
Abstract
Keywords
Introduction
Established by the 1988 Federal Constitution, the Brazilian National Health System (SUS) is one of the largest public health systems in the world, representing a unique initiative that provides free access to health for the Brazilian population.1,2 It has evolved from an exclusionary general health system, in which a small minority had the right to health services, to a universal, complete, and equitable system, in which health became a right for all and a duty of the State; the SUS is constantly improving and creating new policies according to the needs of the population as it is implemented in a country with continental dimensions.1,3 Among the policies constituting the SUS, the National Primary Care Policy was designed to develop accessibility, completeness, social participation, and user embracement with health services. 4 Since its proposal, it has promoted the Family Health Strategy (ESF) in Primary Health Care (APS), which is aimed at families and communities in Brazil. The ESF was instituted to reorganize, expand, qualify, and consolidate primary care in Brazil, encompassing intersectionality, multidisciplinarity, and social participation.4,5 This initiative has created an active connection between communities and healthcare services through collaboration among multi-disciplinary health teams. These professionals, known as Community Health Workers (CHWs), engage directly with families linked to the primary health care facilities in each area. The initiatives spearheaded by CHWs have significantly diminished key factors associated with infant mortality, cardiovascular diseases, and hospitalizations due to chronic conditions.6,7 In this context, digital technology plays a crucial role in modernizing and enhancing healthcare services. The employment of digital platforms and mobile applications makes CHWs more accessible in remote or underserved regions, thereby diminishing geographical obstacles and broadening community engagement. 8 In recent years, the adaptability of smartphones and tablets has stood out as a noteworthy innovation in the health sector. These digital tools have become indispensable in the prevention, detection, and treatment of diseases, as well as in supporting healthcare professionals, particularly throughout the COVID-19 pandemic.9,10 The ongoing necessity for technological advancement that actively promotes accessibility, comprehensive care, community involvement, and patient engagement in healthcare services is clear. 11 The development of new mobile apps, particularly designed for CHWs, aims to streamline these professionals’ work by lowering costs and enhancing the efficiency of time and resources. The e-SUS Território application, incorporated into the e-SUS APS strategy, was developed to streamline the workflow of community-based health dynamics, assisting multidisciplinary CHW teams in delivering equitable healthcare across Brazil. Therefore, this study sought to evaluate the usage of the e-SUS Território app by CHWs in Brazil. The Brazilian government has provided the application free of charge to all municipalities since October 2016 as an integrated technology on the e-SUS APS strategy.
Background
The Brazilian community health workers program
This program was created in 1991 and initially implemented in southeastern and northeastern Brazil. The work and scope of CHWs expanded with the implementation of the Family Health Program, the precursor of the ESF, throughout Brazil to improve the health conditions of communities, broadening the scope of coverage and the structuring of APS in Brazil.12,13
CHWs are responsible for numerous duties, including carrying out the demographic, social, cultural, environmental, epidemiological, and sanitary diagnoses and mapping the team’s area of operation, developing health promotion activities, disease and disorder prevention through home visits, providing guidance on actions and services in its territory, enrolling and registering individuals and families, keeping information systems up to date, developing actions that seek to integrate the health team and the community, and measuring vital signs and changing dressings. Among these attributions, the home visit is the most important activity for the work of the CHWs.4,13
Because they know the region where they work, CHWs strengthen bonds of hospitality, respect, and emotional responsibility for the families they serve. During their work with the population, it is up to them to identify risk situations and report them to other members of the health teams, consolidating user-centered collaborative practices and facilitating health decision-making.14–16
Estimates of the indicators of community health workers in primary health care in Brazil in December 2020.
Source: Data extracted from SAPS panels on March 26, 2024 (SAPS, 2024). 19
Legend: Northeast region: composed of the states of Maranhão, Piauí, Ceará, Rio Grande do Norte, Paraíba, Pernambuco, Alagoas, Sergipe, and Bahia; North region: composed of the states of Acre, Amapá, Amazonas, Pará, Rondônia, Roraima, and Tocantins; Midwest region: composed of the states of Mato Grosso, Mato Grosso do Sul, Goiás, and Distrito Federal; Southeast region: composed of the states of Rio de Janeiro, São Paulo, Minas Gerais, and Espírito Santo; South region: composed of the states of Paraná, Santa Catarina, and Rio Grande do Sul; % of coverage: calculated based on the resident population in each state according to the Brazilian Institute of Geography and Statistics.
