
Abstract
The nursing schedule generation is an important activity that takes a considerable amount of time for managers to prepare and amend. It involves the optimal allocation of nurses to shifts, factoring various constraints like shift timings, holidays, leaves, and emergencies. This paper provides the design and development details for an automated nurse scheduling system called “ROTA,” implemented for a 2032 bed multi-specialty tertiary teaching hospital, having 1800 staff nurses and 98 wards. The system generates daily, weekly, monthly schedules, nurse face sheets, duty allocation charts, swapping schedules, and training details for nurses. The system improved managerial control and saved a considerable amount of time for nurses to prepare the schedule. A survey conducted to gauge the system’s satisfaction level showed that 91% of nurses were satisfied with ROTA. Overall, the system saved 78% of nurse scheduling time, resulting in a 3% cost reduction for the hospital.
Introduction
The nursing care regime at tertiary care hospitals consists of activities which can be categorized as direct and indirect. The clinical activities are classified as direct, and those involving administrative and managerial work are classified as indirect. A 36-Hospital Time and Motion Study in the US found nurses spent 35.3% that is, approximately 147.5 min on documentation activities, which are mostly delegable in nature. 1 Nurse managers are usually involved in making a duty schedule for staff nurses in patient care areas. The schedule should ensure optimal distribution of resources, maintaining the nurse-patient ratio, minimizing the nurse shortage, and utilizing additional staff efficiently and effectively.
A multi-country study showed that nurses’ satisfaction over work schedule flexibility directly impacted their attrition rates. Organizational factors, that is, work environment and satisfaction with work schedule, play a key role in nurses’ intention to leave the nursing profession. 2 These organizational factors can be addressed to retain nurses in the organization, and one such way to bring in schedule flexibility is through automated and self-scheduling systems. Self-scheduling or self-rostering is a methodology that shifts the responsibility of schedule creation on the nurses themselves, rather than a manager. 3 Due to this reason, self-scheduling can also decrease the nurse manager’s time spent to prepare the monthly nursing schedule. In the case study, 4 the nurses perceived adhering to program rules as an individual entitlement rather than organizational benefit, thereby floundered at self-scheduling attempts. Compared to the manual and self-scheduling, it is observed that automated scheduling saves a considerable amount of time preparing the schedule and leads to better control over the nurses’ time in delivering quality patient care.
The hospital under study is a large tertiary teaching hospital in south India with a bed capacity of 2032 and organized into 98 wards. The nursing deployment is done based on average occupancy at the start of the month. The ward’s schedule was manually prepared and maintained by the ward in-charge, who reported to the zonal supervisor. Exit interviews conducted for 207 nurses in 2018 revealed that 24 (11.5%) nurses left the hospital due to improper duty schedules. Manual allotment of nurses to shifts was the primary reason behind the improper duty schedules since all the constraints were not considered during allotment. Hence, there was a need to automate the scheduling process.
The paper presents ROTA, a system for automated scheduling of nursing duties, implemented in the hospital mentioned above. The system features include: scheduling, nurse face sheet generation, individual face sheet generation, leave analytics, dashboard, swap duty, training, etc. The efficacy of the system is analyzed through a nurses’ satisfaction survey conducted at the hospital.
The rest of the paper is organized as follows. Section II reviews the nursing literature on nurse scheduling problem, types of scheduling viz., centralized, decentralized, and automated scheduling. Section III presents the methodology covering the need for ROTA, business and software requirements. Section IV provides the features of ROTA system. Section V provides an analysis of the system’s usage via a nurse satisfaction survey and compares the system with existing literature. Lastly, Section VI concludes the paper with some recommendations for future work.
