
Abstract
Objectives: Continued use of a digital health assistant that helps patients living with diabetes to self-manage and deal with complex problems in order to enhance their health status is a healthcare priority. The objective was to explore the barriers related to the use of a mobile personal health assistant for patients with type 2 diabetes. Methods: Eighty-one participants were offered a personal health assistant through a smartphone application. They completed a questionnaire after initial training (T0) and after 1 month’s experience (T1). Results and Conclusion: Most had a positive behavioral intention before using it, but the opposite was found after 1 month. There were positive correlations between behavioral intention and the eight related factors. The strongest correlations were with satisfaction and perceived usefulness at T0 and T1, respectively. The factors’ mean values decreased after 1 month. The best predictors of behavioral intention were satisfaction and performance expectancy at T0 and T1, respectively, which predicted the status of 88.4% and 82.7% of the sample. Our findings will help health experts to build better tools that satisfy patients and meet their expectations.
Introduction
Diabetes is a costly metabolic disease that can lead to premature death. Long-term complications impact the well-being of individuals, families quality of life, and the economy worldwide. The prevalence of diabetes was 463 million in 2019 and is projected to rise to 700 million in 2045. 1 Type 2 diabetes mellitus (T2DM) accounts for the majority of cases among the three main types of diabetes. Behavior management is essential for preventing or delaying T2DM. Self-management involves complex health behaviors such as medication adherence, blood glucose monitoring, dietary and exercise changes, and health outcomes. 2 Effective self-management behaviors can successfully assist people with T2DM in developing and maintaining their healthcare process. 3
In a previous systematic review of 72 randomized controlled trials examining the effectiveness of self-management training, only 27 studies reported improvements in glycemic control. 4 In a more recent systematic review that strictly defined diabetes self-management using the National Standards for Diabetes Self-Management Education and Support, it was found that over 60% of interventions led to significant improvements in HbA1c. However, some types of intervention have shown mixed results. 5 Various types of interventions can result in improved outcomes for enhancing patients’ self-management behavior. Patients play a critical role in diabetes care, so strategies should include active patient participation and willingness to take responsibility for day-to-day disease management. It’s important to provide tools to help patients integrate diabetes management into their daily lives. Advanced self-management tools can help patients improve their ability to manage their conditions effectively. The three main methods for chronic disease self-management interventions are small-group meetings, Internet-based and mobile health (m-Health) technologies, and printed materials. 6 Employing multiple strategies can enhance the effectiveness of self-management approaches.
Since smartphones have become a vital part of many people’s daily lives around the world, they are now being used as innovative healthcare tools for patients with diabetes. M-Health technologies are often considered as a practical solution for improving the self-management of chronic illnesses. This means that mobile devices can support medical and public health practices. 7 The use of mobile technologies allows for regular communication with patients and timely distribution of health information. With mobile networks expanding rapidly, there has been an acceleration in the development of mobile health applications. Moreover, the number of mobile apps that support healthcare is increasing significantly every year. Several studies on the effectiveness of smartphone apps for diabetes care have shown positive results. 8 Therefore, health professionals can recommend the use of smartphone apps to patients who can benefit from them. While there are numerous resources available to help T2DM patients improve their diabetes management, the successful implementation of new healthcare information management technology depends on user acceptance. 9 The decision to adopt new IT can be complex. Human behavioral intention is the result of a cognitive process that involves decision-making. Despite the potential benefits, the acceptance of smartphone apps among patients is lower than expected. Many diabetes patients hesitate to embrace new technology for self-management, and there are several reasons for this. Consequently, the acceptance of new technology presents a significant challenge for health specialists who are creating and integrating health information systems.
