
Abstract
This study investigates the barriers to implementing electronic health records (EHR) systems for decision support in Tanzanian primary healthcare (PHC) facilities and proposes strategies to address these challenges. A qualitative, inductive approach was used, guided by the Diffusion of Innovations (DOI) theory, the Technology Acceptance Model (TAM), and the Sociotechnical Systems theory. Using snowball sampling, data were collected from 14 participants through semi-structured interviews in Dodoma, Tanzania. Thematic analysis identified key barriers. Critical barriers to EHR implementation include lack of leadership support, poor network infrastructure, increased workload, and resistance to technology due to concerns over professional autonomy. Technical challenges, such as system downtime and lack of skilled personnel, hinder EHR use, resulting in inefficiencies and incomplete system adoption, negatively affecting patient outcomes. This study offers unique insights into barriers to EHR adoption in Tanzanian PHC facilities. Grounded in multiple theoretical frameworks, the findings contribute to health informatics discourse in low-resource settings and provide practical recommendations for improving EHR implementation. The study’s implications are relevant for policymakers, healthcare leaders, and IT developers in similar contexts.
Keywords
Introduction
Electronic Health Records (EHR) systems have become essential instruments in the modern healthcare delivery landscape, helping to ensure accurate, timely, and patient-centred care. 1 These digital platforms promote communication and information sharing among healthcare providers, expediting clinical workflows and eventually improving patient outcomes. 2 EHR systems are computerised replications of paper patient charts. 3 They include detailed data on the medical history, diagnosis, prescriptions, plans of care, dates of immunisations, allergies, radiological pictures, and outcomes of laboratory tests of the patients. 4 The main goal of EHR systems is to give medical staff instant access to current, accurate patient data so they may make well-informed decisions about patient care.
Implementing EHR systems in Primary Health Care (PHC) facilities has been recognised globally as a transformative approach to enhancing healthcare delivery. These systems address issues such as fragmented health information, ineffective record-keeping procedures, and difficulties in monitoring patient health outcomes. For instance, in high-income countries such as the United States and the United Kingdom, EHR systems have been widely adopted to streamline workflows, improve patient safety, and enhance the quality of care. 5 In contrast, low-resource settings such as Ethiopia and Kenya face challenges related to infrastructure and workforce readiness, limiting the full potential of EHR systems despite their promising impact.6,7 Research conducted in both developed and developing contexts consistently demonstrates the revolutionary potential of EHR systems to optimise healthcare delivery, underscoring their significance for Tanzania’s healthcare environment.8,9 However, specific barriers unique to the Tanzanian context, such as limited resources and cultural attitudes, require further investigation to unlock the full benefits of EHR systems in this region.
Tanzania’s healthcare system operates under a decentralised structure with PHC facilities forming the core of healthcare delivery, particularly in rural and underserved regions where the majority of the population resides. The system is divided into three levels: national, regional, and district levels, with PHC facilities such as dispensaries, health centres, and district hospitals serving as the first point of contact for most citizens. 10 Despite government efforts to improve healthcare infrastructure, Tanzania continues to face challenges, including insufficient funding, healthcare worker shortages, and deteriorating physical infrastructure. 11 Many facilities, especially in rural areas, lack adequate equipment, reliable electricity, and consistent internet connectivity, which are critical for the effective adoption of EHR systems. 11 Moreover, the country’s health financing primarily relies on public funding, with mechanisms such as the National Health Insurance Fund (NHIF) and the Community Health Fund (CHF) playing essential roles in ensuring access to healthcare services, though coverage remains limited for a significant portion of the population. 12 These systemic challenges underscore the need for a context-specific investigation into the barriers hindering EHR implementation in Tanzania, particularly in PHC facilities.
However, while several studies have investigated EHR systems implementation across various contexts, such as in developed nations, low-resource settings, and regions with differing health infrastructure and workforce capabilities,6,9,13,14 Tanzania presents unique challenges due to its specific cultural, economic, and infrastructural conditions. For example, in high-income countries like the United States and Europe, EHR systems benefit from robust infrastructure, high technological literacy, and strong policy frameworks. 5 In contrast, Tanzanian PHC facilities have limited resources, a lack of consistent electricity and internet access, diverse cultural attitudes towards technology adoption, and substantial infrastructural deficits. 11 These factors necessitate a focused study to uncover context-specific barriers and strategies, particularly within the Tanzanian context, thereby contributing new insights to the global discourse on EHR implementation.
Recent studies have extensively explored barriers to EHR implementation. For instance, Gesulga et al. 6 identified critical challenges in developing countries such as the Philippines, India, and other Southeast Asian nations, where inadequate training, limited technological infrastructure, and a shortage of skilled workers hinder EHR adoption. Similarly, Kruse et al. 9 examined adoption factors and barriers in diverse healthcare settings, including the United States, where interoperability, data privacy concerns, and user resistance were significant hurdles, and in low-resource settings in Latin America and Africa, where infrastructural deficits and lack of policy support presented major obstacles. Palabindala et al. 15 focused on the adoption of EHR systems in community hospitals in the United States, highlighting that even in relatively resource-rich environments, issues such as system complexity, lack of training, and resistance from clinical staff were pervasive. These studies provide a background against which this study situates its investigation, emphasising the need to address the specific cultural, individual, technical, and organisational barriers unique to Tanzania.
Addressing these gaps, this study explores the barriers to EHR system implementation in Tanzanian PHC facilities. This study seeks to identify and analyse the unique challenges faced in this context by conducting in-depth qualitative research. The findings are expected to inform policy and practice, offering targeted strategies to enhance EHR implementation and improve healthcare delivery in Tanzania. Specifically, the study seeks to: 1. Determine the barriers PHC facilities in Tanzania face when implementing EHR systems. 2. Evaluate how these barriers may affect patient outcomes and healthcare delivery. 3. Provide recommendations to overcome PHC facilities’ obstacles while implementing EHR systems.
By achieving these objectives, the study intends to contribute to the body of knowledge of implementing EHR systems in environments with limited resources and influence healthcare policy and practice in Tanzania.
Theoretical framework
This study was guided by several theoretical perspectives that provided a foundation for exploring the barriers and challenges to implementing EHR systems for effective decision support in Tanzanian PHC facilities. The Diffusion of Innovations (DOI) Theory, the Technology Acceptance Model (TAM), and the Sociotechnical Systems Theory were employed to shape the study’s exploration into how these barriers affect the effective implementation of EHR systems.
DOI provided a guiding framework to explore how various factors, such as relative advantage, complexity, and compatibility, influence the successful implementation of EHR systems 16 Although the study was not focused on how EHR systems were implemented, it used this theory to explore whether such factors hindered the systems from being fully integrated and utilised within PHC facilities.
TAM was another critical framework guiding the study. According to TAM, two primary factors, perceived usefulness and ease of use, influence the acceptance and implementation of new technology.17–20 This study used TAM to understand whether healthcare professionals in Tanzanian PHC facilities perceived EHR systems as useful for enhancing decision-making and whether they found the systems easy to use within their busy work environments. This theoretical model helped explore how these perceptions could impact the systems’ effectiveness in supporting clinical decisions.
The Sociotechnical Systems Theory provided a holistic approach to understanding the interaction between technical and social elements in implementing EHR systems. The theory was instrumental in exploring how organisational, technical, and social barriers affected the systems’ implementation.21,22 The study applied this theory to investigate how factors such as leadership support, resource availability, and technical infrastructure influenced the implementation process in Tanzanian PHC facilities. The sociotechnical approach allowed the study to focus on the technical aspects of EHR systems and how well these systems were integrated into the healthcare settings’ social and organisational structures. This provided insights into how system design, technical support, and healthcare staff readiness contributed to overcoming or exacerbating implementation challenges.