Literature survey
Scheduling refers to the allocation of time and people to perform a defined activity and can be classified as centralized and decentralized. 5 Centralized scheduling is directly under the control of the nursing head of the hospital. In the absence of reliable data on bed occupancy, centralized systems lead to inefficient schedules, compromising on patient care and staff overload. 6 Centralized scheduling can improve nurses’ satisfaction by 34% and reduce costs by 1% while allowing mobilization of nurses to busy locations and avoid overtime costs. 6 In decentralized scheduling, the head nurse plans shifts and allocation, thus facilitating decision making and directly impacting patient. 7 A scheduling case study in Egypt proved that nurse satisfaction increased substantially by creating a fair schedule system that takes care of nurses’ preferences; while decreasing the overall overtime cost by 36%. 4
The process of allocating a designated number of nurses in a specified number of shifts to cater to the hospital demand is termed “Nurse Scheduling Problem (NSP).” A well-planned schedule creates efficiency by accommodating all restrictions and variabilities and offering predefined solutions to address these constraints effectively. Such a system, robust enough to cater to real-world inefficacies, is challenging to build and implement. 8 Computationally efficient software addresses strategic planning while giving immediate solutions to unanticipated staff shortages. Several studies have opined that an investment in nurse scheduling automation improves job satisfaction while greatly reducing the costs related to overtime and turnover. 9 One study showed a positive correlation between the automated scheduler implementation and nurse satisfaction. 10
Consequences of inappropriate staffing can adversely impact hospital performance, patient experience, staff satisfaction, and nursing turnover. Nurse dissatisfaction and general fatigue were attributed to mismanagement of personnel, lack of follow-through, extended shifts, and stretched personal requirements, all of which lead to feelings of burnout. 11 These can be overcome with a robust nurse scheduling system to ensure adequate nurse-patient ratio, fair scheduling, and optimal distribution of shifts. It can improve the cost and nurse satisfaction by pooling nurses and scheduling them in one model. 6 Nursing attrition and turnover can be one result arising out of improper scheduling. Nursing care is directly related to patient outcomes, and hence high turnover rates negatively impact care delivery. 12
Hospital staffing turnover accounts for almost 5% to 5.8% of the operating budget through replacement and training costs. 13 The hospital managers inevitably assume an inseparable dependence on the number of staff required for the scheduling activity. 9 When hospital managers face immediate budget pressures and evidence-based means of rationing nursing care is unavailable, nurse attrition is left unattended whilst assuming that full nursing care will be made available to the patient by the existing workforce. 14 Nursing Turnover Cost Calculation Methodology (NTCCM) includes pre-hire (recruitment, vacancies and hiring) and post-hire practices (training, decreased productivity of the new employees during their learning curve, and termination) costs. 15 If organizations face attrition or turnover due to improper scheduling, then automated scheduling is one solution to optimize this problem and reduce attrition and costs.
There are several challenges to implementing an automated scheduling solution. First, the nursing staff’s satisfaction levels need to be considered, which is affected by multiple-preference ranks and priority ordering of schedules. Second, the planned shifts and days-off should be fair and successfully meet the preferences of all the nursing staff. 16 Preparing a monthly schedule consists of a series of coordinated actions that require recognition of staff, collection of data needed to characterize the clinical reality, comparison of those data with the literature, and development of a proposal for action. 17
Methodology
The methodology consists of three phases viz., the initial exploratory study to consult with the hospital stakeholders on the need for scheduling automation, elicitation of business requirements, and software requirements.
Exploratory study
Brainstorming sessions were held with all the stakeholders involved in organizing the nursing workforce in the hospital. This warranted discussion with the hospital’s administrative heads who were directly involved in all the managerial decisions; clinicians who would be utilizing the services of the nurses at their respective units; the nursing head and her team who faced the challenge of scheduling everyday duties for the nurses. The following issues were raised during the meeting:
(1) Shortage of nursing staff in selected departments and excess in others
(2) The inability of the nursing managers to have a hospital nursing face sheet to identify the excess and shortage of staffs
(3) Administrative issues like inadequate managerial control and
(4) Human resource management issues like the number of working days for staff nurses and uneven distribution of leave, often leading to favoritism in the allocation of shifts
These issues generally brought down the morale of the nursing staff. It was essential to bring to a consensus all the measures being taken to automate the scheduling without compromising the quality of care to the patients. An equally important factor is the nurses’ quality of work life. The size of the hospital was also a concern, with 98 wards and 1800 staff nurses.