The Technology Acceptance Model (TAM) has helped us understand the acceptance of technology from an IT perspective. 9 Users’ acceptance of IT is influenced by their perceived usefulness and ease of use, affecting their attitude towards IT usage and their intention to use it. 10 Venkatesh, Morris, and Davis integrated eight dominant theories and models into the Unified Theory of Acceptance and Use of Technology (UTAUT). The UTAUT consists of four core determinants of intentions and usage (performance expectancy, effort expectancy, social influence, and facilitating conditions) and four moderators of key relationships (gender, age, experience, and voluntariness of use). 11 This model helps clarify the actual use of information systems. Most studies on information system continuance have focused on users’ behavior after acceptance. User expectations regarding the effort needed to use IT may change after actual usage in the technology acceptance process. Bhattacherjee and Premkumar proposed a two-stage model of information system continuance to interpret users’ cognitions about information system usage change over time. 12 Venkatesh, Thong, Chan, Hu, and Brown expanded on the two-stage model by incorporating UTAUT’s key beliefs. They also found that various beliefs appeared in predicting the pre-usage stage and usage stage. 13
Several factors related to the individual (such as knowledge, empowerment, health literacy, motivation, health beliefs, coping and problem-solving skills, locus of control, depression, anxiety, alcohol misuse, and other diseases that may interfere with diabetes management) and the environment (such as social support, provider factors, socio-economic factors, distance to the healthcare facility, other commitments, factors related to the availability of good quality healthcare, nutritious foods, and exercise opportunities) may act as barriers to diabetes patient self-management. 14 Additionally, patient-related beliefs, attitudes, and preferences may affect their willingness to accept or engage in self-care using the information systems mentioned in technology acceptance models. 15 Therefore, it is important to consider these barriers when implementing information systems for disease care, and strategies involving diabetes patients in the treatment process can help in their willingness to adopt and consistently use self-management programs. This approach empowers patients to play a central role in decision-making, and it is essential to eliminate various barriers from the pre-implementation to the rollout phase to shape patients’ beliefs about the transformation process. While various strategies can be used to encourage user adoption of innovative technology, the long-term effectiveness of these tools relies more on the users' continued usage than their initial adoption decisions.
In summary, self-management strategies can improve adherence to diabetes care. Mobile technologies are a new trend for self-management and can help T2DM patients enhance their health and quality of life. Understanding barriers to user acceptance of mobile health apps for diabetes can aid in implementing these strategies. Few studies have focused on the issues affecting T2DM patients’ use of self-management practices via smartphone apps. Exploring these barriers can help healthcare professionals smooth implementation. The aim is to examine factors influencing technology acceptance and barriers related to using a mobile personal health assistant for T2DM patients using the expanded two-stage information systems continuance model and the UTAUT theoretical framework.
Methods
A repeated measures design was used for this study. The relevant Human Research Ethics Review Committees reviewed and approved this study before the research was executed. This study was approved by New Taipei City Hospital REC NTPC protocol #106003-E. Written consent was collected from all participants.
Participants
The participants were recruited from an outpatient center in a teaching hospital in northern Taiwan. Our study included all completed physician visits of individuals aged 20 years or older. We specifically focused on medical visits with diagnoses of T2DM while excluding patients with type 1 diabetes.
Outcomes measures
In this study, we evaluated the acceptance of a mobile personal health assistant (PHA) using a 44-item self-completed questionnaire (see Supplemental Appendix). The questionnaire assessed patients’ views on their intention to use the PHA and included 10 constructs based on the extended two-stage information systems continuance model and the UTAUT theoretical framework. Key factors influencing user intention included performance expectancy, effort expectancy, social influence, facilitating conditions, voluntariness, satisfaction, perceived usefulness, trust, and attitude.11,13 We developed the questionnaire by modifying previously validated items and ensuring cultural adaptations were considered. All constructs, except voluntariness, were measured using a 5-point Likert scale ranging from “strongly disagree” to “strongly agree.” The questionnaire underwent content validity testing, and after minor corrections, it was approved. The Cronbach’s alpha test showed high reliability with an overall score of 0.92 and subscales ranging from 0.88 to 0.94. This indicates that the questionnaire’s items are reliable for use.
Data collection
When eligible participants enrolled, they were offered a smartphone app to monitor their disease, such as blood glucose, weight, and daily activities, and to communicate with healthcare providers. They could also invite their family and caregivers to become partners in controlling their glucose levels. The app’s diary helped them recall what might have caused their data to be too low or too high. It took them 20-25 min to complete the questionnaire, which was administered at two time points: immediately after the initial training (T0) and after 1 month of use (T1). Personal data, including demographic information such as age, gender, marital status, education, religion, number of diseases, and voluntariness of use, were collected at baseline. Actual usage behavior was collected from the app’s platform over 1 month from the initial introduction. For the research, T0 and T1 represented the measurement points to study the effects at the pre-usage stage and usage stage, respectively.
Data analysis
The data was analyzed using descriptive statistics, correlations, independent t-tests, paired t-tests, and multiple linear regression. Mean and standard deviation (SD) were used to describe the central tendency and variance for the continuous data, and number and percentage were used for the categorical data. Multiple linear regression was used to predict behavioral intention. All statistical analyses were performed using IBM SPSS Statistics for Windows version 20.0 (IBM Corp., Armonk, NY). The significance level was set at p = 0.05 for all comparisons.
