
Abstract
Introduction
The prevalence of many diseases is increasing worldwide. There are various reasons for this, including environmental and climate change, as well as unhealthy lifestyles.1,2 Recent technological advances and the increasing digitalisation of healthcare have the potential to address these challenges. In the dynamic field of healthcare, the importance of wearable technologies for continuous monitoring is constantly increasing. These technologies have the potential to effectively monitor patients, improve diagnoses and optimise therapies by tailoring them to the individual needs of each individual.3,4 In the present context, smart wearables are electronic devices designed to be worn close to or on the surface of the skin. These devices are capable of continuously collecting, analysing and transmitting data related to various body signals, including vital signs, biomarkers and environmental information.5–9 An important application of wearable technology is ecological momentary assessment (EMA), which evaluates a person's behaviour and experiences in their natural environment in real time.10,11 This method provides valuable insights into a person's state of health. Ecological momentary intervention (EMI) uses the data to take timely action and improve patient care through personalised and contextualised health strategies.10,11 These applications demonstrate the potential of wearable devices to provide adaptive and timely healthcare treatments. Around 28% of the German population used wearables to monitor their physical activity in 2016.12,13 Wearables are different types of devices such as smartwatches, fitness trackers, rings, hearables and special devices that can collect data via the skin.14–21 Innovative wearables can capture a whole range of measurement data that goes beyond conventional functions such as step counting or heart rate. One possible application of this technology is, for example, the monitoring of alcohol consumption.22,23 This enables continuous and non-invasive measurements that provide both healthcare professionals and individuals with valuable information to detect significant changes in health status. In addition, this technology provides an innovative way to address health issues and encourage people to adopt healthier lifestyles. Wearables can