Elicit business requirements
Subsequent to the exploratory study, a structured questionnaire was prepared to gather the specific requirements for automation. The scheduling solution had to be designed considering the regulatory requirement, operational requirement, and the staff’s personal preferences, as detailed in Table 1. The demand modeling concept was employed to complement the scheduling process automation, which determines how many staff are needed at various clinical units. It further provided clarity on predicted patterns of duties, by considering the staff demand requirements.
Regulatory requirement, operational requirement, and personal preferences.

Software requirements
The next critical phase was identifying the software providers who could provide the solution based on the exploratory study and the business requirements. Since the hospital has 2032 beds and includes teaching modalities, a customized solution was crucial from the business perspective. A meeting with the incumbent software providers of the existing hospital information system was arranged to discuss the software’s functionalities. This also had to align with the hospital’s business requirements and the requirements listed in Table 1. The software partners came up with a definite plan for the automation and customization, keeping all the necessary modules that eventually would be implemented.
ROTA system implementation
ROTA system is developed using Java Spring Framework, HTML5, and Javascript. The backend is implemented using MYSQL database, and the application is deployed on Google Cloud running Apache Tomcat server. The key features of the ROTA system are depicted in Table 2.
Features of the ROTA system.

Some screenshots of the ROTA system are shown in Figure 1. Figure 1(a) shows the ROTA Dashboard; 1(b) depicts the Nursing Face Sheet; 1(c) displays the Daily Schedule; and 1(d) depicts the Monthly Schedule.
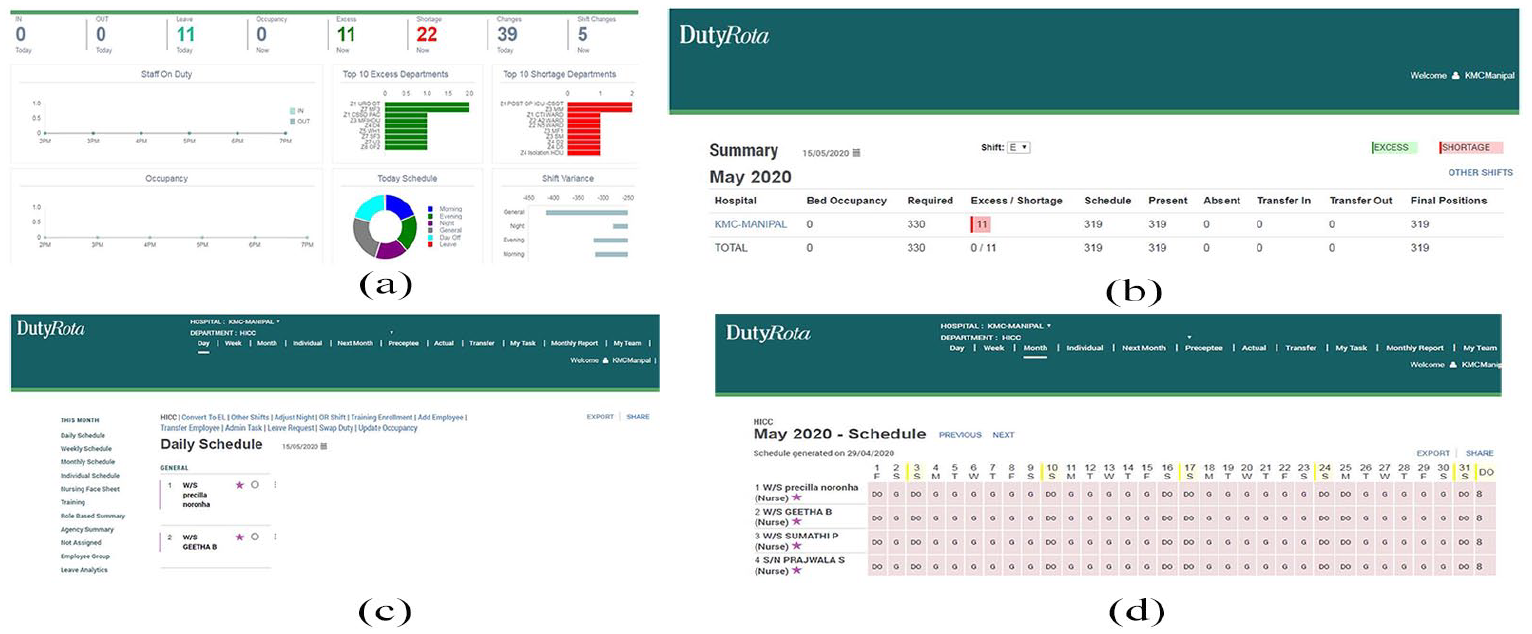
Screenshots of ROTA system: (a) dashboard, (b) nursing face sheet, (c) daily schedule, and (d) monthly schedule.
Results and discussion
Before ROTA system implementation, a manager would spend approximately 45 min to prepare the nurses’ schedule. The time could be extended subject to changes due to patient occupancy, staff availability, internal and zonal transfers, and leave allocation. Thus the man-hours spent for manual scheduling amounted to 73.5 h. As scheduling is done on all working days, considering 25 working days a month, the man-hours spent per year is calculated at 22,050 h. Assuming 8-h shifts, 2756 man-days are required for scheduling. Taking average salary as basis, the cost per man day stands at ₹992. Thus, the total cost for 2756 man days is ₹2,733,952.