Conceptual framework
Together, these theoretical perspectives informed the study’s conceptual framework in Figure 1, which examined the interaction between individual, organisational, technical, and cultural factors that could impede the effective implementation of EHR systems. The framework anticipated that these factors would influence the systems’ ability to support clinical decision-making. By grounding the study in these theoretical perspectives, the study aimed to discover how these barriers affected the implementation of EHR systems in Tanzanian PHC facilities. The theoretical frameworks guided the investigation into how these systems could be more effectively utilised to enhance decision-making and inform strategies for overcoming the identified challenges. Conceptual framework. source: Authors work.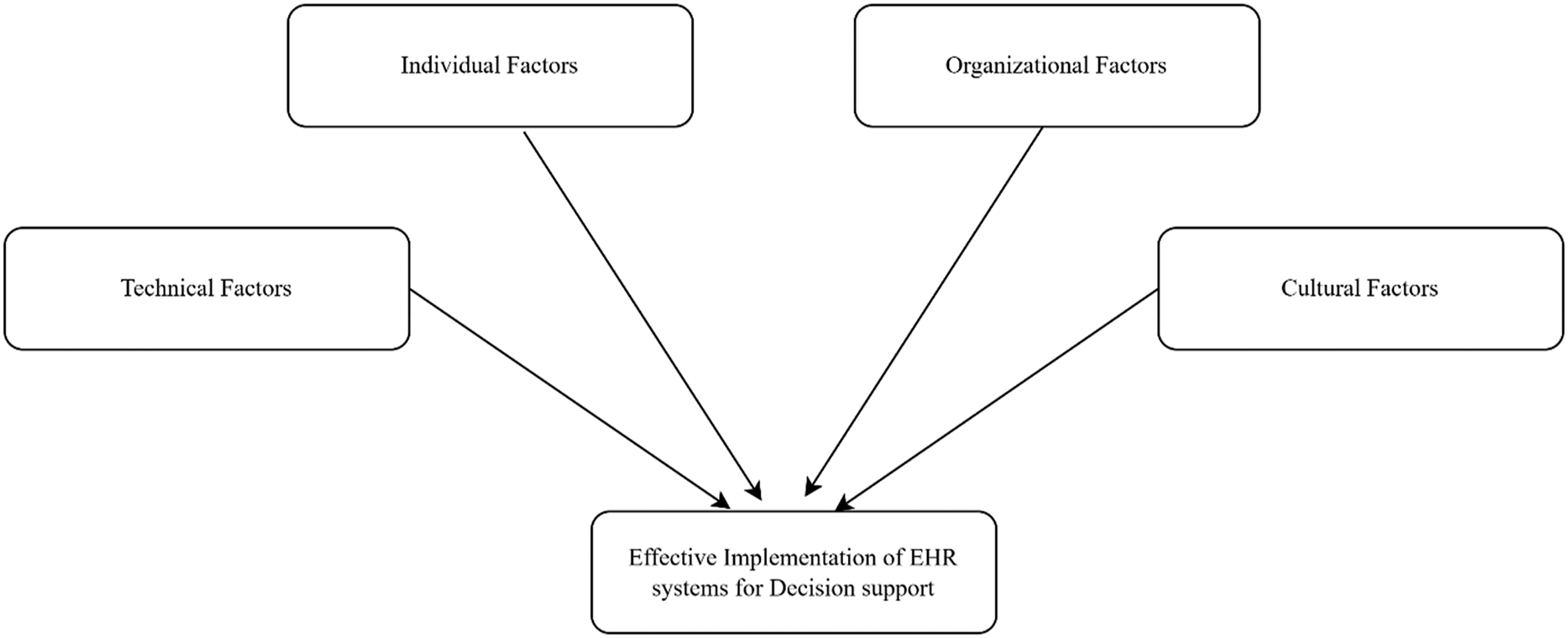
Methodology
Research philosophy
This study follows a constructivist research philosophy, which emphasises understanding the subjective meanings that participants attach to their experiences. 23 Constructivism is suitable for exploring complex social phenomena, such as the barriers to EHR implementation in Tanzanian PHC facilities, as it allows for exploring multiple perspectives from healthcare professionals. This philosophy guided the research to focus on how various stakeholders interpret and interact with EHR systems, acknowledging that social and technical contexts influence these systems.
Research approach
An inductive qualitative approach was adopted for this study. The inductive approach allowed themes to emerge directly from the data rather than testing an existing theory.24,25 This approach was chosen because the objective was to explore barriers to EHR system implementation within Tanzanian PHC facilities without preconceived notions. Qualitative research is particularly well-suited to understanding the context-specific challenges faced in resource-limited settings like Tanzania. However, the findings are context-specific and may not be easily generalised to other regions or healthcare environments. Furthermore, while reflexivity was practised to minimise researcher bias, the influence of the researchers’ prior knowledge on data interpretation cannot be entirely ruled out.
Research design
The study employed a case study design, focusing on multiple PHC facilities in the Dodoma region. This design enabled an in-depth exploration of the barriers specific to different healthcare facilities, considering the varying organisational structures, resources, and levels of EHR adoption. This design is appropriate when the research aims to gain a holistic understanding of a phenomenon in its real-life context.26,27
Study area
The study was conducted in the Dodoma region, in the centre of Tanzania. Dodoma was chosen due to its status as a rapidly growing region that faces many of the same healthcare challenges across the country, making it an insightful location for exploring barriers to EHR implementation. The region includes a variety of public and private PHC facilities, which allowed for a nuanced examination of how different healthcare settings experience EHR challenges. While the findings reflect the specific context of Dodoma, the region’s blend of urban, peri-urban, and rural healthcare facilities provides a valuable lens for understanding similar challenges in other parts of Tanzania.
Study population and sampling procedures
The sample size was determined using the principle of saturation, where new data no longer yield additional insights or themes relevant to the research questions. This study reached saturation after interviewing 14 participants, each providing rich information on the barriers to EHR systems implementation. This sample size aligns with qualitative research norms, where the focus is on depth rather than breadth.
Participants involved in interview administration.
