
Abstract
Keywords
Introduction
The home-based health monitoring system (HHMS) has recently undergone widescale development, aiming to assist individuals in managing health conditions and to enable remote monitoring, 1 such as physical activity, 2 mental functions, 3 and physiological signals. 4 HHMSs use the Internet of Things (IoT) and communication technologies to measure and track individuals’ health data through various devices. For example, fitness trackers (e.g., Fitbit) monitor physical activity and caloric expenditure; smartwatches (e.g., Apple Watch, Garmin Watch) track metrics such as heart rate and sleep patterns; smart scales measure weight and body composition; and blood pressure monitors track cardiovascular health. 5 HHMSs can also use ambient sensors to collect and analyze behavioral data, identify potential health risks, and provide health recommendations to enhance home health management. 6 These systems empower individuals to make positive health behavioral changes. Despite these benefits, however, new HHMSs are not always widely accepted and adopted by end users, their families, or caregivers. 7 Deloitte found that while 28% of individuals use remote health monitoring technologies, regular usage is much lower. 8 This may be attributed to the insufficient embodied connection between the technology and the user’s body. For instance, while current technologies focus on the accuracy of collected health data, they may fail to effectively connect with how users perceive and interpret their own physical sensations and health status. The feedback mechanisms for health information tend to be relatively simple, which may limit their ability to fully leverage the role of physical sensation (e.g., sensory feedback and somatic sensation) in enhancing individuals’ health cognition and behavior. Furthermore, adaptation to users’ daily contexts, such as home settings or routine activity habits, remains limited. This may affect the personalization and contextuality of health suggestions provided by the HHMS. 2 Therefore, these embodied factors may impact usability perceptions and long-term motivation for using HHMSs, which need to be determined to promote successful engagement among different user groups.
Research on individuals’ acceptance behaviors toward HHMSs has predominantly relied on the technology acceptance model (TAM) and the unified theory of acceptance and use of technology (UTAUT) model, 9 which focus on external factors such as perceived usefulness and ease of use. However, cognition is situated and embodied in the physical environment rather than distinct from it. 10 Individuals’ attitudes and decisions are influenced by bodily experiences, physical activity, and environmental contexts. 11 Recent studies have highlighted how health monitoring technologies can transform individuals’ understanding of their bodies and increase awareness. 12 Hence, the TAM and UTAUT models are limited in their ability to capture the dynamics of body, cognition, and technology within HHMSs. For example, physical feedback from HHMSs directly engages the user’s sensory and motor systems: a vibration or notification about a high heart rate can trigger a cognitive response such as concern or conscious behavioral change. 13 Therefore, users’ adoption depends not only on perceived usefulness but also on the integration of the technology with the user’s bodily and cognitive processes. To better understand users’ adoption behaviors, it is essential to explore how interactions between the body, cognition, and environment influence HHMS adoption. Bridging this research gap will deepen our insights into the factors driving user acceptance and inform the design and implementation of more effective HHMSs.
Embodied cognition, an interdisciplinary theory, explores how cognitive processes are grounded in bodily experiences of the physical environment. It emphasizes the roles of sensory experiences, motor actions, and body–environment interactions in shaping cognition.14,15 Embodied experience, based on this theory, helps us understand how physical interactions with technology are crucial determinants of cognitive processes and behavior. 16 Users’ engagement with technology through physical interactions and sensory feedback influences their perception, understanding, and overall experience of the technology. 17 For example, when a smartwatch detects an elevated heart rate during a stressful work meeting, it can deliver a distinct pattern of tactile vibrations against the user’s wrist, creating an immediate, private, and direct alert. The device then analyzes contextual data (e.g., location, calendar events, previous patterns) to distinguish between exercise-related versus stress-related heart rate increases. It may guide the user through a brief breathing exercise using subtle haptic rhythms that physically entrain their breathing to a calmer pattern. Compared to visual-based displays, the feedback loop of measurement, information, and guidance creates an embodied experience, demonstrating how health technologies foster meaningful interactions through bodily engagement rather than abstract data. This understanding can inform strategies to better integrate embodied experiences into the design and improvement of HHMSs.