Results
Between November 2017 and November 2018, we contacted 184 patients with Type 2 Diabetes Mellitus (T2DM). Despite our efforts, only 81 of them (44.0%) agreed to take part in the study. The reasons for refusal included lack of motivation, well-controlled personal management of the disease, difficulty using the mobile PHA, and regular visits to their physician.
Descriptive information for the sample (N = 81).
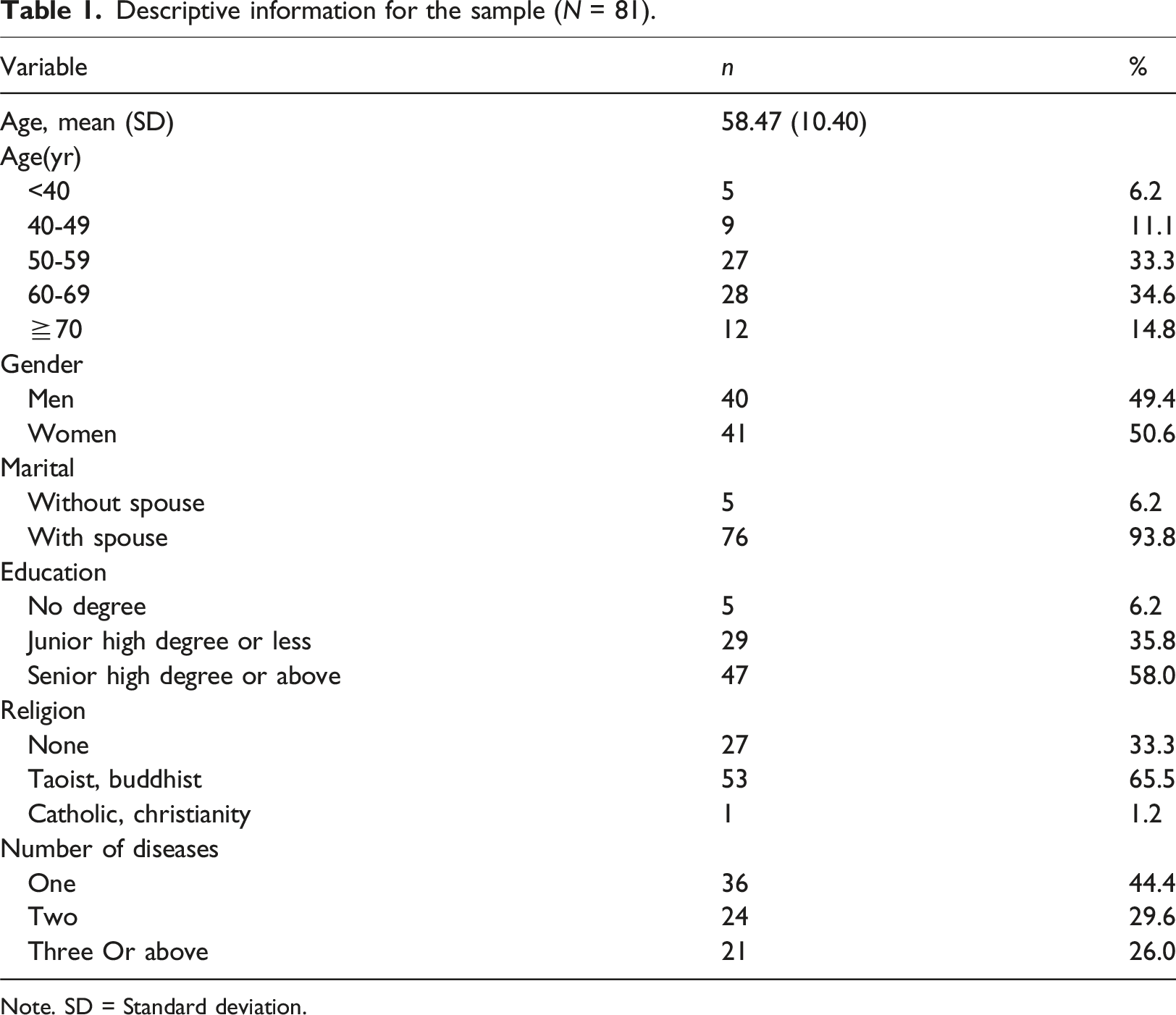
Note. SD = Standard deviation.
