
Abstract
More evidence is needed on technology implementation for remote monitoring and self-management across the various settings relevant to chronic conditions. This paper describes the findings of a survey designed to explore the relevance of socio-demographic factors to attitudes towards connected health technologies in a community of patients. Stroke survivors living in the UK were invited to answer questions about themselves and about their attitudes to a prototype remote monitoring and self-management app developed around their preferences. Eighty (80) responses were received and analysed, with limitations and results presented in full. Socio-demographic factors were not found to be associated with variations in participants’ willingness to use the system and attitudes to data sharing. Individuals’ levels of interest in relevant technology was suggested as a more important determinant of attitudes. These observations run against the grain of most relevant literature to date, and tend to underline the importance of prioritising patient-centred participatory research in efforts to advance connected health technologies.
Keywords
Introduction
There is a growing consensus amongst health care professionals, patients and the public that connected health interventions for remote monitoring and self-management of chronic conditions (like the use of mobile, wearable and other ubiquitous technologies) may improve health outcomes, reduce pressure on the healthcare system and empower patients to take better control of their own health data and ultimately their own health. 1 The importance and potential of connected health interventions has been enhanced in the current Covid-19 pandemic, for example having profound implications for the way care is delivered to patients. 2
Despite the opportunity that modern connected health technologies can offer patients, there are also the dangers of unintended consequences, including infringement of privacy and accentuation of social inequalities due to data protection vulnerabilities and/or lack of wide availability, usability and access.3,4 These dangers are of particular concern when they involve the most vulnerable members of our society, such as the elderly, deprived and people with lower digital literacy. 5 To increase the uptake and impact of such technology-driven interventions, it is important for any implementation strategy to be contextualized and translated to different needs. Understanding the role that different socio-demographic factors can have on patients’ perceptions and attitudes towards the use of these technologies can help move beyond assumptions that one size fits all by targeting the needs and characteristics of different groups. 6
Previous research has provided some evidence that the adoption and use of digital health interventions can be influenced by socio-demographic factors like age, education or deprivation. For example, it is relatively well documented that older people are more reluctant to engage with technology compared to the younger generation. 7 Research has also shown that age, education, deprivation and minority group membership are all significant predictors for access to and use of digital health information, with people who are older, less educated, have lower income and belong to a minority group being less likely to use this type of information. 8 Similar findings also seem to hold across a broad range of patient-facing digital health interventions, including patient portals 9 and social networking technologies. 10
However there is a debate as to whether this can be generalized across all types of digital health technologies. In the case of mobile apps, wearable health devices and text messaging for chronic condition self-management, the role of socio-demographic factors is still not clear. For example, a recent study 11 found that a majority of older adults were interested in using wearable health devices for tracking their health and sharing their data with health providers, challenging the stereotype that older people are negatively disposed towards health technology. It is clear that more methodologically robust research is needed to address this question. 6
Evidence on the role of socio-demographic factors in the adoption and use of connected health technologies by patients is scarce. There is evidence from controlled studies supporting the feasibility and acceptability of these types of technologies among patients, with positive effects on health outcomes.12,13 However there is no evidence outside the limits of a controlled study environment that helps us understand what are patients’ concerns, barriers and attitudes towards these technologies that could affect long term adoption and implementation strategies. This is important considering how diverse patients can be in terms of socio-demographic characteristics. Understanding the role of socio-demographic factors — particularly in relationship to willingness to use and attitudes towards data governance issues, where previous research has shown a growing debate among the public 14 — is important to: 1) help us develop translational strategies for implementing these technologies across a wide range of patient groups and maximise impact; and 2) avoid the risk of excluding certain groups of patients from the benefits that these technologies can offer.
The aim of the research reported in this paper was to present unique knowledge about the effect of different socio-demographic factors on the willingness of patients to use these technologies and share their health data. In particular, we focused on the use of these technologies in the context of cardiovascular conditions, like stroke, where there is a growing body of literature documenting their feasibility and positive effect on health outcomes.15–17 We concentrated on four socio-demographic factors (age, education, living conditions and disability), in line with previous research suggesting that these are the key predictors of technology use among patients. 8
The remainder of this paper is structured as follows. We firstly establish Definitions of the general meaning of “connected health system” and the specific instance of such a system used in this study. The next section explains the Methods we applied, including details on the development and implementation of the online survey questionnaire as well as on the analysis undertaken. The final two sections report the Results of our analysis and a Discussion of our findings.
Definitions
Caulfield and Donnelly introduced a popular definition of Connected Health in 2013: “Connected Health encompasses terms such as wireless, digital, electronic, mobile, and tele-health and refers to a conceptual model for health management where devices, services or interventions are designed around the patient’s needs, and health related data is shared, in such a way that the patient can receive care in the most proactive and efficient manner possible. All stakeholders in the process are ‘connected’ by means of timely sharing and presentation of accurate and pertinent information regarding patient status through smarter use of data, devices, communication platforms, and people”. 18
Connected health systems can harness the power of modern wearable and ubiquitous devices to integrate health data (from electronic health records) with fitness and other wellness data, both objectively measured and self-reported (e.g. electronic Patient-Reported Outcomes, ePROs). 19 Data collected can be reported back to patients using integrated visual screen-based interfaces (for monitoring) or processed by Artificial Intelligence (AI) algorithms to provide tailored health advice and recommendations (for self-management) to the individual patient’s needs.
As stated above, our particular interest for this study was stroke. This was motivated by expectations that stroke prevalence and associated health and care system costs in the United Kingdom are expected to rise rapidly in coming years, 20 and therefore presents as a leading example of the importance and urgency of delivering the connected health benefits mentioned at the outset.
The specific technology used in this study was a connected health system prototype developed as part of the CONSULT project, a health informatics research collaboration. The CONSULT project was motivated by evidence that involving patients in their care leads to better outcomes 21 . The project is exploring the feasibility of employing a collaborative decision support tool to help patients suffering from chronic diseases to self-manage their treatment plans, using the domain of secondary stroke prevention as an initial use case. More information on the CONSULT project is available at: https://consultproject.co.uk/.
The CONSULT system was developed and co-designed with Patient and Health Care Professionals (HCP) focus groups 22 , and includes a dashboard and a chatbot that were pilot-tested on healthy volunteers23, 24. The prototype system uses commercial wireless sensor devices that make it possible for patients to monitor a range of health and wellness data at home, including: blood pressure using a wireless cuff; and heart function using a smartwatch and a disposable ECG patch. It integrates data from these wellness sensors as well as ePROs with patient Electronic Health Records (EHRs), HCP input and clinical guidelines to produce a care plan that is tailored to the patient’s individual needs. As part of its engine, the system deploys argumentation, which is an AI approach to support reasoning about treatments and recommendations, to support dialogue-based interaction with patients and carers and ensure understanding of the health data and information gathered as well as decisions made25-28.
Methods
This study addressed the following research question: “Do stroke survivors’ willingness to use and attitudes to data sharing through self-management mobile health apps vary according to certain socio-demographic factors, and if so how?”
Our questionnaire, data and code has been made available alongside this paper, in a public repository at: https://github.com/kclconsult/remote-survey.
Design
The study team developed a survey questionnaire to address the research question. The study target group was identified as adult stroke survivors living in the UK. Anyone who had a stroke and was at least 18 years old could participate in the survey. No further inclusion or exclusion criteria were applied.
It was clear due to Covid-19 restrictions that online response would be the only feasible option. The survey was designed in Microsoft Forms. Questions were grouped into four sections, as follows: • Section 1: socio-demographic data about participants. • Section 2: familiarity with health technology. • Section 3: willingness to use the CONSULT system. • Section 4: attitudes to data sharing.
The contents of the questionnaire were phrased carefully using writing that corresponds to a US Grade 6 reading level (or Year 7 for England). To do this we used Microsoft Word’s “readability statistics” function. Piloting was undertaken to assess the readability of the questionnaire. The questionnaire was designed with the objective that it should take around 15 min to complete.
The items used in the questionnaire were not tested for reliability and internal validity beyond piloting for readability and extensive checking (for example, Section 4 against relevant language in the UK Data Protection Act 2018). However, the team was reasonably confident that the scales included would successfully measure the concepts under investigation.