Based on the traditional TAM, this study acknowledges the embodied nature of human-technology interactions and making contributions to health informatics. Drawing on the UTAUT model, we investigate HHMS adoption behavior by developing a theoretical framework that incorporates embodied experience characteristics (i.e., perceived body awareness, contextual adaptation, sensorimotor feedback). This approach extends traditional technology acceptance frameworks by integrating embodied cognition theory, providing a novel perspective for understanding interactions with health technology. Our model empirically validates how embodied experiences influence HHMS adoption, offering quantifiable insights into previously underexplored dimensions of health technology adoption. By examining gender and age as potential moderators, we deliver evidence-based design guidelines for health informatics practitioners to develop more intuitive monitoring systems that align with users’ natural bodily experiences. This research advances understanding of how health informatics systems can better integrate with physical experiences and contextual needs, potentially improving long-term adherence to health monitoring.
Research hypotheses development
Drawing on embodied cognition theory and the UTAUT model, we developed a research model with 12 hypotheses to investigate HHMS adoption behavior (Figure 1). Proposed research model depicting new relationships as green lines and original UTAUT relationships as blue lines.
Behavioral intention and performance expectancy
The UTAUT model has traditionally defined technology acceptance in work-related settings through specific task-related outcome expectations. Behavioral intention refers to users’ intent to use technology in the future. 18 It is a widely used and reliable predictor of actual usage behavior in technology acceptance research.19,20 Consistent with prior studies, we used behavioral intention as a proxy for technology acceptance in health technology contexts.21,22 Performance expectancy, defined as the belief that a particular system or activity will lead to improved performance or beneficial outcomes, is a key component of technology acceptance. 23 Drawing on relevant research,24–26 we redefined performance expectancy for HHMSs as the degree to which users believe that the system can enhance their efficiency in accessing health information. Thus, we hypothesized that:
Performance expectancy has a significant positive effect on behavioral intention.
Effort expectancy
Effort expectancy refers to users’ perceptions of technology’s ease or difficult of use. For HHMSs, effort expectancy describes the perceived ease of use, with simpler systems being more likely to be adopted. In other words, the easier users perceive the HHMS to be in terms of obtaining health information, the more likely they will intend to use it. We hypothesized that:
Effort expectancy has a significant positive effect on behavioral intention.
Facilitating conditions
Facilitating conditions, defined as the availability of resources and facilities required for technology adoption, was redefined in the context of HHMSs to include training, technical assistance, and access to necessary equipment or software for effective health monitoring. We hypothesized that:
Facilitating conditions have a significant positive effect on behavioral intention.
Social influence
Social influence was redefined as the impact of others’ (e.g., friends, family, social networks) opinions and recommendations on the HHMS acceptance and use. We hypothesized that:
Social influence has a significant positive effect on behavioral intention.
Perceived body awareness
Perceived body awareness refers to users’ conscious recognition, perception, and understanding of their bodies (e.g., position, shape, size, movement, sensations). 27 It involves deep interactions between interoceptive and proprioceptive sensations, reflecting both internal and external bodily experiences and interpretations. 28 Within the UTAUT model, perceived body awareness may serve as a crucial determinant of users’ expectations, efforts, resource utilization, social influence, and behavioral intentions. In the context of HHMSs, increased awareness of one’s physical state through system use can enhance performance expectancy by enabling users to recognize the system’s utility in health monitoring and management. Improved perception and interpretation of bodily signal allow users to better evaluate how the system enhances the efficiency and effectiveness of health monitoring. 29 As users become more aware of their physical states through the system, they may also find it easier to interpret and respond to feedback, thereby reducing the perceived effort required to use the system. 30 This enhanced body–system interaction could positively influence effort expectancy. We hypothesized that:
Perceived body awareness has a significant positive effect on performance expectancy. As users gain insights into their physical condition and health status through the system, the perceived burden and difficulty associated with usage diminish. This enhanced understanding boosts users’ confidence in the use of system. We hypothesized that:
Perceived body awareness has a significant positive effect on effort expectancy. By increasing awareness of their physical condition and health status, users are also more likely to perceive that the system’s favorable conditions or resources facilitate task performance or goal attainment. We hypothesized that:
Perceived body awareness has a significant positive effect on facilitating conditions. Increased aware of their physical condition and health status may increase users’ receptivity to social norms and expectations, which can influence their health cognition and behaviors. We hypothesized that:
Perceived body awareness has a significant positive effect on social influence. With this improved understanding of physical condition and health status, users are more likely to express a willingness to continue using the system in the future. We hypothesized that:
Perceived body awareness has a significant positive effect on behavioral intention.
