Abstract
Scheduling and coordinating constrained resources in community healthcare settings at a centralized Pathways Community HUB is challenging due to limited resources and the inherent dynamics of the processes and the organizational structures. In this work, we introduce a stochastic programming (SP) approach for connected community health for optimally scheduling community health pathways (CHPs) under uncertainty in resource availability. A CHP is a standardized tool that details multiple steps of a healthcare-related service and the required resources for each step. The SP methodology was implemented and applied to data for a real Pathways Community HUB for a U.S. county involving several CHPs, community health workers, physicians, and other resources. The computational results are promising and they show that client access times depend on the HUB resources uncertain future availability and the level of client demand, with high client demand resulting in relatively longer access time. The study reveals that schedules provided by a deterministic approach where resource availability is assumed to be known can be too optimistic. Several managerial insights are learned from this study, including the observation that the SP model provides client schedules that are equitable across the same type of community health workers.
Keywords
Introduction
Community healthcare agencies in the U.S. such as those at the county level are tasked with providing medical, behavioral, and social services to community members in need. However, providing such services requires careful coordination of limited resources. Agency resources include case managers, community health workers, and office facilities, while external resources include physicians, nurses, social workers, behavioral health specialists, insurance companies, and community-based organizations. Care coordination is the organization of care activities among individual clients and providers to facilitate the appropriate delivery of healthcare services. 1 Performing care coordination involving disparate resources presents significant challenges in terms of scheduling, adhering to the care activities protocols, and tracking progress of these activities for each client in the system. The focus of this paper is on community care coordination using the Pathways Community HUB model of care coordination. 2 This model considers the community level to improve quality of care for individual clients by coordinating community-based health and social services.
This work introduces a stochastic programming (SP) approach for scheduling and coordinating community health pathways (CHPs) under uncertainty in the availability of the limited Pathways Community HUB resources and client demand, while providing equity among community health workers via workload balancing. There are different types of pathways and in this work we focus on CHPs for connected community health services, which are different from clinical or care pathways. 3 A CHP is simply a structured and time-framed multidisciplinary care guideline that details essential steps of a community healthcare process. 4 It provides a sequence of appointments and resources needed for each appointment together with its duration over a specified time horizon. Community health pathways are unique in that they track the individual client being served and each step of the CHP addresses a well defined action towards resolving the issue addressed by the pathway. Such issues include lack of health insurance, medical home, homelessness, pregnancy, immunizations, and so on. Each step can deal with a health, social or cultural issue. A CHP is not considered completed until either the issue is successfully resolved or a specific point is reached to close the CHP that it has not been completed. In addition, payments for a CHP are made at specific points along the pathway, with the largest payment offered at the successful completion of the pathway. 2
The Pathways Community HUB model of care coordination is a construct that was introduced to enable coordination of care activities of different organizations and their services. Pathway models focus on the progress and outcomes of individual clients as they traverse the care organizations.5,6 In turn, pathways coordination can enable a comprehensive approach to community health service focused on reducing the healthcare inequalities to improve health outcomes for the community. 7 Community-based services have been shown to play a vital role in addressing some of the nation’s most difficult health problems, including health disparities and the rising chronic health conditions such as obesity and diabetes. 8 Effective care coordination at the community level is a hard task. Many individuals who need community health services have complex health needs and chronic health conditions. 9 Addressing these needs requires a combination of multiple services (medical services, behavioral health services, and social services) and support from a wide variety of community-based resources to reduce the health and social barriers to improve healthcare outcomes. 10 This complexity poses major challenges in terms of effectively connecting different parties (clients, agencies, service providers) and coordinating them to work in concert to achieve positive outcomes.
The limited number of resources needed to provide community health services calls for optimization methods to aid in scheduling to best utilize the limited resources while providing quick access time for all clients. This scheduling challenge is compounded by the new paradigm of value-based purchasing, 11 which has drastically changed how services are measured, reported, and rewarded in healthcare delivery. The new paradigm of healthcare delivery asks for new designs and innovative methods to support community health service coordination and optimization. This work makes a step toward achieving that goal. However, scheduling CHPs is extremely challenging and literature on solution methods for this problem is scant. The few available works are in the hospital setting: constraint programming model 12 and combined genetic algorithm with particle swarm optimization for scheduling clinical pathways in a hospital setting. 13 Clinical pathways can significantly improve patient access time in a hospital setting. 13 Furthermore, studies have shown that clinical pathways lead to positive outcomes for various cases, including a reduction in the prescription of laboratory tests 14 and in-hospital complications. 15
A variety of models have been proposed to minimize client waiting time while scheduling resources, but literature on pathways scheduling is limited. Mixed-integer programming models to minimize wait time for patients have been proposed.16,17 The objective is to minimize the weighted sum of the total wait times of patients 16 or to find a reasonable schedule within a desired time window. 17 Such works assume perfect information and ignore the uncertainty in the parameters. A few works take demand uncertainty into consideration while minimizing the patient waiting time. 18 In related work, a two-stage SP model is proposed to minimize expected total cost. 19 However, in our work we consider uncertainty in resource availability while minimizing the workload imbalance and client waiting time. To eliminate the imbalanced workload distribution among resources, a satisfaction indicator over 1 month period to inform decisions of resource future assignments was introduced. 20 In our model, workload balancing is done after each CHPs assignment, instead of accumulating the workload over a month.
The main contributions of this paper include the following: (a) an SP model for optimally scheduling individual CHPs under unknown future resource availability while allowing for workload balancing of resources of the same type to enable equity among personnel; (b) a computer simulation model that uses the SP model to assess CHPs scheduling and workload balancing in a structured setting; and (c) a computational study based on a real setting to demonstrate the new approach and gain managerial insights into CHPs scheduling under uncertainty. The rest of this paper is organized as follows: next we present a detailed SP scheduling model in the CHPS Scheduling Model section. Data collection and analysis, model development and implementation, and experiment design are discussed in the Materials and Methods section. We report and discuss our simulation results in the Results and Discussion section. Finally, we provide concluding remarks and point out future work in the Conclusion section.
CHPs scheduling model
A CHP involves several steps with each step requiring one or more resources, and the required resource(s) for each step have to be scheduled for a specific day and time in the future. Thus, scheduling a CHP requires scheduling multiple care activities that have to be processed at some point between an earliest start time and a latest completion time, all while satisfying the required resources’ availability constraints. We derive a two-stage SP model to optimally schedule CHPs under unknown future resources’ availability. The objective is to minimize client access time, i.e., the time from when a pathway appointment request is made to when the client is first seen, while providing equitable workload among the human resources.
In the first-stage, we determine here-and-now the client’s schedule for all the steps in the CHP, i.e., we assign a day, time slots and required resources for each step of the CHP, before availability of the resources is unveiled. Then in the second-stage we account for possible future resource availability for each day and step of the CHP to inform the first-stage in finding an optimal schedule. In SP, unknown future availability of the resources is characterized by probability distributions. Specifically, we consider a probability distributions for the future availability of each resource for each day and each time slot, respectively.
