
Abstract
Background
In low- and middle-income countries, electronic health record (EHR) implementation is often undermined by insufficient user training and digital literacy gaps. Emerging tools such as artificial intelligence (AI)–supported personalised training have the potential to address these challenges, but their applicability and perceived value in resource-constrained contexts remain unclear.
Objective
This study examined healthcare professionals’ perceptions of AI-supported personalised training for EHR use in Tanzanian public hospitals. It assessed perceived benefits, barriers to EHR utilisation, preferred design features and factors influencing user readiness, guided by the Sociotechnical Systems (STS) theory.
Methods
A preliminary exploratory cross-sectional survey was conducted with 20 healthcare professionals from two public hospitals in Dodoma, Tanzania. Data was collected using structured, self-administered questionnaires and analysed descriptively with supplementary inferential tests. Participants’ self-assessed proficiency, training experiences and views on AI-supported training were assessed.
Results
Most participants (90%) had never received AI-based training, yet 85% expressed strong interest and 90% believed it could improve EHR proficiency. Preferred features included simulation-based learning (75%), real-time in-system guidance (65%) and progress-tracking dashboards (50%). Major barriers to EHR use were inadequate training (75%), poor interface usability (60%), limited technical support (50%) and data privacy concerns (55%). A significant positive correlation was found between years of experience and self-rated EHR proficiency (r = 0.46, p = 0.04), and nurses reported more barriers than other cadres (χ² = 5.67, p = 0.04). Qualitative insights reinforced these findings, showing strong expectations for adaptive learning support and perceived organisational benefits such as reduced dependency on IT staff and improved data quality.
Conclusion
Healthcare professionals in Tanzania demonstrated readiness and optimism towards AI-powered personalised training as a means to enhance EHR competence and overcome persistent skill and support gaps. Viewed through the STS lens, the findings underscore the need to align technological innovation with human and organisational capacity for sustainable digital health transformation. Further research with larger samples and real-world pilot interventions is recommended to evaluate feasibility, trust and long-term impact.
Keywords
Introduction
Digital technologies are transforming healthcare systems worldwide, providing new avenues for enhancing service delivery, clinical decision-making and data management. From electronic prescribing to clinical decision support and predictive analytics, health information technologies are now central to modern healthcare reforms. 1 Among these, electronic health record (EHR) systems remain a cornerstone of digital health infrastructure, facilitating better continuity of care, patient safety and health system efficiency.
However, the effectiveness of these systems depends not only on their technical design but also on the ability of healthcare workers to use them competently. Evidence from both high- and low-income countries shows that inadequate user training and poor digital literacy often undermine the potential of EHR systems. 2 As a result, significant investments in digital health risk yield suboptimal returns if healthcare workers are not equipped with the skills to use these systems effectively.
Low- and middle-income countries (LMICs), including those in sub-Saharan Africa, face particular challenges in this regard. While efforts to digitise health systems are ongoing, including the rollout of national EHR platforms, gaps in workforce capacity remain a key bottleneck. In Tanzania, the government has made notable efforts to promote the adoption of EHR systems, particularly in zonal and national hospitals. However, the full potential of these systems remains under-utilised due to persistent challenges related to user proficiency, digital literacy and limited access to effective training mechanisms. 3
Despite the increasing deployment of EHR systems in Tanzanian healthcare facilities, studies indicate that many healthcare professionals lack the necessary skills to use them effectively. A 2024 national review found that fewer than 30% of healthcare workers in primary and secondary care settings felt confident in navigating EHR platforms independently. 4 These skill gaps are further exacerbated by the dominance of conventional training approaches, which typically involve one-off workshops or passive demonstrations, which fail to provide sustained, role-specific learning opportunities. They have been linked to the reliance on traditional training methods, such as brief workshops or one-off sessions, which often fail to accommodate individual learning needs or the complexity of real-time system use. 5 As a result, many healthcare workers resort to workarounds or partial system use, limiting the impact of digital investments on patient care and health system performance.
Globally, there is growing momentum towards leveraging artificial intelligence (AI) to deliver personalised digital training that adapts to individual users’ performance and learning preferences.6,8 Artificial intelligence–powered training platforms are increasingly being implemented in high-resource settings to provide just-in-time learning, simulate clinical scenarios and deliver feedback aligned with user progress.9,10 These tools have demonstrated promise in reducing training costs, improving retention and enhancing confidence among healthcare staff. In sub-Saharan Africa, however, the application of AI for digital training remains in its early stages, with few studies evaluating its relevance and effectiveness in resource-constrained environments. 11 This global context highlights the importance of exploring how AI tools can be effectively integrated into workforce development strategies in LMICs.
This study aims to address this gap by assessing how AI-powered personalised training could enhance EHR proficiency among healthcare workers in Tanzania. Specifically, the study explores healthcare professionals’ perceptions of AI-based training tools, identifies barriers to effective EHR use and examines the potential role of intelligent learning platforms in overcoming these barriers. By focusing on real-world settings in Tanzanian public hospitals, the research contributes to growing efforts to build a digitally capable health workforce in low-resource environments.
