaire was part of the registration process and the post-study questionnaire automatically appeared on the patient’s app on day 90. See Supplementary file A for the questionnaires.
Qualitative interviews. Patients were interviewed before and after using the app for 30 days, to explore their preferences for supporting features available – or wished for – on the app. Healthcare professionals from participating practices were asked about the potential of the app to support self-management and the interface with their clinical practice. Practice managers and administrative staff were asked for their thoughts on the potential impact on their workload if an app system were implemented. See Supplementary file B for the topic guides.
Data synthesis and analysis
Quantitative analysis
Patients’ questionnaire ratings of the app features they wanted, their usage of the features of our app and their pre-/post-study action plan ownership were analysed using descriptive statistics.
Qualitative analysis
Interviews were digitally recorded, transcribed and entered into NVivo version 11 14 for analysis. We used framework analysis employing PRISMS taxonomy of self-management support strategies to explore the features that patients and practices wanted to support their self-management. 8 Two reviewers (C.Y.H. and H.P.) discussed the interviews, coded one interview independently and compared decisions to standardise the coding. The agreed framework and coding conventions were used to code the rest of the transcriptions, with additional decisions discussed iteratively within the study team.
Interpretation
The results of the data synthesis were discussed with a lay advisory group and with a multidisciplinary team of healthcare professionals, ehealth researchers, technology developers at a number of conferences and meetings.
Results
Participants
Professionals
Five medical practices in the UK were recruited (four in Lothian and one in Oxford). Sixteen GPs, asthma nurses, practice manager/receptionists in the five practices were interviewed (14 in Lothian and 2 in Oxford). Most of the participants did not have experience of using healthcare apps or activity tracking devices.
