
Abstract
Introduction
Low back pain (LBP) is the leading cause of years lived with disability (YLDs) globally 1 and its prevalence is increasing due to expanding and ageing populations. 2 In 2020, LBP was estimated to affect 619 million people worldwide 2 and is projected to increase to over 800 million people by 2050. 2 LBP is a long-lasting condition with etiology attributed to physical, psychological, and social factors, which are complex and typically difficult to manage. 3 Empowering individuals to manage these aspects of their pain and disability will decrease reliance on healthcare systems.4,5 As the associated disability and costs of LBP increase worldwide, 3 the Lancet series on LBP,3,6,7 a three-part review of the increasing disability associated with LBP globally and suggestions for future LBP care, strongly recommends LBP management focus on the use of self-management strategies.3,7
Sleep disturbance is commonly associated with chronic illness, leading to poor daytime function, decreased quality of life, and increased use of healthcare.8,9 Sleep disturbance includes problems such as increased sleep latency, poor quality sleep, frequent night wakings or early morning wakings and poor sleep efficiency. 10 Up to two-thirds of adults who have chronic LBP report sleep disturbance such as difficulty falling asleep, difficulty staying asleep, waking too early, night-time wakefulness or daytime sleepiness and an increase of 1 point in LBP intensity on waking (measured on a 0-10 numeric rating scale [NRS]), has been found to be associated with decreased subsequent sleep quality of 0.5 points (measured on a 0-10 NRS), delayed sleep onset latency of >2 min, and wake after sleep onset of 2 – 6 min. 11 While studies suggest a bi-directional relationship between LBP and sleep disturbance,12,13 research shows that sleep disturbance has greater impacts on LBP coping 14 and pain intensity15,16 than the opposite relationship. Sleep disturbance has also been shown to mediate the relationship between common mental disorders and LBP. 17
Cognitive Behaviour Therapy for Insomnia (CBT-I), which is the first-line treatment recommendation for insomnia,18–20 includes behavioural interventions such as sleep hygiene, stimulus control, relaxation, and sleep restriction. 19 These interventions aim to improve sleep drive, sleep-related behaviours, and sleep-related anxiety 19 and have both short-term and long-term benefits for adults with chronic insomnia. 21 While CBT-I is effective for addressing chronic insomnia and related sleep difficulties, other sleep disorders, such as sleep apnoea or restless legs syndrome may require adjunctive treatments,22,23 however there is promising evidence for CBT-I improving sleep and pain for individuals with LBP.24,25
According to the World Health Organization, mHealth interventions (mobile device health interventions) 26 are likely to be effective and efficient methods of health promotion due to the widespread use of mobile phones globally. 27 MHealth applications (apps) for self-management of LBP,28–30 chronic pain,31,32 and sleep 33 have been developed with varying content and efficacy. A recent systematic review found that mHealth apps utilizing multicomponent interventions, such as those that aimed to improve diet, physical activity, and sedentary behavior, are more effective in creating behavior change than stand-alone interventions. 34 However, a systematic review of holistic mHealth interventions published in 2023 35 acknowledges that the combinations of strategies and interventions that are most effective is unknown and requires further research. Further to this, sleep therapy has rarely been combined with other interventions (such as physical activity or diet) in mHealth apps designed to manage multiple behaviours. 36
MySleepSolutions was designed to address this gap in mHealth. It is a 4-week sleep retraining module based on CBT-I principles and has been created as part of the design process of an exercise and lifestyle self-management mHealth app for people with chronic LBP called My Back Exercise. This report aims to describe the design process of the app module, MySleepSolutions, to ensure transparency regarding the theoretical basis and the evidence behind the content.