be divided into different functional subtypes, such as microneedle patches, 12 electronic trans-epidermal tattoos used for non-invasive cortisol measurement via sweat,9,12 and e-textiles,14,24 which are characterized by the integration of sensors into clothing.15,24 The use of wearables in healthcare practice could support and optimize diagnostic and treatment decisions through the continuous monitoring and processing of data collected on an ongoing basis.17,24,25 Furthermore, patients can become more involved in the monitoring of their health status, resulting in possible time savings and cost reductions for patients and physicians.9,26–28 However, studies on the acceptance of wearables for health monitoring in connection with data sharing in the daily routine are limited.
The primary aim of this research study is to investigate the acceptance and usage behaviour of wearables in Germany. The study aims to investigate the willingness of individuals to use wearables for health monitoring, to identify the factors that influence the use of wearables and to examine the associated risks and barriers. In addition, the study aims to capture the demographic characteristics of wearable users and non-users.
Methods
Study design and population
This cross-sectional study adheres to the STROBE statement and guidelines.29,30 Data collection was conducted from July to September 2022 using a convenience sampling technique. Participants were recruited through a multi-channel approach that involved both online and offline methods. The online questionnaire was disseminated via various websites (e.g., university, forums), as well as popular social media platforms, selected for their high traffic and accessibility. In addition, paper-based questionnaires were distributed at an international fair (“Interforst”) that provided access to a diverse group of interested attendees. This venue was part of a health campaign by the German Social Insurance for Agriculture, Forestry, and Horticulture. For this study, the sample size calculation was performed using G-Power 3.1.9.6, 31 with an effect size of 0.2 being specified. The probability of a Type I error was set at α = 0.05, while the probability of a Type II error was set at β = 0.2, resulting in a power of 80%. The total sample size calculated for our study was 788 participants. This study was approved by the ethics committee of this study was approved by the ethics committee of the Technical University Munich (reference number 2022-314-S-NP).