The main challenge identified at the design stage was dependence for applicability and generalisability of the findings from this survey on reaching a large enough cohort of stroke survivors. A target sample was estimated in line with applicable heuristics at 125 participants. 29 Participants were eligible to enter a random prize draw for vouchers. Ethical approval was obtained through King’s College London (MRA-19/2019642).
Data collection
Participants were recruited using purposive sampling. CONSULT project partners and contacts were requested to disseminate a notice including a link to the survey, notably: Stroke Association; Different Strokes; South London Stroke Register; and King’s College London study recruitment circulars. The team also contacted local stroke groups directly using published contact details. Feedback received during data collection was used to augment reflections on study limitations (see below).
The survey was open to responses for 6 weeks and it was closed to participants on 15 December 2020. 80 responses were received. The collected survey data was processed (for example, standardising local authority identifiers). An anonymised version has been added to the public repository cited above.
Analysis
In line with the plan established at the design stage, our analysis involved the following steps:
• Analysis of sample characteristics, including comparison with South London Stroke Register (SLSR) summary statistics as the best-available data on socio-demographic characteristics of the general UK stroke survivor population.
• Primary analysis: Variations in participants’ willingness to use (Section 3) and attitudes to data sharing (Section 4) according to key socio-demographic factors (Age, Education, Living Conditions and Disability).
• Secondary analysis: Variations in participants’ willingness to use (Section 3) and attitudes to data sharing (Section 4) according to other covariates addressed (notably information about participants’ levels of familiarity with and interest in mobile health technology gathered in response to Section 2).
The data collected from this survey contained categorical variables only. When testing hypotheses of independence between the question of interest and covariates, χ2 or Fisher’s exact tests were used. 30 In almost all cases due to the sample size Fisher’s exact test was used. Where necessary we applied multiple comparison procedures to account for the number of covariates being tested, this was done by adjusting the significance threshold α using Bonferroni correction. 31
Results
This section sets out the main results of our data collection and analysis.
Sample characteristics
Sample characteristics (socio-demographic characteristics).
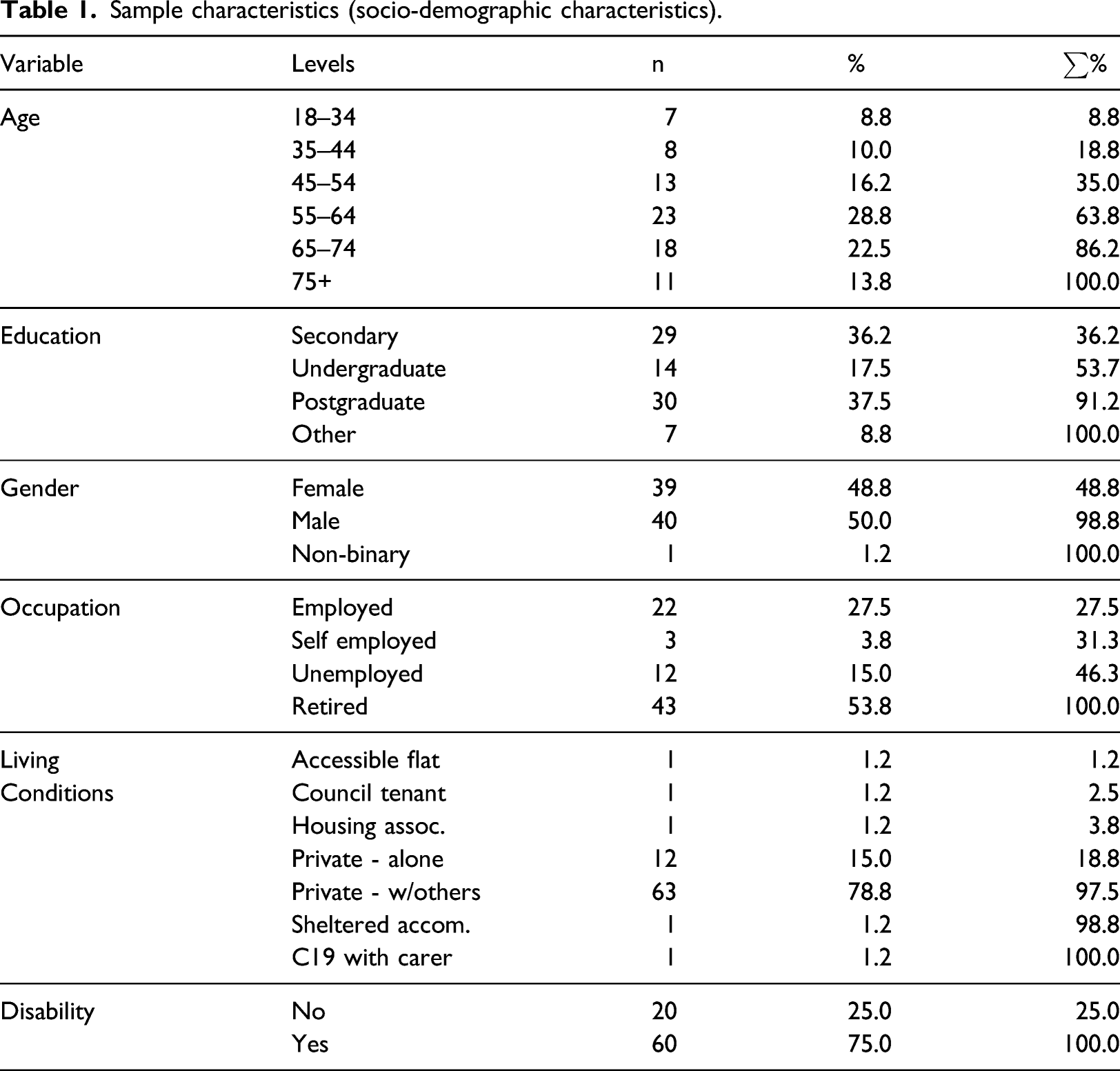
Nearly all participants reported living in private households (75), typically with others (63) rather than alone (12). This concentration of responses indicated that it would not be feasible to draw conclusions about variance in attitudes depending on living conditions. In our primary analysis when considering socio-demographic factors we will be focusing on Age, Education and Disability only.
