
Abstract
Prompt administration of radiotherapy (RT) is one of the most effective treatments against cancer. Each day, the radiotherapy departments of large hospitals must plan numerous irradiation sessions, considering the availability of human and material resources, such as healthcare professionals and linear accelerators. With the increasing number of patients suffering from different types of cancers, manually establishing schedules following each patient’s treatment protocols has become an extremely difficult and time-consuming task. We propose an optimization algorithm that automatically schedules and generates patient appointments. The model can rearrange fixed appointments to accommodate urgent cases, enabling hospitals to schedule appointments more efficiently. It respects the different treatment protocols and should increase staff and patient satisfaction. The optimization algorithm can be connected to a mobile application allowing patients to accept or refuse appointment changes for rescheduling radiotherapy treatments.
Keywords
Introduction
The incidence of cancer is increasing globally, mainly due to the aging of the population. 1 Among cancer treatments, RT has taken an essential place in recent years in view of technological innovations and clinical trials with new irradiation indications. Although around 50% of European cancer patients have an indication for RT, more than one in four do not receive the RT they need. 2 In addition, time is a determining factor in radiation oncology in the extent that RT not delivered on time can lead to local recurrence 3 or even metastasis.3,4 To prevent these complications, RT should commence promptly following standard protocols. Similarly, deviations from the protocol-specified frequency of irradiation sessions can severely compromise local tumor control and overall survival outcomes.
Patient satisfaction is at the center of the hospitals’ concerns. In their RT units, this focus drives continuous improvements in the quality and safety of care. 5 Not to mention that cancer needs a holistic treatment approach to guarantee the best possible quality of life for each patient. In the RT context, it is essential to avoid additional psychological distress for cancer patients due to waiting for RT. Delays may arise from resource shortages, administrative inefficiencies, or unforeseen circumstances. Receiving timely irradiation in accordance with the treatment protocol leads to greater patient satisfaction, which in turn fosters better compliance and strengthens cooperation between caregivers and patients.
In a European context where States seek to guarantee equal access to modern and efficient healthcare for their citizens, patient satisfaction is an important indicator of the quality of healthcare systems. 6 It helps identify areas for improvement and patient needs and, consequently, enables the development of more efficient and better quality services. As healthcare becomes an increasingly competitive field, measuring its level of satisfaction and quality can help healthcare managers monitor and optimize several organizational aspects. 7
The literature shows different hospital optimization systems such as number of nurses for minimizing the expected weighted sum of nurse overtime and patient waiting time. 8 Others find a balance between operational costs and service quality by minimizing the waiting time and the expected cost. 9 The objective of some optimization models is to maximize the number of patients to be scheduled, by taking into account disease priority and treatment sessions. 10
On the other hand, there are several algorithms and approaches to perform the radiotherapy patient scheduling problem (RTPS).
11
In most of the cases the algorithms increase the performance of human experts: 1. Two-stage stochastic mixed integer programming model (SMIP),
8
Multi-objective models,
12
Bi-objective optimization,
9
Integer Linear Programming (ILP)
13
with the aims to reduce the expected cost and increase service quality (waiting time of patient). 2. Based on genetic algorithms (GA)
14
focuses on minimization of the average waiting time of the patients and time difference between the start time and the patient due date. 3. Optimization models
10
try to increase the number of patients that begin the radiotherapy treatment. 4. Operations Research (OR)
15
goal is to investigate how resources, staff and patients can be efficiently coordinated to optimize objectives such as the minimization of waiting times, or the maximization of capacity use. 5. Monte Carlo
16
optimizes for three different range shifter (RS) configurations for Intensity-modulated proton therapy (IMPT) with the goal of reducing the mean dose. 6. ILP
17
combines two robust approaches: the first one considers known patients before they are ready to be scheduled, while the second one considers sets of predicted patients who might arrive in the near future.
Objective
The aim of the present study was to establish an Automated Optimization Algorithm (AOA) for serial irradiation appointment scheduling to help radiotherapy users adapt to increasing cancer incidence, complex treatment, and workflows.
Every week, the RT unit of CHU de Liège faces with the complex task of planning serial irradiation appointments for dozens of patients which must be carried out over several days. This planning must be in accordance with the appointments of each patient set by other units inside the hospital. The task is laborious since it must be completed manually. It requires the acquisition of specific patient information obtained by telephone or by consulting several internal software programs of the hospitals. Due to the complexity of scheduling, an optimization solution is essential.