In 2017, Ordinance No. 2436 was approved, establishing the new National Primary Care Policy. 4 The changes instituted with the new ordinance may have contributed to reducing the CHWs’ population coverage, mainly due to health teams’ flexibility and the non-obligation to hire these professionals.20,21 It is also believed that creating the Previne Brasil Program may have negatively interfered with the calculation basis of coverage indicators. 22 which now considers citizens with active records in the APS records and no longer the population residing in the municipality.
The e-SUS APS strategy
The e-SUS APS is a national strategy instituted and coordinated by the Ministry of Health since 2013 to strengthen information systems and the computerization of APS services. The strategy has focused on developing technological solutions for APS, such as the Electronic Citizen Record (PEC e-SUS APS) and applications that can be used by health professionals (e.g., the e-SUS Território application), which will be described below, and the applications: (1) e-SUS AD, which is used to register home care, (2) Gestão e-SUS APS, which assists managers in viewing indicators and reports, (3) e-SUS Vacinação, used for registering vaccine applications, and (4) e-SUS Atividade Coletiva, utilized for registering collective activities carried out by health teams.
All applications are integrated with the PEC e-SUS APS, which is used in over 24,000 basic health units and is considered the largest APS record in the country. This integration occurs by sending data in thrift format between the application, the municipal installation of the PEC e-SUS APS, and the National Health Center.
Before implementing these solutions, the teams recorded their activities in physical paper records, which presented a series of losses concerning the time used, information security, and storage of records, among others. Without the e-SUS Território application, the ACS carried out their activities in the community using printed forms where patient information and activities were recorded. This model was inefficient since it culminated in typing these forms into the e-SUS APS medical record, culminating in the development and adherence to using the e-SUS Território application over the years, which is detailed below.
The e-SUS Território application
The e-SUS Território application was launched on October 6, 2016, to facilitate the CHWs’ work in collecting and consulting data from citizens and allowing health teams to have greater knowledge about Brazil’s sanitary and health conditions. Its development process was mainly based on understanding and meeting user needs, considering the main scenarios of use and their particularities, both in terms of the process and user profiles.
From the operating model to the color palette, the functionalities were designed to provide comfort, productivity, and work optimization to the CHWs. For instance, the application’s screens are composed of contrasting and calming colors, which, considering the age group of users over 35 years old and the scenario of use during visits to the community under sunlight in open environments, facilitates the assimilation of information and reduces fatigue during use of the tool. Additionally, considering the routine activities of home visits, the application’s content is organized to prioritize the geolocation of the records, further improving its use.
In addition, the application was designed to allow CHWs to register and manipulate information offline, through which the on-demand synchronization process enables users to not rely on internet access to perform their duties. The “offline first” architecture proved to be an essential strategy for low or no connectivity scenarios, which are common given the size of Brazil and the activities carried out in communities far from urban centers, such as riverside and indigenous communities.
The application was also designed for users with low technology proficiency; it was developed with specific interface components that confirm users’ actions, allowing it to be utilized even by users with little dexterity. Such components were integrated with textual feedback for the user to make its use as didactic as possible. When prototyping the application, consideration was also given to its complete responsive adaptation to smartphones and tablets and, consequently, the possibility of using it on small and low-resolution screens and larger ones, thereby expanding its adherence.
Indeed, filling in data on smartphones and tablets poses risks related to typos or entering incongruous information resulting from the low tactile response of on-screen keyboards. To ensure higher accuracy in the records, the application automatically fills in all the data that can be inferred from the context or using the relationships between the records. Lastly, to optimize the processing of interoperated information and speed up the work of the CHW, users can choose to synchronize the records with the database of citizens and properties from their territorial jurisdiction (i.e., without viewing the records of other CHWs). This synchronization model is a strategy for the device’s low storage capacity and possible connectivity limitations, providing an additional layer of privacy protection for the information collected.