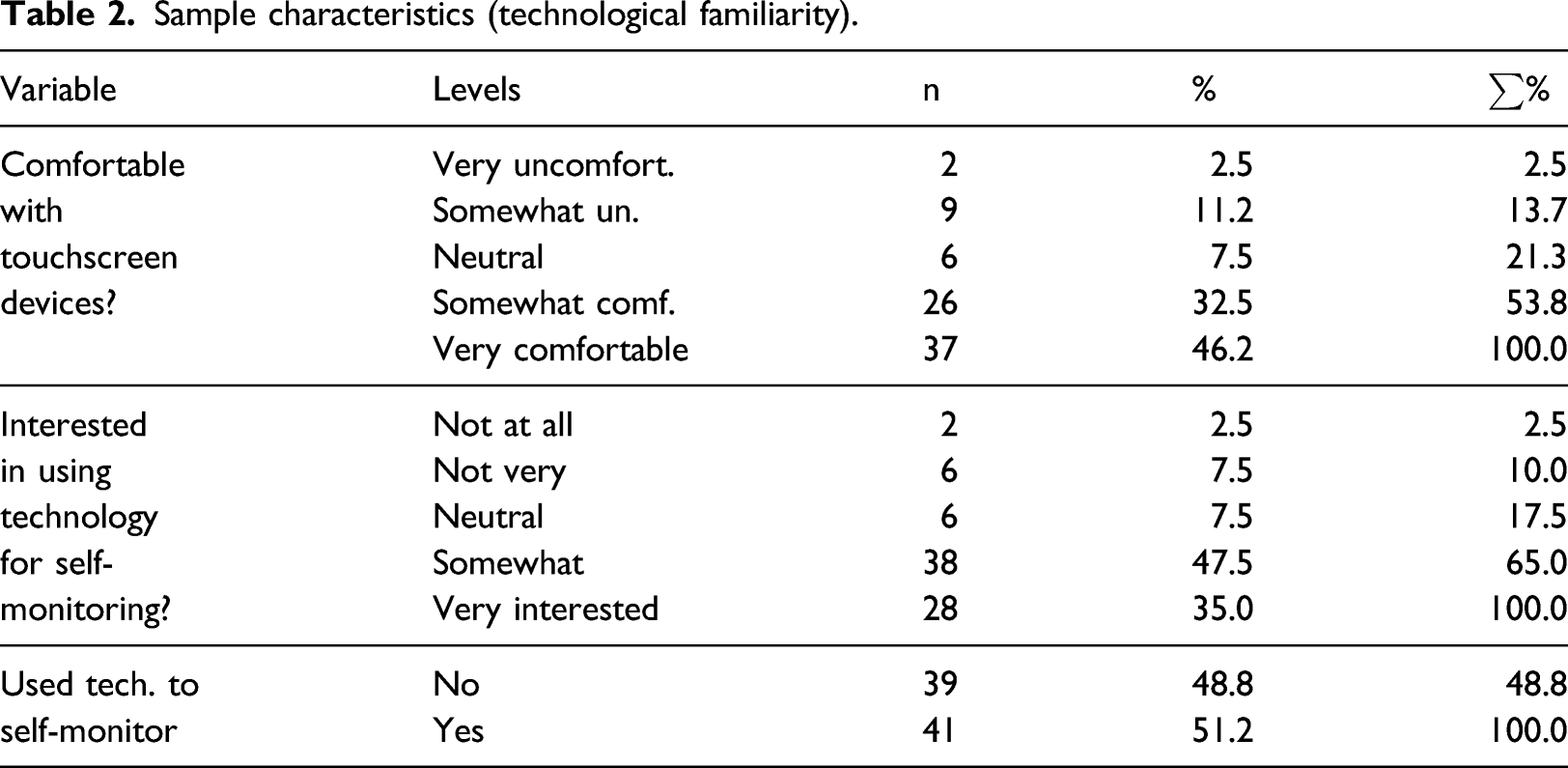
Sample characteristics (technological familiarity).
Our primary analytical objective was to investigate whether the sample can be considered representative of the general stroke survivor population in the UK. The socio-demographic characteristics of UK stroke survivors are not well-known, in contrast to the availability of data and models addressing prevalence.20,32 Although subject to evident limitations associated with specific geographical scope, the best available source of data on socio-demographic characteristics in the population is the South London Stroke Register (SLSR). 33 We compared our sample characteristics to the characteristics of SLSR stroke survivors.
The survey sample included more younger people and fewer older people than the SLSR population (see Figure 1). Age distribution of Survey Respondents and SLSR.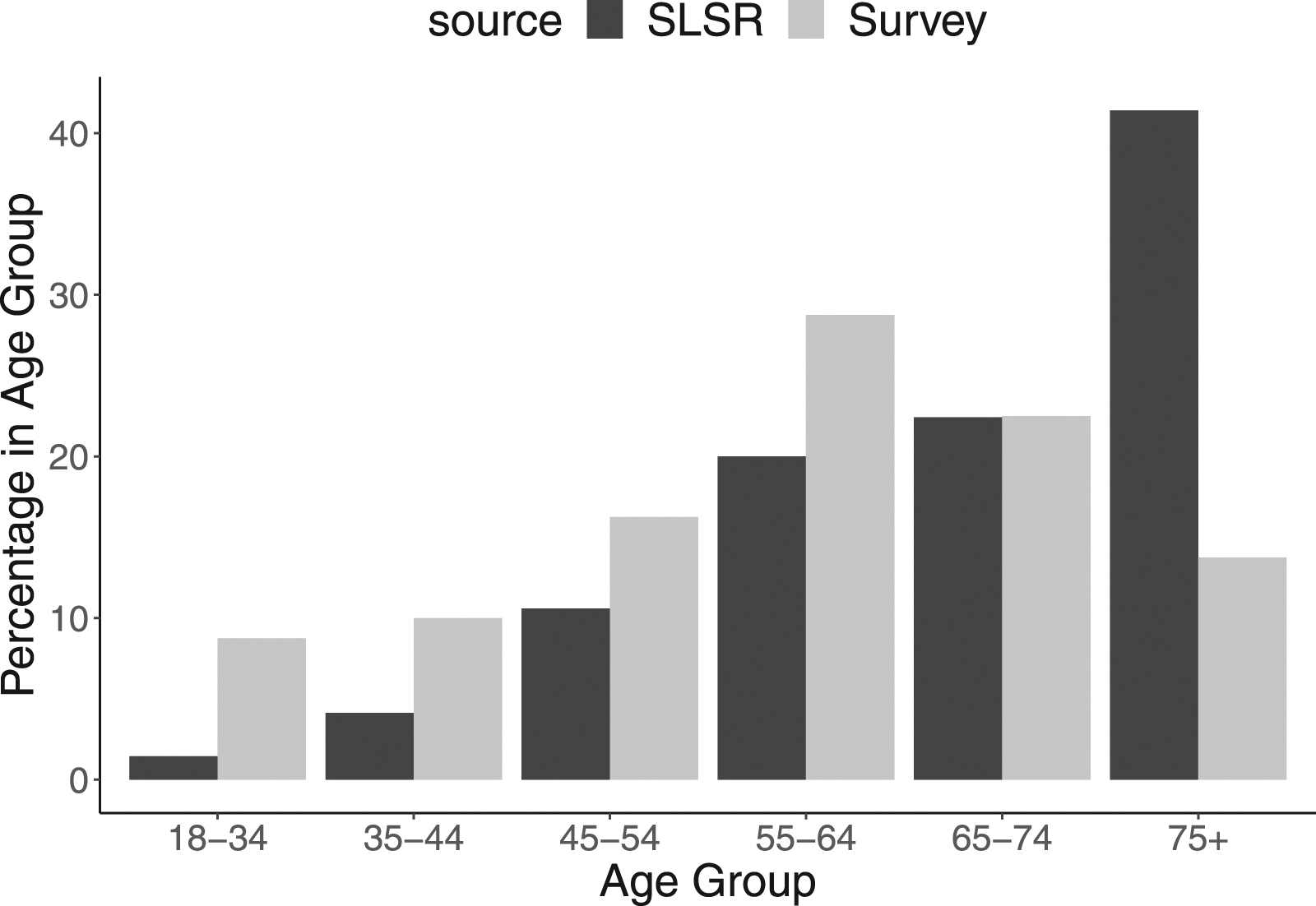
The survey sample also included a higher proportion of people with post-secondary education, above all at postgraduate level: 38% reported postgraduate education as their highest level, compared to less than 4% in the SLSR equivalent; 18% undergraduate, compared to 10% in SLSR; and 36% secondary, compared to 46% in SLSR.
We did not undertake a direct comparison of disability data between the sample and SLSR because of the limited utility of comparing self-reported status at uncertain time after stroke with the more detailed assessment techniques applied by SLSR (see for example 34 ). However a broad assessment is that about two thirds of stroke survivors leave hospital with a disability. 35 On this basis it appeared that stroke survivors with a disability were well-represented in the sample, subject to reservations about possible under-representation of types and severity.
Additional checks did not reveal any additional concerns about representation from SLSR comparison, with living conditions broadly tallying and a slightly higher proportion of people with female gender identity (49% compared to 43% in SLSR). Despite the potential to do so using national area prevalence data, geographical representation checks were not undertaken because of their indirect relevance to socio-demographic variables of interest. However it was clear that stroke survivors living in England, especially in the South, were heavily over-represented in our sample.