Analysis of voluntariness.

Note. SD = Standard deviation.
Correlation matrix for outcome variables at the pre-usage stage and usage stage.
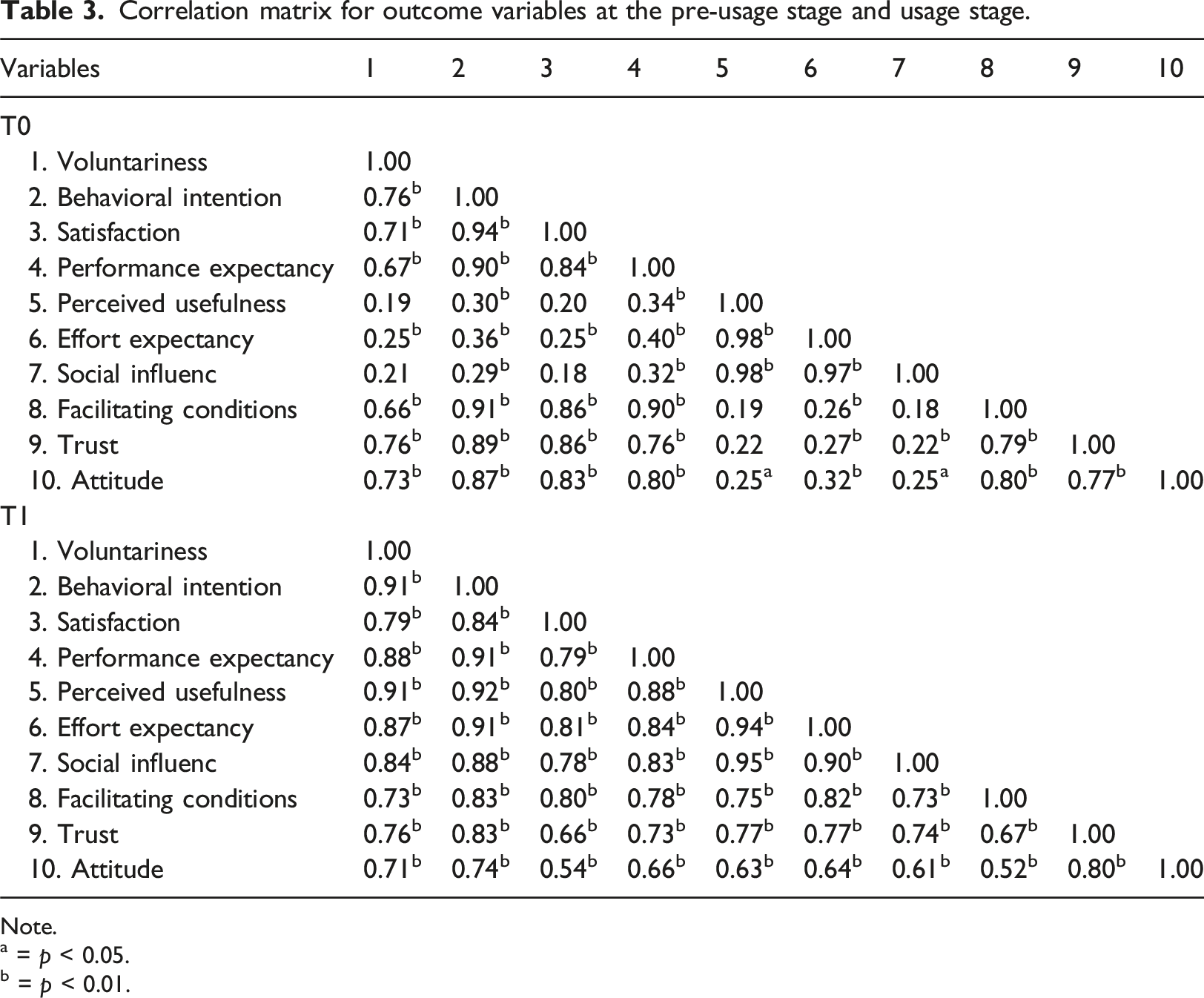
Note.
a = p < 0.05.
b = p < 0.01.
Cognition change between the pre-usage stage and usage stage on using a personal mobile health assistant (N = 81).