Methods
The design and development process utilized for MySleepSolutions followed a high-level framework developed by Aji et al. 18 which provides the structure of the design and development, and was informed by the intervention mapping framework 37 and the Centre for eHealth research roadmap 38 which is an iterative, and cyclic framework.37,38 To facilitate the development of effective, evidence-based apps for sleep disturbance, the Aji and colleagues’ framework 18 was developed to guide researchers and app developers through the process from app conception to release and evaluation. This framework aims to improve the use of best practice designs, implementation metrics (such as privacy and security concerns as well as validated sleep measures), and appropriate evaluation of efficacy. 18
This framework is divided into four phases. Phase one (concept development), two (therapeutic approach, design approach and app features/functionality), three (implementation metrics, security, and regulations) and four (clinical outcomes in end users). Usability, acceptability, adherence, and engagement analyses are currently underway, as well as a randomized controlled trial (RCT) evaluating the effectiveness of the My Back Exercise app in people with chronic LBP. Ethics approval was attained before testing and evaluation from The University of Sydney Human Research Ethics Committee (2023/772). Therefore, implementation metrics in phase three will be described in detail elsewhere.
The My Back Exercise app is a novel, automated, progressive, self-directed, six-week exercise intervention for people with chronic LBP. It has been designed to harness the benefits of digital and mobile health technology, enabling people with chronic LBP to embrace lifestyle change and self-manage their condition. The app is designed to improve patient-specific function with a dynamic, progressive, goal-oriented exercise program which is based on the users’ responses to the patient-specific functional scale.
39
Users are supported by personalized, educational push notifications and optional diet advice as well as the 4-week MySleepSolutions sleep retraining module (Figure 1). The development of the My Back Exercise app will be published following the completion of usability testing. MySleepSolutions module in the My Back Exercise App.
Phase one – Concept development
Concept development occurred between October and December 2022. The multidisciplinary team involved in each phase of the development of MySleepSolutions was led by an experienced clinician and PhD student and consisted of 11 researchers, four clinicians, a sleep specialist, and the app developers, all with extensive experience in LBP management, research, or software development. The first meeting occurred in October 2022 and involved discussing the findings of previous work conducted by the research group regarding what consumers deem important for an app designed to improve sleep for people with LBP. This preliminary research employed a nominal group technique in a focus group involving seven musculoskeletal researchers, one clinician, two sleep researchers and one consumer advocate. The nominal group technique involves exploring issues, generating ideas and problem solving in a structed meeting process. 40 A mixed methods analysis was then conducted to rank the ideas that were generated and offer contextual insights. 41
When designing mHealth apps, a user-centered approach, which addresses the preferences, needs and values of the user, is considered to be the gold standard 42 to ensure user satisfaction and engagement. 43 A design that fails to address the preferences, needs and values of people with LBP, 42 is unlikely to effectively promote self-management. 42 For this reason, both people with LBP and clinicians were represented in the detailed data collected during the concept development 41 and planning phase, the iterative process of drafting and designing MySleepSolutions and its subsequent testing and evaluating phases.
Previous research was utilized to further inform the content of the sleep module from the user’s perspective.44,45 For example, users of mHealth apps for sleep disturbance report valuing audio features, signs of progress and recommendations for helpful websites as well as relevant informative content. 44 Users of mHealth apps for LBP report valuing knowledge and education, choice regarding engagement with the app, personalization of the content 46 and clear self-management strategies. 29 Expert advice (CG) was provided regarding CBT-I-specific information, as well as app development (CJ). The initial concept was then drafted and edited by the development team at eight subsequent meetings.
Phase two – Therapeutic approach, design approach and app features/functionality
The therapeutic and design approaches, as well as the sleep module features and functionality, were developed over the course of several workshops and regular weekly meetings held between December 2022 and December 2023. The team consisted of the same researchers, clinicians, sleep specialists and app developers who were involved in the concept development and the development of the My Back Exercise app. At each meeting, content was discussed, reviewed, and refined in an iterative process, using sketches, storyboards and mock-ups, to ensure it was evidence based and met the needs of the user. The multidisciplinary team also used these regular meetings to ensure the user experience and user interface design requirements were met by discussing the use of appropriate colors and text, the role of the avatar and the ease of using the app.