Perceived contextual adaptation
Perceived contextual adaptation refers to the system’s ability to tailor its functionality, features, and recommendations to users’ unique context. The HHMS considers an individual’s health status, lifestyle, preferences, and environmental factors (e.g., home environment, daily routines) to provide personalized, effective feedback and recommendations. 15 We hypothesized that:
Perceived contextual adaptation has a significant positive effect on perceived body awareness.
Perceived sensorimotor feedback
Sensorimotor feedback involves the integration of sensory perception with motor activities. 31 When we perform physical activities, we receive sensorimotor feedback, such as tactile or proprioceptive cues, 32 which helps us develop an embodied understanding of our body’s position, capabilities, and boundaries. 33 In the context of HHMSs, perceived sensorimotor feedback is defined as users’ perceptions of sensory information and motor responses while interacting with the system. 34 For instance, smartwatches provide haptic vibrations to alert users of elevated heart rates during exercise, fitness trackers respond to walking movements with visual step count animations, and blood pressure monitors offer tactile feedback (cuff pressure) and auditory signals. 28 These multimodal feedback mechanisms create a direct sensory connection between the user’s physical actions and the system’s response, thereby enhancing the embodied experience. We hypothesized that:
Perceived sensorimotor feedback has a significant positive effect on perceived body awareness.
Moderating roles of gender and age
Consistently, studies across various technology domains have shown that technology acceptance varies based on users’ demographics, such as gender and age.35,36 These demographic characteristics also act as moderators technology adoption.37,38 According to this, we hypothesized that these demographic factors moderate the relationships mentioned above.
Methods
Participants
Data were collected from users with diverse sociodemographic backgrounds through a Chinese professional web-based platform (https://www.wjx.cn/), which has been widely utilized in academic research.39,40 We employed a purposive sampling strategy, where the survey was distributed via the platform’s sample service to reach potential participants matching our eligibility criteria. Eligible participants included adults proficient in written Chinese who were potential HHMS users. These included individuals interested in health monitoring, patients with chronic conditions requiring regular health tracking, fitness enthusiasts monitoring physical activities, and older adults (or their caregivers) managing health status at home. The platform screened eligible respondents from its sample library using an automated delivery mechanism. To ensure data quality and validity, this platform provided real-time monitoring and anti-cheating functions during data collection. The study received approval from our institution’s Ethics Committee.
Demographics of participants (n = 459).

Measurement items
The survey began with a brief description of the HHMS (Appendix Table A). Respondents were asked to rate various measures representing constructs on a 5-point Likert scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). The survey was developed by adapting validated measurement scales grounded in the theoretical foundation of embodied cognition. To ensure content validity and comprehensibility, the questionnaire was pilot-tested with 15 representatives of the target user group. Their feedback was used to refine the wording and structure of the survey items. Additionally, a survey design expert was consulted to further guarantee the quality. The final version of the survey was then administered to participants in the main study. Participants were assured that no personal information would be gathered. Appendix Table B provides a detailed summary of the constructs, items, and relevant references.
Data analysis
To explore path relationships among variables, we employed partial least squares structural equation modeling (PLS-SEM) 43 using SmartPLS 4.0 (SmartPLS GmbH, Boenningstedt, Germany). To ensure the robustness of the analysis, we adhered to established criteria from previous research. 44 Specifically, internal consistency reliability was measured using Cronbach’s alpha and composite reliability (acceptable threshold = 0.7). Convergent validity was evaluated through factor loadings (with a minimum threshold > 0.7 for each item) and average variance extracted (AVE, > 0.5 for each construct). These evaluations confirmed plausibility of the measurement model before proceeding to analyze the structural relationships among variables.
Results
Measurement model assessment
Mean, SDs, factor loadings, reliability, and convergent validity of the constructs.