Literature review
Theoretical framework
The study adopts the Sociotechnical System (STS) perspective to conceptualise the relationship between AI-supported training and healthcare professionals’ proficiency in using EHR systems. According to STS theory, effective technology adoption occurs when social and technical subsystems are jointly optimised. In the context of Tanzanian healthcare, AI-powered training should therefore be viewed as part of an interconnected system involving users, technology, infrastructure and organisational culture.
Earlier models, such as the Technology Acceptance Model (TAM) and the Unified Theory of Acceptance and Use of Technology, have been widely used to examine technology adoption,12,13 but they centre primarily on individual perceptions of usefulness and ease of use. In contrast, the STS framework offers a more suitable foundation for this study because it recognises that technology, people and organisation are interdependent subsystems that must function in harmony for innovations to succeed.14,15 Within this lens, AI-supported training is understood not as a stand-alone digital intervention but as a component of a socio-technical ecosystem that encompasses healthcare workers’ practices, institutional culture, leadership and infrastructure. The framework, therefore, guides the interpretation of how social, organisational and contextual dynamics shapes the perceived usability, trust and integration of AI-based training in Tanzania's healthcare settings.
Empirical literature review
Enhancing EHRs systems proficiency through AI-powered personalised training
The successful use of EHR systems depends not only on the availability of infrastructure but also on the digital competence of end users. In many LMICs, healthcare workers report difficulties navigating digital systems due to limited and often ineffective training. 3 These challenges are particularly pronounced in sub-Saharan Africa, where EHR implementation has frequently outpaced investments in digital capacity-building. 16 Common training formats, such as one-off workshops or peer demonstrations, often fail to account for different learning needs, contributing to low system engagement and partial utilisation of core features. 2
In response to these limitations, global interest is growing in the use of AI to support health workforce development. Artificial intelligence–powered training platforms offer adaptive learning experiences by adjusting content and feedback to individual users’ skill levels and progress. These systems have been associated with improved retention, confidence and skill accuracy in controlled studies, particularly in high-income settings.7,17 For example, AI-based simulations and virtual assistants have been utilised to train healthcare workers in documentation, diagnosis and workflow navigation, resulting in significant improvements in knowledge retention and task accuracy.6,18
Although promising, few empirical studies have evaluated the effectiveness of such tools in LMICs. Studies conducted in countries such as India, Kenya and South Africa highlight common challenges, including connectivity constraints, lack of localised content and user distrust in automated systems.19,20 In the Tanzanian context, AI is increasingly discussed in areas such as diagnostics and mental health support; however, its use in workforce training remains largely untested. 21 This gap suggests the need for more empirical evidence on user acceptance and the integration of AI tools into health workforce development strategies.
Beyond AI, other technology-enhanced learning approaches have also been investigated. E-learning modules, virtual reality (VR) and serious games have shown effectiveness in medical training by enhancing engagement, promoting skill retention and reducing errors.17,22 These approaches provide a comparative baseline, demonstrating that while digital methods can improve learning outcomes, AI offers unique advantages in adaptivity and personalisation. For example, AI can deliver real-time feedback and dynamically adjust content to match users’ progress, which traditional e-learning or VR modules cannot achieve as effectively. 23
Equally important are socio-technical and institutional factors that shape the adoption of digital health interventions. Organisational culture, leadership support and policy alignment have been identified as critical determinants of technology uptake in healthcare.24,25 Recent studies have emphasised the need to consider how these institutional conditions interact with digital training solutions, particularly in LMIC contexts where infrastructural and managerial support is often limited. 26 For instance, inadequate ICT infrastructure or weak leadership commitment can undermine even well-designed AI training tools. The conceptual framework of this study, therefore, incorporates these socio-technical dimensions under the domain of institutional conditions.
In addition, recent empirical contributions from global contexts provide important insights. For example, research on healthcare professionals’ acceptance of business intelligence, 27 IoT-based healthcare, 28 blockchain adoption 29 and post-COVID digital service usage 30 highlights that digital adoption is shaped by perceived utility, trust and institutional readiness. These insights align with the findings of this study and further reinforce the need for innovative, context-sensitive training approaches in LMICs.
Taken together, this review highlights both the promise and challenges of AI-powered training for EHR proficiency. It underscores the importance of addressing infrastructural, socio-technical and institutional conditions, while situating AI within the broader ecosystem of digital training innovations.
Challenges hindering EHR system utilisation and the role of AI in addressing them
Numerous studies have identified a complex mix of barriers to effective EHR utilisation in resource-limited settings. Common challenges include poor system usability, frequent downtime, data entry errors, inadequate technical support and concerns about data privacy and security.16,24,31 A workforce with varying levels of computer literacy and minimal prior experience with digital health systems often exacerbates these issues.