Previous literatures reviews were conducted and published by the research group to identify which traditional sleep approaches are effective 24 and the feasibility of digital approaches 25 for LBP as well as the efficacy of digital CBT. 47 The first meeting was preceded by a further review of the literature to determine the main objectives of the sleep module content. These objectives were discussed by the development team. KR performed the literature review researching the connection between sleep disturbance and LBP, behavior change theories and taxonomy, as well as a review of existing evidence regarding apps for LBP self-management and sleep retraining. These literature searches aimed to understand user needs and preferences and to collate evidence-based recommendations for sleep retraining. In accordance with the framework for developing an app for sleep disturbance, 18 the content was revised and updated in an iterative, cyclic manner, with weekly meetings and ongoing testing throughout 2023.
The first draft of the content was based on available research,48–50 Woolcock Institute of Medical Research 25 flyers on sleep health in adults, sleep myths and expectations, learning better sleep and relaxation strategies for insomnia,51–54 the latest research regarding CBT-I55,56 and expert advice (CG). The content of clinical hints and tips were informed by previous research on consumer preference when receiving text messages for self-managing LBP 57 and cardiovascular events, 58 ensuring messages were positively framed, non-authoritarian, socially and culturally appropriate and practical. 57 App features were designed based on user preferences for sleep apps 44 and LBP apps, 59 while also acknowledging that appealing visual features and interactive content assist understanding for users of all levels of health literacy. 42
CBT-I is a recommended first-line therapy for insomnia,18–20 and is highly effective as an mHealth strategy with evidence-based principles.55,56,60 Based on discussions with sleep research experts and the best available evidence, the components of CBT-I that were included in the 4-week program are: sleep education, sleep hygiene, relaxation training and stimulus control, which are presented in four consecutive weeks.
Sleep restriction is known to be a highly effective component of CBT-I56,61 and, for this reason, was included in the modules. However, people often find it a challenging therapy due to common side effects such as fatigue and sleepiness. 56 The development team was concerned that sleep restriction would negatively impact the exercise component of the My Back Exercise app and the score of 80%, rather than 85%, was therefore chosen as the cut-off point (indicating suboptimal sleep efficiency) for directing users to optional sleep restriction tips.
Phase three – Implementation metrics, security, and regulations
Ethics approval has been granted for assessing implementation metrics (i.e., usability, acceptability, engagement, and adherence). These metrics will be assessed using the system usability scale (SUS), 62 the user version of the Mobile Application Rating Scale (uMARS) 63 and a user satisfaction survey. Data security and privacy are important considerations when designing mHealth apps 18 and as such, a privacy policy was developed in consultation with The University of Sydney legal representatives.
Phase four – Clinical outcomes in end users
As MySleepSolutions is designed to support users of the My Back Exercise app, measurement of clinical outcomes will be minimized to decrease survey fatigue among users. Sleep efficiency will be measured using a standard mathematical algorithm. Users are asked about their average hours of sleep per night as well as their average hours spent in bed per night (time awake and time asleep) in the past fortnight, and a percentage is calculated (
Five questions from the Insomnia Severity Index (ISI) were used to measure insomnia severity in the previous fortnight. 66 The ISI is the gold standard for assessment of insomnia and consists of a 7-item questionnaire which is a reliable (r = 0.74) 66 and valid tool for measuring insomnia severity in clinical populations and research. 66 Users rate the severity of sleep disturbance and its impact on daily functioning. Scores for each question are summed, with total scores ranging from 0 to 20 (for the 5 questions used) where higher scores indicate greater levels of insomnia severity.