The RT unit is also keen on respecting the needs of patients and their family/infomal caregivers, such as their time window preference for the patient treatment. Respecting personal needs without neglecting the medical situation requires to consider several variables of each patient before planning appointments. Two administrative staff members are dedicated to this task at CHU de Liège. However, they have reached the limits of human capacity, as they must schedule serial irradiation appointments for hundreds of patients each week. Additionally, urgent irradiation cases often require rescheduling previously arranged appointments, further increasing the workload for the administrative staff. Likewise, in the event of an irradiation machine breakdown, new appointment schedules must be established as quickly as possible.
Aside from the patient’s medical and personnal situation, hospitals must take into consideration the availability of their human (healthcare professionals) and material (scanners, linear accelerators) resources when creating serial irradiation appointments. Thus, scheduling serial appointments requires considering at least 20 to 30 variables linked to the patient, and the human and material resources of the hospital. One should keep in mind that the weighting of each of these variables will differ between patients depending on their medical and personal situations.
It is important to emphasize that RT centers do not operate in the same way, and can weight each of these variables differently and even add or remove some depending on their mode of operation.
We offer a serial irradiation appointment scheduling AI software with the ability to respond to different treatment protocols, while shorting the start treatment time and optimizing the hospital’s human and material resources. The software responds to the need for personalized medicine by offering irradiation appointment planning adapted to each patient by aligning with their other oncological therapies and medical appointments at CHU de Liège but outside the RT department.
Methodology
In this study, we have focused on rule-based optimizers due to the critical need to comply with international regulations governing RT procedures. Other AI algorithms do not reliably meet these requirements, and the current advancement in the field also emphasize the use of rule-based algorithms.
Optimization software
The appointment scheduling software implemented in the Angular programming language keeps systems separated into different modules (frontend, backend, algorithm), thus allowing greater control and security of the system. The software collects the patient’s appointments scheduled in other units of the hospital and the patient’s medical information necessary for scheduling radiotherapy-related appointments using FHIR before running the AOA. The system uses the combination HL7 (Health Level 7) and FHIR (Fast Healthcare Interoperability Resources) protocol, a standard for electronic health data exchange. This algorithm favors: (i) The reduction of the waiting time before the start of radiotherapy. (ii) The reduction of free time slots for the irradiation machines. (iii) The optimization and respect of the working times of the nursing staff.
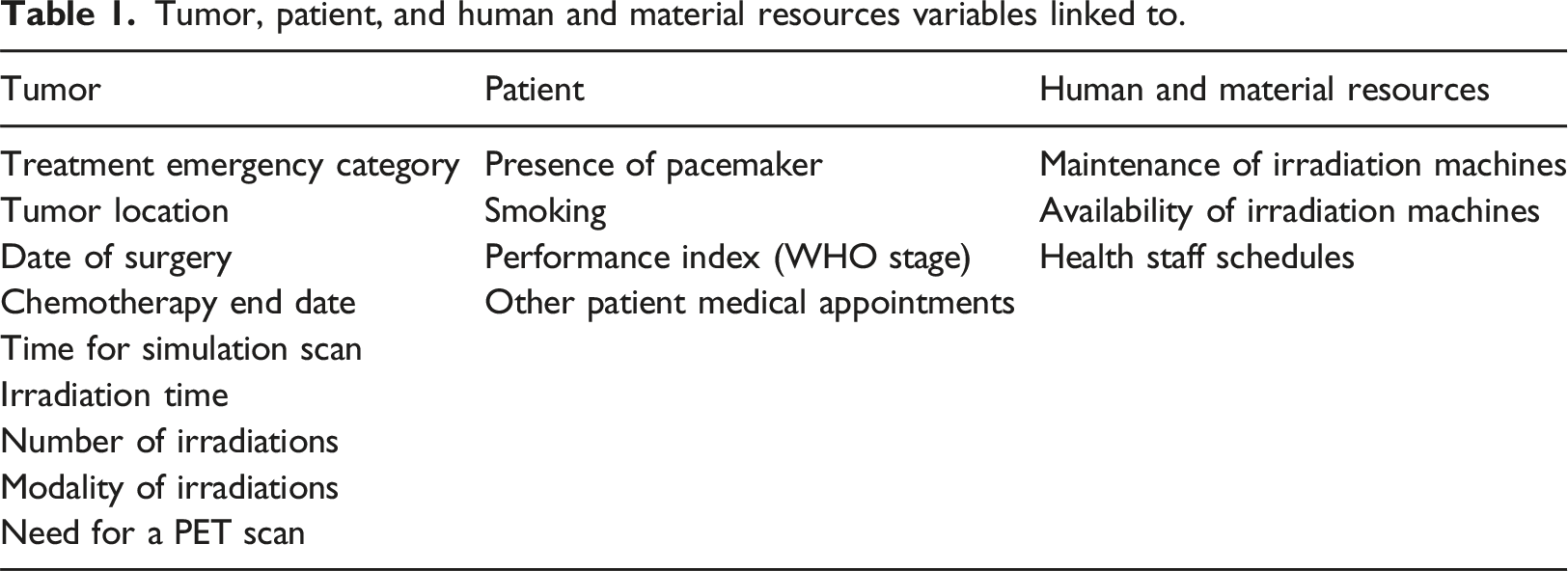
Tumor, patient, and human and material resources variables linked to.