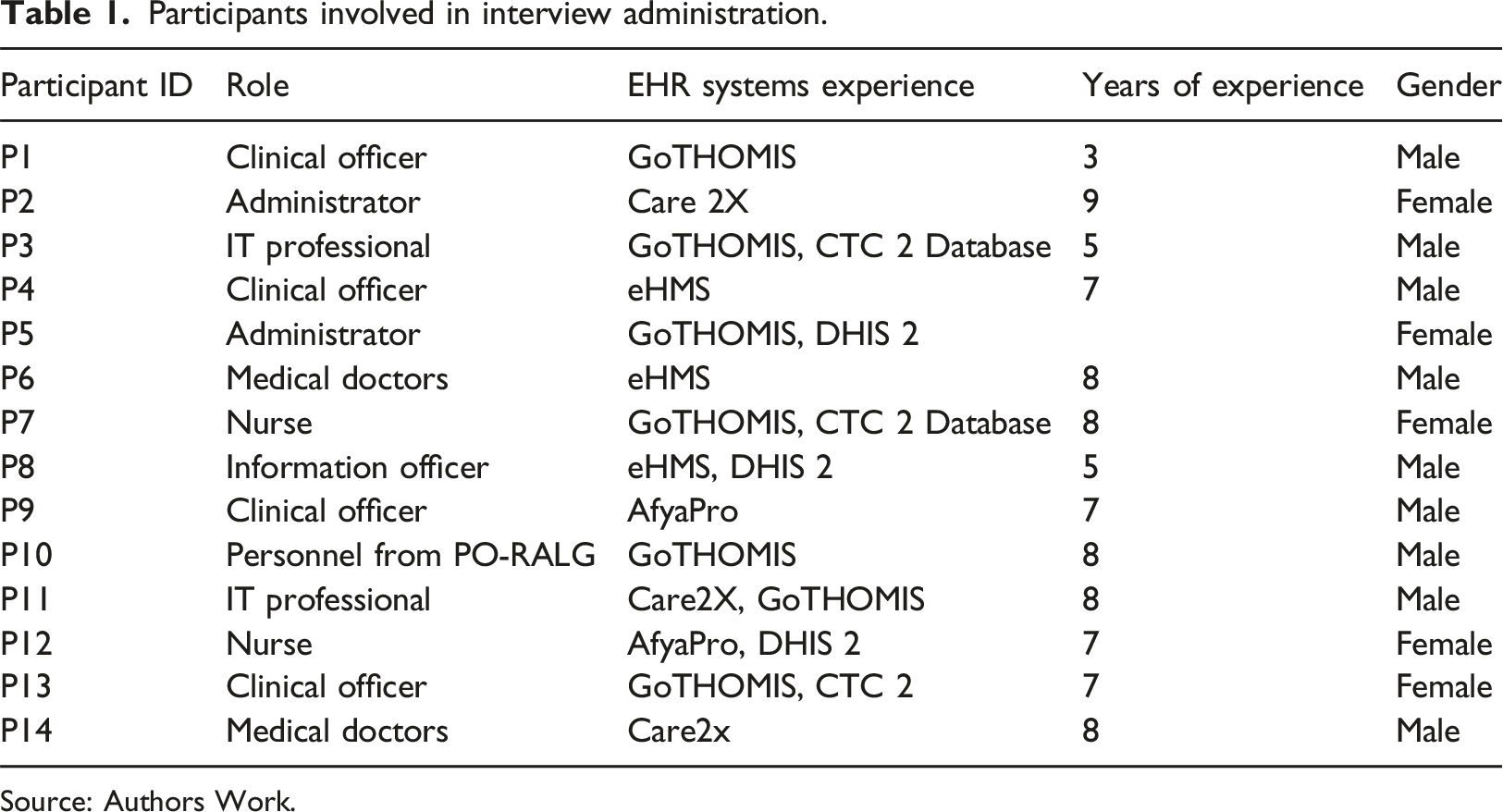
Source: Authors Work.
Data collection methods
Data for this study were collected using semi-structured interviews and document analysis. The semi-structured interviews were designed to explore participants’ experiences with implementing EHR systems in PHC facilities. This method allowed for a flexible yet focused discussion, ensuring key themes were covered while enabling participants to share additional insights relevant to their experiences.
The interview guide was developed based on a thorough review of existing literature on EHR system implementation and consultations with experts in healthcare informatics. It included open-ended questions to encourage participants to elaborate on the barriers they encountered and suggest possible solutions. Key topics included organisational readiness, cultural attitudes towards technology, technical challenges, and leadership support.
Interviews were conducted primarily in Kiswahili, with some in English, depending on participants’ preferences. They were held face-to-face whenever possible, fostering rapport and direct interaction. In cases where face-to-face interviews were not feasible, phone and video calls were used as alternatives. All interviews were audio-recorded with the participant’s consent and supplemented by detailed notes taken by the interviewer. Each interview lasted between 45 and 60 min, ensuring depth while respecting participants’ time constraints. After each interview, the audio recordings were transcribed verbatim. Interviews were conducted in Kiswahili and English, depending on participants’ preferences. Kiswahili interviews were translated into English by bilingual researchers. Moreover, a back-translation process was employed to ensure accuracy and minimise translation-related biases. This step involved translating the English transcripts back into Kiswahili to verify consistency in meaning and interpretation.
In addition to interviews, document analysis was conducted to gather background information on the healthcare facilities and their EHR systems. Documents reviewed included implementation reports, training manuals, and technical guidelines for EHR systems used within the PHC facilities. This secondary data complemented the interview findings, helping to contextualise the implementation challenges and identify potential solutions.
Data analysis
Following the six-phase process outlined by Braun and Clarke, 28 thematic analysis was used to analyse the data. The process began with familiarisation, where interview transcripts were read multiple times to gain a deep understanding of the content. Initial notes were taken to capture early impressions and potential patterns. Next, the transcripts were systematically coded using NVivo software, with an inductive approach allowing codes to emerge directly from the data. The table in Appendix A provides examples of how specific interview extracts were translated into meaningful codes, helping structure the emerging themes. Relevant segments were labelled with codes, and this process was repeated to ensure thoroughness. In the third phase, the initial codes were grouped into potential themes, with attention to identifying broader patterns related to barriers to EHR implementation. These themes were then reviewed and refined by examining all coded data extracts to ensure consistency and coherence. Themes were adjusted or merged as necessary, and weak themes were redefined or discarded. Once finalised, themes were defined and named to reflect their essence, with detailed descriptions explaining their relevance to the research questions. The final phase involved producing a narrative that linked the themes to the study’s objectives, supported by direct quotes from participants to provide a rich account of the findings.
Validity and reliability
Data triangulation was used to collect information from various stakeholders, including healthcare providers and IT professionals. Member checking was conducted by sharing the interview transcripts and themes with participants for feedback and verification, ensuring their views were accurately represented. Furthermore, using bilingual researchers helped reduce the risk of translation-related biases. Interviews conducted in Kiswahili were translated into English and back-translated to ensure accuracy. Researcher reflexivity was maintained throughout the study to acknowledge and mitigate potential biases.
Ethical considerations
Ethical approval for the study was obtained, and all participants were provided with information about the study and informed consent before participating in interviews. The consent process included assurances that participants’ identities would remain confidential and that they could withdraw from the study without penalty. No financial compensation was provided, but participants were thanked for their time and contributions. Anonymity was ensured by de-identifying interview transcripts and securely storing all research data.