Inclusion criteria and missing values
Inclusion criteria for participation were being aged ≥18 years and written informed consent. Participants who did not provide information on the acceptance of wearables (n = 93) were excluded. To ensure data quality, participants who answered less than 80% of the questionnaire were excluded from analyses. For the Poisson regression, a further 12 participants had to be excluded due to missing values.
Study questionnaire
A self-designed questionnaire was used. Questions on the acceptance of wearables were based on previous acceptance studies32–40 that focussed on digital tools and wearables such as fitness trackers. The selected questionnaires were first translated into German. To ensure that our questionnaire comprehensively covered all relevant aspects of user acceptance, we designed it considering key components from the Technology Acceptance Model (TAM) and the Unified Theory of Technology Acceptance and Use (UTAUT). TAM, developed by Davis et al.,
40
is based on two main determinants: perceived usefulness and perceived ease of use. For our study, these concepts were adapted to assess beliefs about enhancing health monitoring through wearables and the effortlessness of their use. UTAUT, proposed by Venkatesh et al.,
41
extends TAM by including performance expectancy, effort expectancy, social influence, and facilitating conditions. In the context of our study, these constructs helped assess beliefs about the wearables. In the paper by Yang et al.,
35
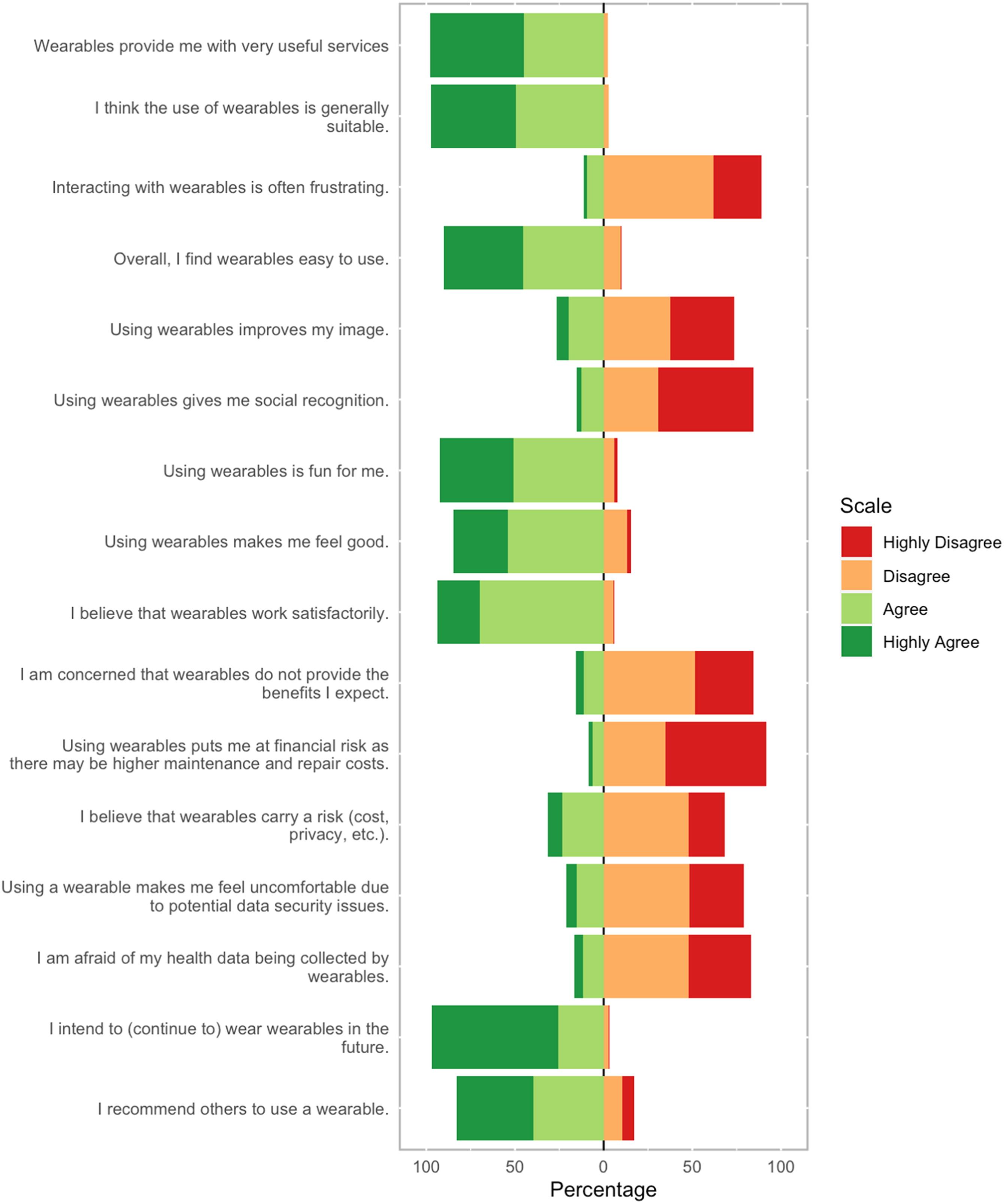
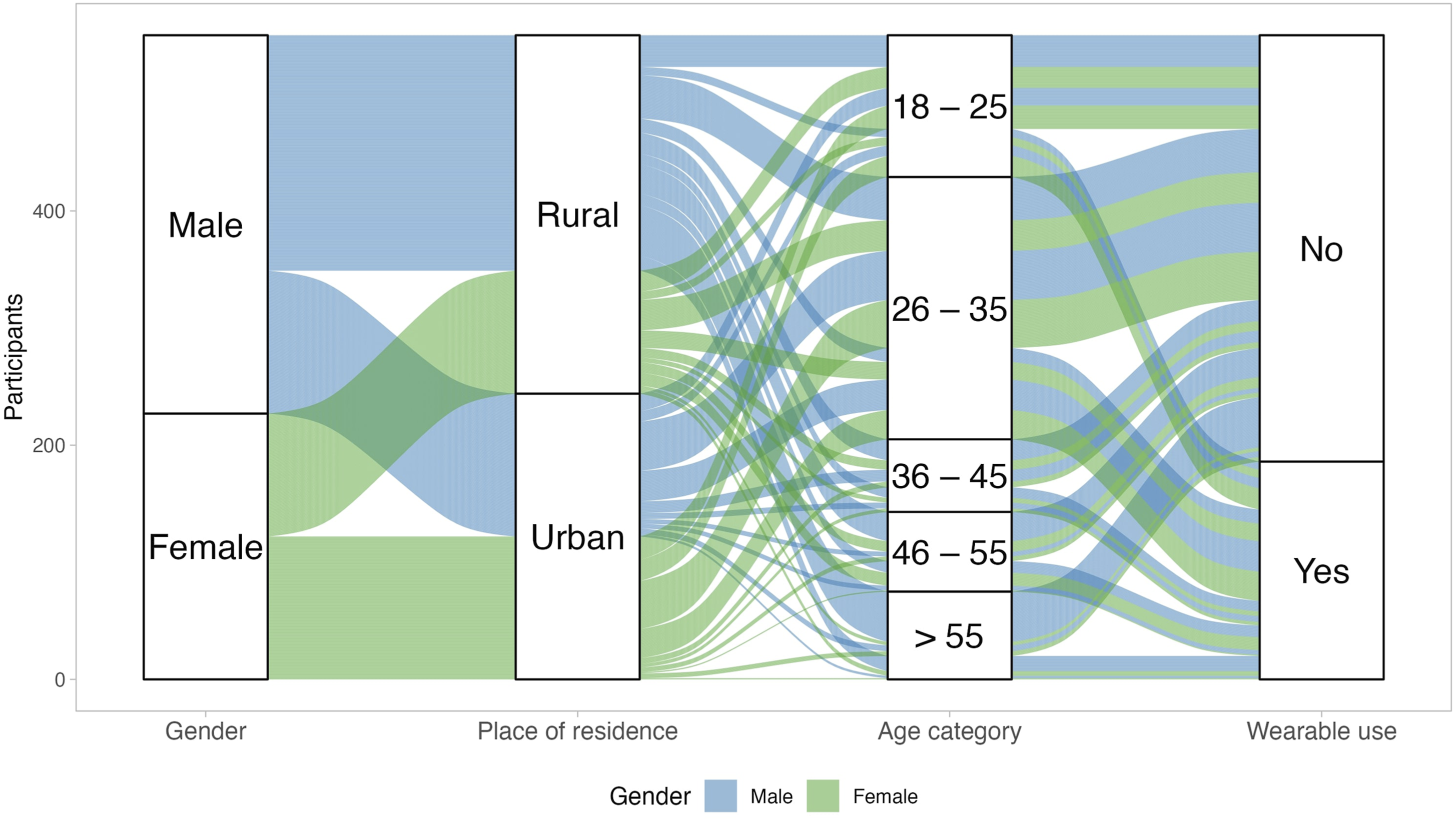
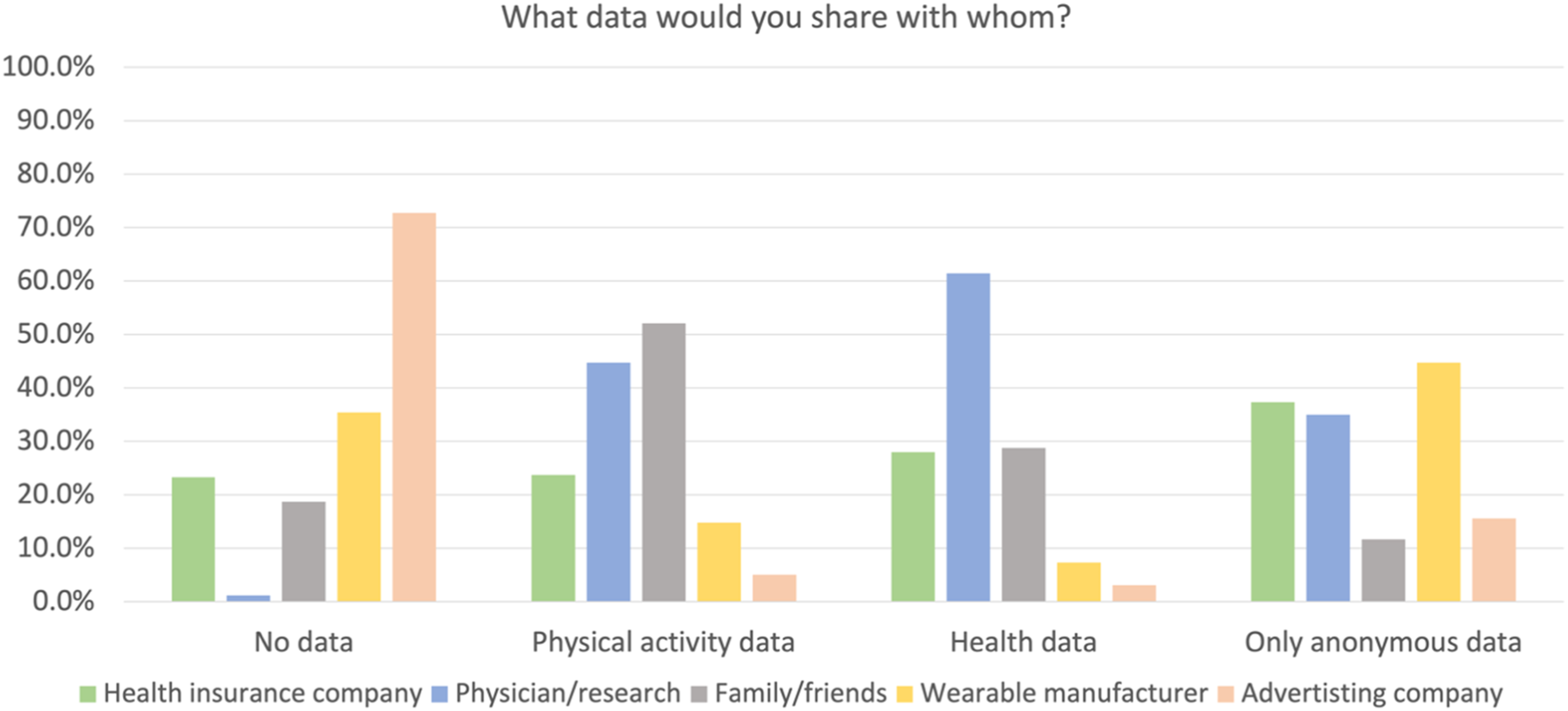
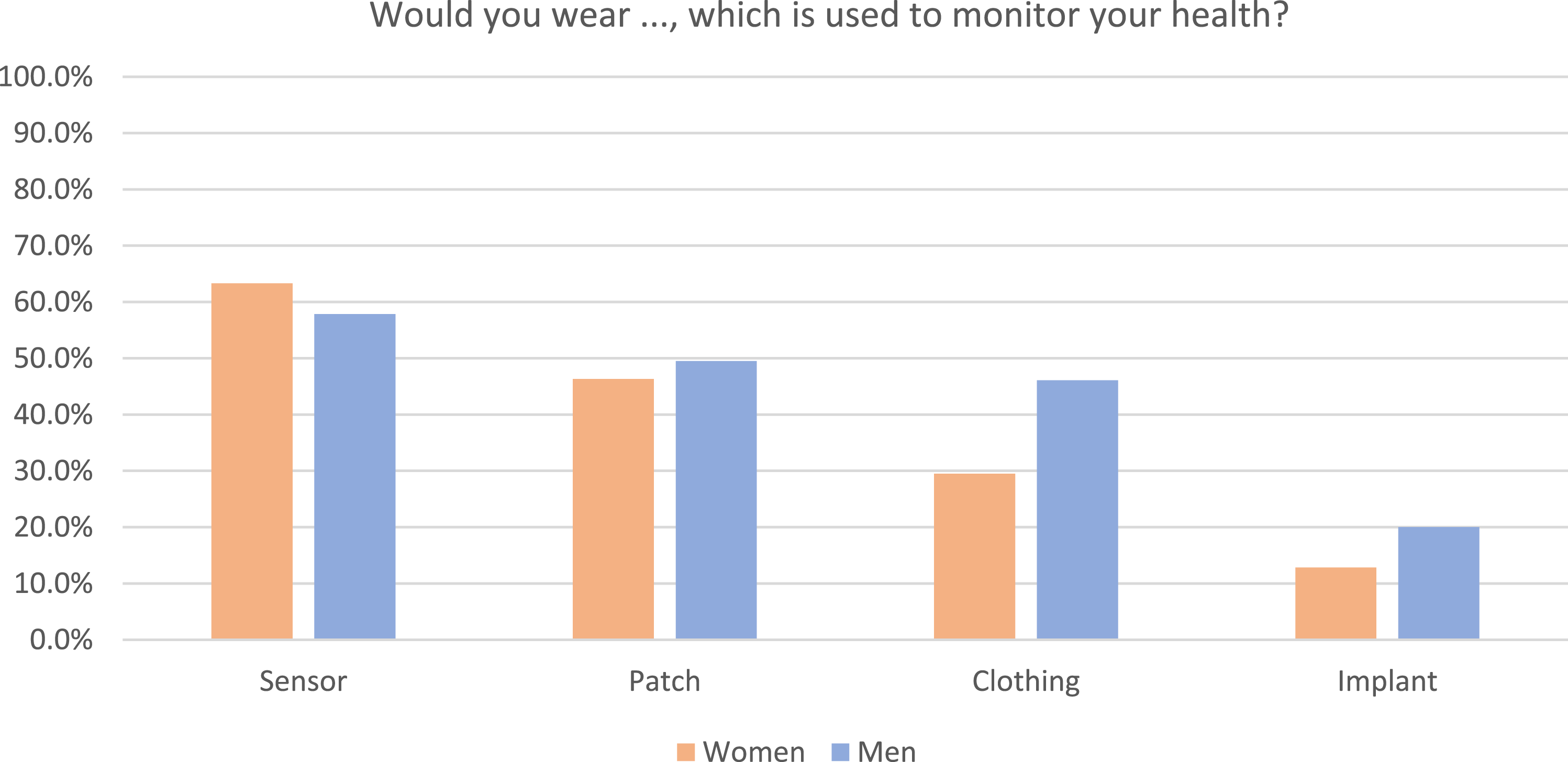
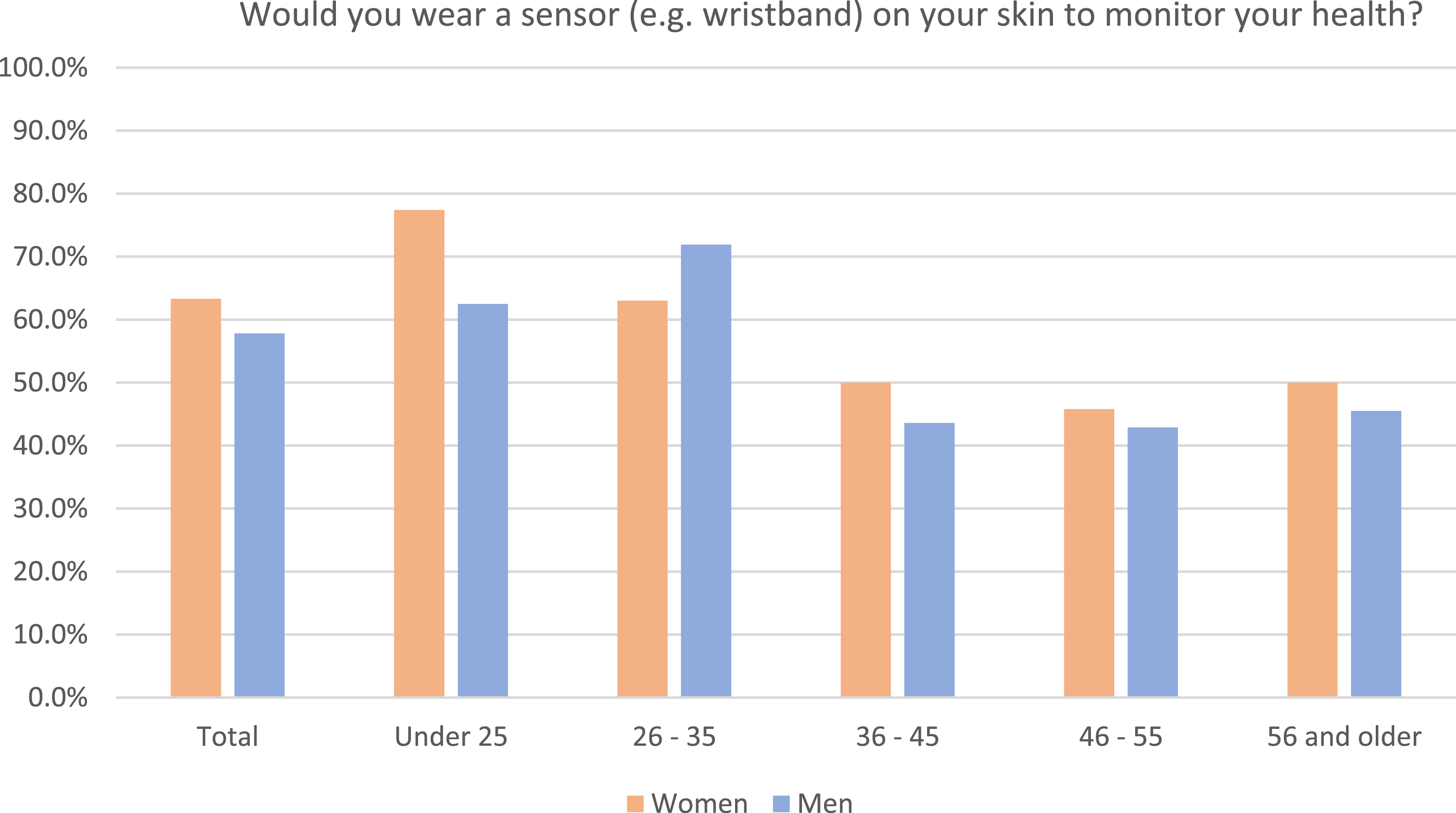
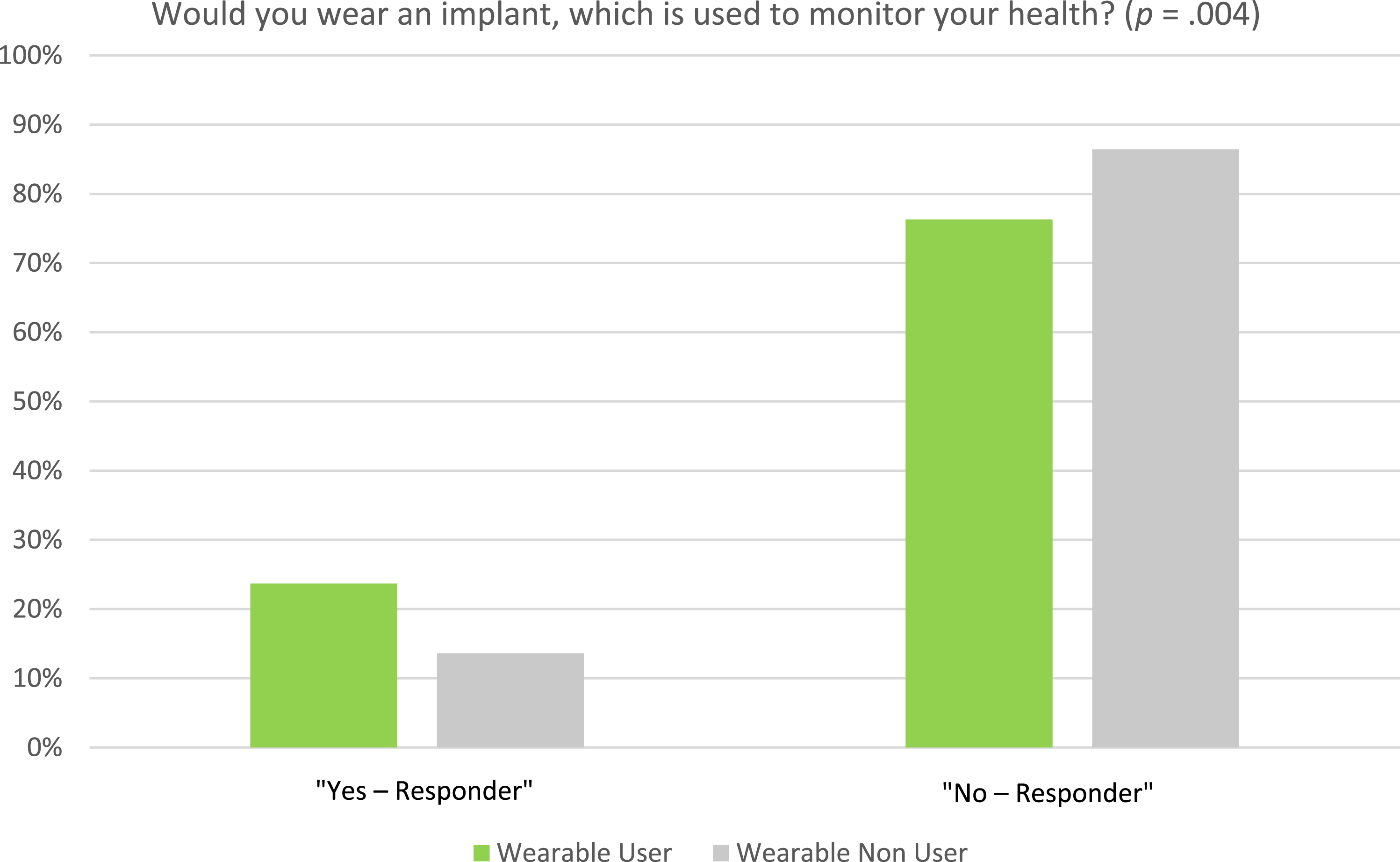
the acceptance questions based on TAM and UTAUT are tested validated instruments. The questionnaire was reviewed by three authors with expertise in dermatology, public health, and statistics. Prior to the main study, we conducted a pilot test with five randomly selected participants. This step allowed us to gather initial feedback and make minor revisions, such as expanding