Willingness to use and attitudes to data sharing
Survey participants generally showed willingness to use the system, with about three quarters indicating that they would be willing to carry out each of the relevant tasks required to use the CONSULT system (see Figure 2). Generally speaking more than half of responses to each relevant question indicated that the participant would be ‘very willing’ to use the relevant component, and about a further quarter ‘somewhat willing’. (Q11) How willing would you be to carry out the following task using CONSULT?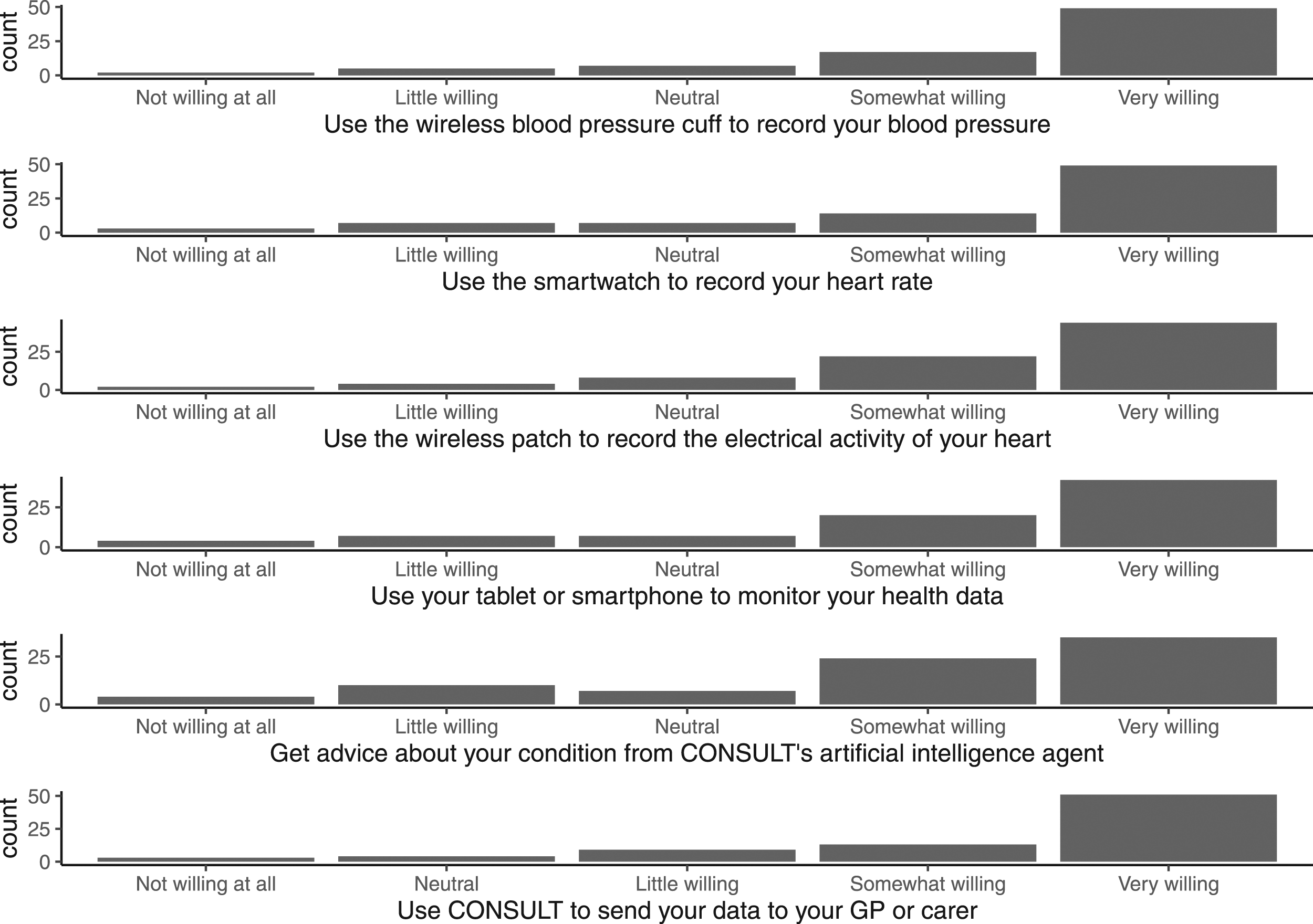
In terms of wellness sensor devices, participants were slightly more willing to use the wireless blood pressure cuff and heart rate monitoring smartwatch (49 participants ‘very willing’ to use in each case, and 17/14 ‘somewhat willing’ respectively) than the wireless electrocardiogram patch (44 ‘very willing’, 22 ‘somewhat willing’). Participants’ attitudes were cooler towards getting advice from the CONSULT system’s AI agent (35 ‘very willing’, 24 ‘somewhat willing’).
Survey participants also tended to positive attitudes towards data sharing, again with about three quarters indicating that they would be willing to share data in relevant ways. A large majority said that they would use the CONSULT system to send data to their GP or carer (51 ‘very willing’, 13 ‘somewhat willing’) (see Figure 2). A similar though more reserved majority said that they would be willing to make their health records and sensor data available to the CONSULT system (35 ‘totally agree’, 28 ‘agree’) (see Figure 3). (Q12) Indicate your level of agreement with the following statements.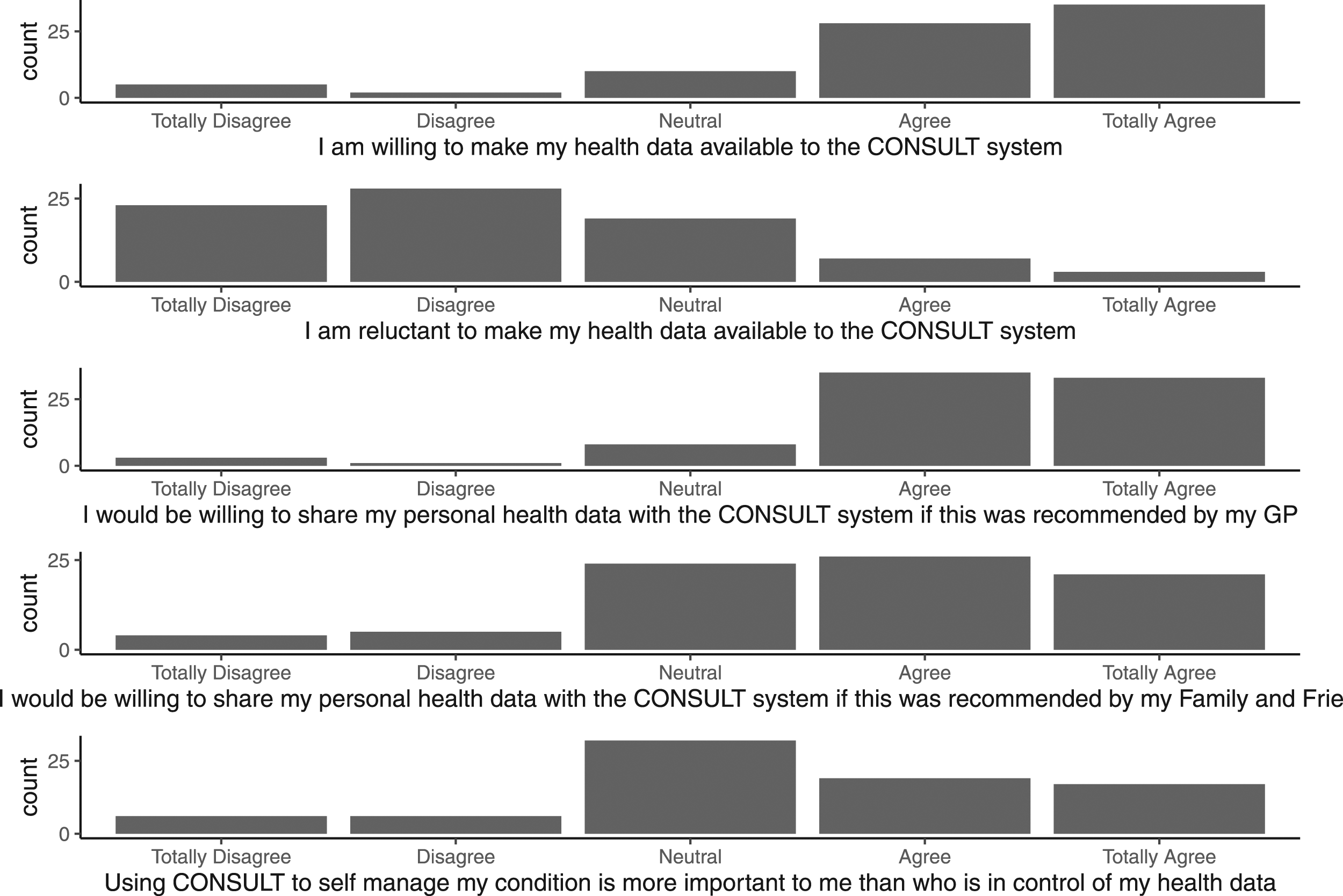
An additional question following the latter question on making data available to the CONSULT system asked participants to indicate how far they were reluctant to do so. Although most participants said that they were not reluctant (23 ‘totally disgree’, 28 ‘disagree’), many were uncommitted (19 ‘neutral’) and a considerable minority reported reluctance (7 ‘agree’ and 3 ‘totally agree’). These responses indicated that some people retain some degree of reluctance about data sharing, or are neutral on this point, even when they are ultimately willing to share it. In other words, these questions were not apparently understood as being totally opposed to each other. This was surprising since the additional question was originally introduced as an attention check. Only one response eventually suggested that a participant was not paying close attention, since ‘totally agree’ to reluctance was selected immediately after ‘totally agree’ for willingness.