The objective of the algorithm is to reduce the time needed for scheduling, therefore a time between 1 and 5 minutes was given to obtain the best possible solution for a patient.
The AOA considers patient appointments they have outside the RT department. This is achieved by coupling the scheduling software to UltraGenda to the main appointment software bringing together all the medical units of CHU de Liège.
Staff members of CHU de Liège consult separate applications, namely UltraGenda, OmniPro, and Mosaiq, to determine the appointment schedule based on the various patient’s treatments.
Therefore, the scheduling software prevent double bookings by ensuring that appointments cannot be scheduled in time slots already occupied in UltraGenda, such as for pacemaker checks or chemotherapy sessions. In addition, the software is coupled to the patient’s Electronic Health Record (EHR) OmniPro containing structured data where radiotherapists prescribe different radiation modalities enabling personalized radiotherapy for each patient. Finally, the AOA is linked to the Mosaiq software which, among others functions, tracks the availability of radiotherapy machines, including scheduled maintenance days for the irradiation machines. Thus, the AOA has to consult the UltraGenda, OmniPro, and Mosaiq applications to propose tailor-made serial appointments based on specific criteria and availability of human and machine resources.
The following pseudocode (Algorithm 1) details the algorithm. Each step and variable is explained in the accompanying text. The algorithm starts by processing the initial values of each parameter. Note that patient information under treatment (pϵP) has already been uploaded to the FHIR server. For example, the AOA consults the EHR to gather essential treatment data, including the type of cancer, priority for treatment, OMS performance status, type of chemotherapy, presence of a pacemaker, and prior consultations relevant to irradiation (e.g., with a physician, dietitian, PET scan results, simulation team, cardiologist, surgeon, etc.). For the Mosaiq machine, the AOA retrieves all appointment slots occupied by other patients or by the same patient to prevent scheduling conflicts and avoids generating overlapping appointments. The final source from which data is extracted is UltraGenda, which is used to retrieve the patient’s appointments with other specialists outside the radiotherapy department. All this information is captured in the 17 variables that the AOA uses for planning. The data is stored in a structured format on the FHIR server, which the AOA later consults to apply the relevant rule. Some of the rules are parameterizable by changing the values on the FHIR, such as the working hours of the RT machines, the duration of the irradiation sessions and the number of simulation sessions for each patient.
The treatment (p) variables which are associated with the FHIR CarePlan, keeps track of the whole treatment for the specific patient, tracking its data like the number of sessions, times, tumours, priority for treatment, types of cancer, etc. Then, for each patient p ∈ Pn, the AOA checked several rules, for example if the solution; (i) only uses one RT machine for the whole treatment; (ii) if the same patient’s appointments do not overlap in time or location, (ii) or if there are no appointments on forbidden days such as machine’s maintenance, weekends or holidays.

The optimization function of the algorithm was based on two parameters IAD (Inter-Appointment Days) and numFollowUp (n° of follow-up appointments), while always considering each of the restrictions defined by the rules established by CHU de Liège.
