
Abstract
Wearable healthcare devices offer tremendous promise to effectively track and improve the well-being of older adults. Yet, little is known about the use of wearable devices by older adults. Drawing upon a national survey in US with 1481 older adults, we examine the use of wearable healthcare devices and the key predictors of use viz. sociodemographic factors, health conditions, and technology self-efficacy. We also examine if the predictors are associated with elders’ willingness to share health data from wearable devices with healthcare providers. We find low level of wearable use (17.49%) among US older adults. We find significant positive associations between technology self-efficacy, health conditions, and demographic factors (gender, race, education, and annual household income) and use of wearable devices. Men were less likely (OR = 0.62, 95% CI 0.36–1.04) and Asians were more likely (OR = 2.60, 95% CI 0.89–7.64) to use wearables, as did healthy adults (OR = 1.98, 95% CI 1.37–2.87). Those who electronically communicated with their doctors (OR = 1.86, 95% CI 1.16–2.97), and those who searched online for health information (OR = 1.79, 95% CI 1.03–3.10) were more likely to use wearables. Though 80.15% of wearable users are willing to share health data with providers, those with greater technology self-efficacy and favorable attitudes toward exercise are more willing.
Keywords
Introduction
Recent years have witnessed a rapid increase in the rise of the older population. Currently, one in 10 people worldwide are aged 60 years and over, and by 2050, it is estimated that one in five people will fall under this category. Though the worldwide population is growing at the rate of 1% annually, people aged over 80 years are growing at 4% per annum. By 2050, people aged over 60 will far outnumber the children aged 14 and under. 1 The rapid rise in senior population has also been noted by OECD, who estimates that by 2060, the proportion of people aged 65 and above will double from 9 to 18%, and those over 80 years will triple to 5.1%. 2 Longer life expectancy, coupled with a decline in fertility rate, has led to this gradual demographic transition where the growth of the older population is higher than that of younger people.3–5
Many older adults prefer to live independently as long as they can, 6 however, many factors can challenge their independence: chronic diseases, diminished social network, physical and cognitive impairment, and low levels of physical activity.7–10 A variety of digital technologies have been proposed to address these challenges and much effort has been invested in developing newer tools and solutions to support aging populations.
Digital technologies, such as the smart wearable healthcare devices, are increasingly being used to support health monitoring, well-being, and independence of the seniors. Use of affordable, wearable technologies has paved the way for new solutions to effectively assist, monitor, and track the health of seniors. Wearable healthcare devices range from activity and fitness trackers like Fitbit, AppleWatch, and Galaxy Fit that gather data on physiological parameters like sleep duration, heart rate, number of steps walked, and calories burnt to more sophisticated devices that can collect advanced clinical data like blood pressure, glucose, and oxygen levels. Healthcare wearable devices are autonomous, noninvasive, wearable equipment with sensors embedded to collect varied physiological health information. 11 Health data collected through smart wearables can be stored and shared with mobile applications on smartphones in real-time, which can be transmitted to computer-based applications for timely interventions. Though many commercially available healthcare wearable devices have been found to provide near accurate measurement of physiological parameters, some studies have pointed out to mixed results regarding the validity and accuracy of health data captured by wearables.12,13
Wearable healthcare devices provide several advantages to seniors. First, these devices can facilitate continuous remote-monitoring of older patients, inform caregivers/physicians about abnormal changes, and help in the early detection and management of a health condition.14,15 Second, wearables can track physical activities, provide alerts, and can also help in fall prevention. 16 Third, wearables can help in self-management of health by providing reminders, increasing physical activity, and aid older adults to make appropriate changes to their daily routines or behavior.17,18 Fourth, regular monitoring of clinical parameters by wearable devices can facilitate home-based telecare for older adults, thereby reducing provider visits and associated costs.19–21
Although, the advantages of wearable healthcare devices are numerous, yet they are not widely adopted or used by older adults. 22 Seniors have had problems in learning and using digital technologies due to technology anxiety and resistance to change.23,24 Therefore, acceptance of digital technologies may be much more difficult for older adults who did not grow up with these types of technologies. In addition, the design of wearable devices has been more geared toward the general population, making it harder for seniors to use them. 25 The complexity and difficulty in customizing the devices tend to inhibit seniors from using wearable devices. 26 Multiple studies have documented ease of use to be a key determinant for older adults’ intention to use technical devices or services.27–29 Furthermore, the ability of the wearable devices to track, store, and transmit patients’ health information raises concerns about data security and privacy,30–32 inhibiting their use by the older population.