Results
The design and implementation process utilized for the development of MySleepSolutions, following the Aji and colleagues framework
18
is presented in Figure 2. Aji et al Framework for the Design Engineering and Clinical Implementation and Evaluation of mHealth Apps for Sleep Disturbance adapted for MySleepSolutions.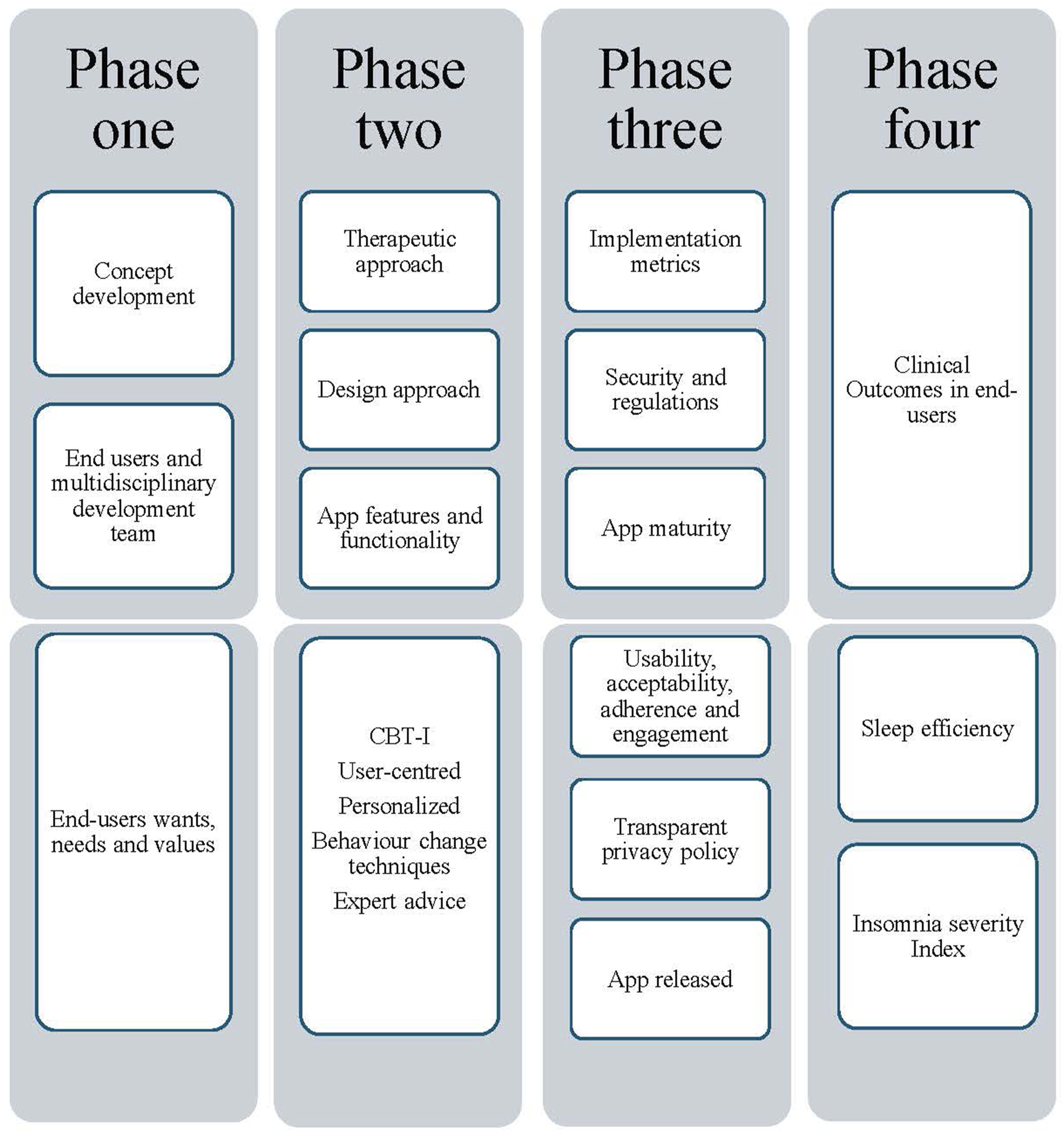
Phase one – Concept development
The MySleepSolutions program was designed to support individuals with LBP who are using the My Back Exercise app. As users of the My Back Exercise app are likely to face challenges such as engagement with exercise and habit change when committing to their exercise program, MySleepSolutions was designed to be a simple and effective adjunct to the exercise program. For this reason, the sleep module is offered to users but is not compulsory, and assessment and follow-up have been kept to a minimum so as not to over-burden users.