the answer options for closed questions or the translation. Forty-two questions were divided into four sections: 1. Sociodemographic data and current usage of wearables (Table 1, Figure 1) 2. Usage behaviour of wearables among current users (Table 2, Figure 2) 3. Willingness to share data from wearable and with whom (Figure 3) 4. Willingness to wear wearables for health monitoring in the future (e.g., implants) (Figure 4–6) Characteristics of respondents. Responses and attitudes among wearable users. Frequency of use and type of measurements among wearables users (n = 186) as well as associated risk of and barriers to using wearables (n = 517). aSome participants owned more than one wearable. bOther: Chest straps. cTotal sums may exceed 100%, as multiple answers were possible. dOther: Dependence, data validity, permanent monitoring not desirable. Characteristics of participants and wearable use. Frequency of willingness to share data measured by wearables for different types of data (total respondents = 257). Frequency of willingness to wear various wearables (men and women who responded with “yes” in each category). Frequency of willingness to wear a sensor to monitor health (“Yes Responder” of total 257 responders). Frequency of willingness to wear an implant to monitor health (“Yes-responder” of total 257 responders).
Wearables were defined in the survey as any wearable electronic device that is worn on the body to collect and analyse information about e.g., body signals and/or environmental data. 42 Except for age, variables were predominantly collected as nominal or ordinal variables. The age of the study participants was divided into five age groups to compare between younger and older users: 18 to 25 years, 26 to 35 years, 36 to 45 years, 46 to 55 years, and 56 years and older. Furthermore, study participants were classified according to their place of residence, physical activity, monthly income, and education level. Places of residence were classified as rural communities (<5,000 residents), small towns (5,000–19,999 residents), medium-sized towns (20,000–99,999 residents), and large towns (>100,000 residents). To assess the physical activity per week, we employed a question from the German-validated version of the European Health Interview Survey (EHIS-PAQ). 