Results
Codes and themes
The findings of this study are based on a thematic analysis of the qualitative data collected from healthcare professionals in Tanzanian PHC facilities. The analysis revealed several key themes representing barriers to the effective implementation of EHR systems. The word cloud in Figure 2 provides a visual representation of the most common terms and challenges mentioned by participants. Words that appeared more frequently in the interviews, such as “workload,” “incentives,” “downtime,” “network,” and “system,” are more prominent in the word cloud, indicating their prominence in the discussion of barriers to EHR implementation. A word cloud diagram of frequent keywords Source: Authors Work.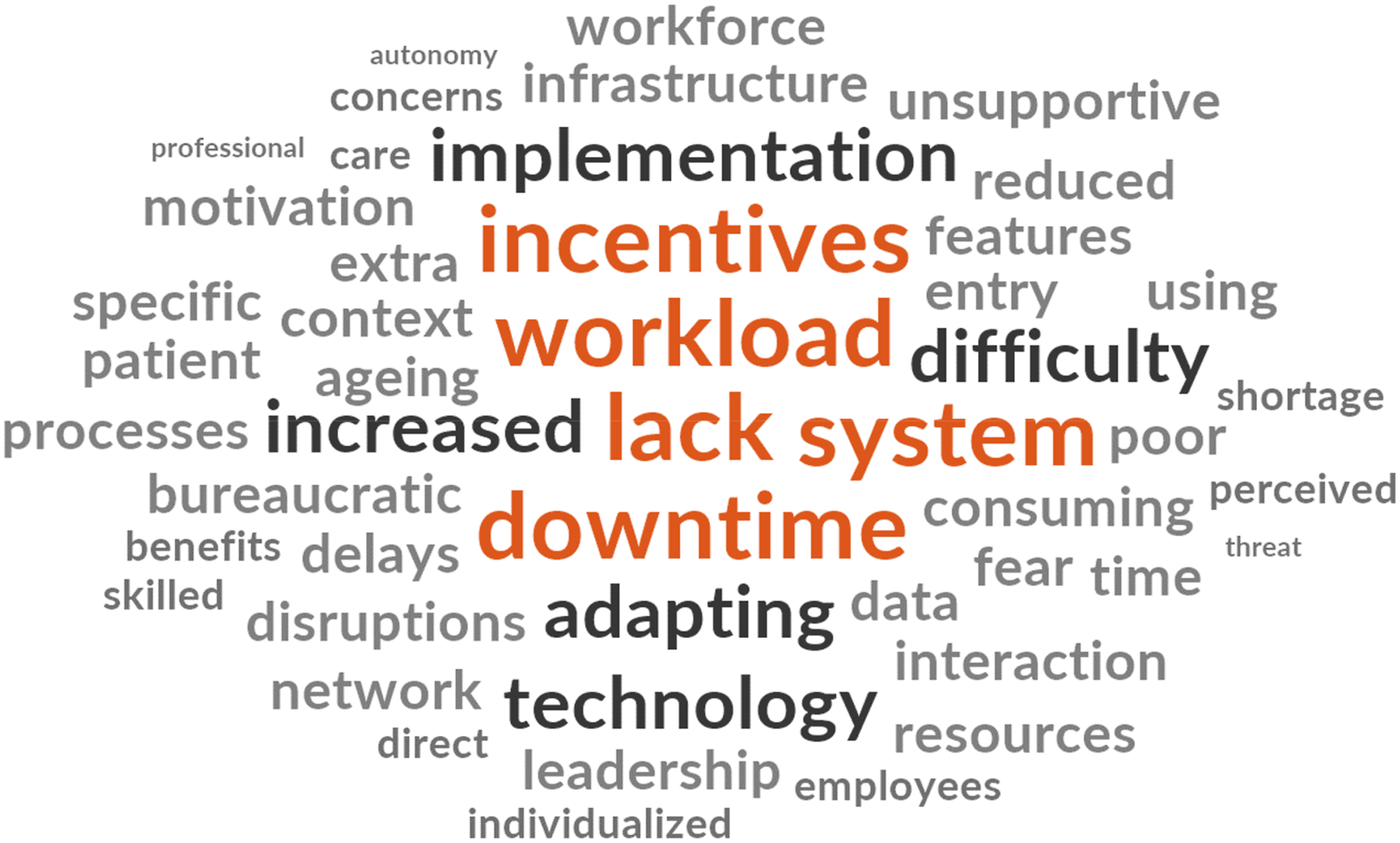
Codes and themes.
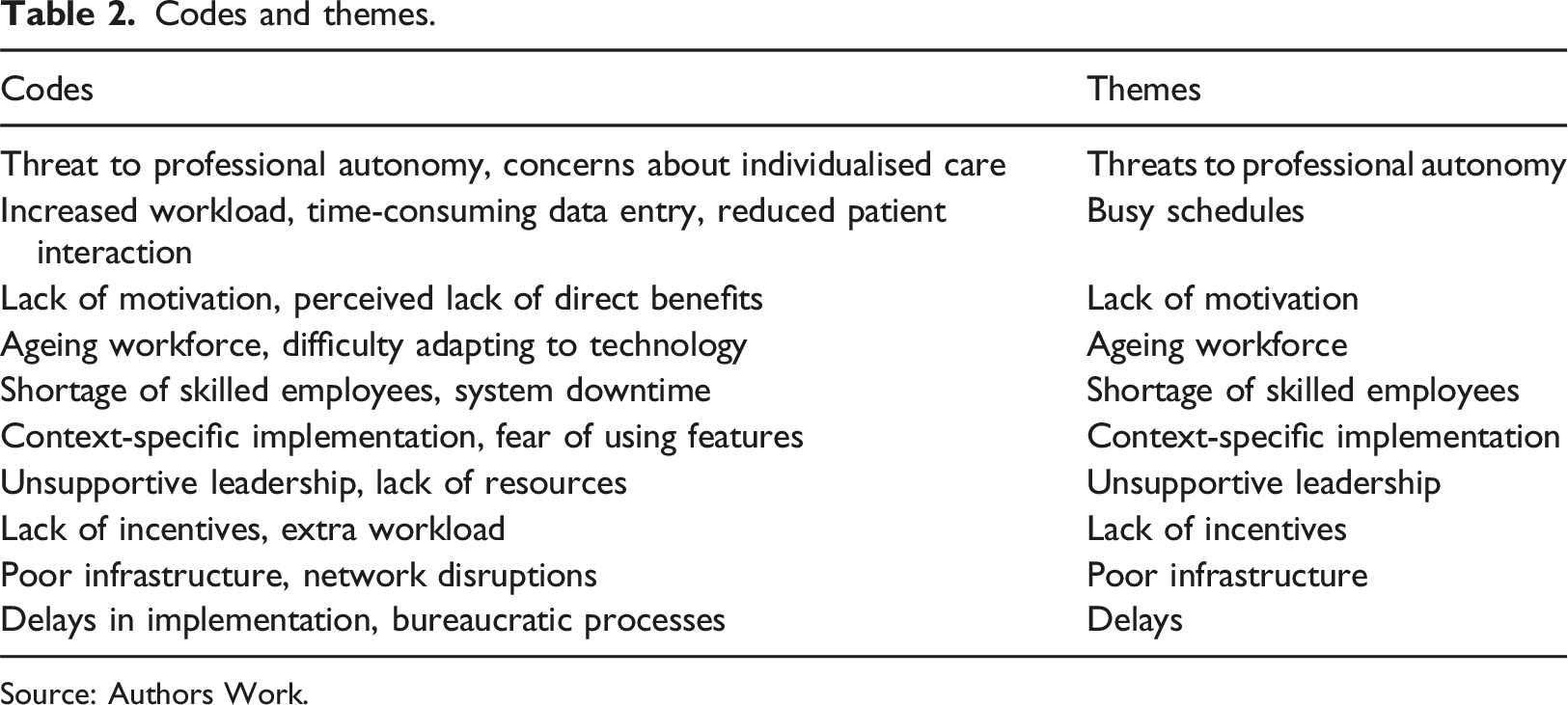
Source: Authors Work.
Barriers to EHR system implementation in PHC facilities in Tanzania
Summary of identified barriers to EHR system implementation.