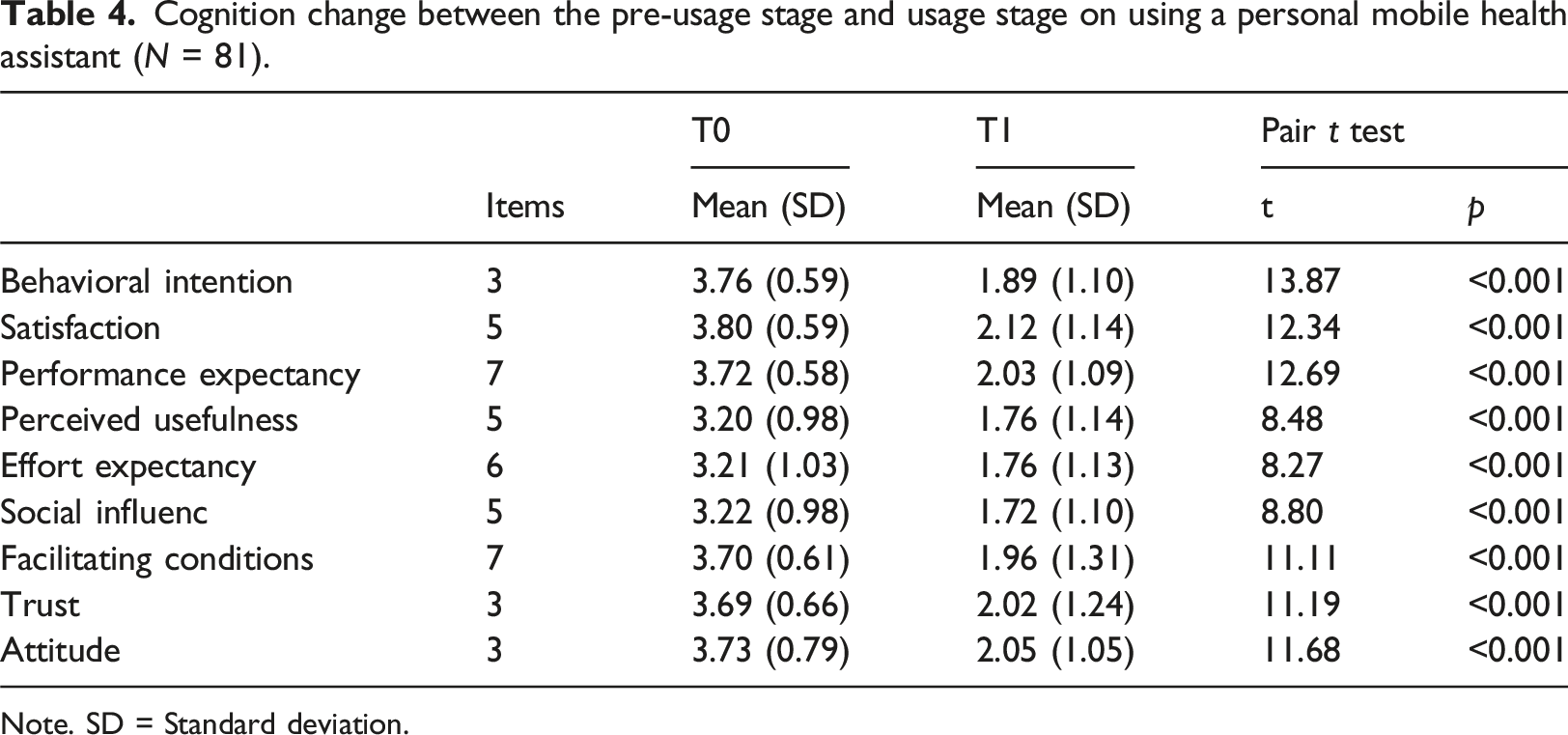
Note. SD = Standard deviation.
Multiple linear regression examining the predictors of behavioral intention on using a personal mobile health assistant at the pre-usage stage and usage stage.