With the implementation of the ROTA system, there is a substantial reduction in both cost and effort. After excluding the cost for software development, the savings from automation is ₹2,373,952 per year, which is nearly 3% of total salaries allotted to the nursing pool. Regarding the effort, it takes a maximum of 10 min for the manager to prepare the schedule, which is a substantial reduction in productive time. The system saved 175 man-hours, that is, 78% of ward-incharge’s time spent on hospital’s scheduling activities.
In order to measure the nurses’ satisfaction with the ROTA system, a Likert-scale based questionnaire was designed, listed in the Appendix section of the paper. A total of 210 nurses participated in the survey having designations as ward in-charge, senior staff nurse, and ANS (Assistant Nurse Superintendent). The socio-demographic characteristics of the nurses’ sample involved in the study are depicted in Table 3. The mean experience of the nurses is 27.66 years.
Socio-demographic characteristics of the nurses’ sample.

The survey responses were captured in five-level Likert items of “Strongly Disagree,” “Disagree,” “Neither Agree nor Disagree,” “Agree,” and “Strongly Agree.” SPSS software was used to analyze and interpret the responses. Cronbach’s alpha coefficient, a statistical tool that quantifies an instument’s reliability on a scale of 0 to 1, was used to assess the questionnaire’s internal consistency. For the nurses’ satisfaction questionnaire, the Cronbach Alpha value is 0.865, which indicates high reliability and correlation among the questions.
Out of the participating nurses, 18 (8.5%) were “Extremely Satisfied” with the system; 99 (47.14%) were “Satisfied” with the system; 73 (34.76%) were “Moderately satisfied,” and only 20 (9.5%) were “Not at all Satisfied” with the system, as shown in Figure 2(a). Designation-wise, senior staff nurses (98.63%) were most satisfied with the system, followed by ANS (92.8%), as shown in Figure 2(b). Department-wise, OPD nurses were extremely satisfied with the system scheduling, as depicted in Figure 2(c). In the not satisfied category, 17 (85%) were general ward nurses. However, a vast majority (86.2%) of them are overall satisfied with the system, hence there is no major concern.