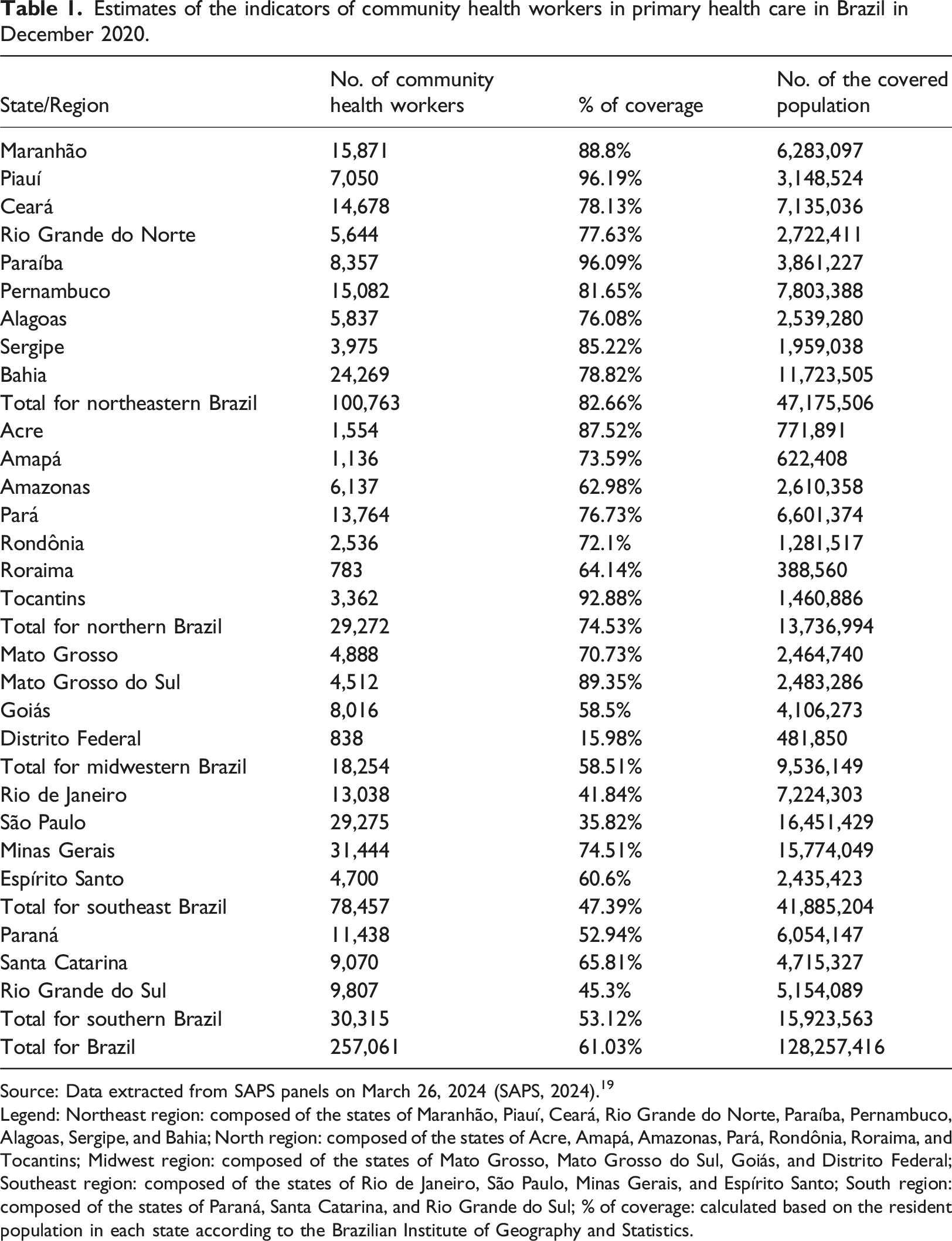
The e-SUS Território application stores, updates, and sends at least three sets of information based on actions performed by the CHW, namely: the Home and Territory Registration Form, the Individual Registration Form, and the Home and Territorial Visitation Form (Figure 1). Home and Territorial Visit registration screen.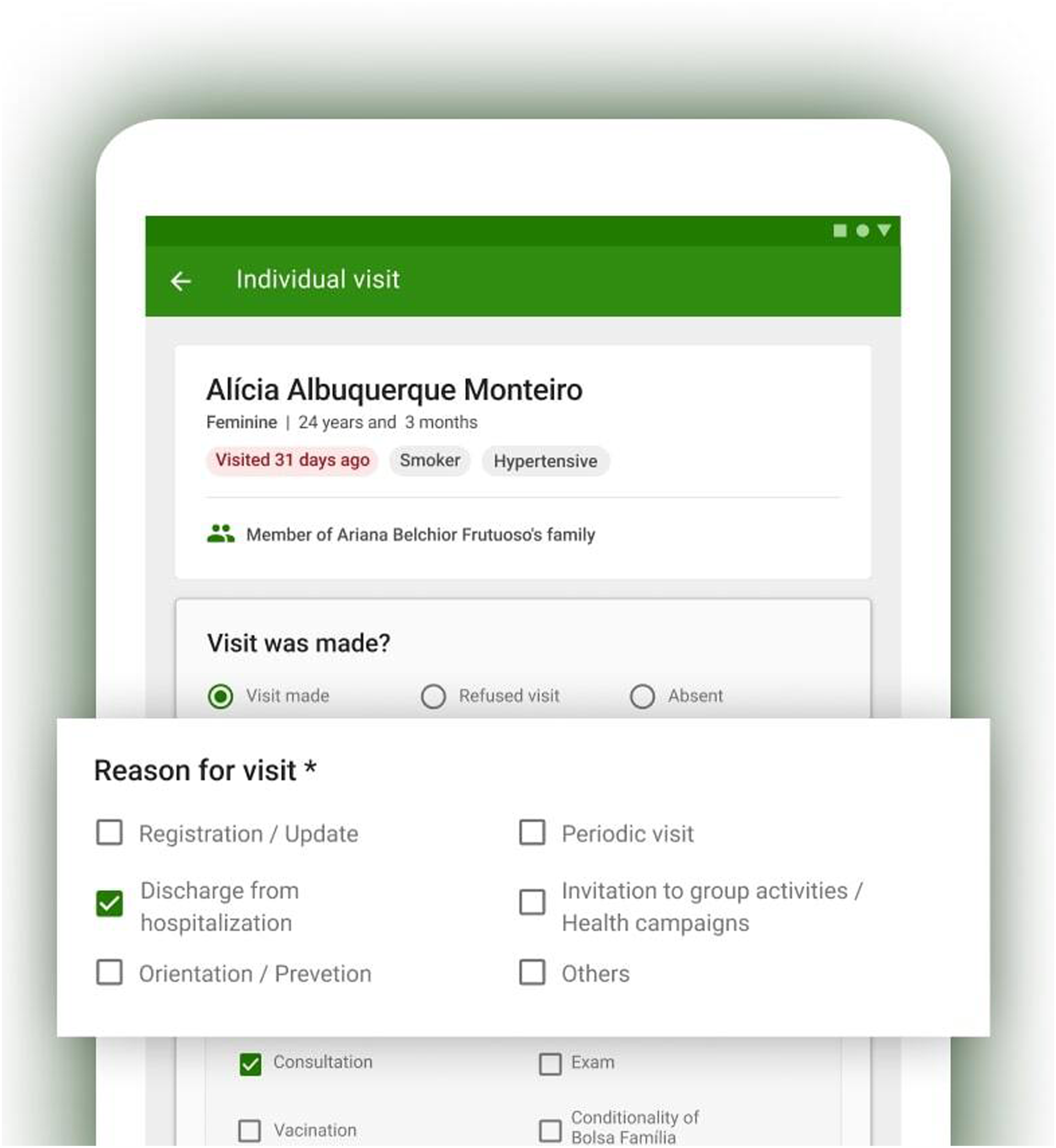
CHWs can manage households, families, and citizens through these information models by updating