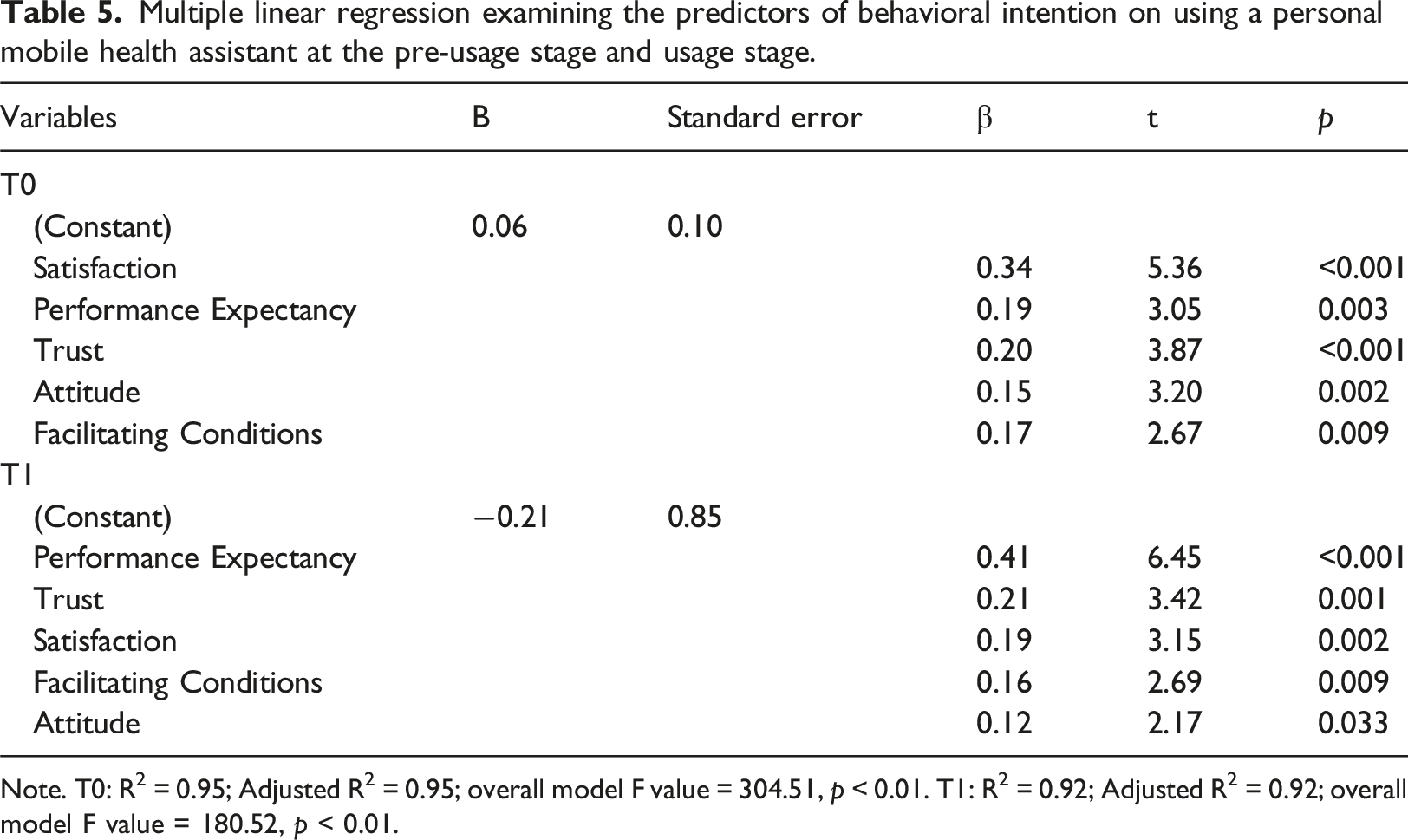
Note. T0: R2 = 0.95; Adjusted R2 = 0.95; overall model F value = 304.51, p < 0.01. T1: R2 = 0.92; Adjusted R2 = 0.92; overall model F value = 180.52, p < 0.01.
Through forward stepwise multiple regression analyses, it was determined that satisfaction, performance expectancy, trust, attitude, and facilitating conditions significantly influenced behavioral intention at both the pre-usage and usage stages. Satisfaction (R2 = 0.88) and performance expectancy (R2 = 0.83) exhibited the greatest impact on behavioral intention at the pre-usage and usage stages, respectively. Furthermore, the combination of these variables explained 94.7% and 92.1% of the variability in behavioral intention at the pre-usage and usage stages, respectively.