While these barriers are well-documented, few interventions have focused specifically on training as a strategic entry point for overcoming them. Conventional training approaches often adopt a one-size-fits-all model and lack follow-up support, which contributes to user frustration and negative attitudes towards digital platforms.25,26,32,33 By contrast, AI-powered training systems offer adaptive support that evolves with the user's experience level, providing context-sensitive guidance and real-time feedback.34–36
Research by Refs.37,38,39 showed that AI-driven learning environments reduce cognitive overload and promote self-paced mastery, even among users with low digital literacy. Similarly,40–42 demonstrated that such systems help reduce error rates and improve compliance with documentation standards by reinforcing correct procedures through immediate, interactive feedback. However, the implementation of these systems is often limited by infrastructure deficits such as poor internet connectivity, insufficient IT support and a lack of policy alignment, challenges that remain acute in the Tanzanian context.3,4,43
Another important gap in the literature is the limited focus on user perceptions of AI-powered tools. Most studies rely on usage metrics or performance outcomes, overlooking how healthcare workers feel about learning through AI interfaces. It is critical, given that fear of technology, trust issues and privacy concerns often mediate the effectiveness of such interventions.44–46
Thus, while AI-powered training holds substantial promise in addressing persistent barriers to EHR use, its success depends on understanding context-specific factors, including user readiness, training content localisation and alignment with institutional support structures. This study aims to address these gaps by examining the perceptions of Tanzanian healthcare professionals towards AI-powered personalised training and evaluating how such interventions can mitigate longstanding barriers to EHR adoption and use.
Research gap
Despite increasing global evidence on AI-enabled training and its potential benefits, few studies have examined how such interventions are perceived and how they could be integrated into resource-limited health systems. Most existing studies focus on technical feasibility rather than contextual and organisational readiness. In Tanzania, little is known about how healthcare professionals understand and evaluate AI-supported learning in relation to their digital work environments. This study, therefore, addresses a critical gap by exploring these perceptions through a socio-technical lens, providing early empirical insights that can inform future design and implementation of AI-based workforce training models.
Methodology
This section describes the methodological approach used to investigate healthcare professionals’ perceptions of AI-powered personalised training. It details the research philosophy, design, setting, population, data collection and analytical procedures adopted to address the study objectives.
Research philosophy
This study was grounded in the pragmatic research philosophy, which recognises that both quantitative and qualitative data contribute valuable insights into complex social—technical phenomena. Pragmatism prioritises research questions over methodological purity and supports the integration of numerical measures with participants’ subjective experiences.47,48 This approach was suitable for exploring healthcare professionals’ perceptions of AI-supported EHR training, where understanding both measurable patterns and contextual explanations was necessary.
Research approach
A mixed-methods approach was adopted, combining quantitative and qualitative strands within a single descriptive framework. The combination enabled triangulation of findings and a richer interpretation of how individual, organisational and technological elements interact.
Research design
This study was explicitly framed as a preliminary exploratory assessment. The choice of an exploratory cross-sectional design was intentional, reflecting the lack of prior empirical research on AI-supported training for EHR use in Tanzanian health facilities. Such designs are commonly used to generate early insights into emerging interventions before committing to large-scale or experimental studies.48,49 By focusing on healthcare professionals’ perceptions, the study aimed to identify user expectations, perceived benefits and challenges, which can inform the design of future pilot interventions.
Study settings
The research was conducted at two major public health institutions in Dodoma, Tanzania: Benjamin Mkapa Hospital and Mirembe National Mental Health Hospital. These facilities were purposefully selected due to their strategic role in delivering specialised care and their ongoing participation in national digital health transformation efforts. Although these hospitals are better resourced than many peripheral facilities, they continue to face critical gaps in digital literacy and EHR system utilisation, making them ideal settings for evaluating the potential of AI-driven training models.
Population and sampling
The target population consisted of healthcare professionals directly involved in EHR use, including medical doctors, nurses and health information officers (also known as medical recorders). These cadres were selected because of their routine engagement with patient data and system-based documentation. Participants were eligible for inclusion if they had at least six months of experience working with EHR systems, were actively employed at one of the two study sites during the data collection period and voluntarily consented to participate. Professionals working in roles unrelated to EHR usage, those with less than six months of experience and individuals unwilling to provide informed consent were excluded from the study.
To determine an appropriate sample size, Cochran's formula 50 was applied based on assumptions of a 95% confidence level, 0.5 estimated proportion and a 15% margin of error. Since the accessible population was approximately 50 healthcare professionals across the two hospitals, the initial estimate was adjusted using the finite population correction approach. The final sample size was set at 20 participants, ensuring both logistical feasibility and statistical relevance. A stratified random sampling strategy was used to ensure representation from each of the three professional groups. Table 1 summarises the distribution of participants by professional category.
Distribution of study participants by cadre.

Source: Authors’ work.
Data collection methods and tools
Data was collected using a structured, self-administered questionnaire. The instrument was designed based on previously validated tools used in digital health and EHR adoption studies and was reviewed by health informatics experts to ensure content and face validity. It included sections on demographic information, EHR proficiency and usage, exposure to and interest in AI-powered training, perceived benefits of AI training, perceived barriers to EHR use and views on AI-powered personalised training.
The majority of questions were closed-ended and used Likert scales, dichotomous items (yes/no) or categorical response options. Several open-ended questions were also included to capture qualitative insights into user expectations and system-related challenges.
The questionnaire underwent pilot testing with five healthcare professionals from a separate public hospital in Dodoma who were not part of the final study sample. Feedback from the pilot was used to improve clarity, response logic and relevance. Reliability testing using Cronbach's alpha51,52 yielded values ranging between 0.78 and 0.86 for core domains such as EHR proficiency and training attitudes, indicating acceptable to high internal consistency.