Performance objectives, content examples and behavior change techniques utilized in MySleepSolutions.

Phase two - Therapeutic approach
Before commencing the sleep program, the user is asked whether they are interested in learning more about their sleep, how it can impact their LBP and whether they would like to commence the program.
The weekly flow of the program is presented in Figure 3. At the start of each week, the user is presented with four to six phenotypes (Table 2) and is asked to rate how closely each phenotype represents them on a five-point Likert scale. Their weekly program will then be based on the phenotype that most closely represents them. The phenotypes were developed in discussion with clinicians and sleep researchers to engage users with the app content and improve the personalization of their experience. Each phenotype describes, in lay terms, the sleep issues commonly reported by people with LBP, as they relate to the weekly topics, allowing the diversity of sleep issues experienced by people with insomnia
44
to be included. An example of the weekly phenotypes is presented in Figure 4. Example of a weekly program. Phenotype options presented to users each week to guide program content. Examples of the phenotypes presented to the user in week one.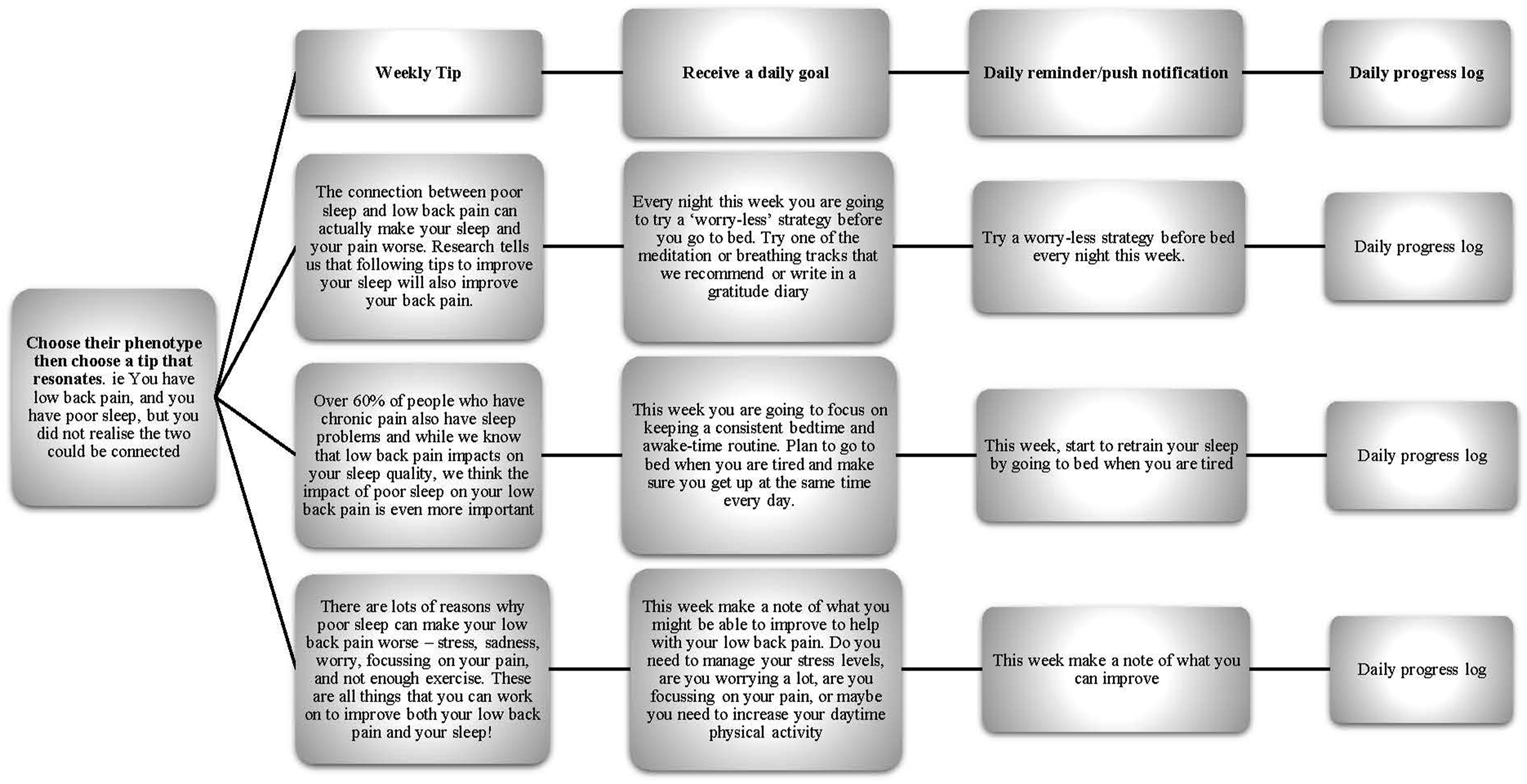


Users will receive an educational tip regarding sleep and/or the sleep-LBP relationship to build an understanding of what constitutes normal sleep patterns in people with and without LBP. They will subsequently be presented with four to six sleep tips that correlate with the phenotype they have selected and will be asked to choose which tip they feel most able to practice that week. This tip is then converted into a daily goal and a short reminder that will be sent as a daily notification to their mobile device. At the end of each day, users can mark off their progress on the progress bar and, at the end of the week, they will be asked to score the effort that they have placed into practicing their daily tip utilizing a simple five-point Likert scale.
The behavior change techniques utilized in the weekly content were based on taxonomy of behavior change techniques proposed by Michie 67 and expanded by Dugas for mHealth. 68 Fourteen techniques were utilized and are presented in Table 1. Weekly content was drafted and repeatedly revised by the authors and research team throughout multiple meetings held between October 2022 and October 2023. Reviews ensured lay terms were used, content was kept brief, and hints and tips were evidence-based. In total 21 phenotypes, 21 hints regarding sleep and 85 tips with corresponding goals were designed for the 4-week program.