Survey responses indicated that a higher proportion of participants would be willing to make their health data available to the CONSULT system if this was recommended to them by their GP (33 ‘Totally Agree’, 35 ‘Agree’) than they would if this was recommended to them by their family or friends (21 ‘Totally Agree’, 26 ‘Agree’). It also appeared that participants’ motivation to self-manage their condition might override data sharing concerns to some extent, with a notable proportion responding that the former is more important to them than the latter (17 ‘totally agree’, 19 ‘agree’) although most demurred on this question (32 ‘neutral’).
Variance in attitudes according to socio-demographic factors
Our primary analysis for this study tested the hypothesis that there is no relationship between a participant’s socio-demographic characteristics (Age, Education and Disability) and their willingness to use the CONSULT system or attitudes to data sharing. We found that there was no significant relationship. There was overall agreement and this pattern was consistent across socio-demographic categories.
See the Appendix for a significance Table 5 showing the non-relevance of these relationships across Age (Q1), Education (Q3) and Disability (Q7). Potential significance was only apparent for the Q11 response to the question ‘How willing would you be to…Use your tablet or smartphone to monitor your health data through the CONSULT system?’, with p-values of 0.0114 and 0.0410 for Education and Disability respectively; however this was insufficient to demonstrate significance after Bonferroni correction.
This means that participants’ tendency to give positive responses to questions about use of and data sharing through the CONSULT system did not appear to vary for any particular relevant factor, applying for example to older, less educated and disabled people as well as younger, more educated and not disabled people.
Our secondary analysis explored whether there was a relationship between other covariates, notably Section 2 responses about participants’ levels of technological familiarity as well as their gender identification and reported occupation, and their attitudes to use and data sharing.
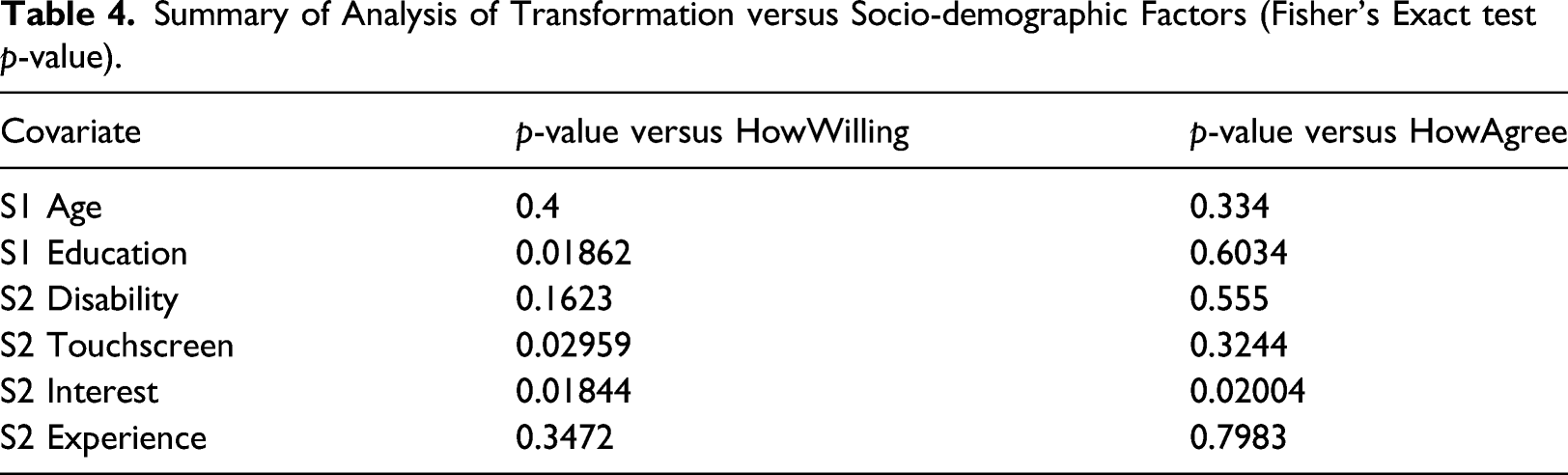
We found two significant relationships here, both indicating that levels of technological familiarity inform attitudes to use and data sharing. Firstly, participants reporting a higher level of interest in using technology to self-monitor their health at home (Question 9) were found to be more likely to report positive attitudes towards certain use and data sharing questions - specifically towards: use of the heart rate smartwatch (Question 11b); use of the wireless electrocardiogram patch (Question 11c); sending data to their GP or carer (Question 11f); and sharing personal health data with the CONSULT system if recommended by a GP (Question 12c).
Secondly, participants reporting existing experience of using technology to self monitor their health at home (Question 10) were found to be more likely to report a positive attitude towards use of a tablet or smartphone to monitor their health data through the CONSULT system (Question 11d).
We found no significant relationship between participants’ gender identification and their willingness to use the CONSULT system or attitudes to data sharing.
Again see the Appendix for these relationships, incuding non-relevance in the case of Gender (Q2) and Occupation (Q4). In some cases the p-values for Fishers Exact needed to be computed using Monte Carlo simulation. The significance level used for these inferences was adjusted to account for the multiple comparisons made (Bonferroni - therefore α = 0.05/11 = 0.0045).
Exploratory transformations
During the course of our analysis, we encountered interesting observations about levels of consistency within participants’ attitudes to use and data sharing across the various questions presented in the survey. We also became interested in the question of whether participants’ willingness to use tended to align with attitudes to data sharing.