Data collection was conducted in person over a two-week period in early 2025. Participants were provided with study information sheets and consent forms. After obtaining informed consent, they were allowed to complete the paper-based questionnaires during their working hours in designated quiet spaces. Completed questionnaires were reviewed immediately for completeness and then securely stored before being entered into the data analysis.
Measurement of variables
Table 2 summarises the study variables, their operational definitions, measurement approaches and response formats. All multi-item constructs were averaged to form composite scores. Reliability analysis (Cronbach's α = 0.78–0.86) confirmed acceptable internal consistency across domains.
Measurement of study variables.

Source: Authors’ work.
Data analysis
Quantitative data was analysed using Python (3.13.3) and IBM SPSS statistics. Descriptive statistics (means, frequencies, standard deviations) summarised respondent characteristics and perceptions. Inferential tests, including Chi-square tests and correlation analyses, examined the associations between demographics, confidence levels and readiness to adopt AI training.
Qualitative responses were subjected to thematic analysis using three iterative stages: open coding to identify key ideas, axial coding to cluster related concepts and selective coding to form overarching themes. Thematic outputs were compared with quantitative trends to identify convergence or divergence in perceptions.
Ethical considerations
Ethical approval for this study was granted by the University of Dodoma Institutional Research Review Committee (approval reference: MA.84/261/02/ ‘A’/2). The Committee reviewed and approved the study protocol and consent procedures. Permissions were also obtained from Benjamin Mkapa Hospital and Mirembe National Mental Health Hospital. All participants provided written informed consent prior to participation, and the study adhered to the ethical principles outlined in the Declaration of Helsinki.
Results
Participant characteristics
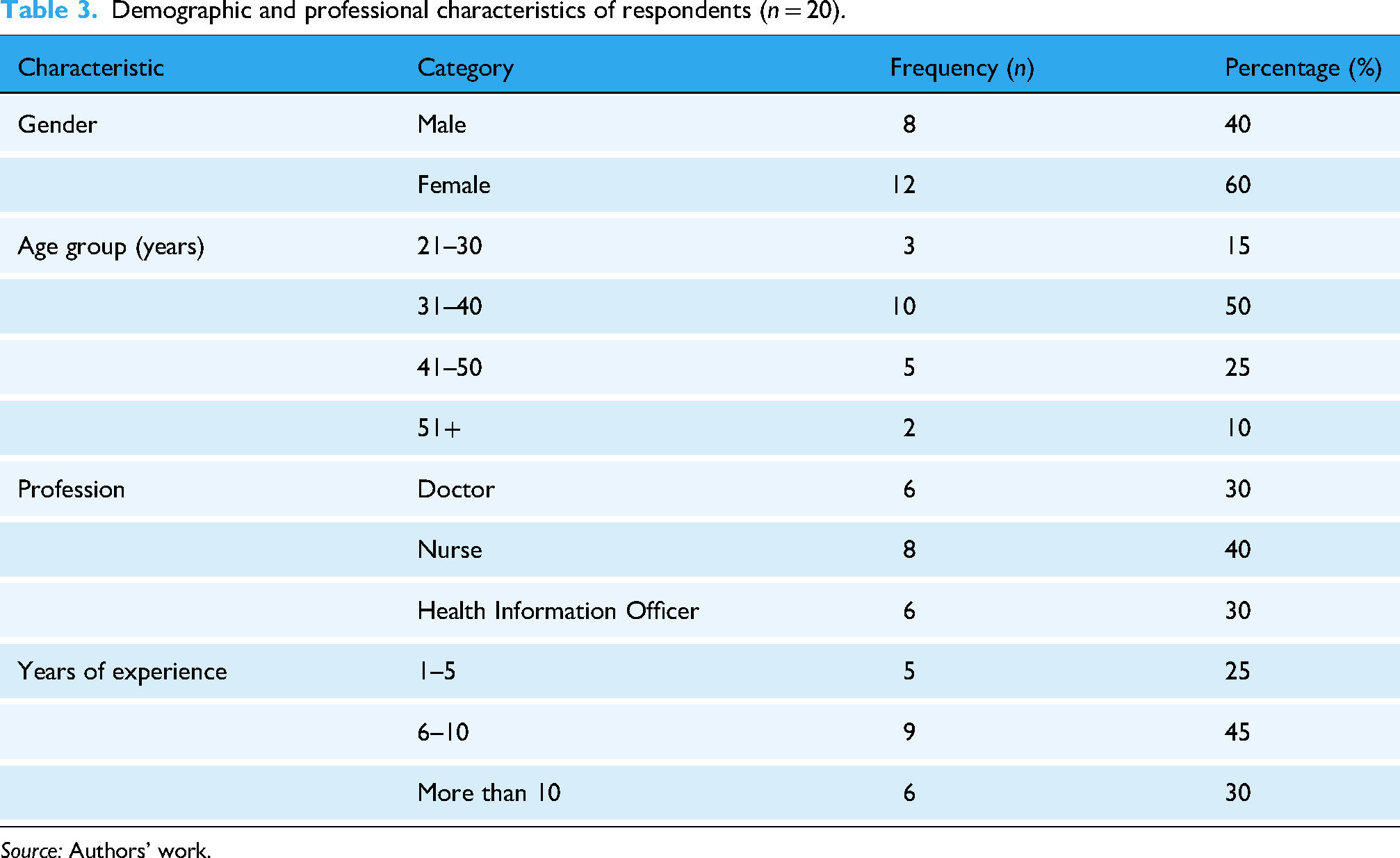
A total of 20 healthcare professionals participated in the study. The sample included a diverse mix of roles, experience levels and demographic profiles. Table 3 summarises the demographic and professional profiles of the participants.