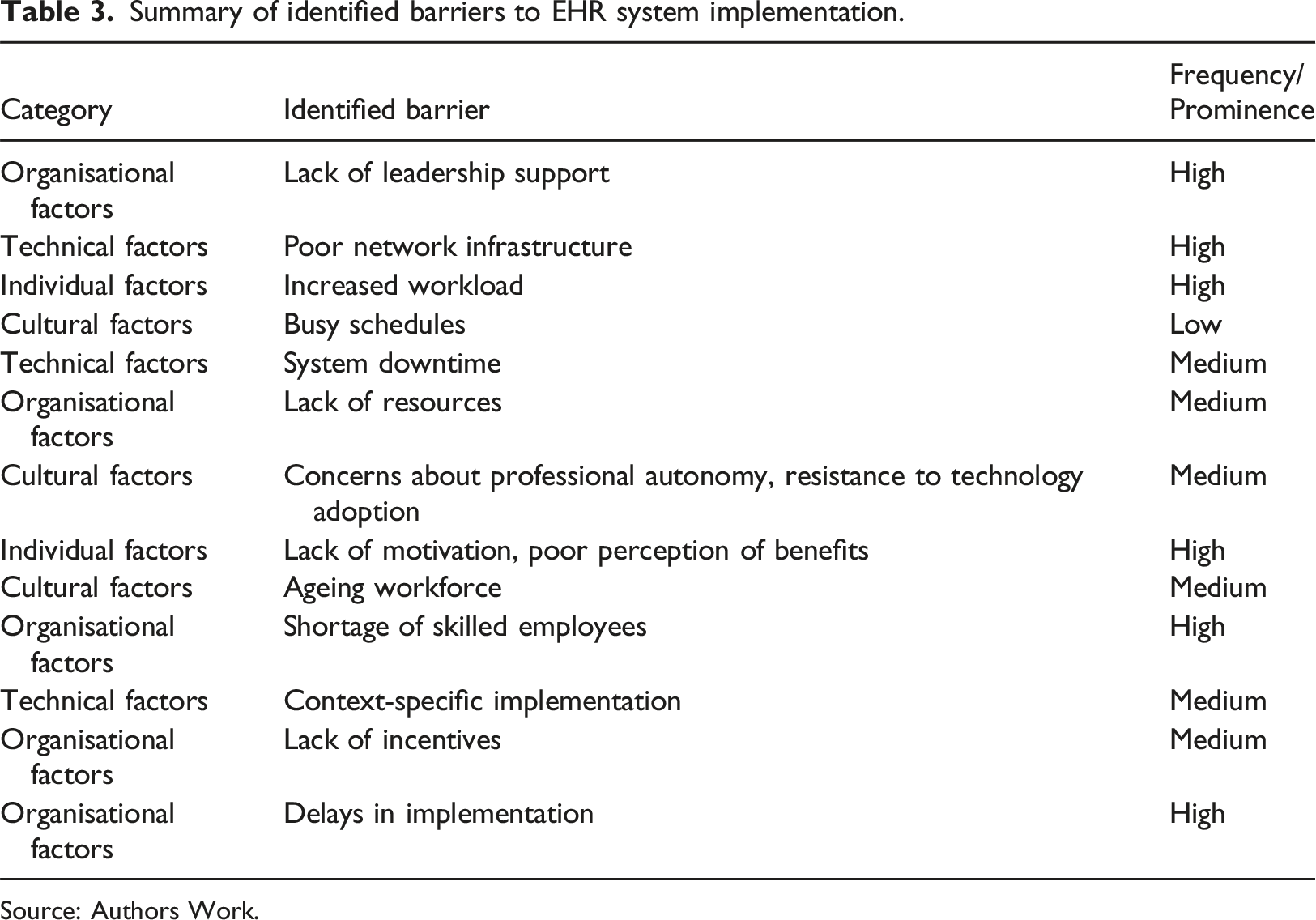
Source: Authors Work.
Cultural factors
Threats to professional autonomy
Several healthcare professionals expressed concerns about EHR systems’ limitations on their clinical autonomy. A clinical officer from a public PHC facility remarked, “While the system seems beneficial for record-keeping, I worry that it makes physicians redundant. Does it mean we won’t need to make clinical decisions anymore?” Similarly, another clinical officer in a rural public health facility emphasised, “These systems sometimes take away our ability to provide individualised care. The system that we have here forces you to stick to what it directs you to do. Otherwise, you won’t proceed with the treatment. You can’t prescribe medication that is not on the list to a patient.”
This sentiment reflects a broader concern that reliance on EHR systems could lead to standardised care at the expense of personalised treatments, potentially reducing the quality of care and patient outcomes. A rigid system prioritising structured data input over clinical judgment may limit healthcare providers’ ability to adapt treatments based on individual patient needs. 29 Research suggests that fostering greater flexibility in EHR systems can help mitigate this issue, enhancing clinical decision-making and patient outcomes. 30
Ageing workforce
The ageing healthcare workforce in Tanzania poses significant challenges to implementing new technologies. A senior nurse from a private facility expressed frustration, saying, “I have been in this profession for 30 years, and learning a new system at this age is difficult. My eyes hurt from staring at the screen, and the training was too fast for me to keep up.” Another respondent, a doctor nearing retirement, laughed as they stated, “We are close to the end of our careers. These new systems are more suited for the younger generation.”
This lack of familiarity and comfort with digital systems can create bottlenecks in healthcare delivery, as tasks that EHR systems should streamline instead become time-consuming and error-prone. 31 Training programs personalised to the needs of older healthcare workers, including slower-paced and continuous training, can alleviate this issue and improve the overall efficacy of EHR systems, leading to better patient outcomes. 32
Individual factors
Lack of motivation
Another common theme among healthcare professionals was the lack of perceived benefits from using EHR systems. A male clinical officer from a public PHC facility remarked, “I don’t see how entering this data benefits me or my patients. It feels like extra work for administrative purposes…..This system benefits the government in collecting revenues” Another participant, an old age medical doctor from a district hospital, commented, “Motivation is low because the advantages of these systems haven’t been communicated effectively to us. It’s just another task added to our day.”
When healthcare workers do not see the value of EHR systems in improving patient care, they may not use them consistently, leading to incomplete data entry and poor clinical decisions. 33 Furthermore, a lack of motivation could cause delays in patient care, as professionals may prioritise other tasks over updating or consulting the system. 30 Communicating the benefits of EHR systems for improving decision-making and care efficiency can help motivate healthcare workers, leading to more consistent system use and, ultimately, better patient outcomes. 34
Increased workload and busy schedules
Participants highlighted the challenge of increased workload, particularly the time-consuming nature of data entry. A female doctor from an urban PHC stated, “We’re already overwhelmed with patients, and now we must type out everything instead of writing with a pen, which I see that it is much quicker. It’s slower and takes time away from patient care.” Another clinical officer from a peri-urban facility echoed this sentiment, noting, “Our workload is too much to accommodate detailed data entry into the system. It’s difficult to find time to enter data accurately without rushing through it.”
The increased time required for data entry detracts from direct patient care, reducing the time healthcare professionals can spend with patients, which can compromise the quality of care provided. 35 This challenge is compounded in busy environments, where professionals must choose between completing detailed records or providing timely care. Studies suggest that optimising EHR system interfaces to reduce the time required for data entry can help mitigate these issues and improve patient care efficiency. 36
Lack of incentives
A healthcare administrator from a public PHC facility expressed dissatisfaction with the lack of recognition for effectively using the system: “There are no incentives for us to use the system properly. It just feels like more work for the same pay.” Another participant from a private PHC facility added, “We are expected to do extra work without any reward, not even public recognition. It is hard to stay motivated without any form of compensation.”
Without appropriate rewards or recognition, healthcare professionals may not prioritise EHR system use, which can result in inconsistent or inaccurate data recording. 37 This can negatively impact patient outcomes, as incomplete or delayed data can hinder clinical decision-making. Offering both financial and non-financial incentives, such as public recognition or opportunities for career advancement, can encourage more consistent use of EHR systems, leading to improved data accuracy and better healthcare delivery. 38
Organisational factors
Shortage of skilled employees
Another significant obstacle to implementing EHR systems was the shortage of skilled personnel to operate and maintain the systems. Several healthcare professionals voiced concerns over the inadequacy of the workforce’s knowledge and experience, leading to frequent disruptions in system use. A clinical officer from a public district hospital shared their frustration, stating, “We have a problem with the experts for this system. For instance, when an issue arises, we are told the expert is from the district council, but it feels like there’s only one person managing everything at the council. It often means we must stop using the system until they can come.” A clinical officer from a peri-urban health facility further explained, “The lack of on-site support is a big issue. When the system fails, it can take days or even weeks to get it back online, depending on how quickly the expert from the district can come over. Meanwhile, we are forced to revert to paper records, adding more confusion.”