43 “How much time in total do you spend on sports, fitness or recreational (leisure) physical activities in a typical week?”. For comparison between participants with different physical activity levels, the variable was included with four different categories (“< 1”, “1 < 2”, “2 < 4”, “>4” hours). For comparison between different incomes, the variable “salary per month (€)” was included with five different categories (“<1,000” to “>4,000”). The variable “education level” comprises three categories, including “lower than high school degree”, “High school degree”, and “University/doctoral degree”. Study data were collected, digitised, and managed using REDCap (Research Electronic Data Capture, Vanderbilt University).44,45
Statistical methods
Data management and statistical analyses were conducted using R version 4.2.146,47 and IBM SPSS Statistics 28 (IBM Corporation, Armonk, NY, USA). All variables were analysed descriptively using absolute and relative frequencies. Associations between current wearable users and non-users with other variables were tested using Chi-square tests. The Generalized Linear Model (GLM) with a Poisson distribution48,49 was employed to investigate the association between the use of wearable devices and various predictors, including gender, place of residence, age, physical activity per week, survey location, and monthly salary. Results of the regression model are presented as prevalence ratios (PR) with their 95% confidence interval (CI). The significance level was set to α = 0.05.
Sensitivity analysis
To ensure data quality, participants who answered less than 80% of the questionnaire were excluded and not included in the analyses. For the Poisson regression, missing values were excluded from the analysis. Sensitivity analyses were conducted to quantify response biases due to missing information regarding the willingness to use wearables. For this purpose, the acceptance of wearables was calculated for two fictitious scenarios in which all individuals with missing information on the willingness to use wearables were either open (scenario 1) or not open (scenario 2) to using wearables. Another sensitivity analyse All study participants were included in this analysis. In addition, confidence intervals were calculated using the bootstrap method (1000 bootstrap samples, α = 5).