Research objectives
The potential benefits of wearable healthcare devices have not been realized due to their poor adoption and use by the older adult community. A rigorous examination of key predictors of the use of wearable devices can greatly help healthcare providers, care givers, administrators, health policy leaders, and device manufacturers to promote diffusion of wearables among seniors and improve healthcare delivery and outcomes. Extant literature on wearable use by older adults have been qualitative,26,33 and the limited empirical studies have largely focused on behavioral intention to adopt and use wearables, rather than exploring the actual use.23,29,34 Though these studies have been useful in enhancing our understanding of wearable healthcare device acceptance by older adults, more research is needed on the actual use of wearables and the key factors affecting the use. Also, we have very limited knowledge about the willingness of older adults to share the health data from wearables with healthcare providers. Unless wearable health data is effectively collected and shared with the providers, timely interventions to help the older population will not be possible.
In line with these research gaps, this study used data from a national survey in the USA to derive insights into the actual use of wearable devices by older adults and the key predictors of wearables use. We also examine how these predictors affect older adults’ willingness to exchange the data from wearable devices with healthcare providers. Health data captured by wearable devices need to be shared with physicians or caregivers for monitoring and timely health interventions. Hence, the willingness of seniors to share the health data becomes a critical variable to realize the potential benefits of wearable devices. Building on prior studies on the topic of wearables that have examined older as well as the younger population,19,23,34–36 we examine a set of predictors related to the health conditions of older adults, personal demographics, technology self-efficacy, attitudes toward fitness and exercise, and their associations with use of wearable healthcare devices. Figure 1 depicts our research model. Research model.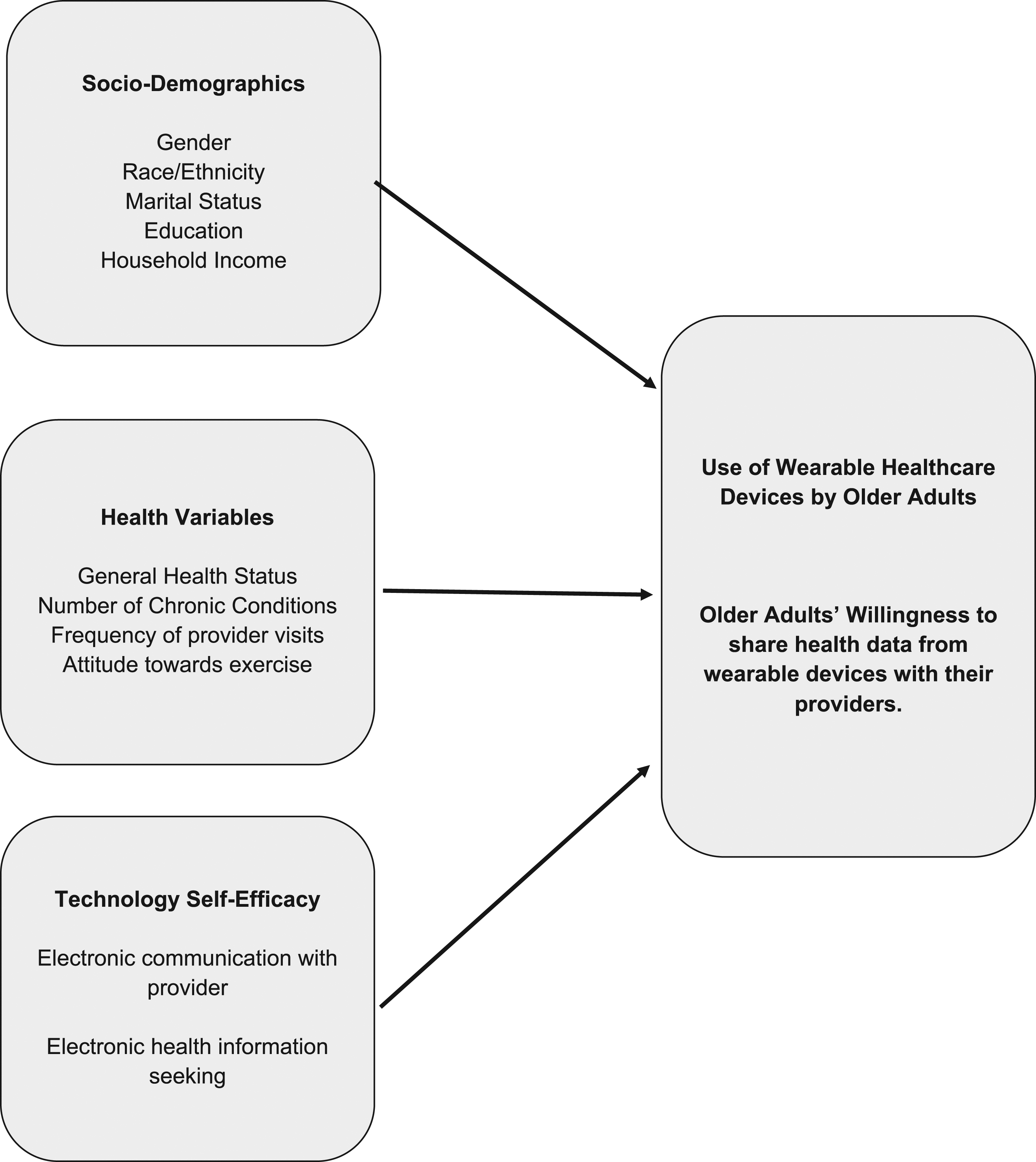
Materials and methods
Data collection