Patients
A total of 111 patients were recruited to pilot the prototype ‘app’ and provide usage/questionnaire data (22 via their practice; 87 from social media). The pre-study questionnaire was completed by 101 patients, 23 filled in the post-study questionnaire. The majority (87%) were female, in the 26–45 years old age group (58%) and only 43 per cent had an asthma action plan. Fifteen patients with a range of demography, healthcare and technological experience contributed to the qualitative data collection. Their characteristics are detailed in Table 2.
Practice and patient demographics.
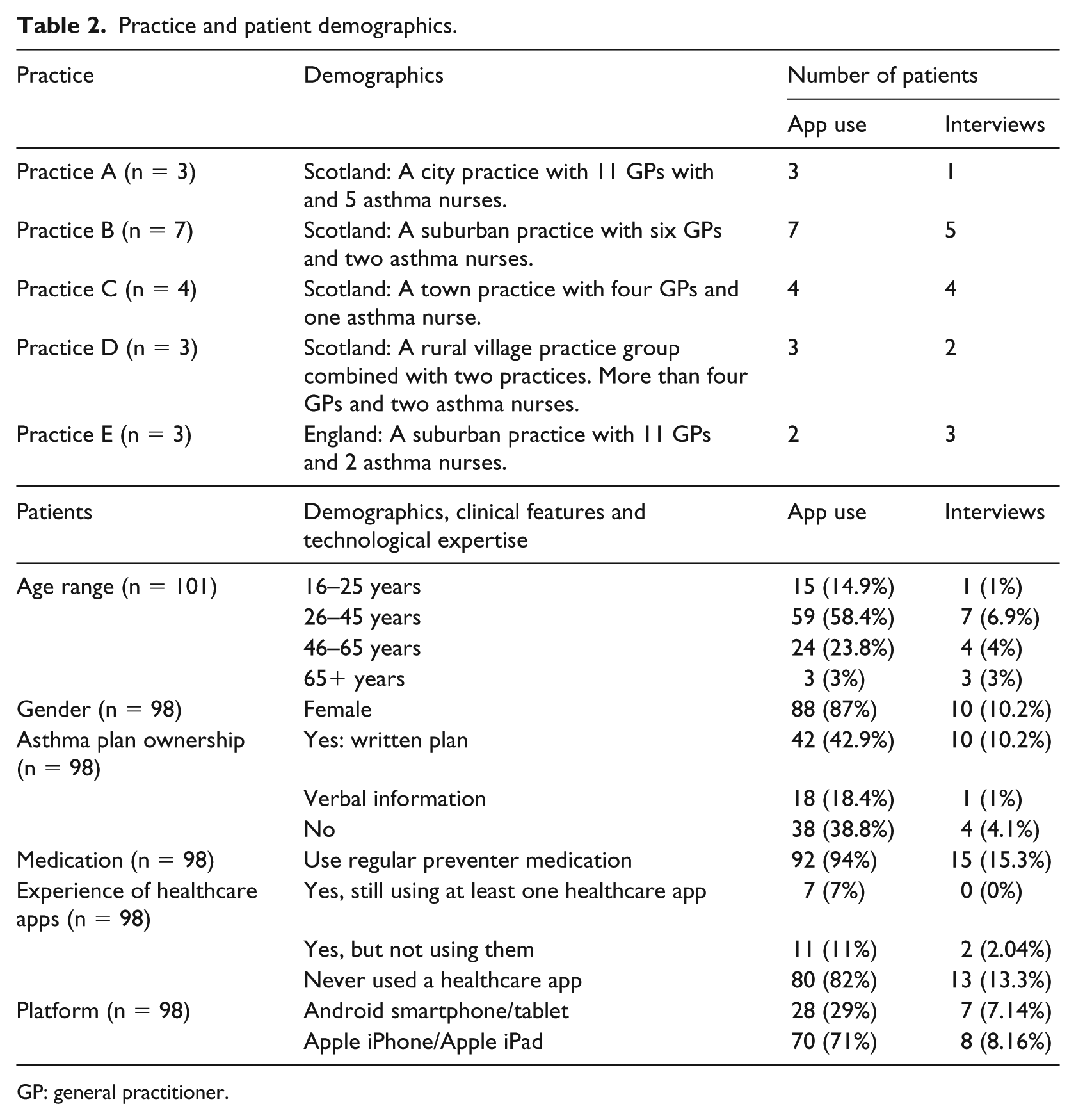
GP: general practitioner.
Usage of the features of the prototype app
Patients’ usage of the self-management support features are summarised in Table 3. The 10-question ‘motif’ was used at least once by almost all the patients (98/111, 88%); the next most commonly used features were the asthma action plan (42/111, 38%) and diary (40/111, 36%). Of the 98 patients who used the ‘motif’, 18 only used the feature once. Other patients used it at various time intervals: daily, weekly or monthly. Eleven of the patients did not use any of the eight features on the app; none of whom had any experience of healthcare apps although six were recruited by social media. A logging reminder that ‘popped-up’ at 18:00 every day was a built-in feature in the app. In total, 105 (105/111, 95%) patients kept this feature, 6 patients (6/111, 5%) disabled it.
Summary of patients’ and healthcare professionals’ wanted features on asthma self-management app.
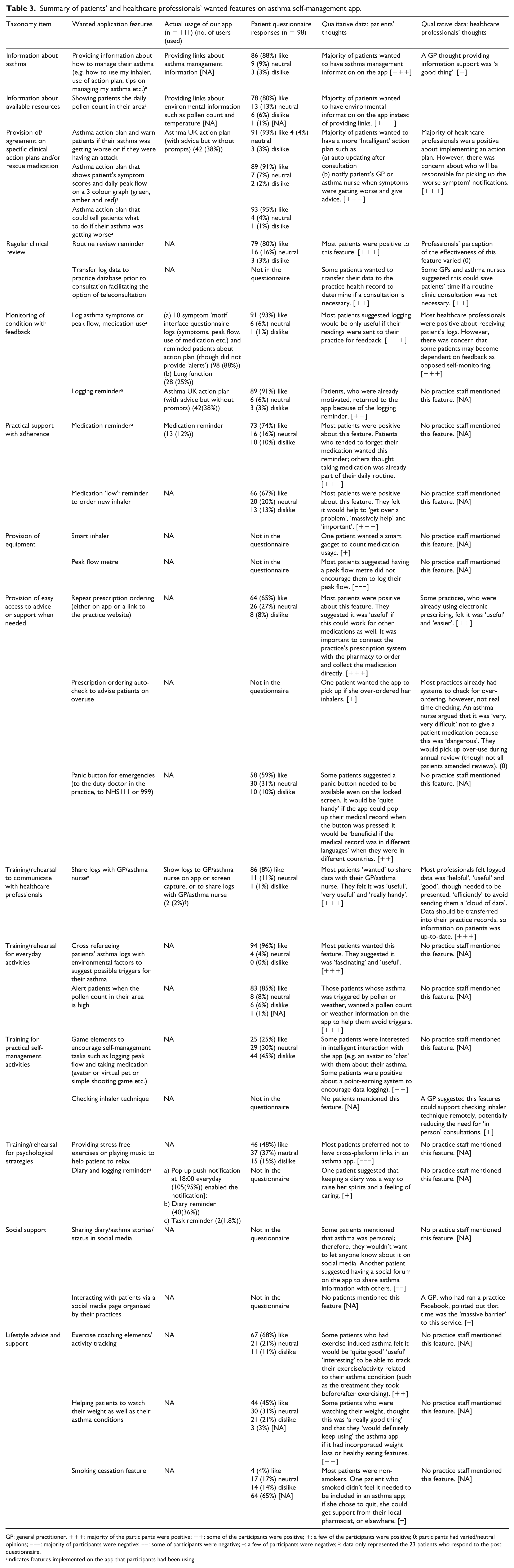
GP: general practitioner. +++: majority of the participants were positive; ++: some of the participants were positive; +: a few of the participants were positive; 0: participants had varied/neutral opinions; −−−: majority of participants were negative; −−: some of participants were negative; –: a few of participants were negative; ‡: data only represented the 23 patients who respond to the post questionnaire.