In order to address these points, we propose a transformation of participants’ responses to use and data sharing questions as described above. For each relevant series of questions (Questions 11a-e for willingness to use; Questions 11f and 12a as the key data sharing variables), participants were divided into three groups using the conservative approach described in Figure 4. These transformations yielded two new variables for the willingness to use and data sharing attitudes (‘HowWilling’ and ‘HowAgree’ respectively) of each participant, each with three levels: one indicating consistent selection of the most positive available response; one indicating selection of a negative response to any question; and one the middle ground (not consistently most positive but not negative either). Transforming use questions into “HowWilling” and data sharing questions into “HowAgree”.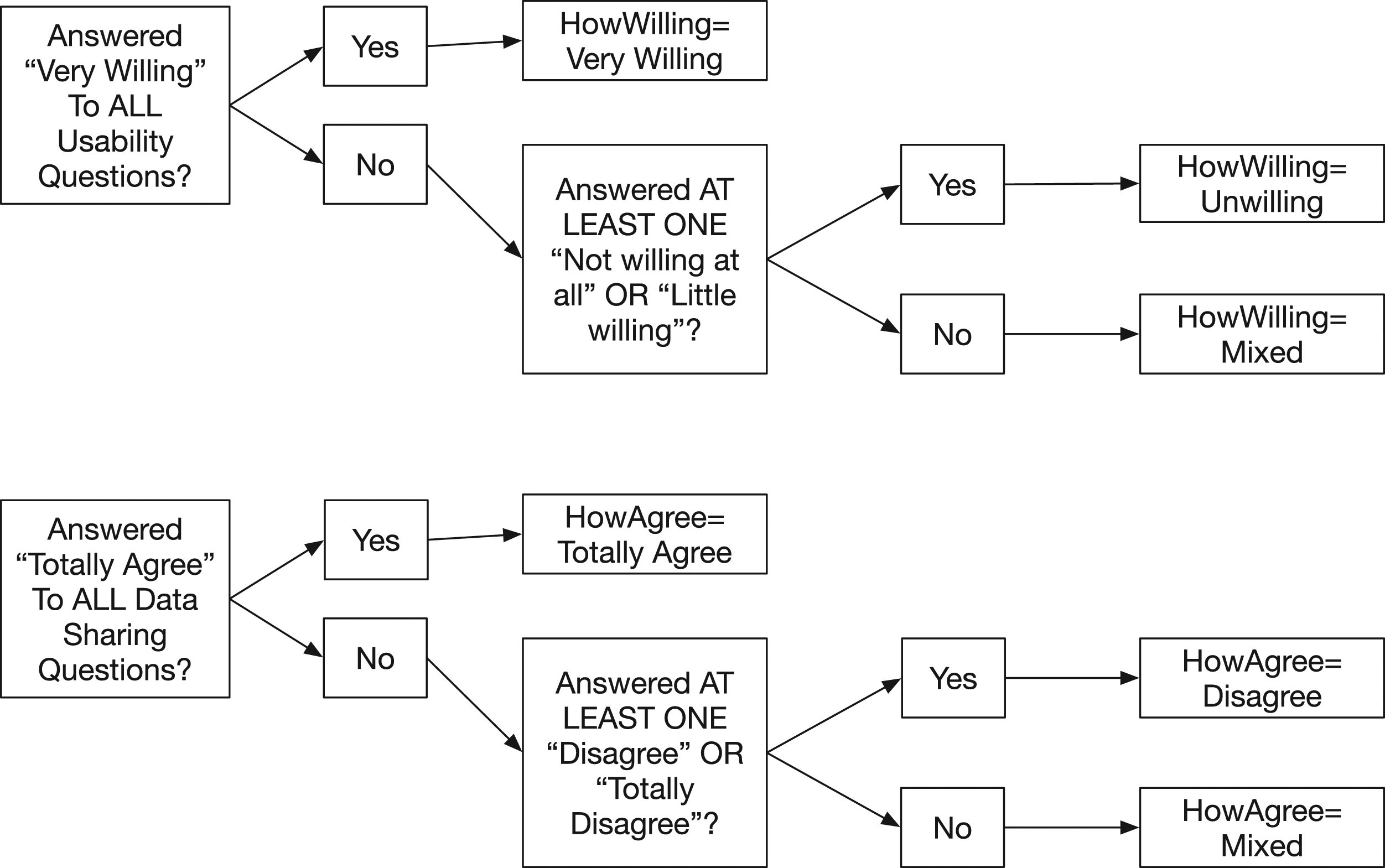
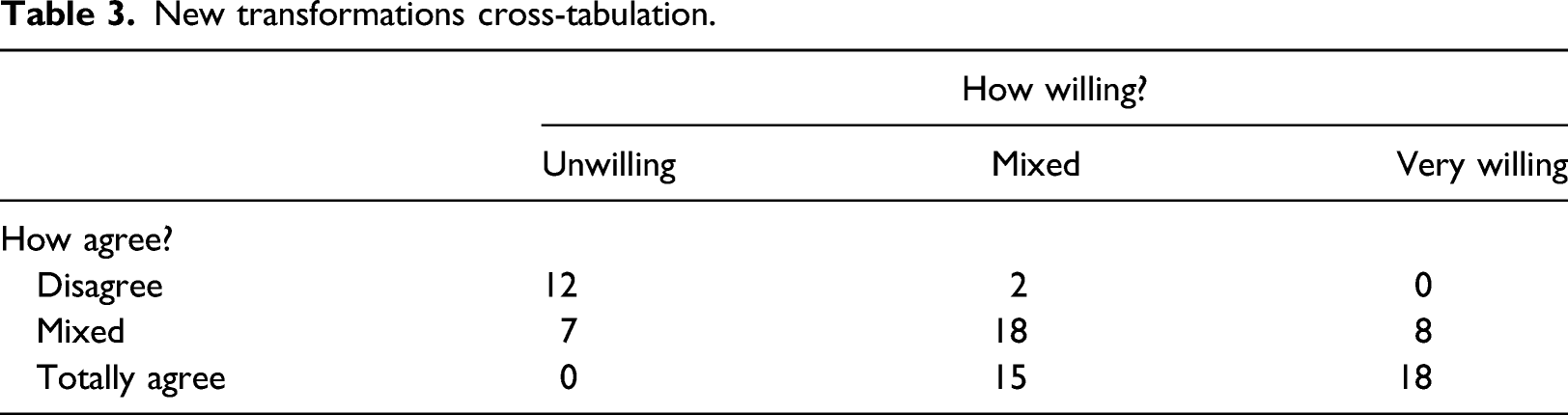
The transformations tended to underline the point that survey responses tended to reflect positive attitudes towards use of and data sharing through the CONSULT system. Even using a conservative approach defining negative attitudes as provision of any sub-neutral response, a minority of participants reported negative attitudes (19 about use, 14 about data sharing).
New transformations cross-tabulation.
Summary of Analysis of Transformation versus Socio-demographic Factors (Fisher’s Exact test p-value).
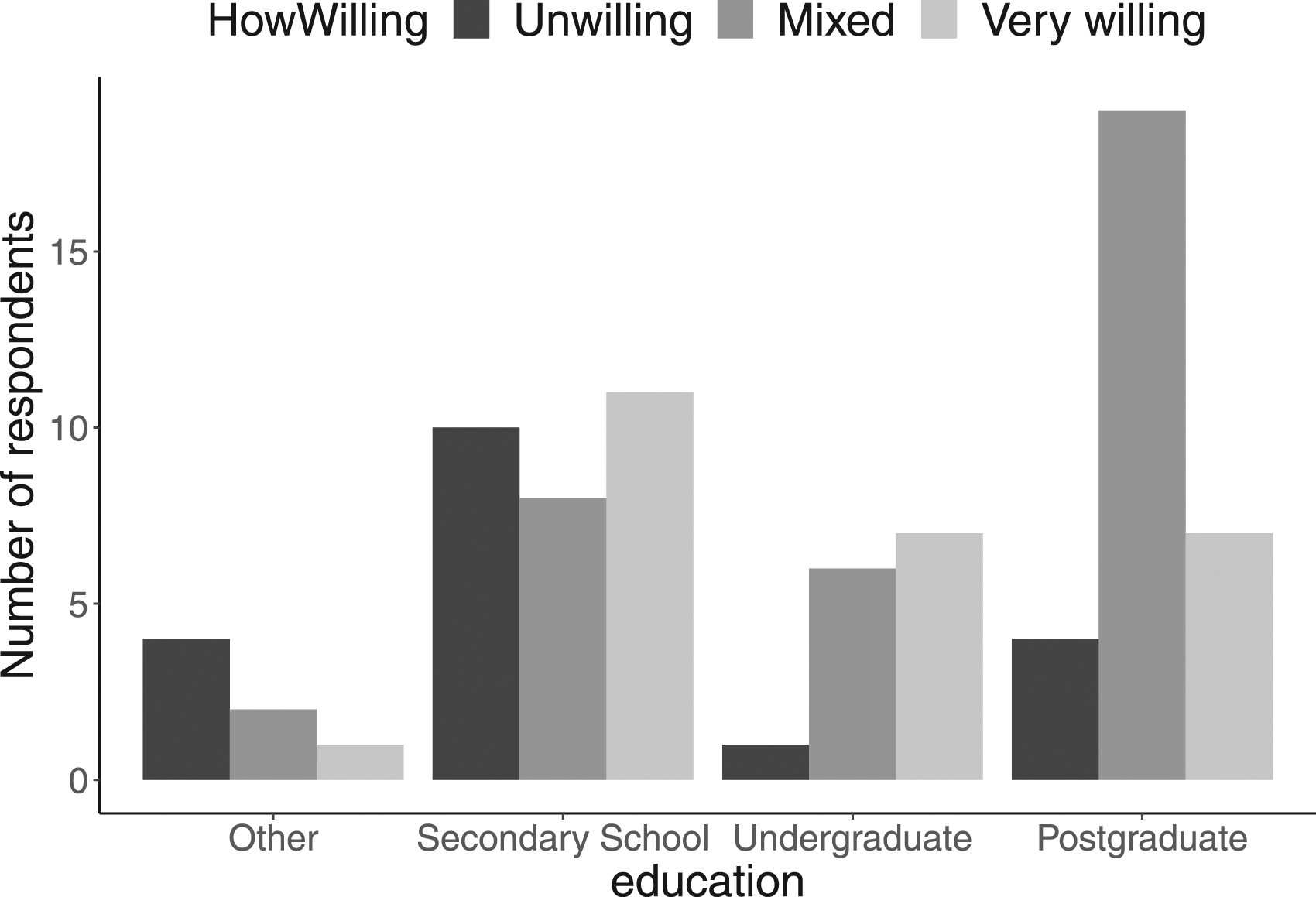
HowWilling distribution by education level.