The data for this study comes from the National Cancer Institute’s Health Information National Trends Survey–5, Cycle 3, collected from January to April 2019 through self-administered mailed-questionnaires and a web-pilot. The Health Information National Trends Survey (HINTS) is a nationally representative survey that includes U.S. adults 18 years of age or older, in civilian, noninstitutionalized settings. This survey collects data on US adults’ need, access, and use of information related to health and healthcare, and related behaviors, perceptions, and knowledge. It uses a stratified sampling method defined by (i) areas with high concentrations of minorities, and (ii) areas with low concentrations of minorities. Survey invitees for both mailed-questionnaire and the web-pilot involved an initial mailing of the questionnaire, followed by a reminder postcard, and up to two additional mailings of the questionnaire as needed for non-respondents. More details on the survey and its methodology can be found on HINTS website. 37 HINTS has been a useful resource for several scholars enabling them to assess several topics pertaining to eHealth and health behaviors. 38
Since HINTS uses probability sampling to improve representation of specific groups, our statistical analysis applied weights to calculate US population estimates and standard errors. Weight adjustment accounted for nonresponse and known population totals based on 2017 American Community Survey (ACS) of the U.S. Census Bureau on age, gender, education, marital status, race, ethnicity, and census region. We used the jackknife approach to compute replication weights. Our approach is consistent with other studies that have used HINTS data with weight-adjustments to compute population-level estimates and analysis.39–41
For data analysis, we included all older adults aged 65 or above who answered the question about their use of an electronic healthcare device to track or monitor their health or physical activity in the past 12 months. This resulted in a final dataset of 1481 respondents. STATA 16.1 software was used for performing the statistical analyses.
Variables
There are two primary variables of interest: (i) Use or non-use of a healthcare wearable device, and (ii) Willingness to share the data from a wearable device with a healthcare provider. Both these variables were captured as a binary variable (yes/no) through questions that asked respondents to indicate their use or non-use of a wearable device (e.g., Fitbit, Apple Watch, or Garmin Vivofit) to monitor or track health or activity in the past 12 months. In a similar vein, users were asked to indicate if they were willing to share health data from their wearable device with a healthcare provider.