Interoperability
For avoiding to couple the implementation of the scheduler with the specific databases and interfaces of UltraGenda, OmniPro and Mosaiq, an abstraction layer offering a FHIR interface was implemented. The choice of FHIR resources (Figure 1) follows the approach presented in the CodeX™ Radiation Therapy Implementation Guide (IG). A radiotherapy treatment plan is represented at a high level by a CarePlan resource. This brings together several ServiceRequest type resources representing the different procedures and treatments to be planned. The CarePlan will therefore always contain a ServiceRequest resource with the SNOMED code 108290001 (radiotherapy) as well as a ServiceRequest resource with the SNOMED code 228705005 (radiotherapy planning with a simulator). Other ServiceRequest resources are created as indicated by the radiotherapist for the treatment intention (MRI, PET/SCAN and/or pulmonary function test). These resources then reference different FHIR Observations that can impact the planning of appointments (weight, WHO score, nutritional score, etc.). The ServiceRequest resource dedicated to radiotherapy additionally contains specific FHIR extensions for the number of fractions, dose and regimen for different treatment volumes. The FHIR layer is also capable of providing all patients appointments at CHU de Liège through Appointment resources. A nomenclature of these Appointment resources allows the scheduler to identify appointments linked to RT treatment (consultation with the radiotherapist, pacemaker monitoring, diet, etc.). All these resources ultimately point to the Patient resource which is the planner’s entry point to discover all the information necessary for the proper planning of appointments. Finally, machine occupancy is exposed via Slot resources for each machine. The sequence of Schedule, Device and Location resources makes it possible to model each processing and imaging machine with their time range of use and their geographical location. FHIR resource diagram.
Conversational robot
In the hospital setting, conversational robots (Chatbots) deployed on mobile phones have the potential to improve organizational workflow, among other things. They also help alleviate the workload of hospital administrative employees. In this study, we developed a mobile application with a chatbot capable of proposing new appointments based on well-defined rules.
The software is coupled with the mobile application where the patient can follow all their appointments. Through the application, the patient can also accept or refuse, thanks to the chatbot, the appointment changes offered to them by the hospital (Figure 2 French version and Figure 3 English version). In addition, the software considerably reduces the time spent on planning, allowing administrative staff to devote more time to listening to the patient. French original Mobile App and Chatbot dialogue. English Mobile App and Chatbot dialogue.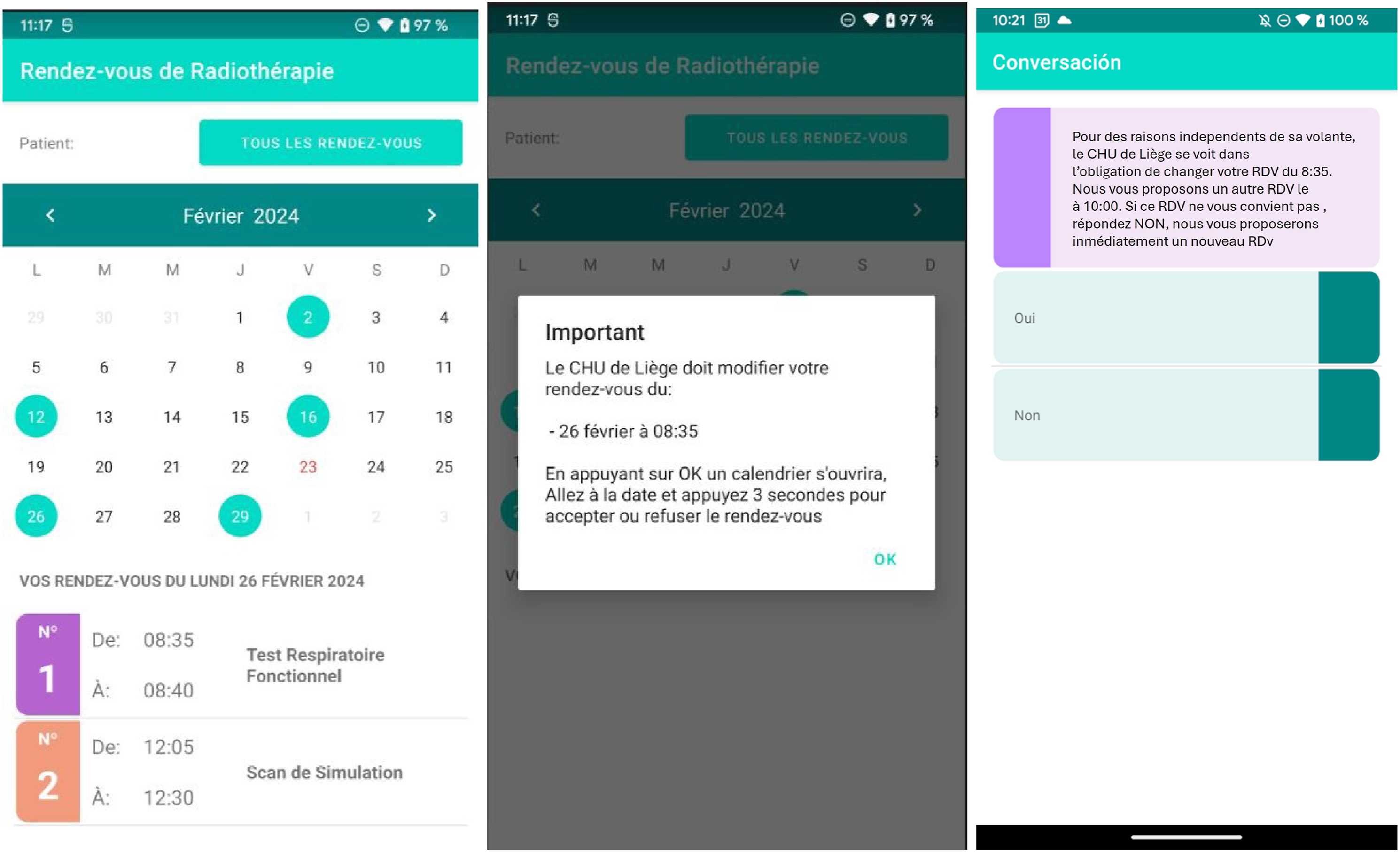

The Chatbot module was intricately designed using the RASA framework,
18
a cutting-edge open-source platform explicitly crafted for constructing conversational systems with robust natural language understanding capabilities. The architecture of the chatbot system encompasses three fundamental components: (i) Natural Language Understanding (NLU), which scrutinizes user input to discern intent and extract pertinent information. (ii) Dialogue Management, responsible for monitoring the conversation flow and current state to determine the optimal subsequent action. (iii) Natural Language Generation (NLG), dedicated to crafting human-like responses tailored to the ongoing conversation context.