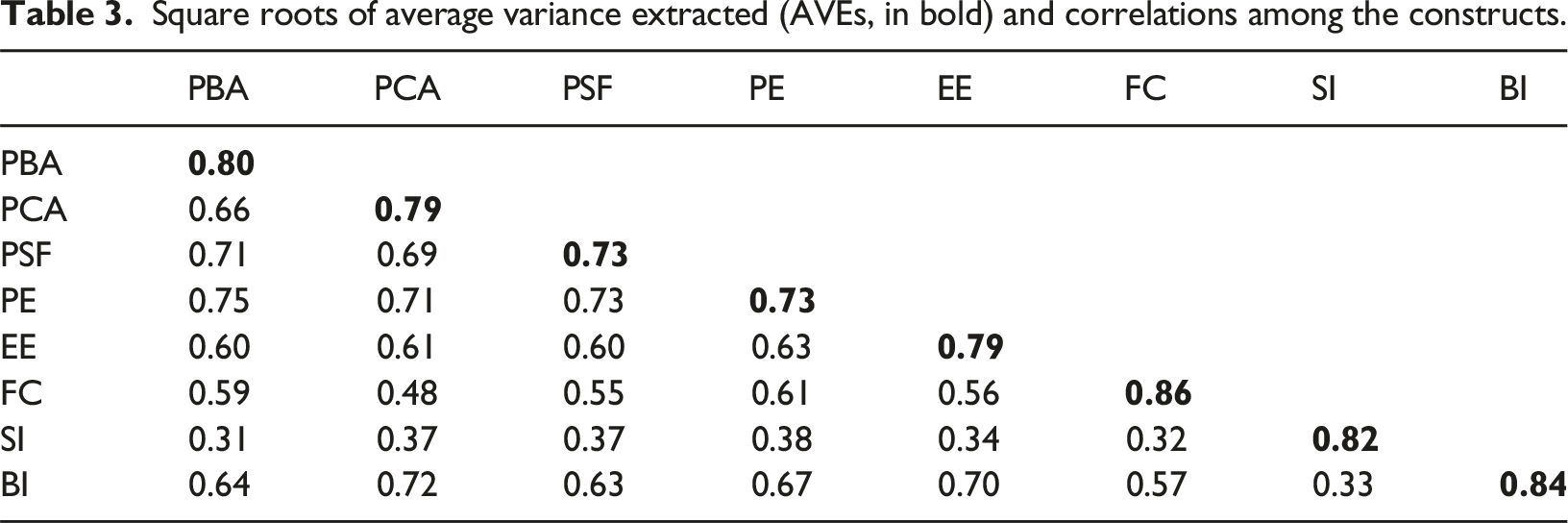
Square roots of average variance extracted (AVEs, in bold) and correlations among the constructs.
Hypothesis testing
Path coefficients and bootstrapping results.
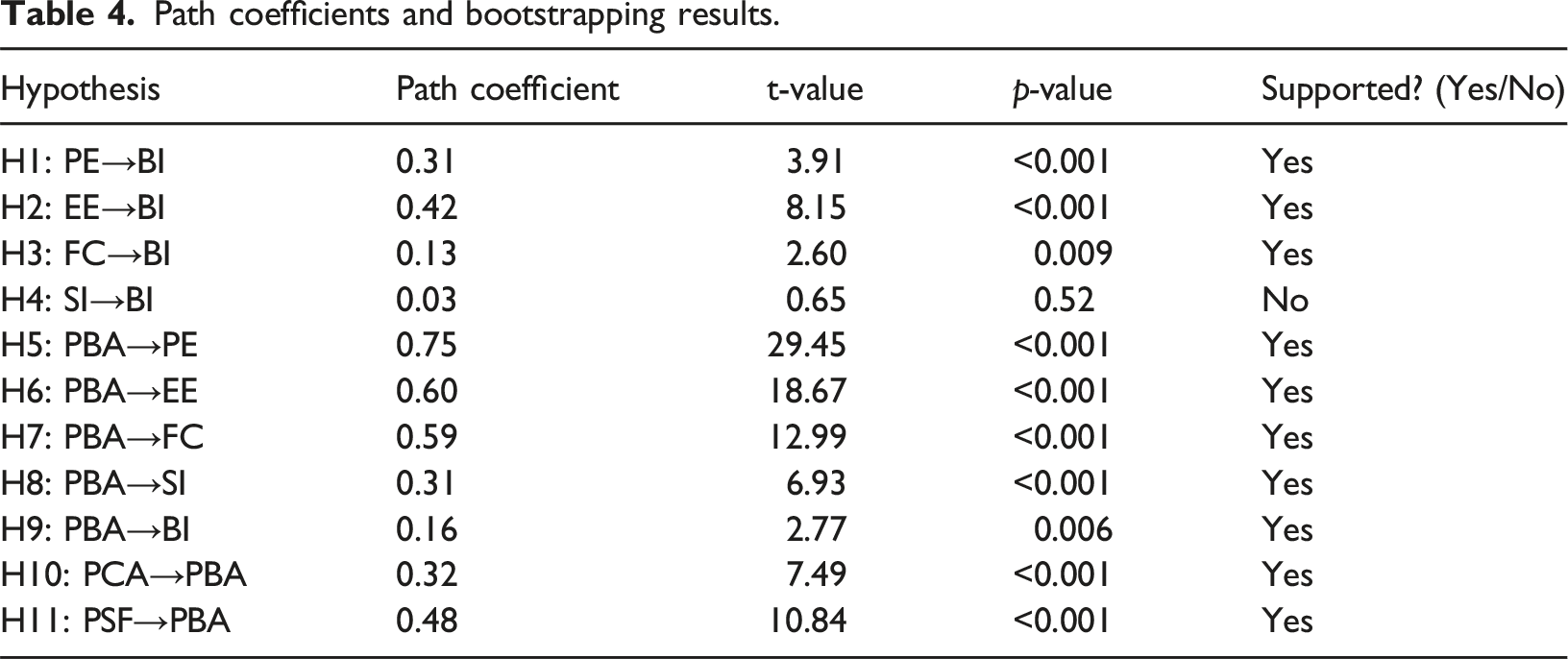
Figure 2 depicts the research model, exploring the factors influencing users’ HHMS acceptance. The proposed model accounted for 59.7% of variance in behavioral intention. Structural model measurement results (***p < 0.001; **p < 0.01; *p < 0.05).
Perceived contextual adaptation and sensorimotor feedback together explained 55.3% of the variance in perceived body awareness. Perceived body awareness, in turn, explained 55.8%, 36.5%, 35.0%, and 9.8% of the variance in performance expectancy, effort expectancy, facilitating conditions, and social influence, respectively.
The direct, indirect, and total effects of predictors on behavioral intention.

***p < 0.001; **p < 0.01.
Multi-group analysis
Multi-group analysis by gender (Male = 219; Female = 240).
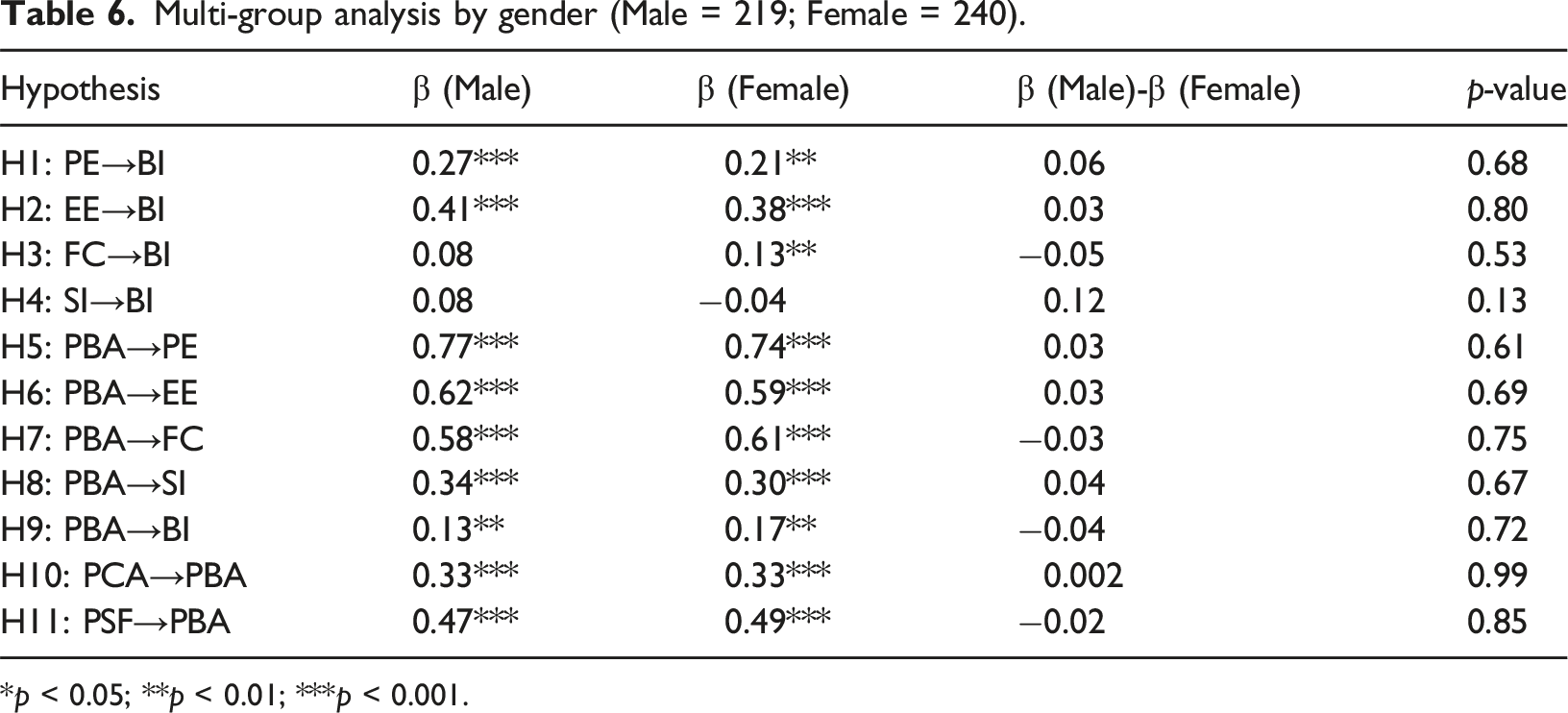
*p < 0.05; **p < 0.01; ***p < 0.001.
Multi-group analysis by age (Young adult = 182; Older adult = 277).

*p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
Main findings and theoretical implications