Health conditions of older adults were captured using three variables (i) self-reported general health status that was measured using a single item asking seniors to rate their health as“1-poor,” “2-fair,” “3-good, “4-very good fair,” or “5-excellent,” (ii) number of chronic conditions, computed as an additive score based on responses indicating presence or absence of the following chronic conditions: diabetes or high blood sugar; high blood pressure or hypertension; a heart condition (such as heart attack, angina, or congestive heart failure); Chronic lung disease (asthma, emphysema, or chronic bronchitis). The values for this variable ranged from 0 to 4. (iii) Frequency of visits to a healthcare provider in the past 12 months: “not at all,” “1–2 times,” “3 or more times.”
Technological self-efficacy was assessed using two questions that pertained to older adults’ use of technology for health-related purposes. These questions asked if the participants used a computer, smartphone or other electronic means to (i) look for health or medical information for themselves (yes/no), and (ii) used e-mail or the internet to communicate with a doctor or doctor’s office (yes/no). Attitude toward exercise was assessed using a likert-scale measure that asked how much the respondent enjoyed exercising: “1-not at all, 2-a little, 3-some, 4-a lot.”
Demographics
The sociodemographic variables that we included were gender, education level, race/ethnicity, marital status, and annual household income.
Data analysis
Researchers use sample survey methodology to obtain information about a larger population by selecting and measuring data from a smaller sample that is drawn from the larger population. Statistical procedures use data from this observed sample to arrive at conclusions about a population. Because of huge variability in population characteristics, scientific sampling design techniques are applied when selecting the sample in order to get a realistic representation of the population. In order to make statistically valid inferences about the population, the statistical analyses must account for the sample