Demographic and professional characteristics of respondents (n = 20).
Source: Authors’ work.
Quantitative results
Exposure to AI-powered training, perceived benefits and EHR proficiency
The majority of respondents (90%) had never received AI-powered, personalised training, with only two participants (10%) reporting any prior exposure. Most relied on traditional learning methods such as printed manuals, peer guidance or short workshops. Despite limited exposure, a large proportion (85%) expressed strong interest in AI-based training and believed it could enhance their confidence and efficiency in using EHR systems.
Self-assessed proficiency levels varied, with half (50%) rating themselves as intermediate users, 25% as beginners and 25% as advanced. These findings indicate a workforce with diverse digital competence and suggest that AI-supported tools could help address uneven skill levels across roles. Table 4 presents the combined distribution of exposure, perceived benefits and proficiency levels.
Exposure to AI training, perceived benefits and EHR proficiency (n = 20).

Source: Authors’ work.
Participants also identified desirable design features for future AI-powered training platforms. The most preferred were interactive, simulation-based modules (75%), real-time in-system guidance (65%) and progress-tracking dashboards (50%). These responses indicate a strong demand for hands-on, adaptive learning solutions that can be integrated into daily workflows without disrupting service delivery. The distribution of these preferences is illustrated in Figure 1.

Preferred features of artificial intelligence (AI)-powered training systems.
Barriers to EHR utilisation and the potential of AI-powered training to address them
Participants described a range of challenges that limit their ability to use EHR systems effectively. The issues raised spanned technical, structural and user-related domains, including difficulties accessing adequate training, navigating digital interfaces and ensuring secure handling of patient data. Others pointed to weak support systems and unreliable infrastructure, which frequently interrupt workflow and reduce confidence in digital documentation. These interrelated barriers contribute to suboptimal engagement with EHR systems and, in some cases, lead to partial or inconsistent use. A detailed overview of these reported challenges is presented in Table 5.
Reported barriers to EHR system utilisation (n = 20).

Source: Authors’ work.
In response to these challenges, participants were asked to consider whether AI-powered, personalised training could serve as a viable solution. The majority (85%) believed that adaptive, user-centred training would help mitigate many of the reported barriers. Specifically, respondents suggested that AI tools could help demystify complex interfaces through real-time guidance, provide refresher support to reduce reliance on help desks and reinforce best practices related to data security. Several participants also emphasised the motivational value of personalised progress tracking and the potential for AI systems to tailor learning to their specific work environments and workflows. Figure 2 provides a visual summary of participants’ views on how AI training could address key challenges.

Perceived potential of artificial intelligence (AI) training to address EHR challenges.
Factors influencing EHR proficiency and training interest
To examine how professional characteristics and workplace context influenced EHR proficiency and attitudes towards AI-powered training, Chi-square and correlation analyses were conducted. The findings indicated no statistically significant relationship between profession and prior exposure to AI-powered training (χ² = 1.64, p = 0.44); exposure was uniformly low across all cadres, suggesting limited access to such tools. A moderate, positive correlation was observed between years of professional experience and self-rated EHR proficiency (r = 0.46, p = 0.04), suggesting that more experienced staff tend to develop greater digital competence through sustained use of the system. Another chi-square test showed a significant difference in the number of reported barriers across professions (χ² = 5.67, p = 0.04), with nurses more likely than doctors or health information officers to cite multiple challenges, particularly inadequate training and limited technical support.
Generally, these results suggest that professional role, experience and access to consistent capacity-building opportunities influence both perceived competence and openness to AI-based learning. Despite generally positive attitudes towards AI training, unequal exposure and persistent structural barriers, particularly among nursing staff, underscore the need for context-specific, adaptive learning interventions that address the diverse needs of users within Tanzania's healthcare system.
Qualitative results
Participants provided written comments in response to open-ended questions within the questionnaire. Their narratives complemented the quantitative findings by explaining why certain barriers persist and how they expect AI-powered training to help. Three main themes emerged from the thematic analysis: (i) training and usability challenges, (ii) expectations of adaptive learning support and (iii) perceived organisational benefits.
Training and usability challenges
Many participants described current EHR training as inadequate and irregular, noting that most learning occurs informally through peer support and mentorship. Several comments referred to “short workshops that do not match real system use” and “difficulty remembering steps when there is no follow-up training.” Respondents also highlighted that EHR interfaces were “not intuitive,” making data entry and retrieval slow and prone to errors. Some participants added that “help is not always available when the system fails” and “we rely on colleagues for support when the IT team is busy.”