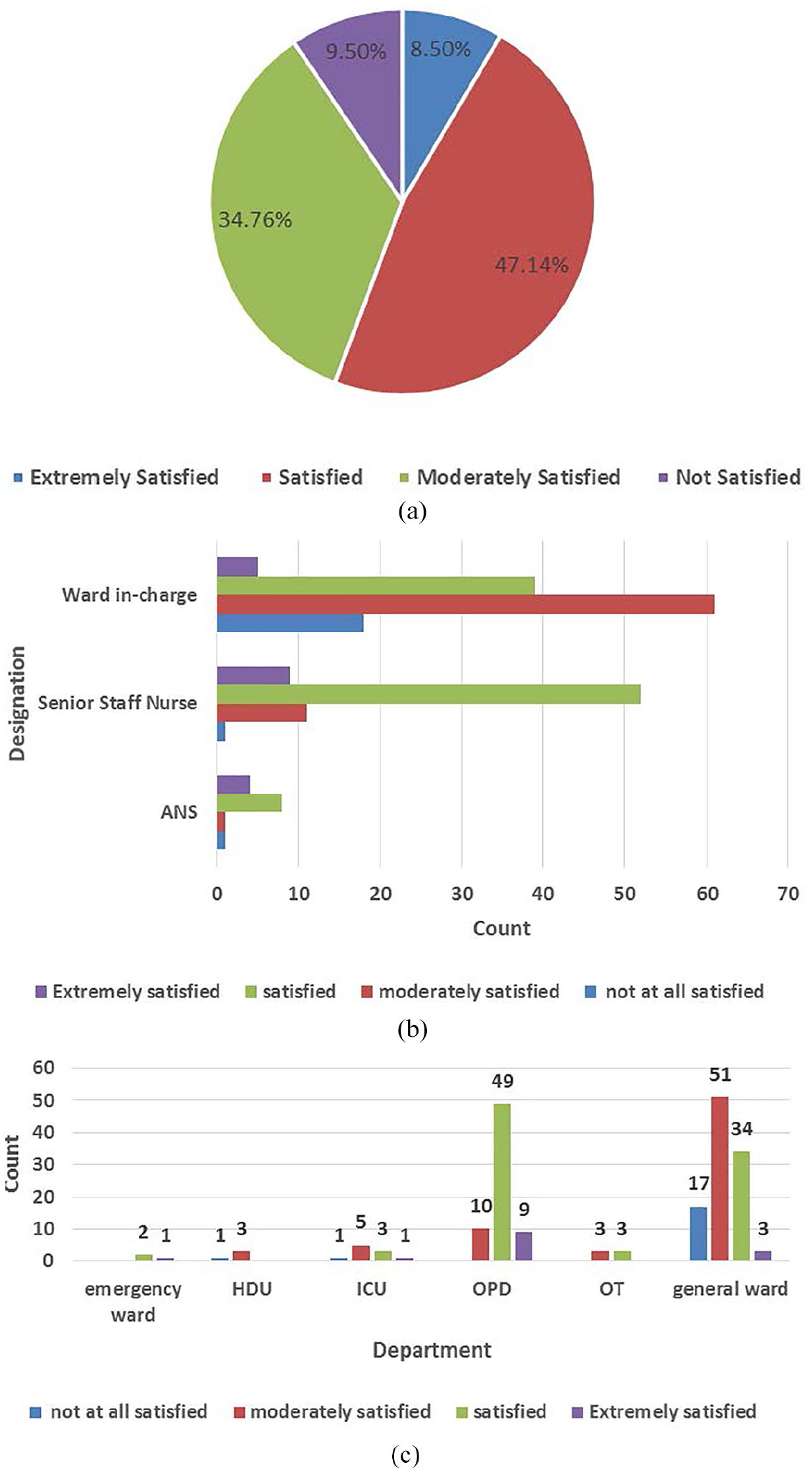
Nurse satisfaction levels for ROTA: (a) overall nurse satisfaction of ROTA system, (b) designation-wise satisfaction levels, and (c) department-wise satisfaction levels.