design process. Unlike studies that rely on data from random sampling, the statistical techniques are not valid if the data comes from other sample designs, such as complex survey designs with stratification, clustering, and/or unequal weighting. In these cases, specialized techniques must be applied in order to produce the appropriate estimates and standard errors. 42 We used statistical tests that were appropriate for the probabilistic sampling that was done to elicit responses for the HINTS survey. In order to account for the HINTS probabilistic sampling design and calculate nationally representative estimates, we applied STATA survey procedures incorporating the jackknife variance estimation technique and HINTS-supplied survey weights. 43 The survey design was declared, weights applied before performing our analyses. In accordance with our research goals, logistic regressions were used to examine the associations between the predictors of interest, and the two primary variables viz. wearables use, and willingness to share wearable data with a healthcare provider.
Results
Weighted US respondent characteristics.
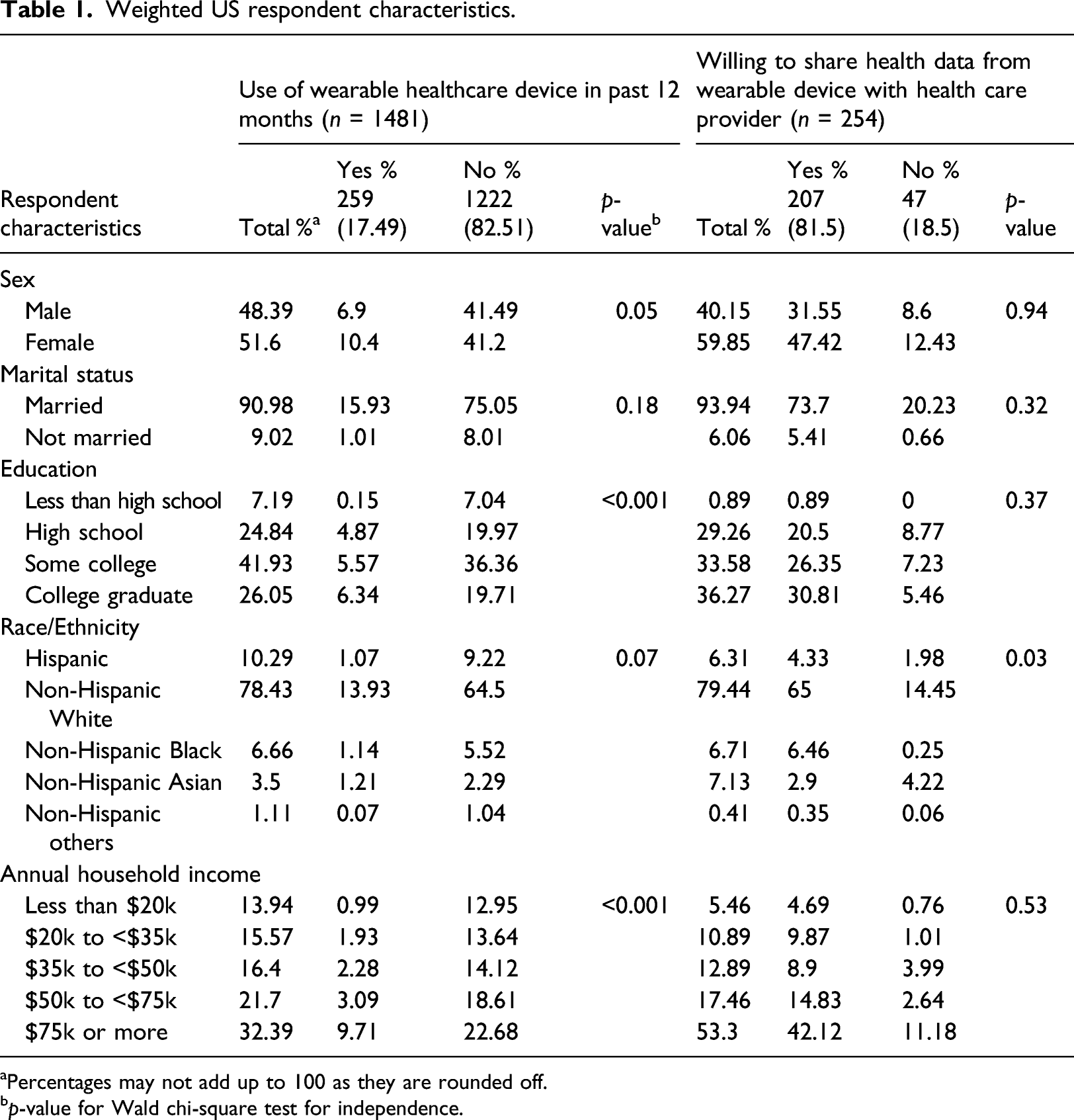
aPercentages may not add up to 100 as they are rounded off.
bp-value for Wald chi-square test for independence.
Significant differences were observed between users and non-users of healthcare wearable devices across gender, education, and household income. Seniors who were women (10.4%), white (13.93%), those with some level of college education or college graduates (11.91%), and annual household incomes above $75K (9.71%) were most likely to report using wearable healthcare devices. There were no significant differences based on marital status.
Among the seniors using wearables, a majority (207, 81.5%) indicated their willingness to share health data from wearables with healthcare providers. The willingness did not vary on any of the demographic factors, except race/ethnicity.
Predictors of wearables use
Logistic Regression Results—Key Predictors of Wearable Use by Older Adults and Willingness to share wearable data with healthcare provider.