Expectations of adaptive learning support
Participants expressed strong optimism that AI-based training could overcome existing barriers by offering real-time, personalised guidance. Comments such as “AI could guide us step-by-step inside the system” and “It should show mistakes immediately and explain the correct procedure” illustrate a clear desire for dynamic, context-aware support. Several respondents envisioned “AI that reminds us when we make data entry mistakes” and “provides short, interactive simulations we can repeat anytime.” They also noted that such systems should “respond to what we do in real time and not require separate training sessions.” Participants also appreciated the idea of “hands-on simulations that allow practice without disrupting patient care,” underscoring the value of practical, low-risk learning environments.
Perceived organisational benefits
Beyond individual skill development, participants viewed AI training as a means to strengthen overall institutional performance. Several noted that “if all staff receive consistent guidance, errors will reduce and reports will be more accurate.” Others commented that “AI could reduce dependence on IT staff because reminders would appear automatically on screen” and “automated refreshers would help maintain quality even when supervisors are not around.” Participants further noted that “AI could remind us about data-entry or security steps,” helping to maintain data-quality and privacy standards.
Integration of quantitative and qualitative findings
Integration of quantitative and qualitative results revealed a clear convergence across both data strands. Quantitative analysis revealed broad enthusiasm for AI-powered training and widespread challenges in EHR use, while qualitative comments explained why these issues persist and how participants expect AI to address these challenges. Table 6 summarises the integrated findings.
Integration of quantitative and qualitative findings.

Source: Authors’ work.
Discussion
This study examined healthcare professionals’ perceptions of AI-powered personalised training for EHR use in Tanzanian public hospitals. The discussion integrates quantitative and qualitative findings through the lens of the STS theory, comparing the results with prior literature and exploring their implications for workforce development in low-resource digital health environments.
Interpretation of the results
A striking finding was the overwhelming interest in AI-powered training, with 85% of participants expressing willingness to adopt such tools and 90% believing that AI could enhance their EHR proficiency. This enthusiasm suggests that healthcare workers in Tanzania recognise the limitations of existing training models and are eager for more dynamic and continuous approaches. Using the STS perspective, this interest can be viewed as a manifestation of the need for better alignment between human and technical subsystems. Artificial intelligence–driven training, by offering adaptive feedback and on-demand guidance, can strengthen this alignment by enhancing user competence within real clinical workflows. Similar patterns have been observed in studies conducted in high-income countries, where AI-assisted training has improved confidence, skill retention and task accuracy.6,7 Research in Kenya and India has also reported early enthusiasm for AI-assisted learning despite limited exposure.11,20 What distinguishes the present findings is the clear link between interest and necessity, healthcare workers view AI not as an innovation for its own sake but as a solution to long-standing gaps in training and system usability that constrain EHR adoption in low-resource settings. 3
The study also confirmed that barriers to EHR use remain significant. Three-quarters of respondents reported inadequate training, 60% cited poor interface usability and half pointed to insufficient technical support. These challenges highlight that EHR implementation in Tanzania has advanced faster than the capacity of users to engage with it effectively. From an STS standpoint, this imbalance indicates poor coordination between the technical design of the EHR and the social structures that support its use. When technology and its users are not co-developed, the system becomes unstable, leading to workarounds and partial adoption. Artificial intelligence–based personalised training could serve as a corrective mechanism by embedding learning into everyday use and supporting continuous skill reinforcement. These observations mirror evidence from other settings showing that traditional one-off workshops are ineffective for building lasting digital competence.2,16
Participants’ preferences for simulation-based modules (75%) and real-time in-system guidance (65%) further emphasise a desire for experiential, hands-on learning. Rather than classroom-based instruction, healthcare professionals prefer training integrated directly into their workflow. The STS framework explains this as a move towards socio-technical integration, where technology not only delivers information but adapts dynamically to the social environment of work. Comparable findings have been reported in studies where AI simulations and virtual trainers enhanced user confidence and accuracy.17,18 In contexts with limited supervision and high workloads, such adaptive and context-aware systems, can also reduce dependence on external trainers, making skill development more sustainable.34,37
The results also revealed professional differences in exposure and perceived barriers. Nurses were more likely than doctors or health information officers to report multiple difficulties, particularly inadequate training and weak technical support. This reflects underlying institutional hierarchies that often limit nurses’ access to structured capacity-building opportunities. Within the socio-technical framework, such disparities represent imbalances within the social subsystem that undermine overall system optimisation. Similar trends have been documented elsewhere, where nurses experienced greater frustration and lower digital confidence because of insufficient training and support.2,25 Addressing these disparities will require context-specific interventions that tailor AI-supported training to different professional groups rather than applying uniform models.