or registering new records in the databases and informing home visit actions with a follow-up approach without necessarily updating the data (Figure 2). The user also has various filters and searches to consult the database and identify target populations for health initiatives. Thus, based on this information specialization, it is possible to prioritize home visits to families and citizens with more needs or be included in target groups of active search actions. Management screen for families residing in a household.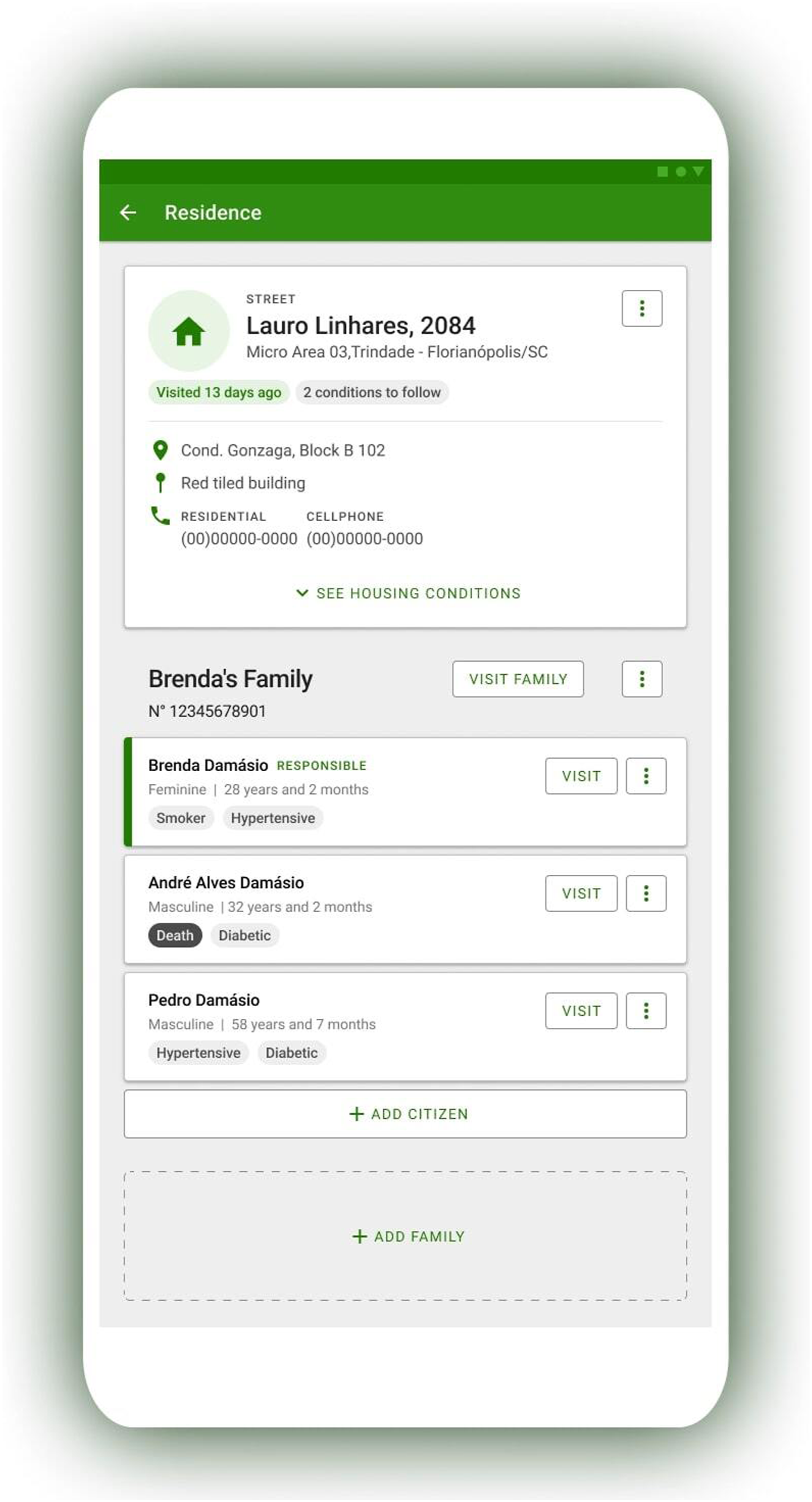
The application also allows CHWs to issue reports on housing conditions, sociodemographic data, and health status. The housing conditions report displays data on housing conditions and basic sanitation, the sociodemographic report presents information on age group and sex, allowing users to demographically analyze citizens, and the health situation report consolidates data extracted from citizens’ self-reported health conditions.