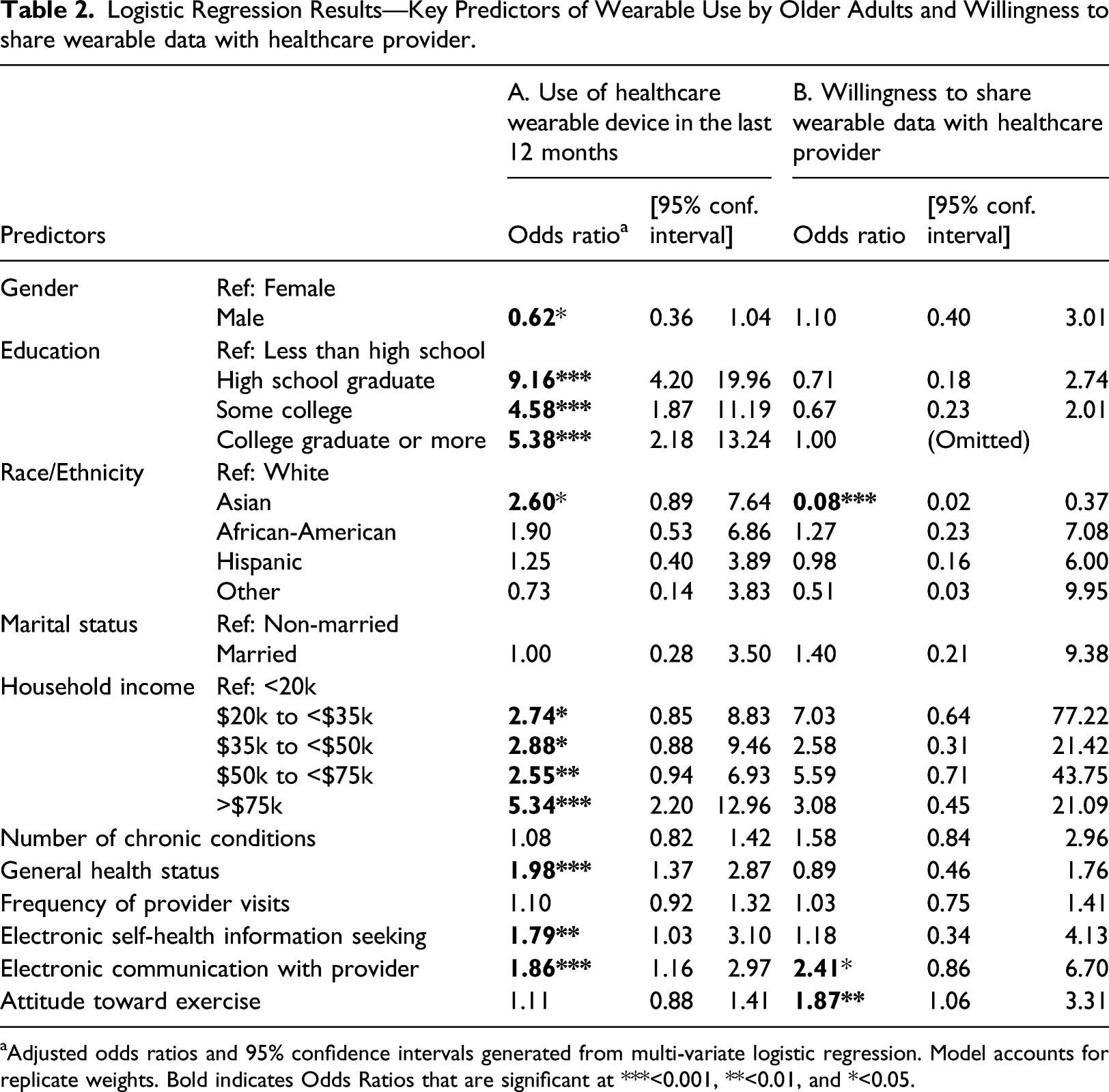
aAdjusted odds ratios and 95% confidence intervals generated from multi-variate logistic regression. Model accounts for replicate weights. Bold indicates Odds Ratios that are significant at ***<0.001, **<0.01, and *<0.05.
Wearable device use
Of the demographic variables, gender, education, race, and annual household income exhibited significant associations with seniors’ use of wearable healthcare devices. Our results indicate that older men are less likely to use wearable healthcare devices, as compared to older women (OR = 0.62, 95% CI 0.36–1.04). Compared to seniors whose educational qualifications were less than high school, others with better education were five to nine times more likely to use wearables. Asian seniors were twice more likely to use wearables as compared to whites (OR = 2.60, 95% CI 0.89–7.64). We also found a strong positive association between annual household income and the use of wearable devices. The likelihood of wearable use steadily increased for seniors as their annual household income levels increased.
Only one out of the three health-care–related variables exhibited a significant association with wearable use. We found that healthy seniors are almost twice more likely to use wearables as compared to those with self-reported poor health (OR = 1.98, 95% CI 1.37–2.87). The number of chronic conditions and the frequency of visits to the healthcare provider did not emerge as significant predictors.