Design approach
Design objectives to ensure user-centered content of the sleep module.

ISI: Insomnia severity index; RCT: randomized control trial; BCT: behavior change techniques; PSQI: Pittsburgh Sleep quality Index
Examples of the design objectives used in the app development based on user preferences to ensure user-centered content of the sleep module.
Personalization is regarded as an important feature in app development to increase user engagement. 59 For this reason, users are presented with a variety of tips that match the phenotype they select to represent themselves each week. Enabling users to select their preferred tip was intended to support program personalization, bolster the user’s self-efficacy to make the appropriate change, and assist the fit of the app to their needs, all of which, are important to app users. 59 By selecting the tip to follow, users are also allowed to choose the goal they work towards each week, further improving adherence, engagement, 70 and motivation. 71
App features and functionality
In line with previous research regarding LBP and self-management strategies,
45
MySleepSolutions was designed to provide personalized, clear, and consistent advice. Screenshots of the app are displayed in Figure 5 to detail some of the app features and functionality. Screenshots of example App content in week one of the module.
At the start of the My Back Exercise app, the user selects an avatar who guides them through their sleep program. The avatar is in important component of the user interface and the user experience and provides personalization and gamification to aid behavior change. 68 If they choose meditation or breathing exercises, they receive a voice to match their avatar. The avatar (and, therefore, voice recording) can be changed at any stage of the program to suit the user’s preferences.
The daily progress bar and the weekly question, regarding the user’s perception of their use of the tips to improve their sleep, were designed to allow the user to self-assess their effort rather than their sleep. Visual tracking of progress has been found to improve user engagement in the long term 59 and is a preference of people using sleep apps. 44
Recent research found that daily use of a mindfulness and meditation app was associated with decreased fatigue, daytime sleepiness, and pre-sleep cognitive arousal in adults with sleep disturbance. 72 Audio features have also been found to be important in sleep mHealth apps. 44
Meditation and breathing tracks were therefore recorded by the research team to introduce users to simple meditation and breathing techniques.