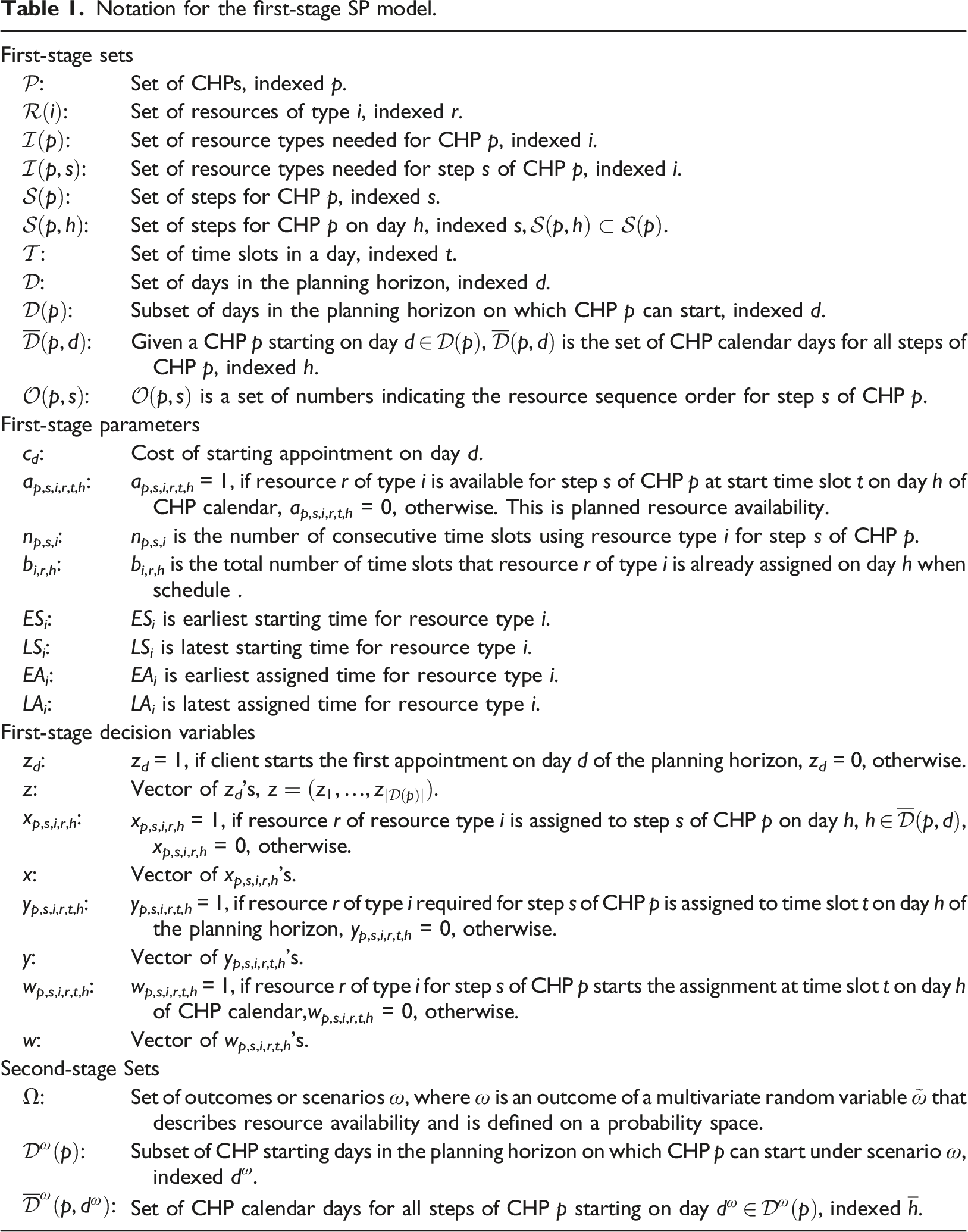
Notation for the first-stage SP model.
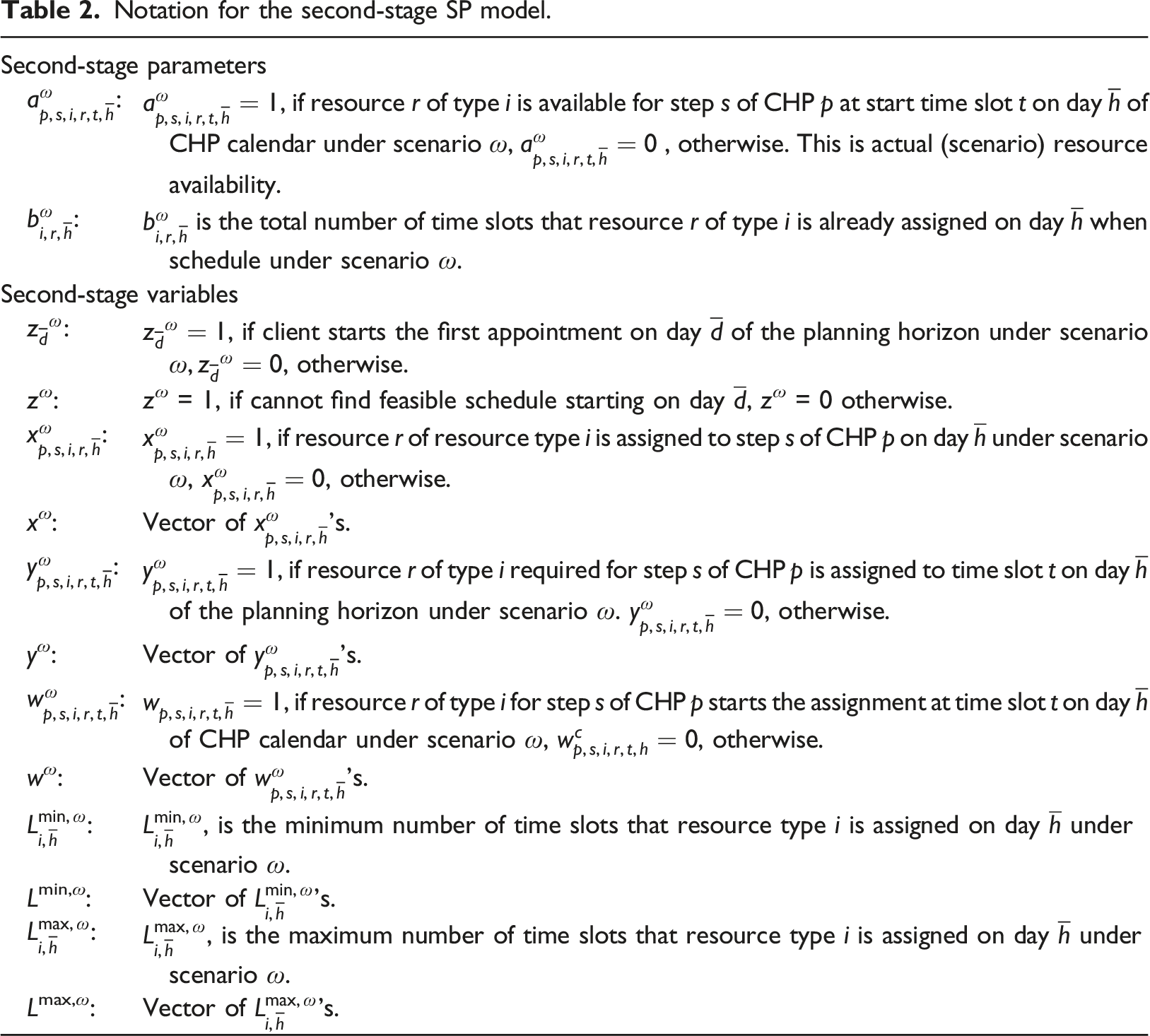
Notation for the second-stage SP model.