Results
Overview
In terms of the survey administration, 235 (42.7%) participants completed the survey using a paper and pencil questionnaire, while 315 (57.3%) participants completed the survey online. Of the 403 online questionnaires initiated, 315 were successfully completed, resulting in an online response rate of 78%. 50
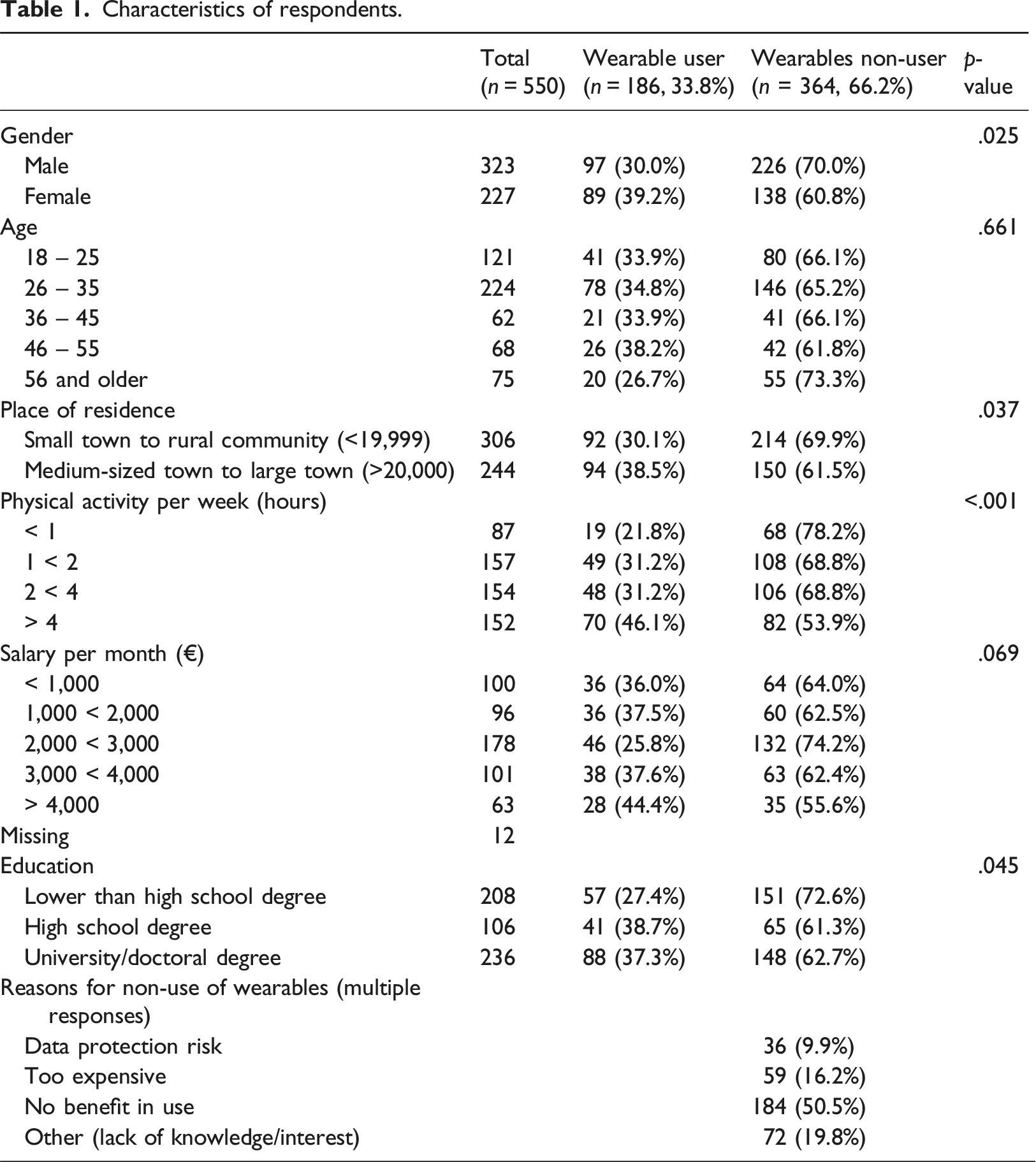
A total of 550 participants were included in this study (Table 1). Participant age ranged between 18 and 81 years, and the mean age was 36.6 years (standard deviation: 13.9). A total of 186 participants (33.8% of the total sample) reported using wearables, with 39.2% of female respondents and 30.0% of male respondents using wearables (p = .025). There was no statistically significant difference in the distribution of wearable users across age groups. For participants aged 18 to 55, 33.9% to 38.2% of participants reported using a wearable depending on the age group (p = .661). Although the proportion of participants reporting wearable use decreased to 26.7% in the age Group 56 years and older, the difference was not statistically significant (p = .661). There were more wearable users in the medium-sized and large towns (38.5%) than in the small towns and rural communities (30.1%) (p = .037).
Regarding physical activity, the largest proportion of wearable users (46.1%) was observed for the category of “>4” hours of exercise per week, which was significantly higher than the percentages observed in the categories with less than 4 h of exercise per week (p < .001). Although the proportion of wearable users was highest in the category of monthly income of more than 4,000€ (44.4%), the difference was not statistically significant when compared to categories for lower monthly income (p = .069). The proportion of wearable users was higher in the category of “High school degree” (38.7%) and “University/doctoral degree” (37.3%) than in the category of “lower than high school degree” (27.4%) (p = .045).
Reasons for non-use
The most prevalent reason, mentioned by 50.5% of non-users, was the perception of no tangible benefit from using wearables. For 16.2% of non-users, cost presented a substantial concern. Approximately 9.9% expressed concerns about data protection and privacy associated with wearables. Furthermore, about 19.8% of non-users fell into the “Other” category, citing various reasons such as a lack of knowledge or interest in wearables.
Usage patterns
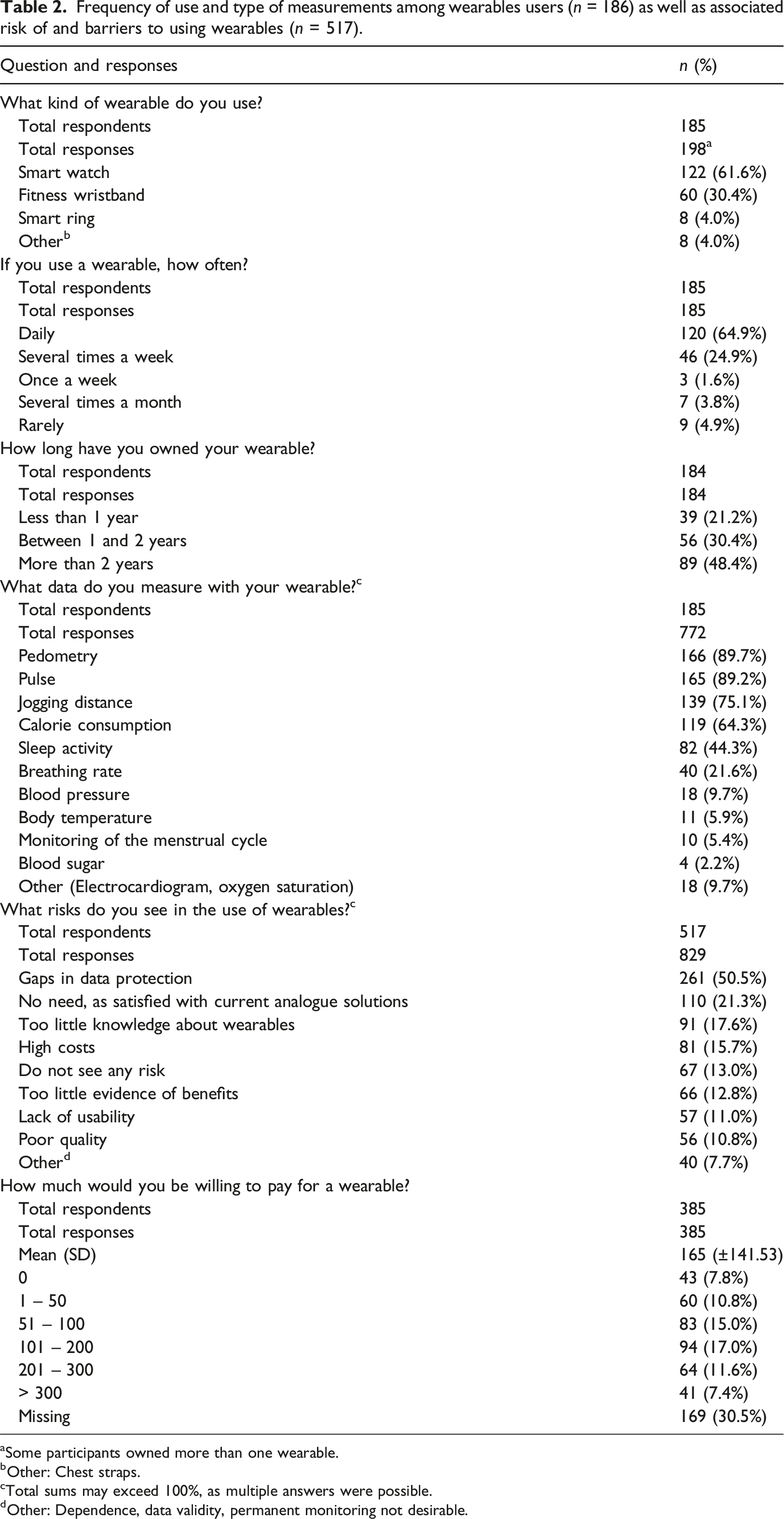