This lack of skilled personnel leads to frequent disruptions in EHR system use, which delays patient care and increases the reliance on paper records. 39 A shortage of on-site support can extend these delays, especially when systems are down for extended periods. 40 As a result, patient outcomes may suffer due to delayed diagnoses, treatment, or data access. Investing in local IT support and training existing staff can reduce these disruptions, allowing healthcare providers to deliver more timely and effective care. 41
Unsupportive leadership
A participant from a public health facility voiced frustration over the lack of leadership support, stating, “Our management doesn’t prioritise the EHR system. They expect us to use it without providing the necessary resources or training. We’re left to figure it out on our own. Here, we only have one office with computers, outdated ones with limited functionality” Another healthcare worker from a rural PHC facility explained, leadership here is focused on other priorities, and they don’t see the potential of EHR systems to improve patient care. Without their support, the system sits there unused.”
EHR systems may not receive the attention or resources required for successful implementation without adequate leadership support. This lack of support can create an environment where healthcare workers feel unmotivated to use the system, ultimately reducing system adoption and usage. 42 Leadership involvement is critical in ensuring the necessary infrastructure, training, and resources are in place, which can directly impact the system’s effectiveness in improving healthcare delivery and patient outcomes.
Delays in implementation
An administrator from a public healthcare facility in an urban area shared, “We had to wait for months just for the procurement process to be finalised, which delayed the entire implementation. By the time everything was approved, we were already behind schedule.” A healthcare worker from a rural PHC facility added, “In our case, the system installation was delayed because of budget constraints and logistical issues. It was frustrating because we were prepared to start using the system but couldn’t proceed due to these delays.”Another respondent from PO-RALG highlighted the issue of bureaucratic delays: “We face many hurdles in procurement and the approval process, which has caused significant delays in implementing EHR systems. This ultimately affects service delivery in our facilities.”
Such delays create gaps in care coordination and information sharing, leading to inefficiencies in healthcare delivery. In rural or under-resourced areas, these delays can have severe implications for patient outcomes, as healthcare providers rely on timely access to patient data for accurate diagnosis and treatment. Streamlining bureaucratic processes and expediting procurement can reduce delays, allowing systems to be deployed more rapidly and effectively. 43
Technical factors
Context-specific implementation
A clinical officer from a rural PHC facility stated, “This system doesn’t fit our needs here. We are unsure what some features do and are afraid to use them because we might break something.” An IT professional from a health centre added, “The system seems designed for larger hospitals, but these health practitioners need something simpler. There are too many features they don’t need, making the system more confusing for these non-IT people at the facility.”
This mismatch between the system’s design and the facility’s needs leads to the underutilisation of EHR systems, limiting their potential benefits for patient care. Adapting EHR systems to healthcare facilities’ specific cultural and clinical contexts is essential for ensuring that they support rather than hinder healthcare delivery. 42 Context-specific implementations allow for greater ease of use, which improves system adoption and ultimately enhances patient outcomes.
Poor network infrastructure
A healthcare administrator from a public district hospital lamented, “The system goes down frequently, and when it does, we have to revert to paper records. What’s the point of having a system if it’s so unreliable?”. This was supported by a nurse working at the reception in a rural dispensary: “The network connectivity is unreliable, often experiencing disruptions ……. Moreover, there are instances where the NHIF server is inaccessible, creating even more difficulties, especially towards the end of the month.” This sentiment was echoed by an IT professional from a peri-urban PHC facility who noted, “The network disruptions are constant, especially during busy times. At the end of the month, when patient volumes increase, it becomes impossible to log in to the system because of the outdated network infrastructure.” Another IT personnel from a rural district hospital echoed this: “We made installations almost all over the hospital while we did not have cash… It was supposed that the push we used there should have ended somewhere. When we get other funds, we call the IT personnel and move us a step. As a result, the LAN was installed in most facility areas due to the initial push, but the system was only used on a few existing computers.”
Inconsistent network connectivity leads to frequent disruptions in EHR usage, making it difficult for healthcare providers to access patient data when needed. This affects the continuity of care, as healthcare providers may be unable to make informed decisions based on real-time data. Strengthening network infrastructure is vital to ensure that EHR systems are reliable and that healthcare providers can access the information they need to make timely and accurate decisions. 44
System downtime
Healthcare professionals repeatedly cited system downtime as a significant barrier. An IT professional from a public PHC facility noted, “Whenever the system is down, we have no choice but to revert to paper records. This creates confusion, making it difficult to sync everything back once the system is up.” A clinical officer from a peri-urban facility added, “We face a lot of technical issues with the system, and it sometimes takes hours for IT support to arrive. During that time, we cannot use the system.”
Frequent downtimes disrupt workflows and compromise patient care by delaying access to essential patient information. The manual transfer of data between paper records and EHR systems during downtimes also introduces opportunities for errors, which can negatively affect patient outcomes. 45 Implementing backup systems and improving technical support can minimise downtime, ensuring healthcare providers have continuous access to patient information for better decision-making and care delivery.
Figure 3 provides a bar chart illustrating the frequency of each identified barrier to EHR implementation. This chart offers a more precise visual representation of the most commonly mentioned barriers. Frequency of identified barriers to EHR system implementation.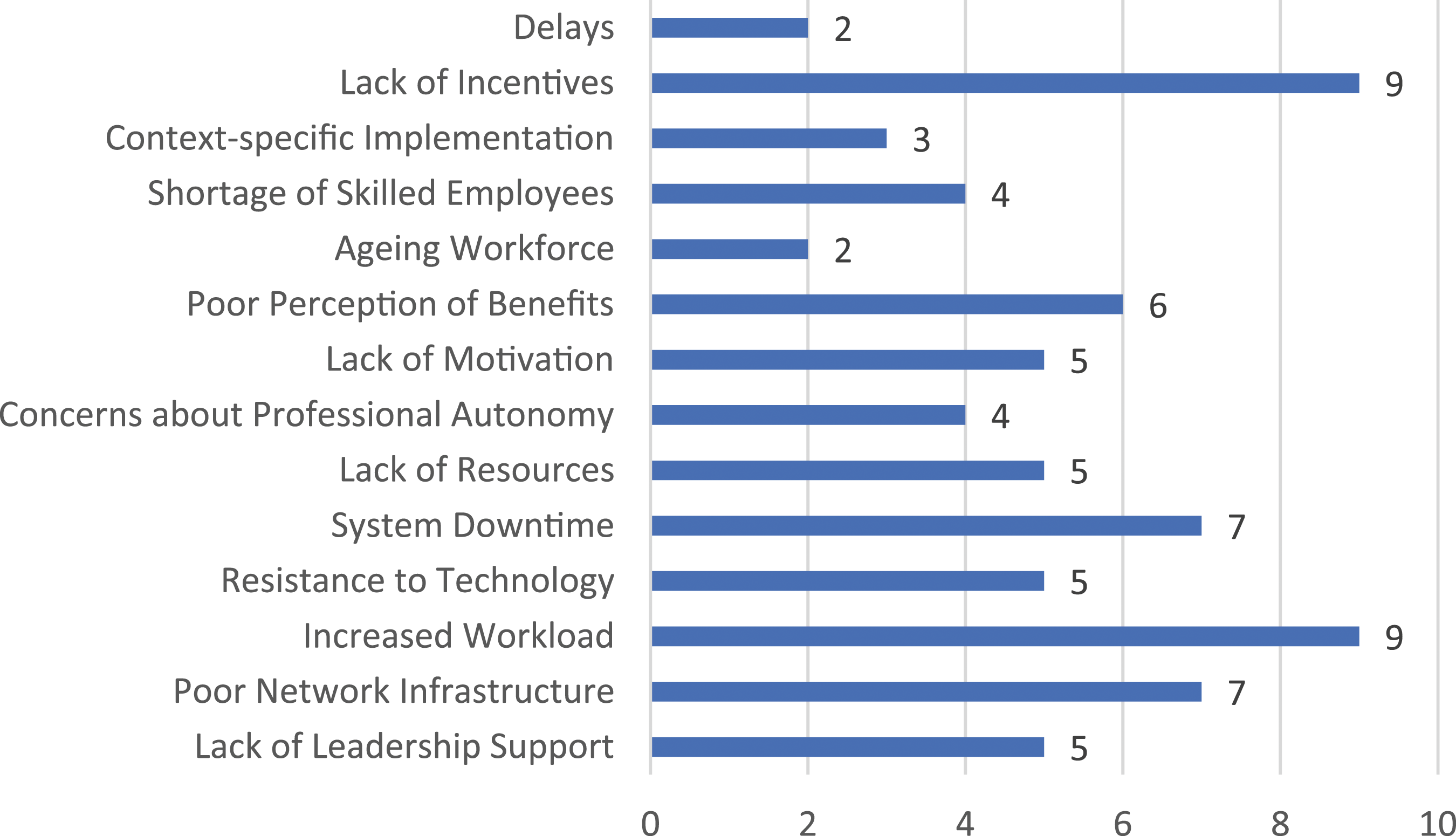
Discussion
This study explored the barriers to implementing EHR systems in PHC facilities in Tanzania, drawing insights from healthcare professionals and stakeholders. The findings revealed that various organisational, technical, individual, and cultural factors hinder effective EHR implementation. To fully understand these barriers, the study’s findings are interpreted through the lens of DOI theory, TAM, and Sociotechnical Systems theory.