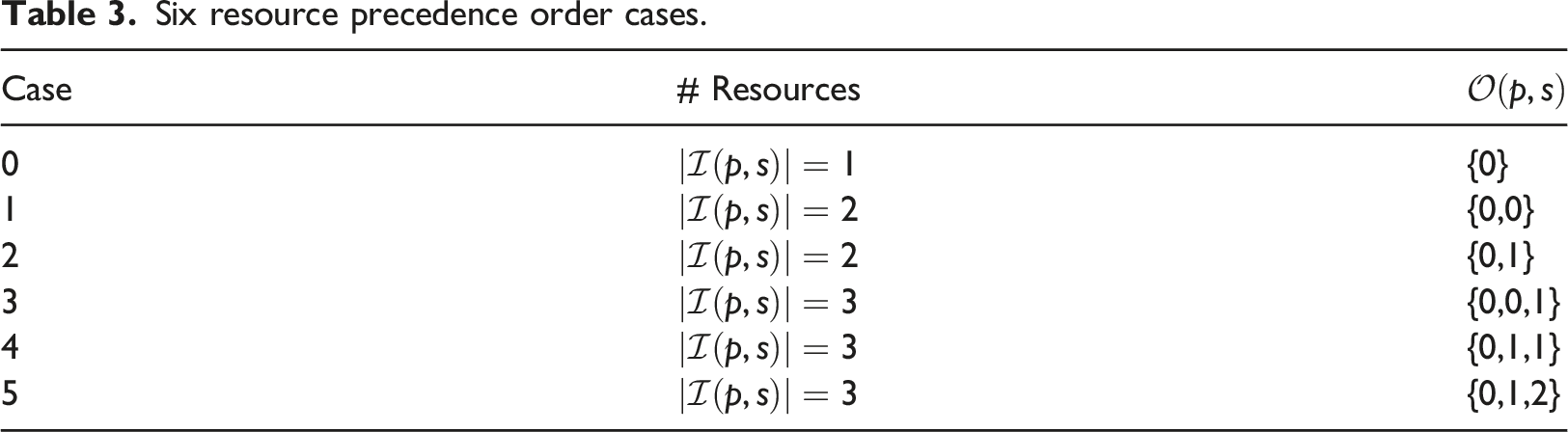
A CHP typically involves multiple types of resources in a given step. For a CHP p, if
Six resource precedence order cases.
We are now ready to derive the SP formulation. For a given client, the first-stage decision variable vector v specifies each resource’s schedule, i.e., days and corresponding time slots the resource is assigned to each step of the CHP, as well as the start time slot on each day in the schedule. The first-stage objective is to minimize client access time while taking into account the resources’ unknown availability in the future. Thus, given the first-stage decision v, the second-stage objective is to minimize expected future cost associated with workload balancing based on the resources’ uncertain availability. Mathematically, the objective is written as follows:
Given the subset of days in the planning horizon on which CHP p can start, 














Putting everything together, the SP model can be written as follows:
Constraints (8)–(12) needed for the CHP

Subproblem (14) minimizes the total difference between the maximum and minimum workload among resources of the same type to enable workload balancing. We add a sufficiently large penalty M to the second term of the objective function to enforce relatively complete recourse by allowing z
ω
to take a value of one when we cannot find a feasible schedule starting on day 








We implemented SP model (13)–(14) in the Callable CPLEX Library
21
and solved instances of the model in the simulation HUB setting study described in the previous section. With 15-min time slots in an 8-h day, the maximum difference
Materials and methods
Motivated by a real Pathways Community HUB, we developed a computer simulation model to mimic client appointment requests arrivals for CHPs, scheduling CHPs, and the arrival of clients at the Pathways Community HUB for their appointment. The goal of the simulation model was to help us gain managerial insights into the computational performance of the SP approach under different demand cases and resource availability scenarios. The SP model was implemented within the simulation framework to determine the schedule for each client request. Next, we describe our data collection and analysis, including the real setting and design of experiments. We devote most of the space to deriving the SP pathway scheduling model.
Data collection and analysis
We consider a Pathways Community HUB setting for a county located in the eastern U.S. that offers health and social services with the aim of providing preventative care and improving health outcomes for high-risk members of the population. Care coordination in this HUB includes multiple providers and several services as depicted in Figure 1. CHPs in this HUB do not only involve clinical services, but also include social services to help overcome social barriers to healthcare access for risk population.
2
Pathways community HUB model.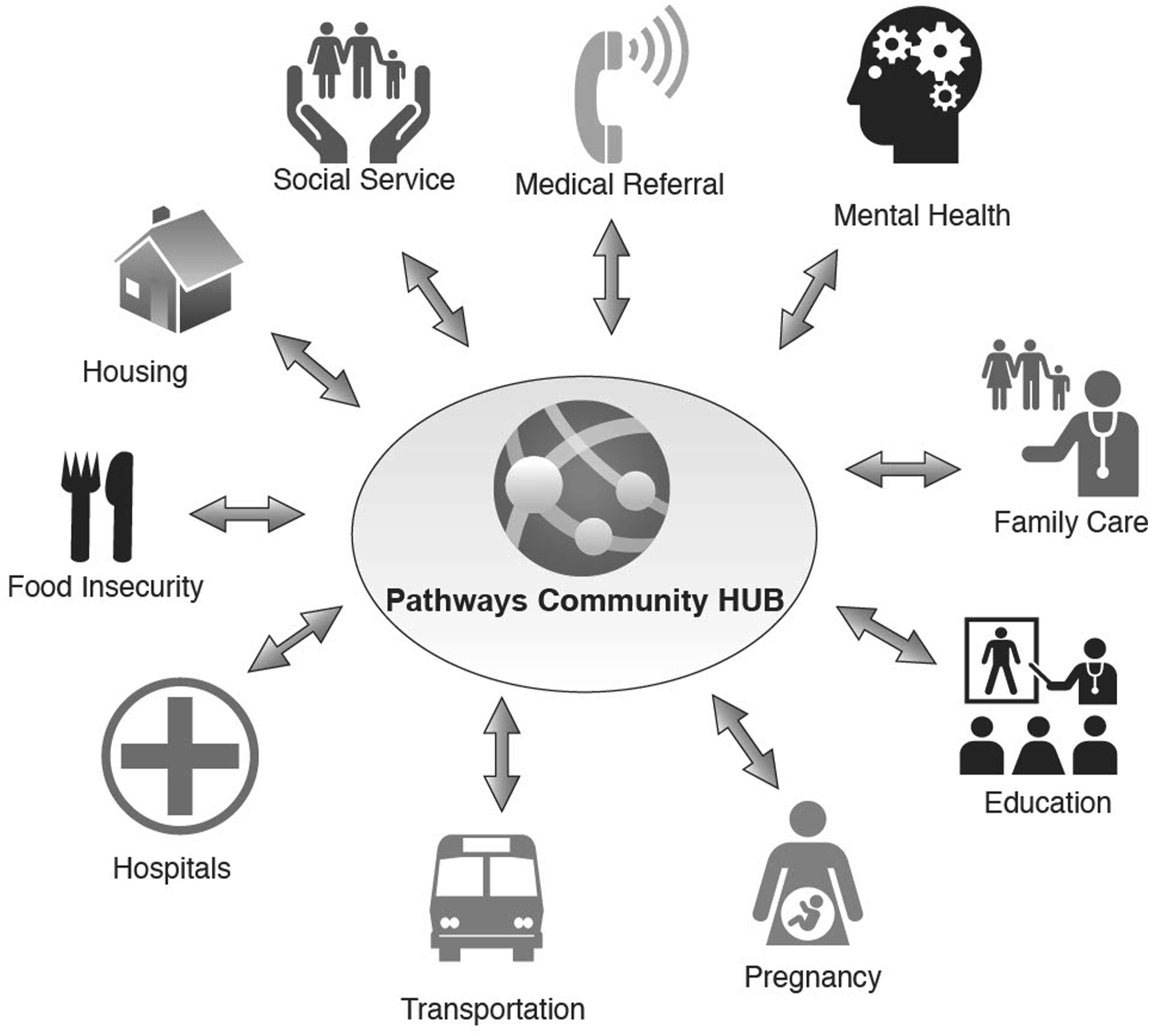
The Pathways Community HUB deals with about 40,000 residents with over 90% of the population belonging to a racial or ethic minority group. The HUB operates 9 h a day from 8:00 a.m. to 5:00 p.m., Monday through Friday, with 1 h lunch break from 12:00 p.m. to 1:00 p.m. The hours of operation are divided into 15-min time slots, and the CHP steps are assigned to time slots. Thus, there are 32 working time slots each day with four lunch break time slots.