We evaluated the Hypothesis: “Whether the years of experience of a nurse has an impact on the overall satisfaction of the system” using SPSS. The Spearman Rho coefficient value was −0.137, which indicates “negative and weak” correlation; also “p” value was 0.051 (which is > 0.05), hence the null hypothesis is accepted and we conclude that years of experience of a nurse has no impact on their overall satisfaction of the system.
The month-wise leave analysis, since ROTA implementation, is shown in Figure 3. In the chart, CL denotes “casual leave,” CYL denotes “casual yearly leave” and CML represents “commuted leave.” The inference from the data is as follows:
CYL+CML data trend has come down from February-19 to March-20.
CL data trend has gone up from February-19 to March-20.
CL+CYL+CML data trend has come down from February-19 to March-20.
CYL+CML has come down from 1963 days in February-19 to 1039 days in February-20. That is an improvement of 924 days leaves in a month.
CYL+CML+CL has come down from 2328 days in February-19 to 1310 days in February-20. That is an improvement of 1018 days leaves in a month.
CL has increased from 365 days in February-19 to 1713 days in December-19.
Total CML+CYL leave reduction considering February-19 as the base is coming as 10,218 days.
Total CL leave increase considering February-19 as the base is coming as 3690 days.
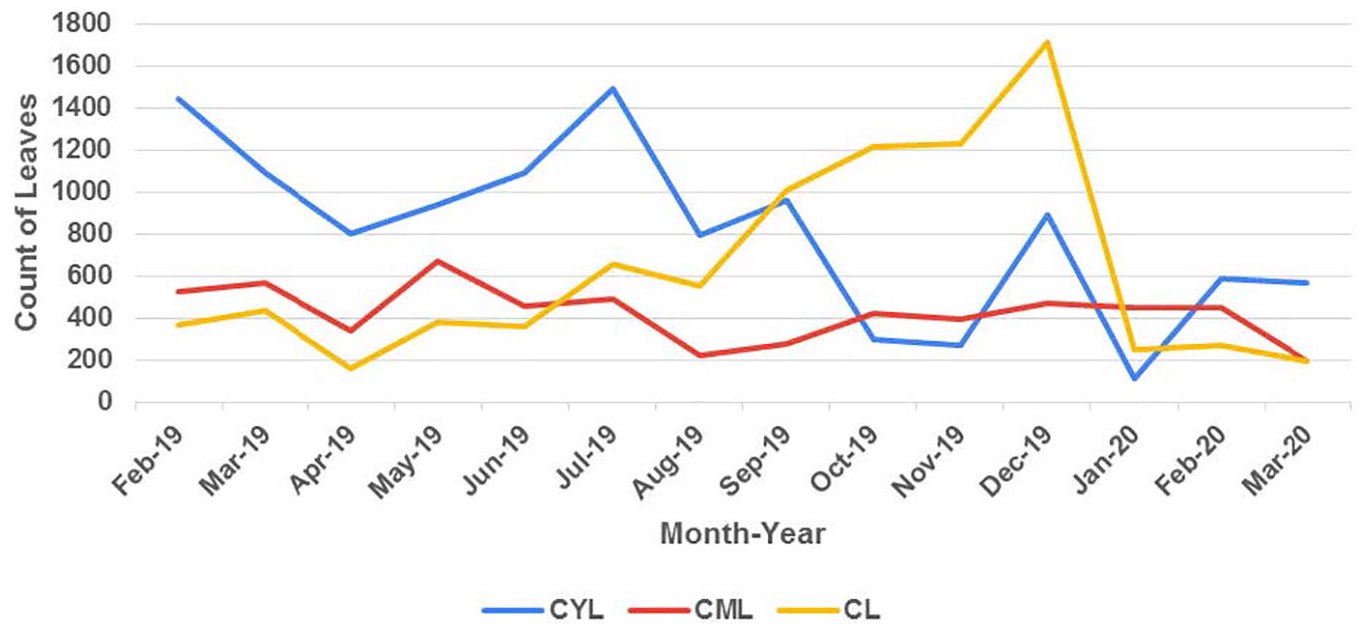
Leave analysis since ROTA implementation.