The DOI theory provides an essential framework for understanding why the implementation of EHR systems in Tanzanian PHC facilities has been slow. In this study, healthcare workers expressed concerns about the lack of clear relative advantage of EHR systems, particularly the perception that these systems increased their workload without offering noticeable improvements in patient outcomes. This aligns with the findings of Gesulga et al., 6 who identified similar perceptions in developing countries where healthcare workers viewed EHR systems as adding administrative burdens rather than facilitating clinical tasks. DOI theory posits that for an innovation to be adopted, its benefits must be readily apparent to users. 16 In this case, the lack of perceived advantage highlights a critical barrier that needs to be addressed through a clearer demonstration of the systems’ benefits for improving clinical efficiency and decision-making.
The complexity of EHR systems also emerged as a significant barrier, especially for older and less tech-savvy healthcare workers. This issue is echoed in previous studies, such as that by Kruse et al., 9 which identified technological complexity as a common barrier to EHR systems implementation in low-resource settings. According to DOI, the more complex a system appears, the less likely it is to be implemented. The participants in this study reported that the EHR systems were difficult to navigate, leading to frustration and delays in workflow. This finding underscores the need for simplification of system interfaces and more accessible training programs, as suggested by Weir et al., 30 who advocate for user-centred design to make health technologies more intuitive and less burdensome for healthcare workers.
Furthermore, compatibility between EHR systems and existing workflows was a recurring theme. Participants noted that EHR systems often disrupted their established routines, leading to inefficiencies. This finding aligns with the research of Palabindala et al., 15 who found that EHR systems are often incompatible with existing clinical workflows, particularly in resource-limited settings where healthcare workers are already overburdened. DOI theory highlights the importance of alignment between innovations and users’ established practices.16,46 Customising EHR systems to better fit the workflows of Tanzanian healthcare workers would likely improve their compatibility and facilitate greater adoption.
TAM also provides critical insights into the barriers identified in this study. According to TAM, users’ acceptance of technology is influenced by their perceptions of its usefulness and ease of use.17,47,48 In this study, healthcare workers did not perceive EHR systems as particularly useful in improving patient care or their daily tasks. Similar concerns were found in a study by Cho et al., 49 which revealed that healthcare professionals in low-resource settings often fail to see the value of EHR systems, viewing them as tools primarily for administrative purposes rather than for enhancing clinical decision-making. To address this, it is essential to communicate the direct benefits of EHR systems to healthcare workers, demonstrating how these systems can improve clinical outcomes and streamline patient care.
Moreover, the study found significant challenges related to the ease of use of EHR systems. Participants reported difficulties in operating the systems due to inadequate training and technical support. This mirrors the findings of Kruse et al., 50 who noted that in many developing countries, the lack of proper training and the complexity of EHR systems discourage healthcare professionals from adopting them. TAM suggests that perceived ease of use is a critical factor in determining whether a technology will be embraced. Simplifying the design of EHR systems, along with providing more comprehensive and continuous training, would likely improve healthcare workers’ acceptance of the technology.
Sociotechnical Systems theory emphasises the interaction between social and technical factors in successfully implementing technologies. This study revealed that the lack of skilled personnel to support EHR systems was a main barrier, especially in rural areas. The findings echo those of Layman, 51 who highlighted the need for robust human resources to support health IT systems in low-resource settings. The theory underscores that technologies must be supported by adequate technical infrastructure and human resources to function effectively. 52 Addressing this shortage requires building local capacity through training programs for healthcare workers and IT professionals, ensuring that systems can be effectively maintained and supported.
The findings also suggest that leadership support plays a crucial role in the success of EHR implementation. Participants noted that the lack of leadership commitment and prioritisation hindered the effective use of EHR systems. This aligns with previous research by Alanazi, 53 who argued that strong leadership is essential for driving the adoption of new technologies in healthcare settings. Leadership support not only facilitates the allocation of resources but also fosters a culture of change within healthcare organisations. Sociotechnical theory emphasises that successful technology adoption requires alignment between technological systems and the social and organisational context in which they are implemented. 21 Engaging healthcare leaders and holding them accountable for the success of EHR implementation could help overcome this barrier.
Culturally, healthcare workers in this study expressed concerns about losing professional autonomy, fearing that EHR systems might limit their ability to make clinical decisions. Similar sentiments were found in the work of Brunner et al., 54 who documented resistance to EHR systems among healthcare workers who felt that the technology imposed rigid structures that conflicted with their clinical judgment. This cultural resistance reflects the broader social dynamics that must be considered when implementing health IT systems. Sociotechnical Systems theory highlights the importance of aligning technology with the values and practices of its users. Customising EHR systems to preserve clinical autonomy while supporting decision-making processes could help reduce resistance and enhance adoption.
The implications of this study span practical, theoretical, and policy dimensions, providing valuable insights for improving the implementation of EHR systems in Tanzanian PHC facilities. The study emphasises the need for context-specific solutions to overcome the barriers to EHR system implementation in Tanzanian PHC facilities. By addressing key challenges like poor infrastructure, inadequate leadership support, and increased workloads for healthcare workers, a clear roadmap for improving adoption and use is provided. Enhancing system usability and infrastructure will streamline workflows, allowing healthcare workers to focus more on patient care and improve outcomes. Continuous training and capacity building for IT support will further ensure long-term system sustainability, while customising EHR systems to meet local needs will reduce resistance and increase user satisfaction, particularly in resource-limited settings.
On a theoretical level, the study contributes to the understanding of health information systems by integrating DOI theory, TAM, and Sociotechnical Systems theory. It extends DOI by stressing the importance of aligning innovations with local cultural and workflow practices, addressing concerns about autonomy and workload. Without this alignment, even beneficial innovations like EHR systems may face resistance. The study also highlights the need for sociotechnical interaction, where technical infrastructure and social context, including leadership support, are vital for successful technology adoption in resource-limited environments like Tanzania.