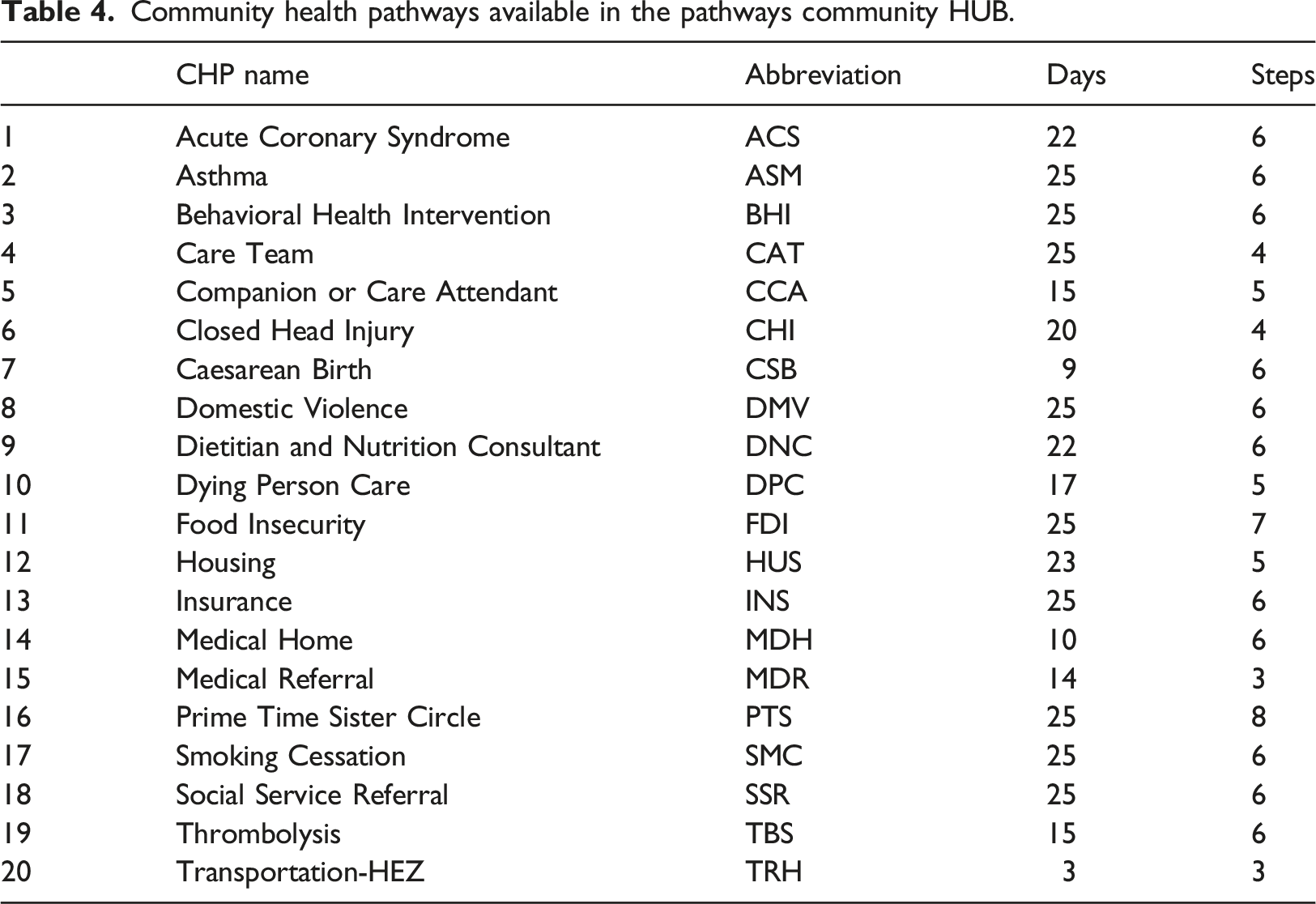
Community health pathways available in the pathways community HUB.
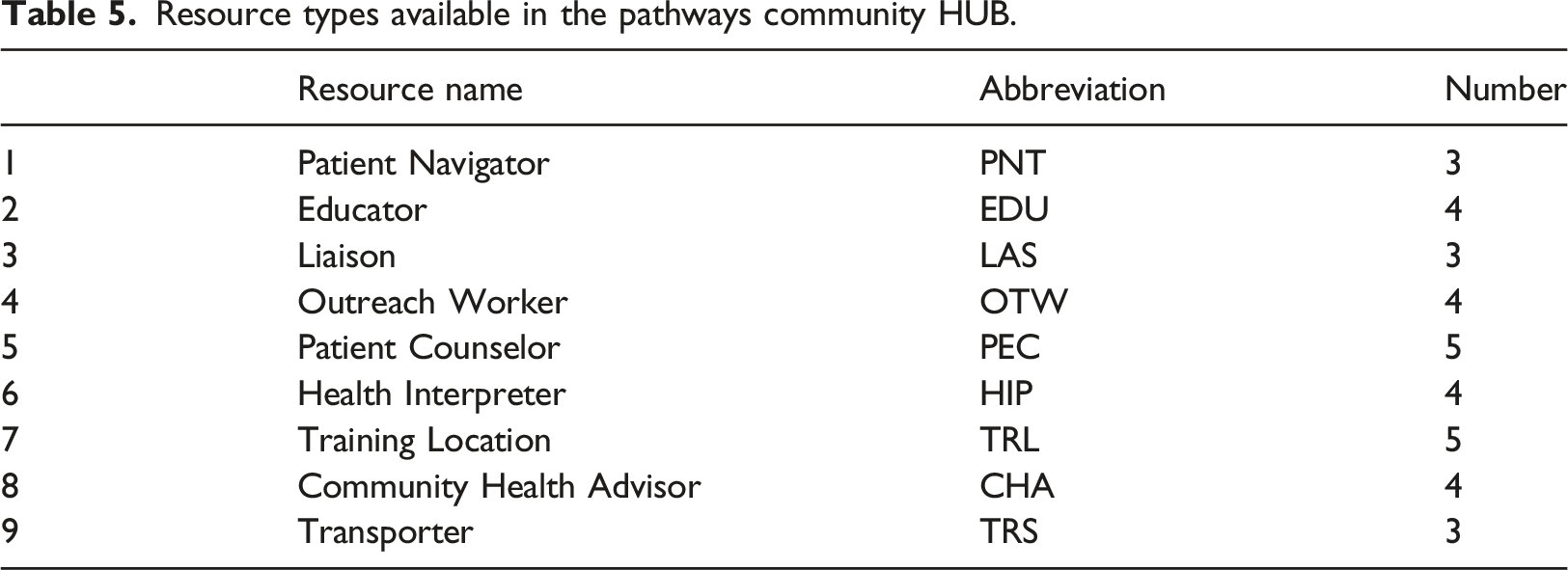
Resource types available in the pathways community HUB.