Among all 186 wearable users, 122 people owned a smartwatch, 60 people owned a fitness wristband, eight people owned a smart ring, and another eight owned other wearables like chest straps for sports or smart patches for insulin measurement (Table 2). About 90% of users stated that they use their wearable more than once a week, of which 64.5% used it daily. The most common measurements recorded with the wearables were the number of steps walked (89.7%), pulse (89.2%), distance jogged (75.1%), calories consumed (64.3%), and sleep activity (44.3%).
Data sharing and sensor use
Our results show that 61.5% of respondents (158 out of a total of 257 respondents) would share their wearable health or physical activity data (44.7%) with their doctor or a researcher (n = 273) (Figure 3). In addition, 42.7% of participants would only share anonymous data with wearable manufacturers. The willingness to wear a health monitoring sensor on the skin was found in 57.8% of men and 63.3% of women among all respondents (Figure 4). (Figure 5) Participants were more willing to wear a (sensor) patch (46.3 % men, 49.5 % women) than a garment with sensors (46.1 % men, 29.5 % women) or a health monitoring implant (20.0 % men, 12.8 % women) (Figure 6). In the wearable user category, the willingness to wear an implant (23.7 %) is higher than in the non-user category (13.6 %) (Figure 6).
Concerns about wearables
Overall, 517 participants responded to the question about the risks and barriers they associate with the use of wearables (Table 2). In most cases, concerns were raised about data protection (50.5%), followed by “no need for wearables” (21.3%), “too little knowledge about wearables” (17.6%), and “high costs” (15.7%). Among all respondents, 13.0% saw no risk at all in using wearables, and 40 respondents provided additional comments specifying the risks they associated with the use of wearables, such as dependence on the device, no confidence in data validity of measurements, and rejection of permanent monitoring.
Factors influencing the use of a wearable
Results of the Poisson regression with wearable use as a dependent variable and gender, place of residence, age, and physical activity as independent variables.
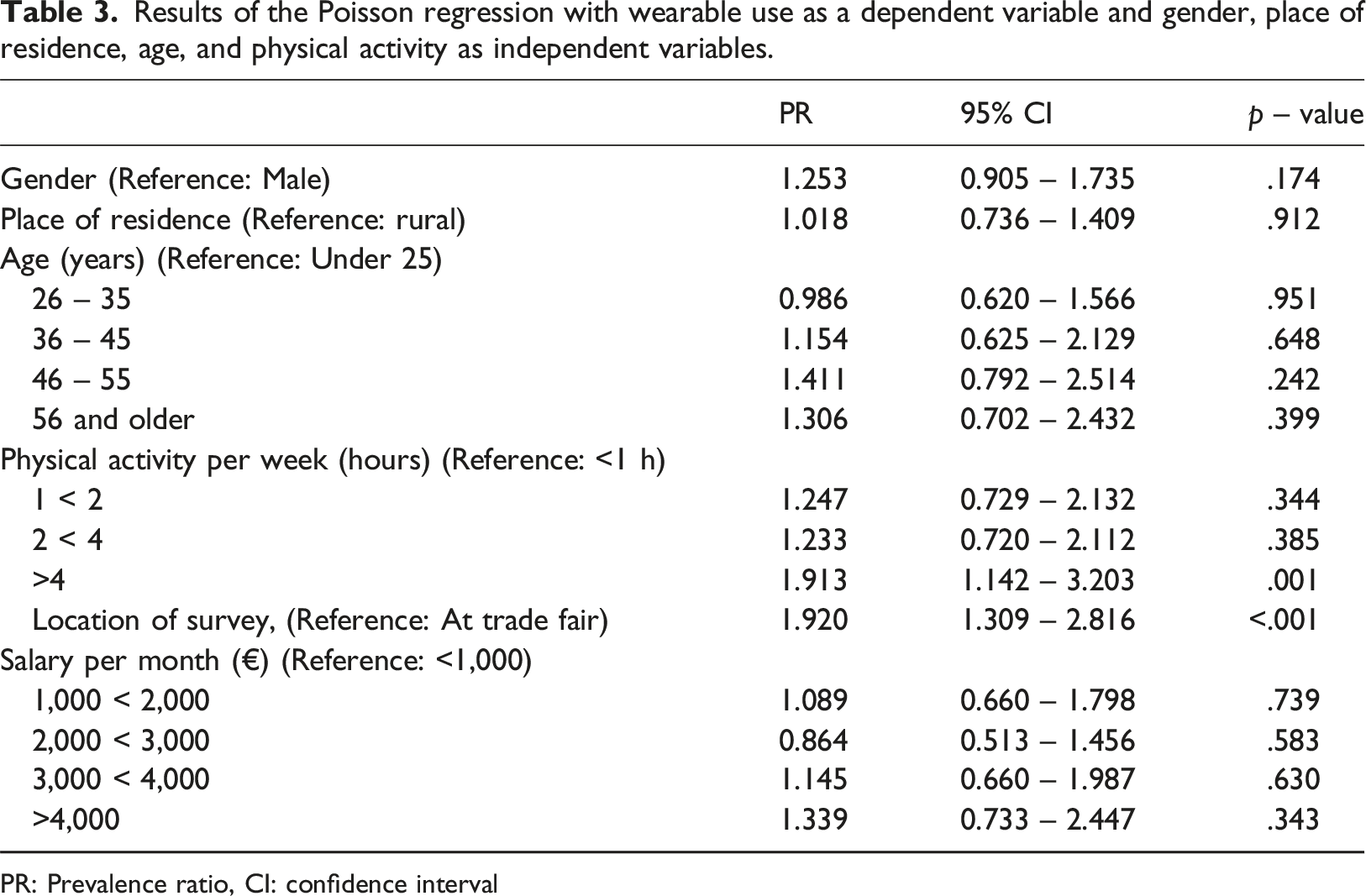
PR: Prevalence ratio, CI: confidence interval
Sensitivity analysis
The sensitivity analyses confirmed the robustness of the primary results (Appendix 1). One analysis involved participants with paper-based questionnaires where gender had a significant effect on wearables use (PR = 2.280, 95% CI: 1.213 – 4.289, p = .011). Further analysis with online questionnaire participants showed that higher levels of physical activity (>4 h per week) significantly predicted wearables use (PR = 1.917, 95% CI: 1.021 – 3.599, p = .043), mirroring the primary findings. No other factors such as place of residence, age or salary showed significant effects.