Indicates features implemented on the app that participants had been using.
Action plan completion
During the course of the study, the proportion of action plan ownership increased from 43 per cent (42/98) to 63 per cent (62/98). Of the 20 patients who were without an action plan before our study and adopted one on our app, 9 patients told us how they completed the plan. Five of them completed the action plan without consulting their GP/asthma nurse; three asked their asthma nurse to complete a paper-based action plan and transferred the data onto the app themselves; and one completed the action plan on the app with an asthma nurse during a consultation.
Perceptions of patents and healthcare professionals on features related to the PRISMS taxonomy
Table 3 maps the usage of features on the prototype app, questionnaire responses and findings of the qualitative interviews related to the 14 items of the PRISMS taxonomy. Additional supporting quotations can be found in Supplementary file C. Figure 2 illustrates the features that patients wanted in an app. The text below synthesises the findings from the qualitative interviews with the usage and questionnaire data.
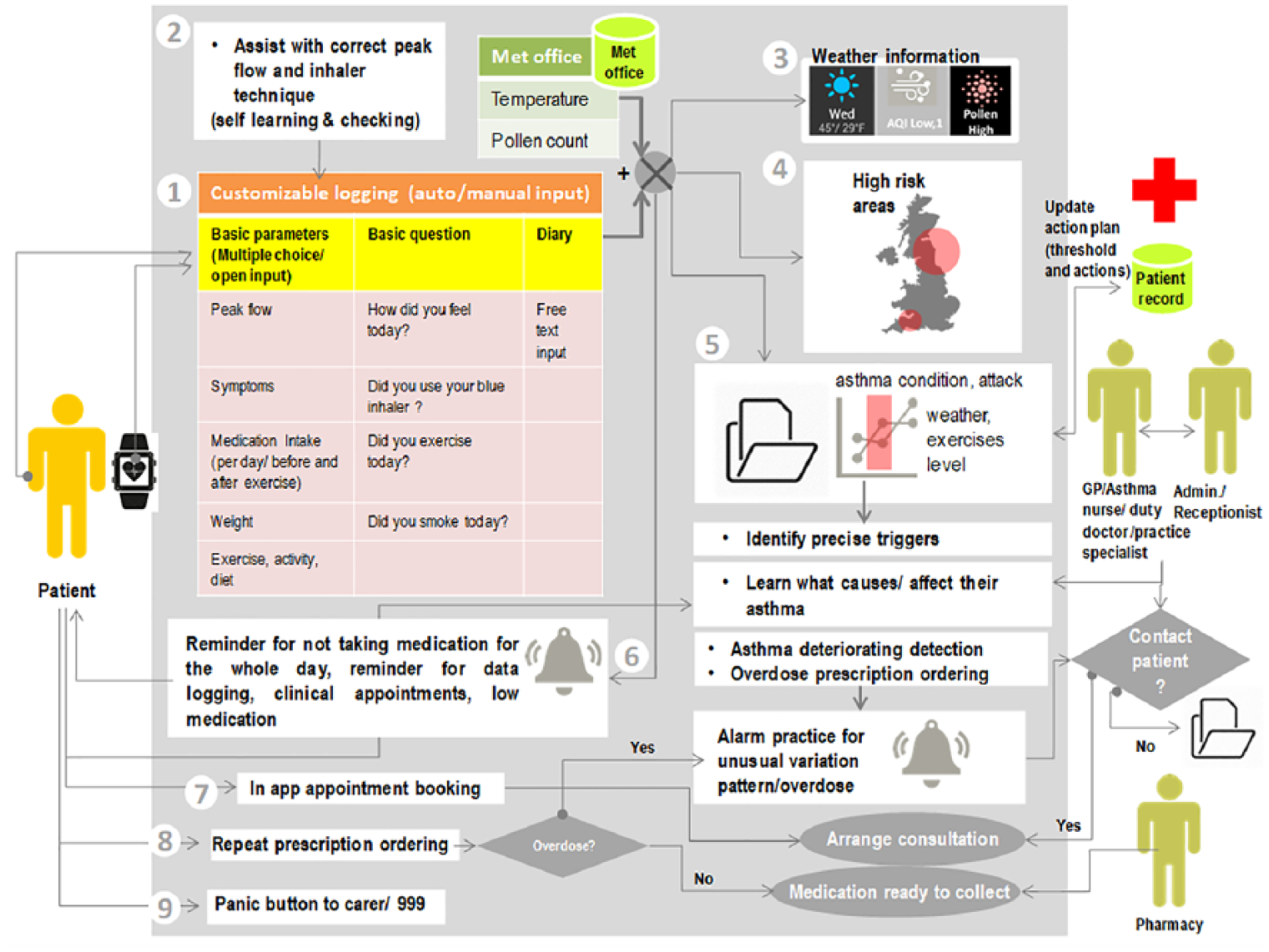
Schematic of the features that patients and healthcare professionals wanted to see on app.