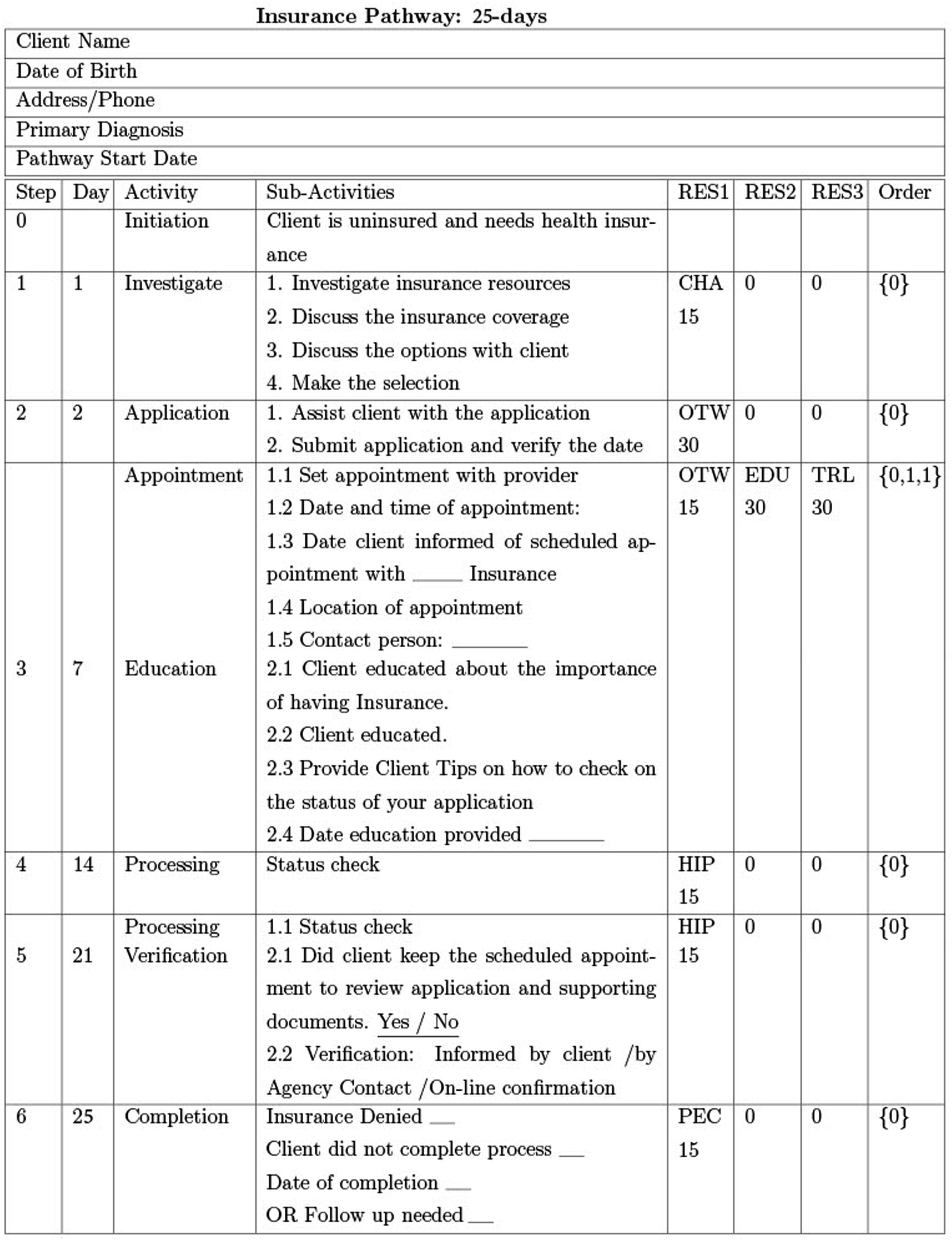
The Insurance CHP in Figure 3 in the Appendix takes 25 days to complete and involves six steps after initiation: step 1 (Investigate) on day 1 requires one resource, CHA, for one 15-min time slot; step 2 (Application) on day 2 requires one resource, OTW, for two 15-min time slots; step 3 (Appointment, Education) on day 7 requires three resources, OTW for one 15-min time slot and EDU and TRL for two 15-min time slots concurrently and; step 4 (Processing) on day 14 requires one resource, HIP, for one 15-min time slot and; step 5 (Processing Verification) on day 21 requires one resource, HIP; and step 6 (Completion) on day 25 requires one resource, PEC.
Model development and implementation
Managing clients and resources in the Pathways Community HUB in extremely challenging, as it relates to scheduling clients for different pathways using limited resources whose future availability is uncertain. We developed an SP pathway scheduling model together with a simulation model of the HUB to evaluate the performance of the SP approach. The computer simulation and SP models were coded in the CPLEX 12.9 Callable Library 21 using C++ and experiments were performed on a Dell T7600 Workstation with a Intel(R) Xeon(R) CPU E5-2643 0 @3.30 GHz MHz processor and 64.0 GB RAM.