The system’s modular architecture is built upon a unified API, seamlessly integrating diverse Natural Language Processing (NLP) and Machine Learning (ML) libraries. 19 Notably, RASA adopts a distinctive approach, predicting ”slot-labels” and ”slot-values” within user input rather than relying on a traditional sequential word analysis. This study extends the application of the developed chatbot within the ambit of the PERSIST project, 20 contributing to the creation of a conversational platform for scheduling appointments. The mobile application facilitates user interaction with the conversational agent through an API, presenting available appointment slots that align with the irradiation protocol. Employing guided conversations, users can effectively navigate and select the most suitable appointment time option for themselves. This research underscores the innovative use of the RASA framework in developing a multilingual conversational platform, showcasing its potential applications in enhancing user engagement and accessibility.
Results
We aimed to compare the performance of the human-driven scheduling and the automated scheduler. Patient satisfaction was assessed for identifying items to be improved in the Chatbot and the AOA.
To obtain this performance information the AOA was tested with data from patients with breast cancer. Three treatment modalities were taken into consideration: (i) Hypofractionated RT according to the Fast-Forward protocol WITH Deep Inspiration Breath Hold (DIBH) coaching, (ii) Hypofractionated RT according to the Fast-Forward protocol, (iii) Several fraction regimen. The Fast-Forward protocol (modality i and (ii) significantly reduces the number of treatment sessions. Instead of the traditional 15 irradiations, the Fast-Forward protocol delivers the entire treatment in only five irradiations. For patients with a tumor in the left breast, the DIBH technique (modality (i) is used during radiation therapy to minimize radiation exposure to the heart and lungs. The patient is instructed to take a deep breath and hold their breath during treatment. This reduces the radiation dose to the heart, lungs and other critical structures. Thus, the schedule of patients who have had a tumor in the left breast differs from that of patients who have had a tumor in the right breast. Left breast patients not only require longer time slots but other appointments are added, including an appointment with a cardiologist after each irradiation.
To generate the appointments, the data found in the irradiation prescription were entered into the software. The software generates each patient’s appointments taking into account all his other appointments set by other units in the hospital. Two appointment coordinators verify that the appointments offered to patients by the scheduling software follow the rules imposed by the hospital.
The AOA follows the rules imposed by the hospital according to the three modalities of breast cancer irradiation treatment. The performance of the software has a high-speed execution; 2 to 15 seconds are sufficient to generate patient appointments. In comparison, this same work takes appointment coordinators at least 10 to 20 minutes.