This research expands the UTAUT model by incorporating the internal relationships among characteristics of embodied experience in the context of HHMSs. The theoretical implications are four-fold. First, perceived body awareness is identified as a significant direct and indirect determinant of key UTAUT constructs and behavioral intention regarding HHMS adoption. This consistents with previous findings on the embodied nature of human–technology interaction.12,45 Users’ ability to interpret and understand their bodily signals is foundational for technology acceptance. When HHMSs help increase users’ attention to their physiological states (e.g., heart rate variability, sleep patterns, physical activity levels), users may be more willing to adopt such technologies. Second, this study highlights the crucial role of sensorimotor feedback in shaping users’ HHMS adoption. By emphasizing the importance of physical feedback, the research extends the UTAUT model, showing how sensorimotor feedback creates a direct sensory connection between users’ actions and system responses. This connection shapes users’ understanding and acceptance of the technology. These findings are consistent with Ziemke’s 34 work on embodied interaction, demonstrating how multimodal feedback mechanisms (i.e., visual, auditory, haptic feedback) in health monitoring systems create an integrated physical–digital experience. Third, perceived contextual adaptation compensates for external dynamics in the UTAUT model and highlights the importance of integrating HHMSs into users’ daily lives and environments. 9 Rather than immediate acceptance, technology adoption is gradually formed through continuous situational interactions. System adaptability to environmental changes may affect users’ long-term technology acceptance. 46 For instance, the adjustment of monitoring thresholds, feedback methods, and suggestion content according to the user’s specific context (e.g., different rooms, daily activities) may increase the usefulness and ease of use of the HHMS.
Finally, age and gender did not influence the relationships between antecedent factors and behavioral intention. In contrast to Escobar-Rodríguez and Grávalos-Gastaminza, 47 who highlighted age and gender as moderators within an expanded TAM, our findings did not indicate that gender affected the strengths of the hypothesized relationships. The underlying reasons may be due to the unique context of health monitoring. Unlike general consumer technologies, HHMSs are focused on addressing universal health needs, which may traditionally observed gender differences in technology adoption. 35 Evolving changes in gender roles and technology access may have reduced documented gender gaps in technology acceptance and digital health literacy. 20 These findings suggest that current HHMSs are general-purpose functions rather than gender-specific solutions, and further research is needed to investigate the need for gender-specific HHMSs.