A CHP scheduling flowchart of the computer simulation model is shown in Figure 2. The simulation model has several entities including a Client Generator, CHP Scheduler, and Resource Allocator. The responsibility of the Client Generator is to create client arrivals on each day d of the planning horizon. Clients arrive one at a time and are given an ID (index) c
d
and assigned a CHP by the CHW based on their needs. Next, the CHP Scheduler invokes the SP model (13)–(14) to search for an appointment for the client within 10 days with minimum access time and workload imbalance (if workload balancing is selected). The Resource Allocator in turn updates the future availability of the resources assigned to the CHP steps, i.e., makes them unavailable at the scheduled time slots for that CHP. After the client is scheduled, the Client Generator generates the next client and the scheduling process is repeated. Otherwise, if the client cannot be scheduled within 10 days, the simulation records them as not scheduled. The simulation ends when the last appointment day is reached. CHP scheduling simulation flowchart.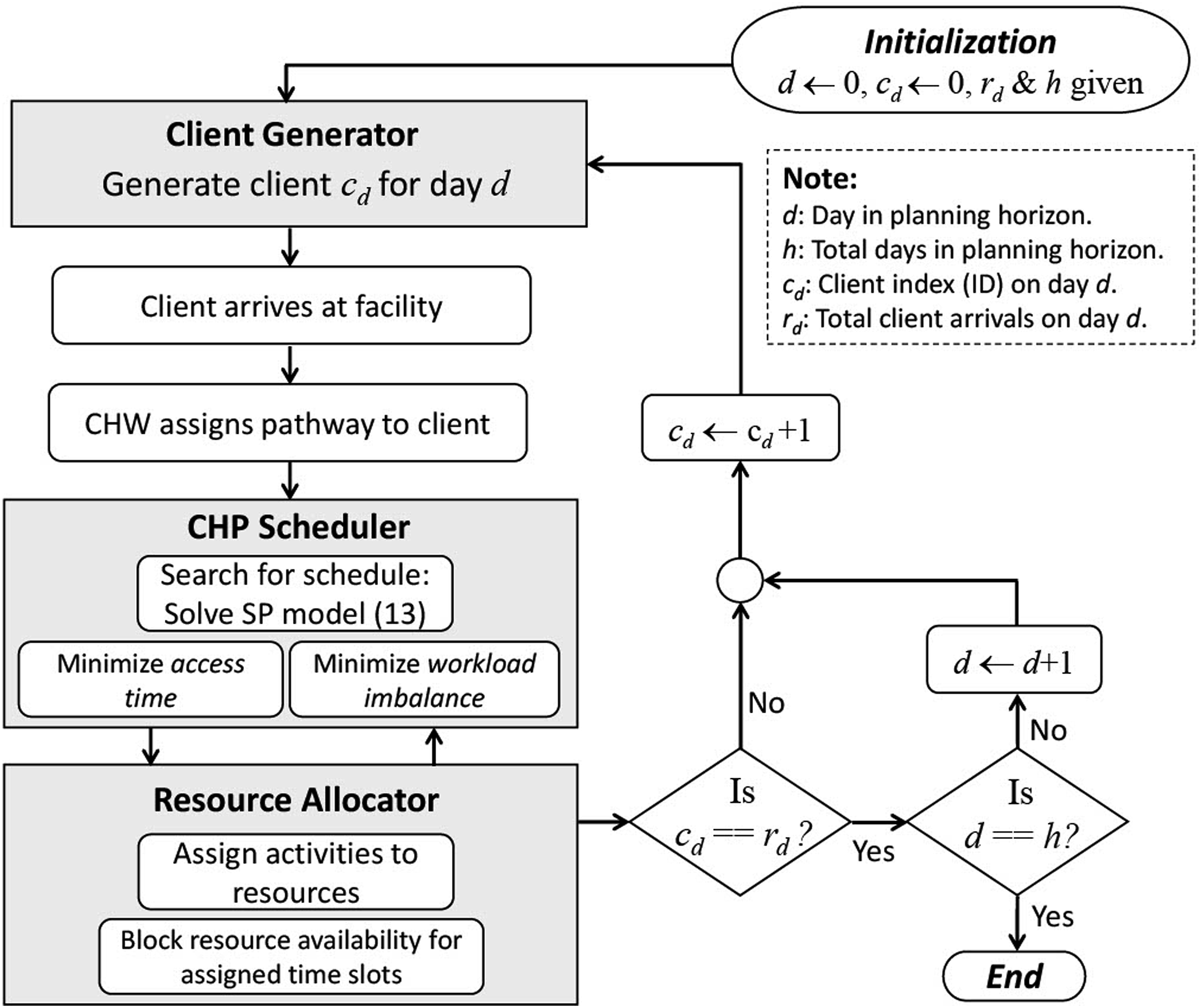
Experimental design
Several experiments were conducted to assess the schedules determined by the SP model over a specified time horizon with an overall goal of gaining managerial insights. Specifically, we studied the following four main aspects of CHPs scheduling under uncertainty: (i) variation of client access time; (ii) impact of client demand on scheduling; (iii) resource utilization; and (vi) workload balancing versus no workload balancing. The motivation behind these four factors stems from the practical needs of Pathways Community HUBs, which include minimizing access time for their clients, efficiently managing different levels of demand, maximizing resource utilization, and ensuring workload equity among the human resources.
We considered the following key performance measures: access time, number of clients scheduled (throughput), resource workload or utilization (number of time slots assigned), and workload coefficient of variation. Client request daily arrival rate is a critical factor in scheduling CHPs. It translates into client demand volume, which significantly affects scheduling decisions in terms of client access time. Therefore, to study the effect of demand level on access time, we experimented with three cases: low demand (Case I), medium demand (Case II) and high demand (Case III).
Experiment cases and settings.
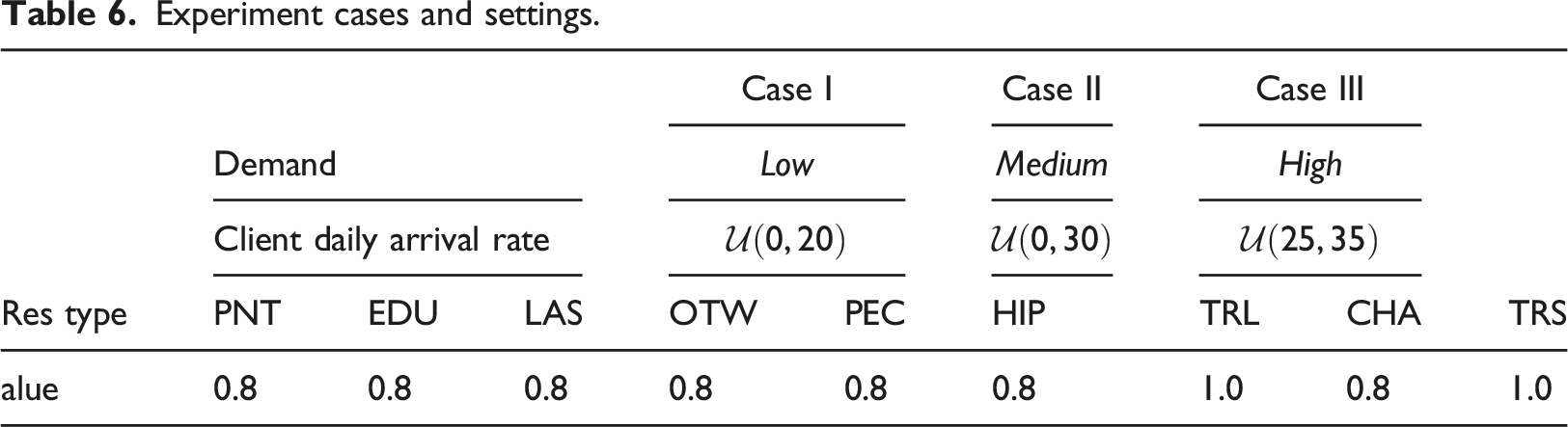
The time slot availability of each resource for each of the 32 time slots per day follows
The number of scenarios was set to 10 and several replications ranging from two to 10 were performed for each demand case to guard against spurious cases. We recorded the average (mean) for all the performance measures and in some cases the minimum and maximum values. We first investigated the impact of using deterministic (assumed to be known) resource availability versus stochastic resource availability on the performance measures. We specifically compared the results of under under no workload balancing (NWB) and under workload balancing (WB) to evaluate equity issues among CHW resources of the same type. The size of the SP model instance depends on the CHP under consideration. CHPs requiring more steps and resources lead to larger instances and generally take relatively longer to solve. Another factor that affects computation time is whether of not load balancing is required. In our experiments, the average runtime to schedule a CHP was 56 s under NWB and 77 s under WB. To determine the appropriate number of replications, we varied the number of replications from two to 10 for all three cases. We obtained similar results for number of replications above five. Therefore, we report the results based on 10 replications, which is more than sufficient for this computational study.