The features that respondents to the questionnaires said that they wanted varied. Most of the patients and healthcare professionals wanted to see asthma action plans and the ability to monitor their asthma with feedback features on the app. Although patients used the monitoring and action plan more than other features on our app, <40 per cent actually used the action plan.
Other desired features were related to patients’ asthma type. Ninety per cent of patients, who had pollen/environmental-triggered asthma, wanted to be able to cross reference their asthma logs with environmental factors to suggest possible triggers and support decisions on everyday activities. Some people with exercised-induced asthma wanted to incorporate exercise coaching elements on the app such as advice on running intensity with reference to their asthma. In contrast, there was less interest in incorporating weight loss and smoking cessation elements. Although not available on the app, some patients mentioned they would like to share their asthma story on social media, and wanted the facility to order repeat prescriptions. Game elements such as avatars, virtual pet or shooting games to incentivise adherence to peak flow logging and taking medication were not considered desirable by most of the patients.
Provision of asthma action plans
Over 90 per cent of patients wanted a digitised action plan but they felt that the plan needed to be ‘intelligent’ such as auto updating their best peak flow and treatment schedules after consultations and to notify them when symptoms were getting worse and to give advice. Sending a notification to the practice computer system when symptoms were moving into the amber zone of the action plan was also suggested by some of the healthcare professionals. However, there was concern about who would pick up the alarm: So if things weren’t good then Google would tell us and then we could text back or send a message saying this is going on could you come and see us. (Asthma nurse 01) It depends where the alarm is situated … It would be annoying if it was on the actual front reception desk where we’re very busy, patients coming in, telephone calls coming, whereas if it was in a specific, you know obviously we have the admin team, you know in the rear office therefore it would pull attention and somebody would obviously attend to it. (Administration staff 04)
Thirty-eight per cent of our app users looked at the action plan, though they felt that the app did not encourage them to use it. However, they suggested the app did provide a trigger for some patients who did not already have an action plan, to acquire one.
Monitoring of condition with feedback
Over 90 per cent of patients indicated in the questionnaire that they wanted to be able to log their condition on the app, though in reality 75 per cent (83/111) had stopped logging by 30 days. The commonest reason given for stopping logging was that they had well-controlled asthma and that they ‘knew themselves’; therefore, it was boring or unnecessary to monitor their peak flow or symptoms: Bored to the extent that I think ‘why am I doing this?’ … I know how to manage my asthma. (Patient participant A7, 65+, M)
Patients suggested the logs ‘needed’ to be sent to their healthcare professional in order to make logging worthwhile. Most healthcare professionals were positive about responding to patients’ logs and one GP suggested it was helpful because ‘they (the practices) don’t have a mechanism for knowing when people are either symptomatic or asymptomatic unless they have an exacerbation’. However, some thought this approach might create patient dependence on professionals and discourage self-management. For logging frequency, some suggested it could be adjusted according to asthma controlled status: Well as long as my asthma is very minor and it’s under control but if it got to a stage where my asthma was beginning to be a big problem and was out of control then it might be useful to have the app giving me extra information but I don’t need it just now. (Patient participant A1, 46–65, M)
Discussion
Summary of findings
Patients and professionals expressed interest in a broad range of self-management support strategies that they would like to see incorporated into an app. The most ‘wanted’ features were provision of asthma action plans and monitoring of control with feedback. Professionals wanted to be able to transfer patients’ logs to their practice records, though they were concerned about managing data and the potential for encouraging patient dependency. Apps had the potential to support routine tasks, such as ordering medication, and providing reminders. Flexibility was needed to enable those who wanted specific features (such as monitoring of environmental triggers or running coaches) to address individual problems or cope with their asthma in particular contexts.