The study’s findings have several important policy implications, particularly for the digitalisation of healthcare systems in Tanzania. Policy interventions should prioritise infrastructure investment, especially in rural areas, to provide the foundation for EHR systems. Leadership development programs are also crucial to ensure accountability and support for health IT projects. Moreover, financial and non-financial incentive structures are needed to encourage healthcare workers to adopt EHR systems consistently. Lastly, policies focused on standardisation and interoperability will enhance data management and care coordination across healthcare facilities, paving the way for more widespread and effective adoption of EHR systems.
While this study provides significant insights, several limitations should be noted. The qualitative nature of the research limits the generalizability of the findings to other settings. Moreover, the sample size, although sufficient for achieving saturation, may not fully represent the diversity of experiences across Tanzania’s PHC facilities. Moreover, the study focuses primarily on the barriers to EHR implementation rather than potential success stories or best practices in Tanzanian PHC facilities. Future research could expand the scope to include facilities where EHR systems have been successfully implemented, offering lessons that could be applied more broadly across the country.
Future research should focus on conducting longitudinal studies to track the long-term impact of EHR system implementation on patient outcomes and healthcare delivery. Expanding the research to other regions of Tanzania, including those with varying resource levels and healthcare structures, could provide a more comprehensive understanding of the barriers and facilitators to EHR adoption. Besides, further studies should investigate the role of incentives and policy changes in driving greater adoption of EHR systems among healthcare professionals. Research into customising EHR systems to meet Tanzanian healthcare workers’ specific cultural and clinical needs would provide valuable insights into overcoming the identified barriers.
To enhance their reliability, future research should prioritise developing, validating, or pilot-testing data collection instruments, such as interview guides. In this study, the semi-structured interview guide was not formally validated, which is acknowledged as a limitation. Validating future instruments will ensure that the tools used for data collection are robust and applicable across different settings, providing more reliable and generalisable findings.
Conclusion
This study has provided in-depth insights into the barriers hindering the effective implementation of EHR systems in Tanzanian PHC facilities. The findings indicate that organisational, technical, individual, and cultural factors contribute to these challenges. Among the most significant barriers are a lack of leadership support, poor network infrastructure, increased workload for healthcare workers, and resistance to technology adoption, particularly concerns about the loss of professional autonomy.
By examining these barriers through the lenses of DOI theory, TAM, and the Sociotechnical Systems Theory, the study has identified critical points where interventions can be made to improve EHR systems implementation. To move forward, a comprehensive approach is required to address the technical deficiencies in infrastructure and system usability and consider the social and organisational factors that influence healthcare professionals’ engagement with EHR systems.
This study contributes to the growing body of literature on health information systems in resource-limited settings. It offers practical insights for policymakers, healthcare leaders, and technology developers working to improve healthcare delivery in Tanzania.
Recommendations
Based on this study’s findings, the following practical steps, supported by insights from existing literature, are proposed to address the barriers to EHR implementation in Tanzanian PHC facilities.
Strengthening leadership support
Leadership plays a pivotal role in the successful implementation of EHR systems. Studies have shown that strong leadership is essential for driving organisational change and ensuring technology adoption.13,54,55 To address the lack of leadership support identified in this study, healthcare leaders should receive targeted training programs highlighting EHR systems’ importance for improving clinical decision-making and operational efficiency. Such training programs should also emphasise the role of leaders in creating a supportive environment for EHR adoption, which has been identified as a key success factor in other contexts.55–57 Moreover, leaders should be held accountable for the progress of EHR implementation through structured evaluation frameworks, aligning with findings from Regan and Wang, 58 who emphasise the need for leadership accountability in health IT projects.
Building technical infrastructure
As noted in this study, a major technical barrier to EHR adoption in Tanzanian PHC facilities is the poor state of network infrastructure. Similar challenges have been identified in other low-resource settings, where inadequate infrastructure hinders the effective use of EHR systems. 6 To mitigate this, investments must be made to enhance network infrastructure in rural and peri-urban areas, ensuring reliable connectivity. Research by Nsaghurwe et al. 8 emphasises the importance of stable infrastructure for maintaining continuous system availability. In addition, it is crucial to establish on-site or remote IT support teams to promptly address system downtime, as delays in technical support have been linked to lower system adoption rates. 50
Promoting cultural change and professional autonomy
Healthcare professionals in this study expressed concerns over the potential loss of professional autonomy due to EHR systems, echoing findings from Weir et al. 30 and Kruse et al. 59 To address these concerns, it is essential to involve healthcare workers in the design and customisation of EHR systems, ensuring that the systems meet their clinical needs and preserve their decision-making autonomy. In line with TAM, perceived usefulness and ease of use are critical to technology adoption. 48 By adapting EHR systems to the specific requirements of Tanzanian healthcare professionals, it is possible to foster greater acceptance and reduce resistance. Furthermore, research by Elsyed et al. 32 and Xie et al. 60 highlights the need for personalised training programs, particularly for an aging workforce that may struggle with new technology. Providing additional training sessions and ongoing support can help healthcare professionals feel more confident in using EHR systems.
Reducing workload and enhancing usability
The increased workload associated with EHR systems was a recurring theme in this study, with healthcare workers feeling burdened by the time-consuming data entry process. Similar challenges have been identified in other studies, such as those by Olson et al. 36 as well as Kataria and Ravindran, 1 where healthcare professionals highlighted the inefficiencies of EHR systems in busy clinical environments. To address this, EHR systems should be optimised for usability, reducing the time required for data entry and minimising workflow disruptions. This could be achieved through user-centred design approaches that streamline the interface and incorporate automation tools, such as voice recognition, as Jedwab et al. 61 suggested. In addition, reconfiguring clinical workflows to integrate EHR use better can help reduce the administrative burden on healthcare workers, enabling them to focus more on patient care.
Creating incentives for EHR system usage
Lack of motivation and incentives for using EHR systems was identified as a key barrier in this study. Similar findings have been reported in the literature, with healthcare professionals often feeling that EHR systems add to their workload without offering direct benefits. 5 To overcome this, healthcare workers should be provided financial and non-financial incentives to encourage the effective use of EHR systems. Incentives could include performance-based bonuses, public recognition, or opportunities for professional development, as suggested by research on motivating healthcare workers in low-resource settings. 15 Moreover, continuous learning opportunities that demonstrate the tangible benefits of EHR systems for clinical decision-making and patient outcomes can help increase motivation, as highlighted by Jedwab et al. 61
Facilitating continuous evaluation and improvement
Lastly, continuous monitoring and evaluation are essential for ensuring the long-term success of EHR systems. Studies have shown that regular feedback loops, where user experiences are collected and systems are updated accordingly, are critical for the sustained adoption of health technologies. 62 In this context, it is recommended that Tanzanian PHC facilities implement a monitoring framework to track EHR system performance, user satisfaction, and clinical outcomes. This will allow for timely adjustments and improvements, addressing any emerging issues before they become significant barriers. Furthermore, piloting new EHR solutions in select facilities before nationwide rollout can provide valuable insights, enabling the system to be refined and optimised for broader implementation.58,63
Supplemental Material
Supplemental Material - Unveiling barriers to EHR implementation for effective decision support in tanzanian primary healthcare: Insights from practitioners
Supplemental Material for Unveiling barriers to EHR implementation for effective decision support in tanzanian primary healthcare: Insights from practitioners by Augustino Mwogosi, Stephen Kibusi in Health Informatics Journal.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to the healthcare professionals and administrators who participated in this study for their valuable insights and time. We also extend our thanks to the healthcare facilities’ leadership, whose support made this research possible. Lastly, we acknowledge the University of Dodoma for providing the necessary resources and institutional support throughout the research process.
Author Contributions
• Augustino Mwogosi: Conceptualization, methodology, data collection, analysis, and manuscript drafting. • Stephen Kibusi: Supervise, refine methodology, and revise the manuscript critically.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.