Results and discussion
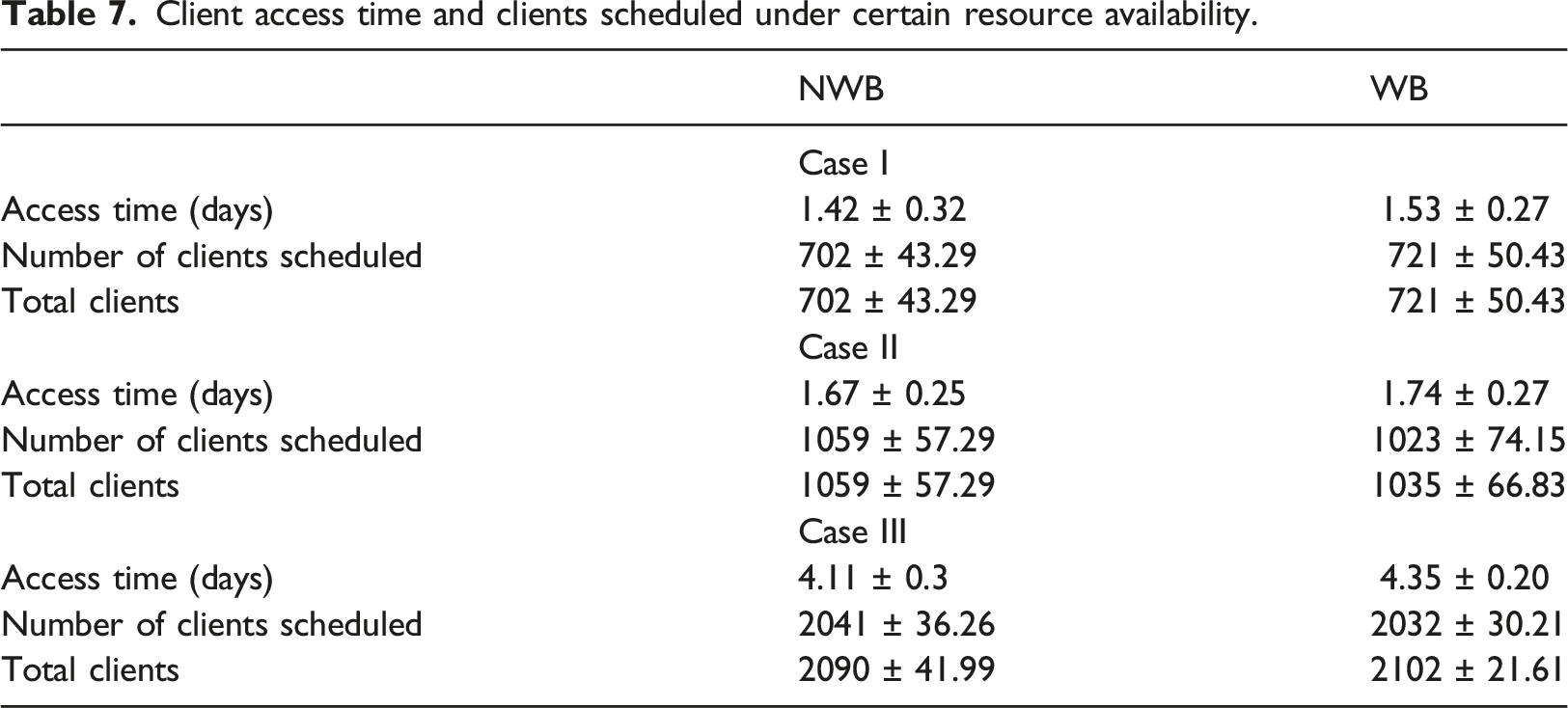
We report results for the three demand cases: Case I, Case II and Case III, which correspond to low, medium, and high client demand, respectively. We considered scheduling performance measures of client access time, number of clients scheduled, resource workload, and workload coefficient of variation, and reported these performance measures under NWB and WB. To set a baseline for comparison, we ran experiments involving 10 replications for each case using one scenario with certain resource availability randomly set using the Bernoulli distribution given in Table 6. This is often the case in practice when Pathways Community HUB managers assume expected values of resource availability. We compare this deterministic approach to the SP approach involving uncertain resource availability based on multiple scenario realizations of the random variables.
Client access time and clients scheduled under certain resource availability.
Client access time and clients scheduled under uncertain resource availability.
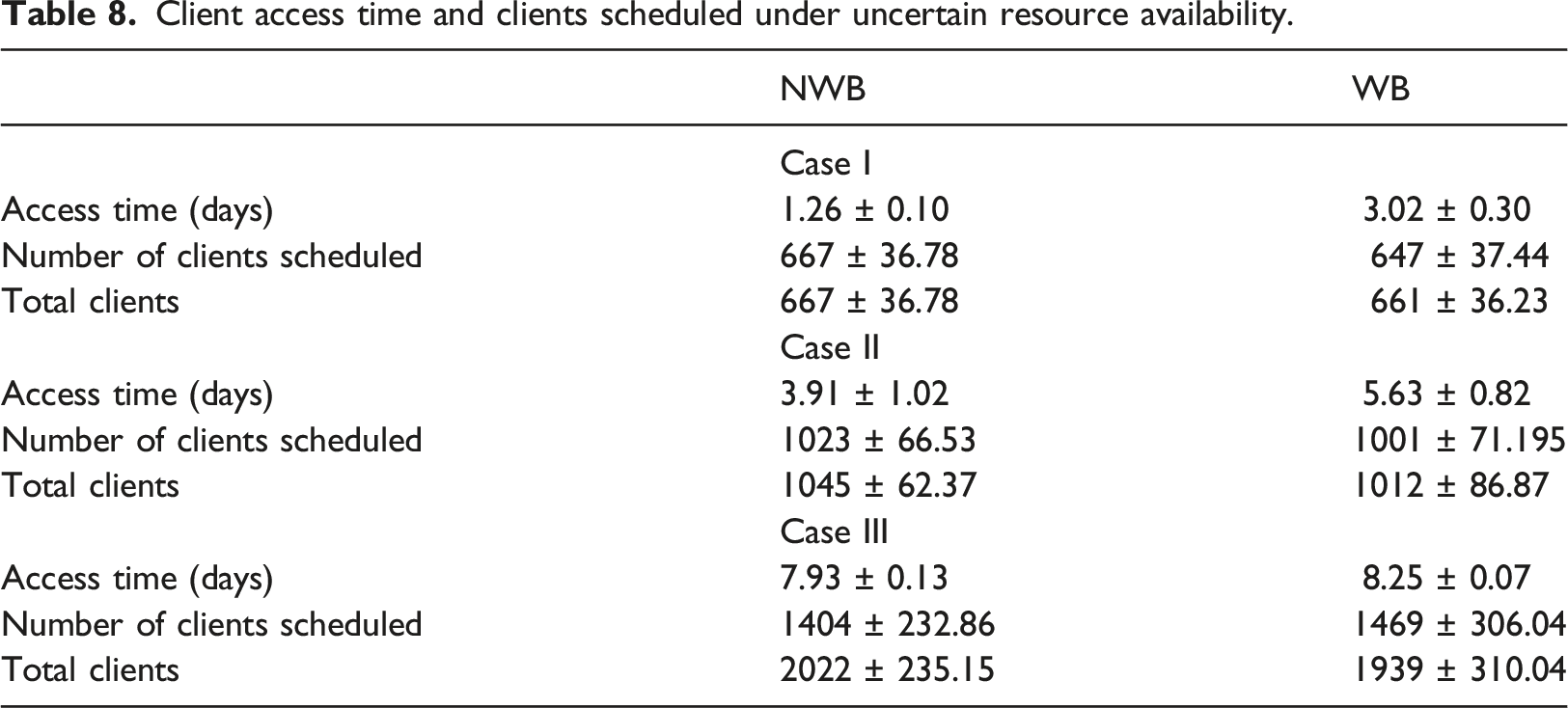
The results for the SP approach show that workload balancing can in fact affect client access time. Under NWB client access is about 1.3 days for Case I, about 3.9 days for Case II, and about 7.9 days for Case III. With WB, client access is about 3.0 days for Case I, about 5.6 days for Case II, and about 8.3 days for Case III. The results show that in general increased client demand results in increased access time and a reduction in the number of clients scheduled. Also, we see that workload balancing increases access time for both Case I and Case II. With Case III which involves high client demand, however, there is no significant increase in access time with workload balancing.