Comparative study with prospective data
This research aimed to compare the IAD from irridation protocols generated by the CHU de Liège staff with those produced by an automated scheduler. Our null hypothesis assumes that there is no difference in IAD between human-driven scheduling and AOA planning. Therefore, the alternative hypothesis states that there is an IAD difference between human-driven and automated scheduling.
The present version of the AOA was based on 17 variables relevant to breast cancer. In the future, an enhanced version will incorporate up to 30 to 40 variables, covering medical conditions, psychosocial aspects of each patient, complex cancer treatment pathways, and hospital logistics, including staff and equipment availability. The ultimate goal is to offer increasingly personalized medicine and introduce in the AOA other kind of cancers whose planning of radiotherapy sessions is more complex and requires more variables.
We explored four temporal windows in 20 enrolled breast cancer patients (60.9 ± 8.6 y/o) as follows: 1. Temporal window 1: Number of days between the 1st consultation and scan simulation appointment. 2. Temporal window 2: Number of days between scan simulation and 1st irradiation. 3. Temporal window 3: Number of days between 1st irradiation and last irradiation. 4. Temporal window 4: Number of days between 1st irradiation and last consultation.
The general hypothesis states that the 17-variable method does not generate differences between the IAD generated by the AOA and the human-driven scheduling. This implies that our data shows that it provides evidence in favor of the null hypothesis. For this reason, we performed a Bayesian analysis using JASP software 21 in the three breast cancer treatment modalities.
Fast-Forward with DIBH: Hypofractionated RT according to the Fast-Forward protocol WITH Deep Inspiration Breath Hold (DIBH) coaching
BF01 to be changer with 01 underscored For breast cancer patients treated with the hypofractionated RT according to the Fast-Forward protocol
22
and receiving a DIBH coaching, the AOA did not generate any variability for the patients (Figure 4). Therefore, we performed a one-sample Bayesian t test for each temporal window against the mean value (i.e. single value) of the AOA. Fast-forward with DIBH.
For the temporal windows 1, three and four the analysis revealed a Bayes Factor (BF) ofBF01 = 1.052, BF01 = 1.006 and BF01 = 1.093 respectively. These results provides a moderate evidence (BF01 > 1) in favor of the null hypothesis suggesting no IAD difference between human-driven and the automated scheduling. This suggests that both methods perform similarly in finding available time slots for the scan simulation, all serial irradiation appointments, and scheduling the final consultation with the radiotherapist. Nonetheless, these three BF (i.e., 0.3
In contrast, only in temporal window 2 (BF01 = 0.05), the alternative hypothesis is more likely. This implies that, by achieving a lower IAD, the CHU de Liège staff is more efficient than the AOA in securing a free slot for the first irradiation following the scan simulation.
The main task of CHU de Liège staff is to adhere as closely as possible to the ground truth protocols for each of the radiotherapy modalities. Thus, comparing the range (light green) or unique protocol IADs with those generated by the AOA and the CHU de Liège staff helped identify which method was more precise and better aligned with the hospital’s internal planning guidelines.
Figure 4 illustrates that, for temporal windows 1, 3, and 4, the IADs computed by the AOA are more closely aligned with the protocol (reference values) compared to those generated by the human-driven approach. This implies that the AOA might be outperforming CHU de Liège staff in estimating IADs in these three specific windows. In contrast, the IAD generated by the human-driven approach is actually closer to the protocol’s IAD than the AOA’s IAD for the temporal window 2. This indicates that for this particular temporal window, CHU de Liège staff outperform the AOA in matching the counterpart protocol IAD. In addition, in the fourth temporal window, the IADs generated by the AOA showed no variability whereas those produced by the CHU de Liège staff did.
Fast-Forward without DIBH: Hypofractionated RT according to the Fast-Forward protocol
For breast cancer patients treated with hypofractionated RT according to the Fast-Forward protocol, who did not need a DIBH coaching, we conducted an independent samples Bayesian t test for each temporal window to compare the human-driven scheduling and the automated scheduling. (Figure 5). For temporal window 1, the analysis revealed a Bayes factor Fast-forward without DIBH.