However, we found that the correlation between social influence and behavioral intention was more significant among older versus young adults. Multigroup analysis revealed that while the relationship between social influence and behavioral intention might not have been significant across the entire sample, the effect was pronounced among older adults. This finding is consistent with previous research showing that older adults’ decisions to accept technology are influenced by their social networks, such as family, peers, and professional caregivers. 48 Our findings also align with Chen and Chan’s 49 study, which emphasized that the acceptance of gerontechnology among elderly Hong Kong Chinese is significantly impacted by perceived social support and self-efficacy. This age-specific effect may be attributed to older adults’ greater reliance on trusted social networks when making health-related decisions. 22 For instance, older adults are more likely to adopt health-related technologies when they receive hands-on guidance from peers who have successfully used these tools or when family members provide reassurance and practical advice with data privacy concerns or usability challenges. 50 These findings suggest that different age groups may have varying levels of experience, knowledge, and preferences that influence interactions with the variables in a study. Older adults’ adoption of technology may be greatly influenced by their social environment, which includes the opinions and perspectives of their family and peers.
Practical implications
This research offers important practical implications for the design and deployment of HHMSs. By integrating embodied experience into the UTAUT model, researchers and practitioners can enhance the adoption of HHMSs across different age groups. First, body awareness generally declines with age due to sensorimotor and cognitive changes. 51 For older adults, this declines often show dependency tendencies and a need for encouragement to actively manage their health. HHMSs should focus on addressing changes in interoception and body representation to stimulate engagement, while also respecting cognitive capacity limitations. For middle-aged and younger adults, they have greater needs for mental health promotion. HHMSs can assist these users by connecting body awareness with mental states, such as linking collected health data to daily activities and environmental conditions to regulate their psychological state through body signal monitoring. Second, to enhance perceived sensorimotor feedback, HHMSs should accommodate age-related changes in sensorimotor processing. 51 Older adults experience sensory declines that fundamentally alter the way they interact with technology. To address this, HHMSs should incorporate sensory compensation design principles. For instance, multi-modal interactions or health-related feedback could compensate for diminished vision and hearing, such as providing health reminders through haptic feedback tailored to varying levels of haptic sensitivity. 52 For younger users, whose sensorimotor systems typically process information more efficiently, subtle vibration patterns and gesture controls can create a more seamless extension of their embodied experience with technology.13,53 Third, regarding perceived contextual adaptation, HHMSs should tailored for different needs across age groups. For older adults, who are more influenced by social influence, the embodied experience is often socially situated within family care networks. HHMSs could facilitate these social connections by allowing family members to participate in monitoring while respecting autonomy. Middle-aged and younger users often involve balancing multiple responsibilities, may benefit from systems that adapt to their dynamic lifestyles. So, HHMSs should recgnize contextual transitions between work and home environments, with adaptive monitoring thresholds during different activities. 54 These age-specific design guidelines may lead to create more engaging and effective health monitoring experiences and improve users’ adoption rates and health outcomes.
Limitations and future work
Although this study offers valuable insights into the factors influencing the adoption of HHMSs, it has some limitations. First, the cross-sectional research design captured behavioral intention at a single point in time, which may have missed important temporal dynamics in HHMS adoption. Future research should use longitudinal designs to track how users’ intentions and actual usage behaviors evolve over time, particularly during the crucial periods of initial adoption, habituation, and long-term engagement. Second, limitations in participant recruitment emerged. Participants aged 40–54 were underrepresented (4.3%) in our sample. This group typically represents working professionals who may use HHMSs for managing work-related health concerns but may be less available to participate in for voluntary studies. Future studies should implement targeted sampling strategies to ensure better representation of this age group. Additionally, although older adults are the primary target group for HHMSs, the number of older adult participants in the sample needed to be increased, especially those who are solitary and might have distinct needs and adoption barriers. Lastly, the high proportion of participants living with partners (83.0%) may have influenced our findings, particularly regarding social influence factors. Individuals living alone may experience somewhat different patterns of technology adoption (e.g., remote support or motivation) compared to those with cohabiting partners who can provide immediate support and feedback. Future studies should explore how different living arrangements shape adoption patterns.