The deterministic approach provides client schedules that are too optimistic as compared to the stochastic approach. This is due to the fact that uncertainty in resource availability is not considered and results in the omission possible future scenarios. The number of clients that are not scheduled within 10 days due to resource unavailability increases with client demand. This is an indication that client volume significantly affects schedules and more clients have to wait longer to access the HUB. Gleaning further into the results, we found, for example, that most of the clients that were not scheduled were those assigned to the CHP Transportation-HEZ (see Table 4). One step of this CHP requires transportation time for 12 consecutive time slots. Consequently, to schedule this CHP the SP model has to find a schedule with 12 available consecutive time slots.
Resource utilization under no workload balancing and with workload balancing.
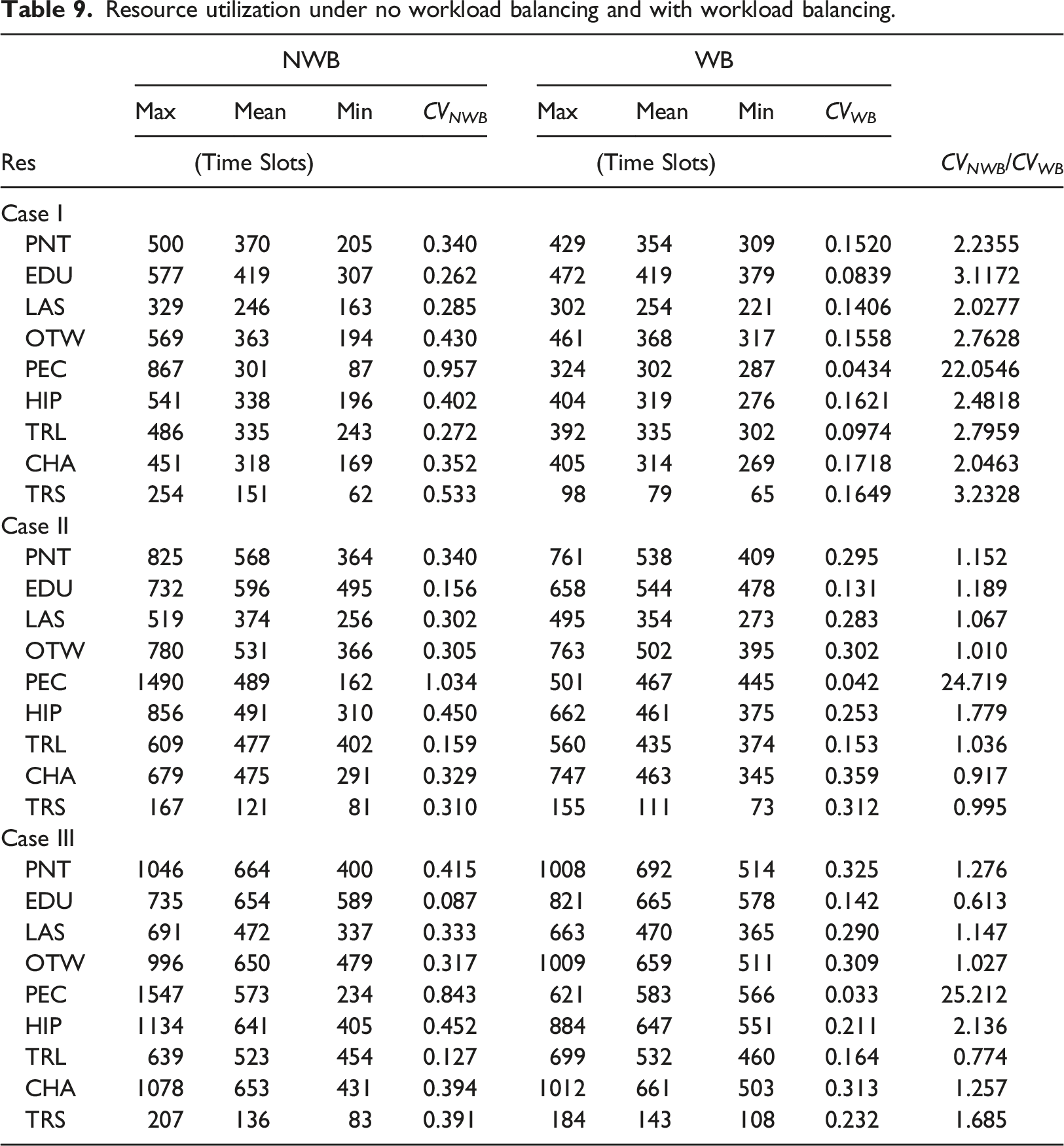
The computational study reveals that the SP approach allows to schedule clients in a Pathways Community HUB by minimizing client access time and enabling workload balancing among the resources. The results show that a deterministic approach can be too optimistic depending on how the future resource availabilities are set. Therefore, we recommend to HUB managers to use the SP approach with workload balancing. This is because the SP model significantly reduces workload imbalance among the same resource types while providing reasonable access time to clients, especially under high client demand. We should emphasize that the SP model without workload balancing can create schedules that are not equitable to some CHWs. We saw for example, how one patient counselor (PEC) worked eight times more than another PEC. Clearly, this would create unfairness concerns for the Pathways Community HUB manager. Therefore, we recommend using workload balancing to get client schedules that are equitable in terms of resource utilization.
Another advantage of the SP model is that it can easily be adapted to any real HUB and can also provide the HUB manager or scheduler a slew of useful information beyond the schedules and resource utilization results we presented. For example, by analyzing the client wait time and resource utilization, the results can provide guidance regarding which CHPs are being assigned the most and what resources are being utilized the most. This can aid the HUB manager in making decisions regarding resource capacity expansion.
Conclusion
Scheduling limited resources at a centralized Pathways Community HUB can be challenging. We introduce an SP approach for connected community health for optimally scheduling CHPs under uncertainty in resource availability. The SP methodology was implemented in a simulation setting and applied to data for a real Pathways Community HUB for a U.S. county. The computational results are promising and show that client access times depend on the HUB resources uncertain future availability and the level of client demand, with high client demand resulting in relatively longer access time. The study reveals that schedules provided by a deterministic approach where resource availability is assumed to be known can be too optimistic. Several managerial insights are gleaned from this study. For example, the SP model computes schedules that with workload balancing provide client schedules with equity across the same type of community health workers. Future work include extending the SP model to allow for resource capacity expansion considerations and developing fast decomposition techniques to speed up computations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Appendix
An example community health pathway: Insurance CHP.