Discussion
Our data indicates that there is a lower-than-average use of mobile technology for managing T2DM through smartphone apps, especially among younger T2DM patients. Although individuals diagnosed with diabetes at a younger age are more likely to develop diabetes complications earlier. 16 Younger patients, particularly those under 45 years old, seem less interested in using smartphone apps for diabetes self-management, possibly due to a lack of motivation. Studies have shown that younger T2DM patients have higher HbA1c levels and struggle to follow dietary recommendations. 17 On the other hand, older patients are more likely to adhere to diabetes care, possibly because many of them choose early retirement due to poor health, leading to higher adherence to self-management practices. 18 Additionally, social competition and health-related stigma may contribute to poor self-care practices among younger patients. 17 This is concerning as diabetes patients, especially younger ones, are at higher risk of developing chronic complications, which pose a significant economic burden on the healthcare system. Notably, the prevalence of diabetic kidney disease in Taiwan rose from 10.5% to 17.9% between 2005 and 2014. 19 Additionally, a study by Wang, Wu, Shin, Tien, Chin, and Hwu revealed that patients with T2DM have a higher risk of disease-specific hospitalization compared to those without T2DM. 20 Furthermore, diabetes patients are at a greater risk of developing chronic complications, which also pose an economic burden on the public healthcare system. Another study by Sheen, Hsu, Jiang, Huang, Liu, and Sheu suggested that the increase in diabetes incidence is most noticeable among individuals aged 20–39 in Taiwan. 21 Therefore, health professionals must be equipped with innovative healthcare to better support diabetes patients, especially the younger demographic, during the transition from an aging era to a new age. 22
The smartphone app used in our study was one of the best diabetes apps in 2020, with a rating of 4.7 stars on iPhone and 4.4 stars on Android. This app simplifies and personalizes diabetes management. We observed that T2DM patients initially showed a positive willingness to use the smartphone self-management program before using it. However, most participants displayed the opposite attitude of perceived willingness after using the app. Voluntariness is an important factor that influences users’ decisions to accept or reject innovative technology and moderates their behavior. Moore and Benbasat were the first to identify voluntariness as a crucial factor that influences the continued usage of an information system. 23 In our study, we noticed a higher level of voluntariness and greater behavioral intention at the pre-usage stage. The participants’ perceptions also contributed to adopting the diabetes self-management app. However, over the 1-month period, there was a decrease in voluntariness, behavioral intention, and all influencing factors during the usage stage, and these changes were significant. During data collection, we attempted to gather information on participants’ diabetes duration, HbA1C levels, and diabetes medication, but most participants could not provide these details. Most patients follow their physician’s instructions without a willingness to understand disease care, indicating a lack of motivation for chronic disease self-management. This lack of motivation seems to cause the rapid decline in voluntariness, behavioral intention, and all influencing factors over the 1-month period. In addition, reasons for this decline could include the perception that their disease was well-controlled personally, the inconvenience of using the mobile app for self-management, and regular visits to their physician. Clinical inaction may hinder the use of PHA for self-management of diabetes care. The causes of clinical inaction involve a complicated interplay, which includes the patient. 24 Researchers have also indicated that inertia slows down personal change and adaptation when an innovative strategy is implemented, signaling an important but less-addressed issue. 25
Our study did not take into account how willing patients are to manage their diabetes independently. Simply agreeing to participate in the study does not necessarily mean that the patient is highly willing to self-manage. This could have contributed to our findings. When researchers investigate the barriers to the use of information technology by patients with illnesses, they should not only consider the perspective of the technology acceptance model. Patients’ attitudes toward managing their illnesses are also significant factors to consider. Healthcare professionals need to address the barriers to using diabetes self-management PHA. They should focus on describing the acceptance of self-management PHA from the perspective of people with diabetes rather than just the technology viewpoint. Despite strong evidence supporting the benefits of using a diabetes self-management PHA, there is poor adoption of digital self-management technology by chronic disease patients. 26 Most studies on technology adoption have focused on user beliefs and attitudes during usage, but rarely have they explored changes in these factors or user feelings over time. When implementing technology for disease care, we should also consider other factors that are important, not just those influencing technology acceptance. Participants’ cognitive perceptions may change as they voluntarily gain first-hand experience using digital technology, which could affect their future usage behavior. Overcoming the barriers to adopting self-management technology is imperative in the era of chronic disease that demands innovative self-management practices to achieve optimal clinical outcomes.