Furthermore, the application allows CHWs’ to associate geographic coordinates to property registrations, allowing the user to map their exact location and filter resident citizens and households in terms of information on the date of the last visit, sex, age group, health condition, type of property, and others (Figure 3). This functionality enables follow-up actions to be easily directed to the priorities defined by the health team. Territory map screen with the filters applied.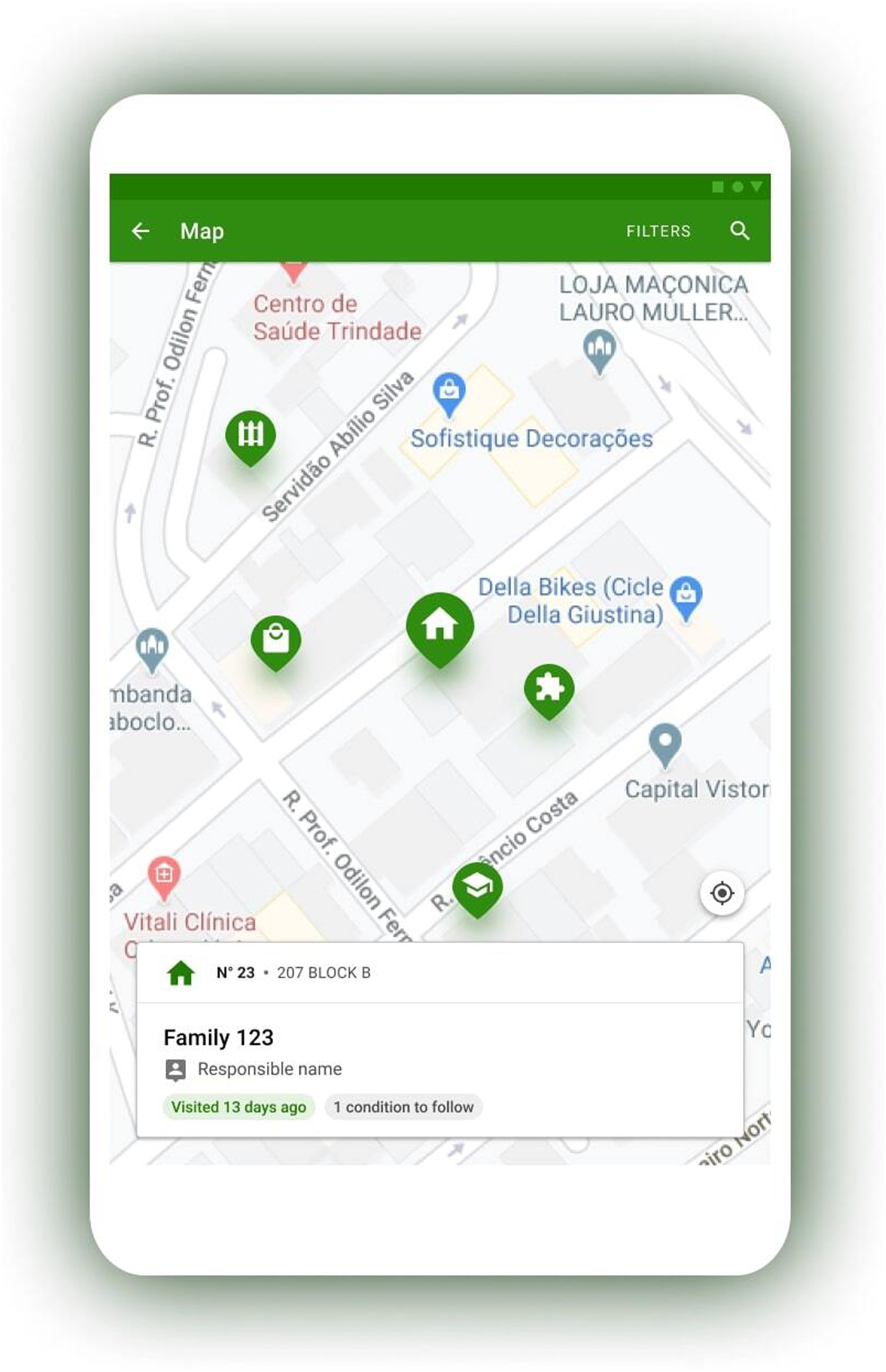
The application also has the functionality of georeferencing visits, and the data is collected from the device’s geographic coordinates when the CHW registers a home visit. This enables this professional’s work to be analyzed in the territory concerning the productivity of the professional and accuracy of the information, as it can be inferred that data recorded in loco is more accurate than those recorded later.