Benchmarking with the protocol showed that the mean IAD values for the AOA temporal windows one is closer to the counterpart protocol than the one generated by CHU de Liège staf. However the IAD values for AOA exhibited greater variability than those generated by the CHU de Liège staff. The opposite was true for temporal window 2, where the mean IAD generated by the CHU de Liège staff fell closer to the range accepted by the protocol, with less variability compared to the mean IAD for AOA. This indicates that the AOA faced greater difficulty in finding available slots for both the scan simulation (after the 1st consultation) and the 1st irradiation (after the scan simulation) compared to the CHU de Liège staff. Interestingly, for temporal windows three and 4, the AOA successfully adhered to the IAD values imposed by the protocol while the IADs generated by CHU de Liège staff exhibited variability. This implies that the AOA tended to follow the protocol’s favored approach of starting the first irradiation on Mondays, ensuring that the fifth irradiation (last irradiation) is completed on Fridays. In contrast, the CHU de Liège staff also proposed the first irradiation on Wednesdays or Thursdays to ensure at least three or two irradiations in the first week, with the remaining irradiations scheduled for the following week (temporal window 3). The same is true for temporal window 4, where the AOA aligned with the protocol by offering the last consultation strictly 14 days after the final irradiation. In contrast, CHU de Liège staff offered the last appointment with greater flexibility knowing that a few more or fewer days for this appointment would not jeopardize the patient’s care pathway.
Several fraction regimen with or without boost
For patients receiving more than five irradiation sessions, we conducted four independent samples Bayesian t-tests, one for each temporal window, comparing the automated and human-driven scheduling. (Figure 6). The results revealed BFs of 1.469, 1.286, 0.552, and 0.507 for temporal windows 1, 2, 3, and 4, respectively. BFs of temporal windows 1 (BF01 = 1.469) and 2 (BF = 1.286) indicated moderate evidence in favor of no IAD difference between human-driven and automated scheduling. In contrast, for temporal windows three and 4, the alternative hypothesis was more likely, suggesting that the AOA and CHU de Liège staff were not performing in the same way. Nonetheless, the data remain inconclusive as these BF values are 0.3 < BF < 3. Several fraction regimen.
Benchmarking with the protocol showed that the mean IAD generated by the AOA in temporal window one fell closer to the IAD range accepted by the protocol than that of CHU de Liège staff. Thus, by achieving a lower IAD, the AOA was more efficient than the CHU de Liège staff in securing a free slot for the scan simulation after the 1st consultation. As stated above, there is no strong evidence in favor of the null hypothesis for temporal window 2, nevertheless, both scheduling methods aligned with the IAD range accepted by the protocol. Although the performance of the automated and human-driven scheduling for temporal windows three and four was likely not the same, both methods generated similar mean IADs that did not align with the protocol. This indicates that, for long irradiation protocols (e.g., 15 irradiations), both methods faced difficulties in finding available slots to complete the radiotherapy, which also delayed the appointment for the final consultation.
Patient satisfaction
Chatbot patient satisfaction.

AOA patient satisfaction.

Chatbot patient satisfaction
To assess patients’ opinion on the Chatbot’s usability, acceptability, and appropriateness a Patient Reported Experience Measure (PREM) was assessed through a generic Likert scale questionnaire (Table 2). The 20 patients enrolled in the study were able to experience the use of the written chatbot in the presence of the hospital project manager. More than half of the patients (55%) did not have a clear opinion on the Chatbot as a tool allowing them to communicate with the hospital (question 1). This is reflected in the preference of 80% of patients (question 5) to communicate directly with a member of the hospital staff. However, several patients have understood the usefulness of Chatbot since at least 50% of them remain open to using a Chatbot (question 4). Moreover, in the event a Chatbot was offered to patients, no clear predilection between an oral (50% question 2) or written version of it (65% question 3) was observed. Importantly, 65% of patients found the version of the Chatbot they tested to be satisfactory (question 8), and more than half (75% question 9) agreed that the new appointment automatically offered by the Chatbot met their needs (Table 2).
AOA patient satisfaction
Patients (63.2%, question 1) were highly satisfied with the time period offered by the AOA between the simulation and the first treatment appointment, as it was customized to suit their specific irradiation modalities. However, the AOA did not meet the expectations of most patients (68.4%, question 2) regarding the proposed time for the first treatment appointment, as it was scheduled too early in the morning during peak traffic hours. Nonetheless, patients were extremely (84.2%, question 3) satisfied with the new appointment offered by the AOA when an appointment change was simulated via the Chatbot (Table 3).
Clearly, further testing with larger numbers of patients is needed to validate these results in diverse hospital settings, to ensure that the results are generalizable and reliable across diverse clinical environments. Each hospital may have unique workflows, patient demands, and technical resources, all of which can influence the effectiveness and applicability of the approach. A potential limitation is the need for customization, as the solution may need to be adapted to fit the specific operational practices, equipment, and protocols of different institutions.