In this study, we utilized the two-stage information systems continuance model and the well-established UTAUT to investigate how patients’ experience influences the determinants of behavioral intention for using the self-management PHA over time. User perceptions have long been crucial for predicting users’ continued intention to use a strategic information system. In the context of self-management PHA adoption, T2DM patients agreed that satisfaction, performance expectancy, trust, attitude, and facilitating conditions would increase their behavioral intention. These five positive factors play significant roles in the continued intention to use the self-management PHA. The results align with those of previous studies. 27 This study’s findings further illustrate that satisfaction and performance expectancy are key determinants of the patients’ pre-usage and post-usage behavioral intention. The results indicate that different factors impact the intention to use the self-management PHA over time compared to previous research. With the increasing presence of IT, some scholars have sought to explore users' behavior to predict their continued use of mobile technologies. 28 Throughout these studies, user satisfaction has been identified as a motivating factor affecting their acceptance of innovative technologies. When the services offer effective functions, users are more likely to be satisfied with the system and decide to use it. 29 Satisfaction can be seen as the degree to which users believe that a self-management PHA would be valuable for conducting chronic disease self-management. It has also been identified as a critical predictor of the intention to continue using self-management PHA. Furthermore, it is reasonable to assume that greater satisfaction will lead to more positive trust, attitudes, and intention to use the self-management PHA. Consequently, increasing trust will reduce barriers to adopting the service. Mobile app design and information quality should be enhanced by focusing on satisfaction, attitude, and trust, strengthening users’ continued intention and leading to the continued use of self-management PHA.
Our study also showed that performance expectancy is crucial in determining behavioral intention and continued adoption. Performance expectancy means that the users expect to benefit from adopting the technology. 30 Consequently, performance expectancy primarily influences behavioral intention during the usage stage. When users adopt a healthcare service to self-manage their chronic disease, the impact of performance expectancy on behavioral intention is significant. Before using the app, users will assess the performance expectancy of self-management PHA in terms of improved health outcomes and increased service effectiveness. A previous study also indicated that performance expectancy determines behavioral intention, which affects mobile app use. 27 Another some researchers have suggested that facilitating conditions are not a significant driver of behavioral intention when performance expectancy exists, 31 and that facilitating conditions are an external factor generally not under the users’ control. 32 Therefore, healthcare professionals should emphasize performance expectancy when providing self-management PHA to better benefit users.
To our knowledge, this study was the first to explore the barriers to continuing the usage of PHA for diabetes care. However, there are limitations to consider when interpreting the results. Firstly, the data was collected at a single point in time during the usage stage, so it’s possible that patients’ preferences for self-management PHA may have changed over time. Secondly, the results may not be generalizable to other populations, as the sample mainly consisted of participants from Taiwan whose responses may have been influenced by cultural or geographic differences. Thirdly, the participants’ preferences for app services may have been influenced by their treatment regimen, and this study did not account for these differences. Fourthly, the participants were recruited from a hospital outpatient center so that app use may differ among patients managed in clinics. Lastly, the questionnaire was pilot-tested, and future studies should consider shortening the instrument to achieve higher enrollment rates with a more concise questionnaire.
Conclusion
The results of this study add to our understanding of how people with T2DM take up and use PHA to manage their condition. The study emphasizes the importance of behavioral beliefs in influencing users’ perceptions of the technology. We found that users’ overall views of the PHA play a key role in determining how they use it. There were no outcomes to show the actual impact of the technology. Although our findings differ from some other studies, they truly capture the perspective of T2DM patients. In our research, patients were found to base their decisions on adopting the technology more on their awareness of the disease rather than facilitating factors. Several studies have shown that self-management of diabetes by patients themselves is effective in improving their lifestyle, physical health, and emotional well-being. Managing diabetes throughout one’s life is essential for long-term health. Digital health technologies have the potential to change the way patients with diabetes traditionally manage their care by allowing for continuous and remote monitoring of their symptoms, physiological data, and behaviors. Electronic health tools have become crucial for patients to manage their chronic diseases. Our study’s findings are particularly valuable as they help to identify the obstacles to technology adoption.
Supplemental Material
Supplemental Material - Barriers to mobile personal health assistant in patients living with diabetes
Supplemental Material for Barriers to mobile personal health assistant in patients living with diabetes by Mei-Chen Kuo, Chiou-Fang Liou, Jyh-Horng Lin, Ching-Feng Huang, and Li-Chueh Weng in Health Informatics Journal.
Footnotes
Authors’ note
All authors have read and approved of the submitted manuscript.
Author Contributions
Conceptualization, M.C.K. and J.H.L.; formal analysis, C.F.L.; methodology, M.C.K, J.H.L., C.F.L. and C.F.H.; project administration, M.C.K.; writing-original draft, M.C.K.; writing-review and editing, L.C.W. All authors have read and agreed to the published verson of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology (grant number: MOST 106-2314-B-469-001).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.