Discussion
Bailyn et al. 17 implemented a pilot project on self-scheduling for hospital nurses. They contend that the attempt floundered, since the nurses did not adhere to the program’s rules, despite repeated efforts by the nurse manager. We also faced similar issues regarding non-compliance and resistance to change. Constant reinforcement, deliberations, training, and retraining strategy was adopted to combat this problem. Managers have now willingly accepted the system.
Lack of basic computer skills and lack of confidence, limit the usage of the system effectively by the nurses. 18 To mitigate this problem, exclusive training was provided to the nurses in using the system. Since most nurses have a basic “nursing” degree and have used computer systems before (excel, word applications), they adapted quickly to the system. This fact is established in the nurses’ answer to Question item 3: “I have adequate computer skills to operate the system” in the survey, wherein 74.76% of the nurses agreed that they were very comfortable in using the system.
The shortage of nurses can have a detrimental effect on the operations of the hospital. 19 It impacts the care delivery process, resulting in delayed nurse response to patient calls, staff communication problems, reduced number of available beds, delayed discharge, increased patient wait time for surgery or tests, discontinued/closed patient care programs. In the ROTA application, the nursing face sheet enabled the view of the distribution of nurses across the hospital’s various units. This led to efficient utilization of the nurses, wherein excess nursing staff were distributed to areas having a shortage.
The paper 6 recommends that centralized scheduling of nurses reduces overtime and improves cost savings. In congruence with this argument, the ROTA system performs centralized scheduling by pooling nurses from multiple zones, which reduced 78% of total nurse scheduling effort and achieved 3% overall cost reduction. In addition, the system solved the challenge of inadequacy of senior staff nurses at each shift. Since the attrition rate among nurses is high and cut off allocation was 10% of seniors, which was later raised to 20%, more nurses were recruited to fill in the shortage of nurses at various departments.
Intra team communication plays a key factor in providing robust healthcare. 20 Post ROTA implementation, intra nurse communication w.r.t administrative activities has improved. On a ballpark calculation, approximately 3000 days of casual leaves are saved annually, and 7000 days of productivity improvement is seen, resulting in more nurses reporting to duty.
The paper 21 argues that hospital information systems significantly improves the decision making capabilities of hospital administrators. Supporting this argument, the ROTA system implementation has substantially improved the decision-making process within the hospital. From an administration perspective, nurses’ shortage can be identified beforehand, and adequate steps can be taken to fill the shortage. Nursing care has also improved, because of adequate nurse-patient ratio.
Conclusion
Nurse scheduling is an important activity within any hospital, which involves assignment of nurses to shifts, under constraints of time, efficiency, and cost. The paper presents ROTA—an automated solution for nurse scheduling, implemented for a tertiary teaching hospital in south India. The system provides a centralized solution for automating the daily, weekly, and monthly schedules; generating nurse face sheets; furnishing attendance graphs and leave analytics; and enabling nurse transfer among hospital units. The system’s efficiency was analyzed by conducting a nurse satisfaction survey on a sample size of 210 nurses, wherein 91% of them expressed overall satisfaction with the working of the system. Overall, the ROTA system implementation was a success and well received by the hospital’s nursing community.
Future work includes: (a) integration of ROTA with HR application within the hospital; (b) analyzing the reduction in attrition rate due to proper allotment of nursing shifts in the hospital.
Footnotes
Appendix
Nurses’ survey questionnaire is presented below:
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not needed, since there was no research involving human subjects or animals.