Methods
This is a descriptive study, where usability data from the e-SUS Território application were extracted and analyzed, from 2019 to 2022. Data was exported from Google Analytics in January 2023. Productivity indicators (records sent to the database and user engagement), the number of users (monthly and annual active users), and their distribution in the national territory (users by state and municipality) were analyzed.
The data was extracted and organized into a table by two different authors, where it was possible to analyze the evolution of adherence to the application over the years. This extraction was conducted using Google Sheets. To delimit the years, temporal delimitation filters were used (for example: January 1, 2019 to December 31, 2019). Figures from the Google Analytics dashboard itself were also analyzed, which present graphs and a map of the application’s usability in the country, were evaluated.
As this research descriptively presents the application’s functionalities and uses its usability data from Google Analytics, approval from the human research ethics committee was not requested. The usability data extracted from Google Analytics is not individualized, so it is not possible to identify application users.
Statistical analysis
Descriptive statistical analyzes were performed to assist in describing the data set. A percentage calculation was developed to summarize the coverage of community health workers. For all other analyzes absolute values were used.
Results
e-SUS Território usability data
Since its launch and implementation in the basic health unit, the e-SUS Território application has increased exponentially, making it an important tool for the CHW and other health professionals. In 2019, the application had 65,000 active users in that year, leaping to 229,000 in 2020, 364,000 in 2021, and 425,000 in 2022. In June 2022, it reached the mark of 141,000 monthly active users, representing 54.8% of the total CHW working in Brazil. 23
Number of e-SUS Território users in Brazilian states in 2022.
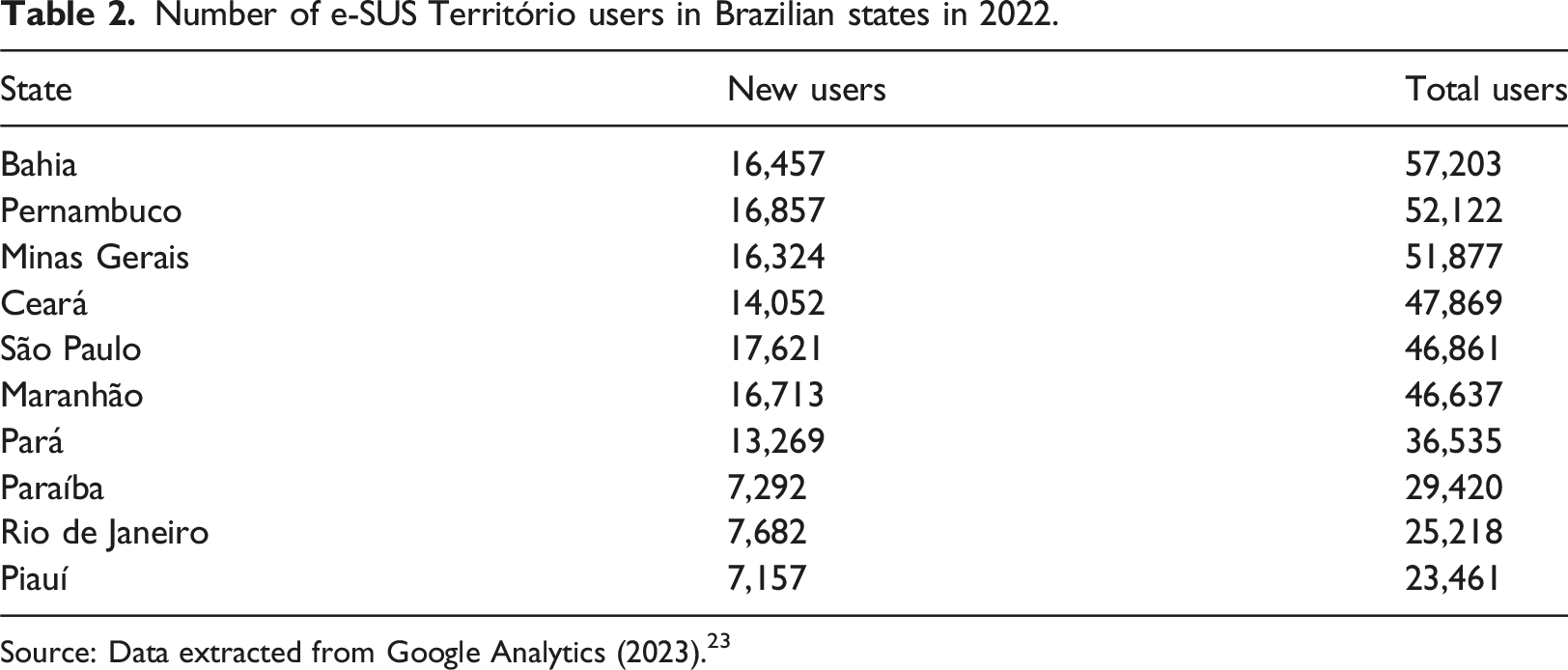
Source: Data extracted from Google Analytics (2023). 23
Nevertheless, the municipalities with the most users are São Paulo, Recife, Fortaleza, Belo Horizonte, Rio de Janeiro, Belém, and Salvador, totaling over 144,000 users in 2022. 23 Along with the increase in users, the production data generated by the application also grew proportionally, demonstrating the assiduous use of the CHWs. In 2022, 50,383,450 inclusions or alterations of citizen records, 17,255,587 inclusions or alterations of household and family records, and 293,383,678 visits to homes, families, and/or citizens.
The average engagement time per user in 2022 was 22 h and 11 min across an average of 78 sessions per user in the same year. Combining these indicators results in an average of 17 min of use per session. 23 Such findings are positive, as they demonstrate that the CHWs spent less time recording their work information in each logged session, leaving more time of their workload for caring for and providing attention to families and communities.