Technology self-efficacy turned out a significant predictor of wearable use with both variables exhibiting significant positive associations. Seniors who electronically communicated with their doctors (OR = 1.86, 95% CI 1.16–2.97), those who looked up online for health information (OR = 1.79, 95% CI 1.03–3.10) were more likely to use wearables. Seniors’ attitude toward exercise did not emerge as a significant predictor of wearable use.
Willingness to share health data from wearables with providers
Though we found many seniors, in general, to be willing to share their health data (Table 1), the logistic regressions revealed three factors that affect their willingness. As shown in Table 2 (Panel B), three variables—race, attitude toward exercise and technology self-efficacy exhibited significant associations with seniors’ willingness to share health data from wearables with providers. Compared to Whites, Asian seniors were less likely to share health data (OR = 0.08; 95% CI 0.02–0.37). Though our findings show that Asian older adults have a higher likelihood to use wearables as compared to Whites, we also find that they are less willing to share their health data. We also found older adults with a favorable attitude toward exercise (OR = 1.87, 95% CI 1.06–3.31) and those who had greater technology self-efficacy as exhibited by their electronic communication with a doctor (OR = 2.41, 95% CI 0.86–6.70) were more willing to exchange their health data with healthcare providers.
Discussion
Wearable healthcare devices offer tremendous opportunities to ensure the well-being of the older adult community. With technological advances in the internet of things (IoT) and health data analytics, wearables provide a cost-effective mechanism to significantly improve the quality of life for older adults and improve their health. Yet, we know very little about the use of wearables by seniors and factors associated with wearable use. This study advances the current knowledge on the use of wearable devices by examining factors that are associated with older individuals’ use of wearable healthcare devices. Unlike prior studies that examined intention to use, this study focused on the actual use of wearables by older adults. We used data collected by HINTS to gain insights into how US seniors use wearables and their predicting factors.
A primary finding from this study is that only a limited set of older adults are currently using wearable healthcare devices. Many studies have reported slower and low levels of technology adoption and use by older adults, which is primarily fueled by lack of technical skills, negative attitudes or anxiety toward technology, and age-related changes including difficulties with vision, hearing, and fine motor skills.44–47 Though technologies such as wearable devices can greatly improve the quality of life for older adults, 48 it is important to make it easier for them to adopt and use these technological devices.
Results from our analysis show that technology-efficacy variables are positively associated with the older adults’ use of wearable healthcare devices. Older adults’ general use of technology for health-related purposes provides them with familiarity and openness to use wearable healthcare devices. More exposure to and the use of simpler technologies like the internet, email and texting can help the older individuals to develop positive attitudes toward accepting complex devices such as wearable healthcare devices. Our results validate and extend the findings from prior studies on technology acceptance models23,29,49 to the realm of wearable use in the context of older adults.
This study finds strong support for the influence of socio-demographic variables on seniors’ use of wearable healthcare devices. With increasing age, older adults could face challenges with reduced skills and cognitive abilities that could pose a challenge to learning newer tools or technologies. However, our findings point that education and higher income levels can facilitate their adaptation to learn and use newer technologies like wearable healthcare devices. We also noted the race/ethnicity background of seniors to be an influencing factor in their use of wearables. Most older Asians in the US tend to be immigrants with typically higher education, jobs and higher income levels, 50 and this could help them in accepting and using wearable healthcare devices. Our findings about senior women’s use of wearables to be more than that of older men are consistent with findings in the context of other technologies such as e-health 51 and social media. 52 Our results about the important influence of demographic factors resonate with other studies that have reported their importance in the context of adoption of technologies such as the internet,53,54 smart phones, 55 and mHealth. 24
An encouraging result from our analysis is that most older adults who use wearable healthcare devices are willing to share the health data with healthcare providers. And, this willingness was seen more among those older individuals who had a favorable attitude toward fitness and exercising, and those who were more tech-savvy. When viewed holistically, our results imply that the bigger challenge is to make the seniors use wearable healthcare devices, rather than having them share the health data with providers. Once older adults adopt and start actively using wearables, it might be easier for them to realize the value from using the wearables, paving the way for sharing the data for real-time health interventions.