Interestingly, participants also viewed AI training as having organisational benefits beyond individual skill improvement. Many anticipated that automated feedback and refresher prompts could enhance documentation accuracy, reduce reliance on IT personnel and improve overall data quality. This interpretation is consistent with the STS view that technology should not merely support individuals but help the wider system achieve equilibrium between human competence, organisational routines and technical infrastructure. Studies in other contexts echo this potential: AI-enabled learning environments have been shown to foster institutional consistency and efficiency by embedding automated support mechanisms into routine operations.27,35
Despite the optimism, concerns about privacy, data security and trustworthiness emerged among more than half of the respondents. Trust in automated systems remains a crucial determinant of adoption, especially in clinical settings where accountability and confidentiality are central. Within the STS perspective, this highlights the need for cultural and organisational readiness alongside technological innovation. Without clear policies on data protection and transparent communication about AI functions, even well-designed systems may struggle to gain user confidence. The literature similarly points out that perceived security and trust strongly influence technology acceptance.44,45 These concerns underline that successful AI integration in Tanzanian healthcare will depend not only on technological feasibility but also on governance frameworks that safeguard ethical standards and build user assurance.
The findings depict a health workforce that is both realistic and receptive. Healthcare professionals understand the limitations of current EHR training and recognise the potential of AI-supported systems to provide sustained, personalised learning. When interpreted through the STS lens, these results suggest that Tanzania's digital health transformation must prioritise co-evolution of human capability, organisational support and technological design. Artificial intelligence–powered training offers a promising pathway towards this integration by reinforcing competence at the point of use, reducing dependency on scarce technical staff and promoting system reliability. However, for such innovations to succeed, they must be accompanied by investment in infrastructure, inclusive training strategies across cadres and institutional policies that cultivate trust and accountability.
Implications of the study
The findings of this exploratory study hold several implications for practice, policy and future research in digital health workforce development within Tanzania and other similar resource-constrained contexts. At the practical level, the results highlight the limitations of conventional training approaches in developing EHR proficiency. One-off workshops and peer demonstrations, which dominate current training practices, fail to accommodate differences in users’ skill levels and learning speeds. The strong interest in AI-supported learning expressed by participants highlights the need to adopt more continuous, adaptive and context-aware training models. Implementing AI-driven platforms could enable healthcare professionals to learn while working, receive instant feedback and reinforce their knowledge through simulation, all without disrupting service delivery. This would also reduce dependence on limited IT support staff and promote self-efficacy among users.
At the organisational level, the findings suggest that integrating AI-based training aligns well with the socio-technical systems perspective, which advocates for joint optimisation of human and technical subsystems. Hospitals and health facilities should therefore view AI training not merely as a technological upgrade but as part of a broader organisational learning strategy. To realise its full potential, institutional leaders must ensure that such systems are embedded within existing operational frameworks, supported by policies on digital competence development, supervision and data quality assurance. This would help establish a culture of continuous learning and system improvement, strengthening the overall reliability and efficiency of digital health operations.
From a policy standpoint, the study offers timely evidence to inform the implementation of Tanzania's Digital Health Strategy, particularly its workforce capacity-building agenda. While the national strategy recognises training as a key enabler of digital transformation, there is limited focus on personalisation and long-term skill retention. Introducing AI-powered training within this framework could modernise national training standards by promoting adaptive learning, local content development and scalable delivery models. Policymakers should also ensure that adequate infrastructure investments, such as reliable internet connectivity, data security measures and interoperability with national EHR platforms support such initiatives.
The study further raises important considerations regarding ethics, trust and data governance. Although participants expressed optimism, concerns about data privacy and system reliability reveal that readiness for AI adoption extends beyond technical capacity. Regulatory bodies and implementing partners must therefore develop clear guidelines for AI ethics in healthcare, focusing on transparency, accountability and fairness in automated learning systems. Building user trust through awareness and participatory design will be essential for the sustainable integration of AI into health workforce development.
Ultimately, the results have several implications for future research. Given the small sample size and exploratory design, future studies should adopt larger and more diverse samples to capture variations across facility types, regions and professions. Experimental or quasi-experimental studies could evaluate the actual impact of AI-powered training on user performance and patient outcomes. Mixed-methods designs would also help explore deeper contextual issues, including cultural perceptions, leadership influences and infrastructural readiness. Collectively, these efforts would advance the evidence base on how intelligent learning tools can be effectively localised and scaled across low- and middle-income healthcare systems.
In sum, this study suggests that AI-powered personalised training represents a feasible and desirable pathway for enhancing EHR proficiency in Tanzania. By situating the intervention within the socio-technical realities of healthcare work, stakeholders can move towards a more adaptive, sustainable and user-centred model of digital capacity building that strengthens both individual competence and organisational resilience.
Contribution of the study
This study contributes to the growing body of knowledge on digital health capacity building by providing one of the earliest empirical examinations of how healthcare professionals in a low-resource setting perceive AI-powered personalised training for EHR use. While most prior studies have focused on technical feasibility or performance outcomes in high-income contexts, this research shifts the attention to user perspectives and organisational realities within Tanzania's public healthcare system. In doing so, it offers a nuanced understanding of readiness, perceived benefits and contextual barriers that influence the potential adoption of AI-based learning interventions.
A key contribution lies in the integration of the STS theory as the interpretive framework. By applying this lens, the study moves beyond TAMs that focus solely on individual attitudes, instead positioning AI training as part of an interconnected system of users, tools and institutions. This theoretical framing highlights how technological innovation, human capability and organisational culture must evolve together for successful digital transformation. It also provides a conceptual foundation for future intervention research that aims to strike a balance between technical functionality and social and institutional alignment.