TAM and UTAUT constructs in wearables acceptance
In the analysis of the constructs of TAM and UTAUT, the reliability assessment for the construct of perceived usefulness resulted in a Cronbach’s alpha of 0.798. The construct of perceived ease of use showed a Cronbach’s alpha of 0.444. A Cronbach’s alpha of 0.62 was determined for the intention to use construct.
Discussion
Key results
The main objective of our study was to investigate the acceptance and usage behaviour of wearables in the German population. The results showed that 33.8% of participants reported using a wearable - mainly to measure physical activity. In addition, a high proportion of respondents (57.8% of men and 63.3% of women) showed a willingness to use wearables with health monitoring sensors, indicating a positive attitude towards modern health technology. 50 This trend was more pronounced among women and people with higher activity levels, consistent with other studies.51,52 Individuals who set health-related goals, such as those related to physical activity, will likely find wearables useful for monitoring their progress toward these goals.50,51,53 Regarding data-sharing preferences, participants showed a clear inclination to share health data with healthcare providers rather than other organisations, highlighting an important aspect of privacy and security in digital health. These aspects align with other results of studies in this field.8,51,54,55
Innovative wearables may have great potential for empowering individuals, especially in the medical field, when it comes to diagnosis, behavioural changes, and monitoring of chronic diseases.7,26,56–58 For example, Hirten et al. 59 showed that wearables can provide important information for patients and can be a suitable approach to routine management of diseases. Our study confirms that people who already use wearables are more open to innovative wearables like implants for monitoring their health.33,34,50 Our findings regarding the association between physical activity and wearable use are consistent with the findings of the study by Chandrasekaran et al. 51 who reported that people who consider themselves healthier and lead a more active lifestyle are more likely to use a wearable.
Limitations
There are a few limitations in our study that could affect the interpretation of the results. One limitation is the sampling method. As part of the data collection at a fair, it is plausible that this venue attracted individuals with a pre-existing interest in or knowledge of wearable technologies. This selection bias could lead to overestimating the acceptance and usage rates of wearables. Self-report in data collection raises the possibility of recall bias, in which participants do not accurately remember their usage behaviour or preferences, and social desirability bias, which causes them to give responses that they perceive as more favourable or acceptable. In addition, demographic bias, with an average age lower than the national average and a potential over-representation of male participants, could limit the representativeness of the results. 60 The direction of bias created by these limitations is likely to be towards an over-representation of positive attitudes towards wearable technology, and the extent of this bias, although difficult to quantify, could influence important findings.
Interpretation
The Interpretation of these results requires careful consideration of the study objectives and limitations, as well as the context provided by similar studies. The high levels of acceptance and willingness to use wearables for health monitoring found in our study are consistent with global trends in the adoption of digital health technologies.61–63 However, these findings may represent an optimistic view of wearables uptake, given the methodological limitations of the study. Concerns about privacy and data security are consistent with broader challenges in digital health, highlighting the need for robust data protection measures to encourage wider adoption. Comparisons with similar studies underscore the potential of wearable technologies in healthcare and highlight the common hurdles of privacy and demographic representativeness.6,9,25,64–67
Generalizability
To increase the generalizability of the study results on wearables for health monitoring, an extension to the medical context should be considered. Including patients could provide information on how wearables can be used specifically to monitor health conditions and support therapeutic measures. This would enable an understanding of efficient use under the requirements of the healthcare sector (e.g. data protection, reliability). Expanding the study population to include different age groups and socioeconomic backgrounds would also help to develop a more comprehensive understanding of the acceptance and use of wearables beyond the younger, tech-savvy population included in this study.
Conclusion
This study investigated the acceptance and perception of wearables and found that most people have a positive attitude towards wearables. The wearables used were mainly used to monitor physical activity. The high willingness to use wearables for continuous health monitoring and to share health data with healthcare providers offers great potential. However, secure digital solutions are needed to address concerns such as data security. Further research is needed to learn more about the acceptance and benefits of wearables in medicine, e.g., microneedles or implants, which offer great potential for continuous monitoring and improvement of patient care in the context of personalized medicine.
Supplemental Material
Supplemental Material - Continuously monitoring the human machine? – A cross-sectional study to assess the acceptance of wearables in Germany
Supplemental Material for Continuously monitoring the human machine? – A cross-sectional study to assess the acceptance of wearables in Germany by Michael Hindelang, Hannah Wecker, Tilo Biedermann, and Alexander Zink in Health Informatics Journal.
Footnotes
Acknowledgements
We would like to thank all participants for their time and effort in sharing their experiences and opinions in the survey.
Authors’ contributions
M.H. conceived and designed the analysis, did the data collection, performed the analysis, and wrote the paper. H.W. supported the data collection and analysis and reviewed the paper. A.Z. conceived and designed the analysis and reviewed the paper. T.B. reviewed the paper.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Authors declare no Competing Financial Interests but the following Competing Non-Financial Interests. AZ - Chairman of the Digital Dermatology Working Group, German Society of Dermatology. Development of wearables funded by the German Federal Ministry for Economic Affairs and Climate Action (BMWK) based on a decision by the German Bundestag. All other Authors have no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Department of Dermatology and Allergy, Technical University of Munich, Germany.
Ethical statement
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.