Discussion
This study indicates that there is no straightforward relationship between basic socio-demographic factors (age, education and disability) and stroke survivors’ willingness to use and attitudes to data sharing through self-management connected health technologies like CONSULT. We were unable to test the relationship between stroke survivors’ living conditions and their attitudes.
To our knowledge, there is no prior published research on this relationship in the context of connected health. Existing research on attitudes towards mobile health apps in general has indicated that age and level of education are predictors of mobile health app use among patients.36,37 However, Bol et al. (2017) 36 also found that their effect may differ in predicting use of specific types of mHealth technologies. This could be the case for connected health technologies like CONSULT and may help explain the lack of straightforward relationships in this study.
Our main finding is that there are a considerable number of stroke survivors living in the UK who are interested in using connected health systems to self-manage their health, and who tend to a positive attitude towards its use as well as towards the data sharing required. Participants’ attitudes were more upbeat than expected, especially considering that the CONSULT system they were asked to consider is a proof-of-concept research prototype. It may be that Covid-19 restrictions, including difficulties accessing non-urgent health and care services, made the potential benefits of remote monitoring technology clearer for participants than they might otherwise have been. This certainly appears to have occurred in the context of chronic diseases like diabetes and cancer, where patients were observed to have engaged more with the use of telemedicine and mHealth to access health care services.38,39 A large majority, about three-quarters of participants, gave no negative answers when asked about use and data sharing; and a significant minority, about a quarter, were consistently highly positive about all aspects considered.
Participants in the sample reported high, though not consistent, levels of technological familiarity, with over three quarters saying they had some degree of comfort in using touchscreen technology and the same proportion some degree of interest in using technology to self-monitor their health at home. Most strikingly, over half said that they use, or have used, technology to self-monitor their health at home. This suggests that possibly, to an extent greater than is appreciated, the question for connected health might be one of harm from non-use of available data as much as benefit from new uses of data. 40
Our results suggest that the adoption of connected health systems does not in itself necessarily imply the exclusion of any particular group. Our sample included many older and less educated stroke survivors, with three quarters reporting that they had a disability. It was particularly interesting that the median age range of our sample was 55–64. This is an age not typically associated with ‘digital native’ behaviours, but on the other hand still working-age and including people no doubt often being required to adapt to technological change in other aspects of their lives. 41 Not developing connected health systems risks disregarding the preferences of these people. In this sense, our study contributes to other work treating the challenge as one of supporting and assisting groups to take advantage of the benefits of technology. 11
The finding that connected health system adoption does not necessarily exclude older people is atypical to what published research has shown before the COVID-19 pandemic. 42 But there have been numerous observations that patients across different age groups became more familiar with and willing to use different types of technologies during the pandemic, including mobile health 43 and other non-health-related consumer technologies.44,45 Such a shift in attitudes might help explain the positive attitudes towards connected health technologies and data sharing from older adults in our survey. Even if so, these changes seem to have been complicated; one rapid review found that during the beginning of the pandemic the elderly patients had difficulties using digital health care compared to their younger counterparts and these difficulties may still prevail. 46
Participants’ attitudes apparently varied according to their level of technological familiarity more than their socio-demographic characteristics. Similar results were reported by Chandrasekaran et al. (2021) 48 who examined use of wearable technologies among older adults in the United States. This finding also accords with findings from earlier studies examining acceptance and use of mobile health apps and eHealth in general.29,48,49 Above all, stroke survivors who said they were interested in using technology to self-monitor their health at home were more likely to respond positively to use and data sharing questions. In other words, individuals’ emotional orientation and motivation to devote attention to the technology appeared to be more important than conventional socio-demographic categorisations. This finding tends to support work highlighting personalisation as an important consideration for connected health systems implementation, focusing on developing the ‘personal involvement’ of users. 50
Although we found participants’ attitudes to be generally strikingly positive, we also found that most participants tended to have at least some degree of reservation. Our exploratory transformations indicated that nearly half of people tending to a consistently positive opinion of data sharing had more reserved views on use, for example. Again this might tend to focus attention on means for supporting and assisting groups in overcoming their reservations. Our finding that participants were more likely to be willing to share personal health data following a GP’s recommendation is in line with established evidence that the recommendations of health care providers is relevant to patient decision-making. 51 Family and friends were found to be less relevant for attitudes to data sharing. The relevance of these different types of stakeholders to willingness to use was not tested, but might prove relevant for future research.
We found an interesting possible relationship between general willingness to use (following transformation) and stroke survivors’ level of education. Whereas participants with a secondary education tended to be more likely to be ‘unwilling’ to use the CONSULT system and those with an undergraduate education more likely to be ‘very willing’, participants with a postgraduate education appeared to be much more likely to take a ‘mixed’ view. This suggests a possible ‘goldilocks’ effect of education on attitudes to use: too much or too little might mean reservations; an undergraduate degree might be ‘just right’.
Given the lack of other connected health technology research on this causal relationship, further research is needed to support this suggestion. Previous research has shown a positive correlation between level of education and mobile health technology uptake 52 or online health information seeking. 53 More recently, studies on COVID-19 vaccine hesitancy have shown a negative correlation between level of education and vaccine hesitancy. 54 In all these cases the authors observed a linear relationship between factors. We propose a possible ‘inverted-U’ relationship instead, possibly specific to this type of connected health technology.
Limitations
There are various evident limitations to this study, for example it is cross-sectional and only addresses the United Kingdom. This section focuses on data collection issues and general reflections.
There are problems with exclusive use of an online survey questionnaire for this study because it presupposes technology use. It was foreseeable that a proportion of the target population would be unable and/or unwilling to participate due to overlapping issues with skills/experience, accessibility or motivation. Steps were taken to mitigate the risks involved, for example video-based explanation of the CONSULT system in Section 3 of the survey. However limitations were largely accepted as a reasonable constraint under the extraordinary circumstances of a global pandemic.
Two approaches were used to understand the resulting bias. First, sample characteristics were compared to best-available data on the general population of interest as described above. Survey participants were demonstrably a younger and more educated group than stroke survivors generally. Additionally their apparent levels of technological familiarity provided a strong suggestion that survey participants were – for a combination of reasons including abilities and skills as well as inclination – probably more likely to contemplate using and less likely to exclude the possibility of connected health systems than the general stroke survivor population.
Second, email feedback during data collection (see above) was recorded and reviewed for any apparent themes in decision-making about whether or not to participate in the survey. This suggested complicated combinations of factors, for example with Covid-19 and disability factors motivating as well as inhibiting efforts to address issues with stroke survivors’ access to relevant technology. Intermediaries often decided simply not to present patients with relevant decisions, hinting at preferences that therefore probably under-represented in our results. The most common feedback received was simply that older people do not use technology. For example:
I’m afraid I’m going to have to pass on this one. The average age of my members is c. 80 and they don’t generally have computers or tablets. If they did have an email address or online access they’d probably never check it and are definitely a group that prefer good old fashioned letters. So I’m not sure you’d ever find a way to make better use of technology for them.
Our conclusion was therefore that the survey sample cannot be regarded as representative of UK stroke survivors generally. Rather, our analysis above speaks to the attitudes of stroke survivors predisposed to contemplate relevant uses of technology rather than directly to the attitudes of stroke survivors overall.