Conclusion
This project aimed to develop an Automated Optimization Algorithm integrated with a chatbot application to enhance the quality and accelerate the scheduling of irradiation appointment series in the CHU de Liège Radiotherapy department.
The AOA adhered to the scheduling requirements imposed by the three irradiation modalities for breast cancer treatment. It considered 17 variables related to patients, as well as human and material resources, such as machine handling days and caregivers schedules to optimize human resource efficiency while ensuring well-being within the hospital. For achieving this, three internal hospital software programs were integrated into the AOA. The time required to transfer patient data from the three software to the AOA was currently estimated between 1 and 5 minutes. Once this data was acquired, the AOA was able to quickly (between 2 and 15 seconds) generate the appointment schedule for each patient. In comparison, this same work takes appointment coordinators at least 10 to 20 minutes. This highlights the AOA’s potential for real-time scheduling, which can have a direct impact on patient outcomes. The reduction of administrative burden and improvements in patient satisfaction, especially regarding the system’s capacity to handle urgent rescheduling, are notable outcomes of this work.
Given that our study enrolled a limited number of patients, our results were inconclusive. Nevertheless, despite the small sample size, moderate evidence in favor of no difference in IADs between human-driven and automated scheduling (the null hypothesis) was observed in several temporal windows. Additionally, several mean IADs from the AOA matched those of the protocol. Altogether, these results suggest that the current version of the AOA tends to perform similarly to humans and therefore is progressing in the right direction. Despite these achievements, the integration of the AOA into the hospital workflow is not without its challenges. Indeed, the AOA’s success in maintaining protocol-consistent IADs suggests that further optimization might be required to outperform human schedulers in complex, multi-variable scenarios. In addition, our study demonstrates a significant positive outcome in patient satisfaction regarding the efficacy of AOA scheduling, particularly when rescheduling appointments is necessary.
Nevertheless, patient satisfaction, especially among older adults, was an area identified for improvement, with the chatbot application needing upgrades to enhance usability for patients over 60 y/o. Personalization, while effective, may not yet fully capture the individual preferences and needs of patients across all demographic groups, indicating that further user testing and iterative improvements to the AOA interface are required. In conclusion, these findings indicate that the algorithm behind the automated scheduler can effectively address current scheduling challenges. Further improvements in patient satisfaction, such as personalized scheduling, will be incorporated in the next AOA version. We are also considering to facilitate future management of nurse shortages by integrating long-term absences in the next AOA version, which are often the result of the physically demanding and emotionally challenging nature of the work. By incorporating new variables (up to 30-40 in total), the improved AOA version is expected to provide more personalized treatment, further enhancing patient and healthcare staff satisfaction, while optimizing hospital resources to reduce costs.
Currently, the resulting schedule is manually verified and entered into the radiotherapy software, Mosaiq. This process ensures that the responsibility for the schedule remains with the hospital staff, not the scheduling software. In the future, this process could potentially be automated; however, it is important to note that this would likely require medical device certification, as the responsibility for treatment programming would shift from the staff to the scheduling system. For the automated transfer of schedules to Mosaiq, the ESI interface, based on HL7/FHIR, could be implemented, provided it supports writing appointments into Mosaiq.
Given the economic crisis facing European hospitals, tools like this AOA can help alleviate the workload of existing staff without increasing the administrative burden. This will become increasingly relevant in the coming years, which are expected to see a rise in cancer diagnoses. The rising demand for healthcare services is straining the sustainability of health systems globally. If hospitals fail to deliver services efficiently, they risk compromising their long-term sustainability. The present automated scheduler can be applied not only to other types of cancers but also to other hospital departments, addressing the complex task of appointment scheduling and various other types of planning, such as coordinating operating rooms or managing nurses’ schedules, which require the integration of multiple software systems. The ultimate goal is to make the entry of constraints into the algorithm more flexible so that each hospital can configure its own data and operate according to its specific rules.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The software was the result of a co-creation between Instituto Tecnológico de Castilla y León (ITCL, Spain) and the University Hospital of Liège (Belgium). The application and the Chabot were collaborative efforts between ITCL and the University of Maribor. Both achievements were part of the HosmartAI project that received funding from the European Union’s Horizon 2020 Research and Innovation programme under grant agreement No 101016834.