Contributions and limitations
This study offers interesting insights to the literature and adds to the ongoing dialogue about the older adults’ use of wearable health devices. First, in comparison to existing qualitative and behavioral intention studies, the study draws on data resulting from a large population of probabilistic sampling of older adults in the USA. Second, we examined both individual-level sociodemographic predictors and those pertaining to technology and health conditions. Third, we also draw some insights on older adults’ willingness to share the health data from wearables with providers.
Our study makes contributions to both research and practice. We contribute to the literature on wearable technology use by throwing light on how older adults use these devices, and their willingness to share the health data from the device with healthcare providers. Our main finding is that the penetration of wearable devices and their use among older adults is still low. However, we document the important predictors pertaining to sociodemographic characteristics, health conditions, and technology self-efficacy that can improve wearable use among older individuals. Our findings are also useful for health policy makers, healthcare professionals, providers, and wearable manufacturers. Insights from our study can help leaders target-specific older groups to promote and accelerate wearable use.
This research also has several limitations that must be kept in mind while interpreting the results. Our study relied on data from a national survey across the US that was done by the National Cancer Institute. We used a subset of data from a larger study to gather insights on wearable use as the original HINTS survey was not specifically designed to do a detailed assessment of wearable devices. Hence, we were constrained by the use of secondary data and had to use measures that were incorporated into HINTS. An advantage of our approach was cost-effective access to a fairly large sample that was representative of the US population. On the other hand, this imposed limitations pertaining to use of single-item measures for some of our variables and inflexibility to design our own measures. The study also has certain limitations related to self-reported data that could be based on subjective interpretation of respondents.
Implications and conclusion
Healthcare wearables that continually collect elders’ health data in real-time can facilitate better diagnosis by providers who can prescribe appropriate treatments of care. Remote patient monitoring through wearables has assumed greater importance in light of COVID-19 pandemic that has restricted the movement of elders due to potential risks of exposure. Our findings indicate low usage of wearable healthcare devices by elderly adults in the US, and more work needs to be done by policy makers and healthcare professionals to enhance the adoption and use of these devices. In 2018, Centers for Medicare and Medicaid Services (CMS) approved providers to receive separate reimbursements for time spent in gathering and utilizing remote patient health data. This policy shift was a major step to encourage clinicians to leverage tools such as smart healthcare wearable devices and use patient-generated health data for care coordination and management. However, these efforts need to be matched by increased use of wearable devices by elderly so that the health outcomes can be vastly improved. Policy interventions that incentivize and promote the diffusion and use of wearable devices by the senior population could help offset the potential barriers in using these devices. For instance, a specific strategy to promote at-home telehealth services for elders with active use of healthcare wearables can help replace office visits and can enhance healthcare delivery, simultaneously reducing overall costs.
Our findings also point to racial and income disparities that inhibit wearable use by seniors. Policy interventions tailored to low-income seniors or awareness programs aimed at Hispanic, or African-American elderly populations can help improve wearable use by these groups. A coordinated effort by both clinicians and public health policy makers to promote awareness and benefits of wearables among specific groups of seniors can help realize the promised benefits of these devices. Further, wearable device manufacturers can work with smartphone and telecommunication service providers to promote the use of wearable devices among seniors.
At a global level, the COVID-19 pandemic has intensified long-standing challenges facing older adults. 56 Significant disparities exist on how older adults are viewed and supported by their families and communities in different parts of the world. 57 The pandemic has led to an increase in ageism, discrimination and digital divide against older adults in many parts of the world.58–60 However, many older adults have used technology to keep informed and feel connected during the course of the pandemic. 61 Many technological tools, mobile applications, and telehealth opportunities have also been proposed in multiple countries to help older adults deal with impacts of the pandemic.62–64 While the use of wearables among older adults in different nations is not known, the increased use of technological tools by older adults in recent months since the pandemic began, provides an opportunity to introduce wearable devices and activity trackers amongst older adults.
As the world moves toward increased use of wearable health devices, older adults cannot be left behind. Wearables offer an effective mechanism to improve the well-being of the senior population. This study provides preliminary insights into the older adults’ use of wearable devices and the key predictors of wearable use, and their willingness to share health data with providers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.