The limitations of this study tend to confirm existing evidence about the risks of exclusion along socio-demographic lines as connected health systems become more widespread, 8 especially with respect to age and also apparently levels of education although not necessarily with respect to disability. In addition to larger sample sizes, future studies should consider methodological approaches to reduce selection bias and improve representation of older and less educated stroke survivors. Ideally this would refer to improved data about the socio-demographic characteristics of stroke survivors in the UK. Experience with this survey also suggests that understanding relevant attitudes in living conditions other than private households will require a specifically targeted approach, and that understanding the relevance of disability will require more details on types and severity.
Conclusion
This study found no simple relationship between key socio-demographic factors and patients’ willingness to use and attitudes towards data sharing through a self-management connected health system. It indicated instead that patients’ levels of interest in relevant technology was a more significant factor in determining these attitudes. The results underline the importance of prioritising patient-centred participatory research in efforts to design and implement connected health technologies, maximising the benefit for patients with varying requirements and characteristics yet minimising the risk of excluding certain groups.
We recommend that future studies seek larger sample sizes, address the problem of understanding socio-demographic characteristics of the stroke survivor population as a whole, and apply techniques to improve representation of groups that are otherwise at risk of exclusion.
Footnotes
Acknowledgements
Many thanks to everyone who kindly gave their time to participate in the survey. Thanks also to Prof. Anthony Rudd and the members of the project’s Clinical Advisory Board for their encouragement and support, in particular our patient & carer representatives and Richard Francis at the Stroke Association for his interest in this study. Finally thanks to our collaborators and suppliers of devices and data for the prototype: Garmin, Withings, MediBioSense and EMIS.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UK Engineering & Physical Sciences Research Council (EPSRC), grant #EP/P010105/1.
ORCID iDs
Appendix
Summary of Analysis: Variance in attitudes according to socio-demographic factors (Fisher’s Exact test p-value, where justified computed using Monte Carlo simulation and Bonferroni adjusted).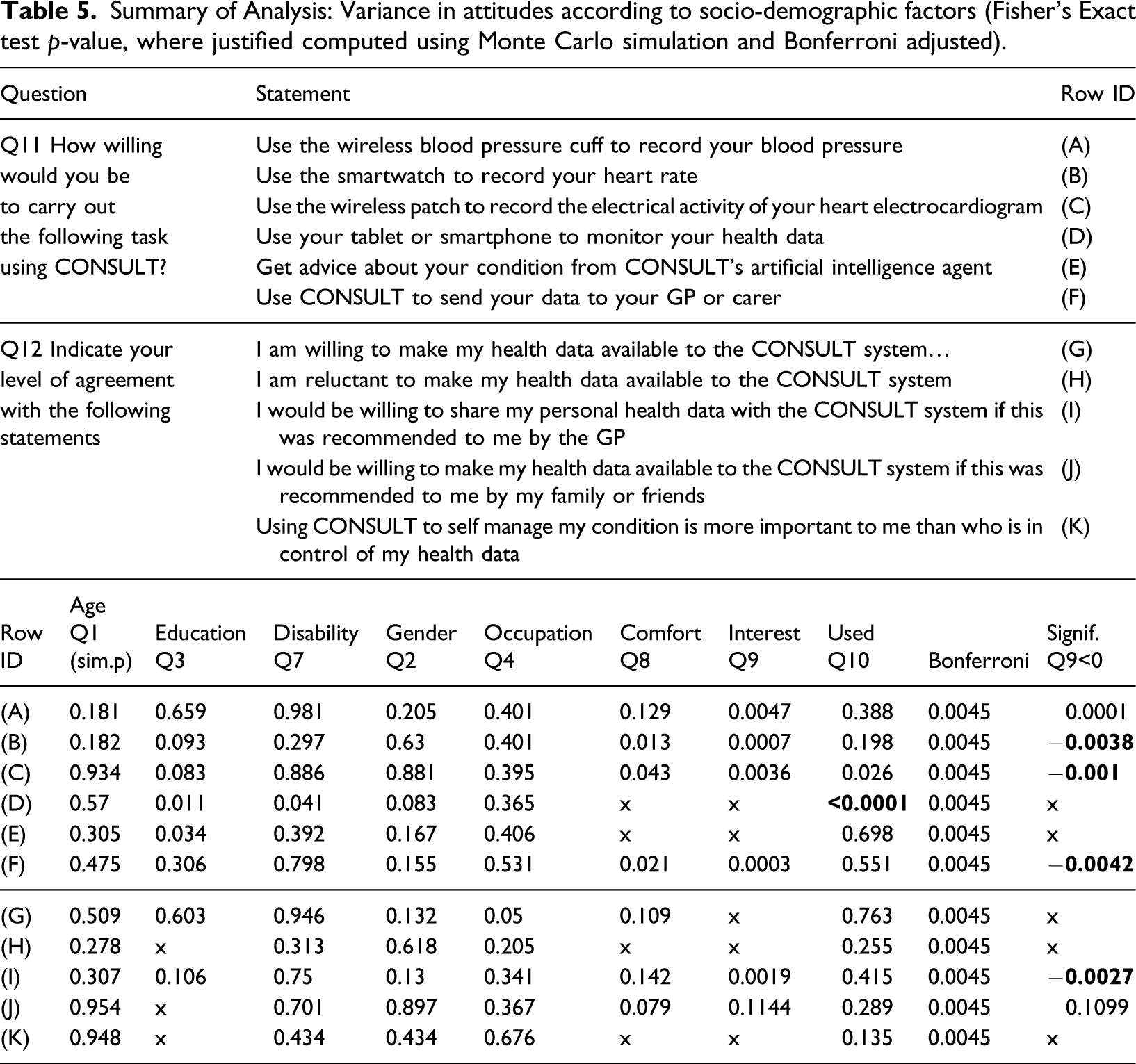
Question
Statement
RowID
Q11 How willing
Use the wireless blood pressure cuff to record your blood pressure
(A)
would you be
Use the smartwatch to record your heart rate
(B)
to carry out
Use the wireless patch to record the electrical activity of your heart electrocardiogram
(C)
thefollowingtask
Use your tablet or smartphone to monitor your health data
(D)
using CONSULT?
Get advice about your condition from CONSULT’s artificial intelligence agent
(E)
Use CONSULT to send your data to your GP or carer
(F)
Q12 Indicate your
I am willing to make my health data available to the CONSULT system…
(G)
level of agreement
I am reluctant to make my health data available to the CONSULT system
(H)
with the following statements
I would be willing to share my personal health data with the CONSULT system if this was recommended to me by the GP
(I)
I would be willing to make my health data available to the CONSULT system if this was recommended to me by my family or friends
(J)
Using CONSULT to self manage my condition is more important to me than who is in control of my health data
(K)
Row ID
Age Q1 (sim.p)
Education Q3
Disability Q7
Gender Q2
Occupation Q4
Comfort Q8
Interest Q9
Used Q10
Bonferroni
Signif. Q9<0
(A)
0.181
0.659
0.981
0.205
0.401
0.129
0.0047
0.388
0.0045
0.0001
(B)
0.182
0.093
0.297
0.63
0.401
0.013
0.0007
0.198
0.0045
(C)
0.934
0.083
0.886
0.881
0.395
0.043
0.0036
0.026
0.0045
(D)
0.57
0.011
0.041
0.083
0.365
x
x
0.0045
x
(E)
0.305
0.034
0.392
0.167
0.406
x
x
0.698
0.0045
x
(F)
0.475
0.306
0.798
0.155
0.531
0.021
0.0003
0.551
0.0045
(G)
0.509
0.603
0.946
0.132
0.05
0.109
x
0.763
0.0045
x
(H)
0.278
x
0.313
0.618
0.205
x
x
0.255
0.0045
x
(I)
0.307
0.106
0.75
0.13
0.341
0.142
0.0019
0.415
0.0045
(J)
0.954
x
0.701
0.897
0.367
0.079
0.1144
0.289
0.0045
0.1099
(K)
0.948
x
0.434
0.434
0.676
x
x
0.135
0.0045
x