Conclusion
This study integrated embodied cognition theory into the UTAUT model to explore the key factors influencing the adoption of HHMSs. Our findings highlight the importance of considering individuals’ cognition, physical capabilities, and environmental context in enhancing HHMS adoption, offering health informatics researchers measurable constructs for future investigations. Empirical findings of our research model revealed that characteristics of embodied experience, such as perceived body awareness, perceived contextual adaptation, and perceived sensorimotor feedback, are key determinants of performance expectancy, effort expectancy, facilitating conditions, social influence, and behavioral intention. Furthermore, we present actionable design implications for practitioners developing HHMSs that better integrate with users’ embodied experiences. By bridging theoretical frameworks with practical applications, this research provides a foundation for more intuitive, effective, and user-centered health monitoring systems.
Supplemental Material
Supplemental Material - Integrating embodied cognition with the UTAUT model to investigate factors influencing the adoption of home-based health monitoring systems
Supplemental Material for Integrating embodied cognition with the UTAUT model to investigate factors influencing the adoption of home-based health monitoring systems by Zhen Zhao, Kaifeng Liu, She Lyu, Stephen Jia Wang, Yun Hei Chak, and Hailiang Wang in Health Informatics Journal
Footnotes
Ethical consideration
The study protocol was approved by the Institutional Review Board of Hong Kong Polytechnic University (approval number HSEARS20240430001).
Consent to participate
All participants gave written informed consent.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Health and Medical Research Fund, the Health Bureau, Hong Kong [no. 20211201], the Hong Kong Polytechnic University grants [no. P0049595, P0045769, and P0045577], and the National Natural Science Foundation of China [no. 72104176].
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
Description of the HHMS.
Description of the HHMS
The home-based health monitoring system (HHMS) is a comprehensive technology that enables remote health monitoring within home environments. Through integrated sensing technologies, it creates an intelligent environment that continuously monitors and evaluates users’ health status through multiple dimensions, including 1) wearable devices such as smartwatches that track vital signs, physical activity, and sleep patterns; 2) non-wearable monitoring equipment like blood pressure monitors and glucose meters that connect to mobile applications; and 3) ambient monitoring sensors that placed throughout the home to detect falls, daily activity patterns. With users’ consent, the HHMS can securely transmit collected health data to authorized parties such as family members, caregivers, or healthcare providers, thereby facilitating more effective health management.
Measurement items.
Constructs
Items
Perceived body
Awareness55,56 (PBA)PBA1 by using the HHMS, I can increase my perception of physiological changes in my body.
PBA2 by using the HHMS, I can increase my awareness of my health status.
PBA3 using the HHMS allows me to pay more attention to my body and its needs.
Perceived contextual
Adaptation10,15 (PCA)PCA1 I feel comfortable using the HHMS in my surrounding environments.
PCA2 I feel comfortable using the HHMS in my daily activities.
PCA3 it would be more trustworthy and useful if the HHMS provided health advice based on my current environment or activities.
Perceived sensorimotor
Feedback33,34 (PSF)PSF1 it would enhance my perception of my health if the HHMS had visual feedback (i.e., graphs, charts, or animations).
PSF2 it would enhance my perception of my health if the HHMS had auditory feedback (i.e., auditory cues or alarms).
PSF3 it would enhance my perception of my health if the HHMS had haptic feedback (i.e., vibration prompts).
PSF4 if the HHMS could be interacted with through body movements or gestures, I think it would enhance my awareness of my own health.
Performance expectancy
18
(PE)
PE1 I feel the HHMS is useful in collecting health information.
PE2 using the HHMS enables me to obtain health information quickly.
PE3 using the HHMS provides me with the health information that I need.
PE4 if I use the HHMS, I will increase my chances of managing my health.
Effort expectancy
18
(EE)
EE1 I can use the HHMS quickly and easily.
EE2 I can skillfully use the HHMS and its provided health information.
EE3 I find the HHMS easy to use.
EE4 I think learning to operate the IHMS is easy for me.
Facilitating conditions
18
(FC)
FC1 I have the necessary resources to use the HHMS.
FC2 I have the necessary knowledge to use the HHMS.
FC3 if I have trouble using the system, someone will help me.
Social influence
18
(SI)
SI1 My family influences my decision to use the HHMS.
SI2 My friends influence my decision to use the HHMS.
SI3 people who are important to me influence my decision to use the HHMS.
Behavioral intention
18
(BI)
BI1 in the future, I will often use the HHMS to manage my health.
BI2 I predict I will use the HHMS to manage my health soon.
BI3 I can develop a habit to use the HHMS soon.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.