Empirically, the study extends existing literature by offering early evidence from Tanzanian hospitals, demonstrating that healthcare workers are not only aware of their training deficiencies but are also open to innovative, adaptive learning solutions. The strong preference for simulation-based and real-time guidance features indicates that AI-supported learning could address long-standing challenges of intermittent training, limited supervision and inconsistent technical support. These insights provide actionable guidance for policymakers, software developers and hospital administrators designing user-centred AI training tools tailored to local infrastructure and workforce conditions.
Methodologically, the study contributes by combining quantitative and qualitative data within an exploratory cross-sectional design, allowing for both statistical description and contextual interpretation. Although the sample was small, this mixed descriptive approach provided convergent evidence of enthusiasm for AI-supported learning and revealed the underlying reasons behind it. The approach demonstrates the value of exploratory, perception-based assessments as a preliminary step in digital health innovation, helping to identify design priorities before larger experimental evaluations are conducted.
Finally, the study makes a practical contribution by informing the design of scalable capacity-building strategies under Tanzania's national digital health agenda. It provides a basis for integrating adaptive AI tools into health workforce development frameworks and underscores the importance of co-evolution between technical infrastructure and human capacity. Beyond the national context, the findings offer transferable lessons for other LMICs seeking to bridge digital literacy gaps while adopting advanced learning technologies responsibly and sustainably.
In essence, this study makes a conceptual, empirical and practical contribution by establishing an initial understanding of how AI-supported training can be integrated within the socio-technical realities of Tanzanian healthcare. It lays the groundwork for more rigorous, intervention-based research aimed at testing the real-world feasibility and effectiveness of such systems, ultimately supporting a more digitally competent and confident health workforce.
Limitations of the study
This study had several limitations that should be considered when interpreting the findings. The small sample size of twenty participants from two hospitals limits generalisability to the wider Tanzanian health workforce. The cross-sectional design captured perceptions at one point in time and cannot determine changes or causality.
Data was based on self-reported measures, which may be affected by bias or inaccuracies in assessing one's competence. The qualitative input, though useful, was brief and lacked the depth that interviews or focus groups could provide. Moreover, participants evaluated AI-powered training conceptually rather than through actual experience, meaning responses reflect expectations rather than outcomes.
Finally, while the STSs framework guided interpretation, relationships among variables were not statistically tested. Future studies should use larger samples, longitudinal designs and real pilot interventions to validate these early insights.
Conclusion
This study explored healthcare professionals’ perceptions of AI-powered personalised training for improving EHR use in Tanzanian public hospitals. The findings revealed strong interest in such training, reflecting awareness of existing gaps in digital competence and the shortcomings of current one-off workshops. Participants believed that adaptive, simulation-based learning could enhance confidence, efficiency and data accuracy while reducing dependence on limited technical support.
Viewed through the STSs lens, the results highlight that improving EHR utilisation requires simultaneous attention to human capability, organisational support and technology design. Artificial intelligence–supported training offers a potential bridge between these subsystems by embedding continuous learning within daily workflows.
Although limited by its small, cross-sectional sample, the study provides early evidence of readiness for AI-enabled capacity building in Tanzania. It establishes a foundation for future intervention studies to assess feasibility, user trust and real-world impact. Strengthening digital literacy through intelligent, user-centred training could play a crucial role in achieving sustainable EHR adoption and advancing the country's digital health agenda.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251404506 - Supplemental material for Perceptions of AI-supported training for electronic health record use in Tanzania: A preliminary exploratory study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251404506 for Perceptions of AI-supported training for electronic health record use in Tanzania: A preliminary exploratory study by Augustino Mwogosi, Mathew Maganga, Secilia Gregory, Upendo Msaru, Anitha Amos and Jeremiah Kajala in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank the management and staff of Benjamin Mkapa Hospital and Mirembe National Mental Health Hospital for their cooperation and participation. We also acknowledge colleagues from the University of Dodoma for their input during tool development and piloting.
Ethical considerations
Ethical approval for this study was granted by the University of Dodoma Institutional Research Review Committee (approval reference: MA.84/261/02/ ‘A’/2). The Committee reviewed and approved the study protocol and consent procedures. Permissions were also obtained from Benjamin Mkapa Hospital and Mirembe National Mental Health Hospital. All participants provided written informed consent prior to participation, and the study adhered to the ethical principles outlined in the Declaration of Helsinki.
Consent to participate
Written informed consent to participate in the study was obtained from all respondents prior to data collection.
Consent for publication
Not applicable. This study did not collect any identifiable personal information, images or recordings requiring individual consent for publication.
Author contributions
Conceptualisation: Augustino Mwogosi.
Methodology: Augustino Mwogosi, Mathew Maganga.
Data Curation: Secilia Gregory, Anitha Amos.
Formal Analysis: Augustino Mwogosi, Upendo Msaru.
Writing-Original Draft: Augustino Mwogosi, Jeremiah Kajala.
Writing -Review and Editing: All authors.
Supervision: Augustino Mwogosi.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.