Strengths and limitations
Our study identified a number of features that patients and professionals wanted in an asthma self-management app; however, there are some limitations. First, we only recruited from five practices, though they were demographically diverse and people recruited via social media extended the population beyond these practices. We excluded ‘high risk’ asthma patients and children under 16 years, and females and 26–45 years old were over-represented which limits generalisability. In addition, it is highly likely that participants were those with an interest in using technology for their health.
Second, we had limited flexibility to change the modules and design (button, notification, message box and positions) which may have influenced opinions. However, we explored other potential features with patients in the interviews and the online questionnaire.
Third, we selected a sample size of 15 for the qualitative interviews. Our purposive sampling ensured a range of perspectives, and we achieved data saturation with regard to ‘wanted’ features; however, we may not have encompassed all possible perspectives.
Finally, we could not explore some detailed usage data (such as the average time that participants spent on each feature), though the usage data we used gave an overview of patients’ preference for different features and we asked patients about their usage in interviews and questionnaires to supplement the information.
Interpretations in relation to published literature
Healthcare is one of the core capabilities in the coming 5G Smart City 2.0, which promotes a vision of technology moving from providing standalone tracking and monitoring applications to intelligent applications that connect people and are capable of responding to people’s behaviour in order to solve real-world complex challenges.15–17 Different stakeholders are enthusiastic to engage in this future market.18,19 though they have different perspectives on telehealth.
Clinically, the focus for variable conditions (e.g. asthma) is on action plans, which advise patients to be aware of deterioration in their asthma control, support their decision on adjusting medication or seeking professional help in a timely manner.20,21 Technologically, the emphasis is on easily supported features such as monitoring symptoms, peak flow and treatment usage; providing reminders for logging or medication; and lifestyle monitoring and advice such as activity tracking, weight watching and running coaching.12,13,22,23 Patients, however, are living with asthma and the PRISMS taxonomy highlights that the support needed is much boarder than either the clinical and technological perspectives: for example, facilitation of communication with the practice, behaviour change support for medication adherence and lifestyle changes, customised allergen and pollution warnings, inhaler technique advice, and access to support from social media forums. The challenge is to meld these perspectives such that technology can support the wide-ranging self-management support needed by people living with asthma. Hitherto, in many telehealth design projects, a technology-led approach is used to design digital support for patients. Technology providers offer solutions based on what can be measured or easily delivered (ideally avoiding medical device legislation), 24 but which may or may not solve the problems faced by patients and healthcare service providers.
Conclusion
We need to shift from a paradigm in which apps are built around features that are technologically easy to deliver, to an approach in which theoretically grounded preferred components are identified and apps designed that can deliver to these requirements. An evidence-based taxonomy of potential components of self-management support could stimulate a dialogue between app developers and both users and healthcare services providers, and underpin technological solutions that address the breadth of support that people need to live with asthma.
Supplemental Material
Supplemental_file_A_B_C – Supplemental material for Time to change the paradigm? A mixed method study of the preferred and potential features of an asthma self-management app
Supplemental material, Supplemental_file_A_B_C for Time to change the paradigm? A mixed method study of the preferred and potential features of an asthma self-management app by Chi Yan Hui, Robert Walton, Brian McKinstry and Hilary Pinnock in Health Informatics Journal
Footnotes
Acknowledgements
The authors are grateful to the patient and professional participants for taking part in this study; Asthma UK and the Asthma UK Centre for Applied Research for help on patient recruitment; Richard Parker for his advice on the statistics presentation; and uMotif Limited for providing app configuration services.
Author contributions
C.Y.H., R.W., B.M. and H.P. designed the study. C.Y.H. undertook the data collection and synthesised the data with H.P. R.P. was the statistical advisor. H.P. is the study guarantor. C.Y.H. with H.P. wrote the initial draft of the manuscript. All authors contributed to the writing of the article and reviewed the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: C.Y.H. is funded by a PhD studentship from the Chief Scientist Office (Scotland; AUKCAR/14/01). This work is carried out with the support of the Asthma UK Centre for Applied Research (AUK-AC-2012-01). The views expressed in this publication are those of the authors and not necessarily those of the Chief Scientist Office (Scotland).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.