Examples of sleep education content, sleep tips and daily goals.

Phase three – Implementation metrics, security, and regulations
After extensive testing, the My Back Exercise app has been released and is available for download on the Google Play and Apple App store. The privacy policy has been made publicly available on the My Back Exercise app to ensure transparency of privacy and security protocols such as which health data is collected and where it is stored. Ten experts, stakeholders and consumers will provide important information on the user experience and the user interface via usability, acceptability, adherence, and engagement analyses which are currently underway and will be reported on completion.
Phase four – Clinical outcomes in end-users
The modified version of the ISI and the sleep efficiency calculation have been integrated into the onboarding process of MySleepSolutions56,65 and are re-calculated at the end of the 4-week program. The sleep efficiency score is used to guide the sleep program, whereas the modified ISI is used to calculate improvement in insomnia following the 4-week program. Where no improvement is seen, or clinical insomnia is still evident, the app provides advice to seek professional help from a sleep specialist or a psychologist.
Discussion
This study aimed to provide a detailed description of the process of designing and building a sleep education module, embedded in a lifestyle self-management app, for people with chronic LBP. It describes the development of MySleepSolutions, utilizing a framework that was created specifically for mHealth apps for sleep disturbance 18 and was informed by the intervention mapping framework 37 and the Centre for eHealth research roadmap. 38 This detailed description utilizes a best practice design approach ensuring transparency of the design process and the evidence-base behind the content.
MHealth has the potential to improve access to information and improve health self-management globally, but there is a lack of standardization and limited research on the development of these apps.18,76 Research suggests that available mHealth apps for sleep are variable in quality 77 and, to the best of our knowledge, no other sleep apps have been developed specifically for people with chronic LBP. Once the planned usability testing and the My Back Exercise randomized controlled trial have been completed, if the sleep module is found to be effective, it could be instrumental for future management of patients with LBP and associated sleep disturbances. Further to this, the transparency provided through this study allows for the reproduction or replication of the app in the future.
Strengths and limitations
The main strength of this study is that the development of the MySleepSolutions sleep module for the My Back Exercise mHealth app followed a best-practice design approach. The development process, which occurred over an 18-month period, used an existing mHealth app framework for sleep disturbance. The cyclic, iterative process involved continual editing, reviewing, testing, and remodeling of the content and the functionality of the program by a multidisciplinary team of users, clinicians, researchers, and developers, some of whom had prior experience in developing mHealth apps. Further, the sound evidence base to the content and the functionality of the program adds to the strengths as well as the evidence supporting the need to include sleep retraining in LBP management. 78 The clinical evaluation of the sleep program in the form of usability and acceptability testing and a randomized controlled trial, are currently underway. These studies, however, have not yet been finalised, which could be considered a limitation of this study.
Conclusion

Footnotes
Ethical statement
Authors contributions
KR: conceptualisation, methodology, writing of original draft, review and editing, visualisation. JC: conceptualisation, methodology, app design, review, and editing. JC: conceptualisation, methodology, app design, review, and editing. AMC: conceptualisation, methodology, app design, review, and editing. CMC: conceptualisation, methodology, app design, review, and editing. EH: conceptualisation, methodology, app design, review, and editing. CJ: App design, review, and editing. CG: conceptualisation, methodology, app design, review, and editing. PB: conceptualisation, methodology, app design, supervision, review, and editing. PF: conceptualisation, methodology, app design, supervision, review, and editing. All authors were involved in the concept development and project design. All authors made contributions to the drafted manuscript. All authors read, edited, and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KR is funded by a University of Sydney LBP research scholarship [APP1180474]. AMCS is funded by a University of Sydney Faculty of Medicine and Health Research Centres Stipend Scholarship and a University of Sydney International Tuition Fee Scholarship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.