Unfortunately, it was not possible to compare usability data from e-SUS Território with markers of the work process performed in the period before the launch of the application, where manual records were made on printed forms, which characterizes a limitation of our study. Furthermore, the official database from which the numbers of CHWs were extracted only presents information up to 2020 (Table 1). 19 It was also not possible to analyze the indicators of health conditions where the application was widely used to assess its impact on the health of populations, characterizing a gap to be studied in future research.
Discussion
After nearly a century of experience, innovation, adaptation, and evidence, national CHW programs have emerged as critical components to achieve global health objectives, including achieving universal coverage by 2030. 24 Several countries have implemented health policies and programs with a community focus, deploying professionals to work directly in these areas. While the roles and responsibilities of CHWs are recognized across the Americas, Europe, Africa, and India, there are variations from one country to another. In most South American countries, with the exception of Uruguay, these professionals bear a resemblance to Brazilian CHWs, as they are integral to multidisciplinary teams and serve specific territories, in capacities ranging from salaried employees to volunteers.25,26
In the United States, for instance, a standardized national framework for the licensing or credentialing of CHWs is absent, and only 16 states provide some form of professional certification or training for CHWs. Yet, in other nations, such as Canada, Bangladesh, and Afghanistan, the role of CHWs is more established, encompassing their involvement in the determination of social indicators among immigrant and refugee populations.27,28 In Brazil, it is estimated that the contributions of CHWs in executing high-impact health initiatives, such as oral rehydration therapy, vaccination campaigns, and the monitoring of pregnant women and children, have positively influenced maternal and child morbidity and mortality rates. 12 Further studies highlight activities like verifying the pregnant woman’s health card, arranging prenatal consultations, monitoring for risk signs, and providing newborn care guidance as critical functions of CHWs. 29 Given Brazil’s diverse biomes and extensive geography, extending public policies to all communities presents a formidable challenge. Brazil’s rich cultural diversity, which includes riverside communities, indigenous tribes, and descendants from numerous ethnic groups, further complicates the access to and comprehensiveness of health-focused public policies. With a burgeoning population of 212.6 million spread across its vast 8,516,000 km 2, Brazil’s demographic and territorial diversity stands out.20,30,31 Many low- and middle-income countries have recognized the potential of mobile technology to enhance PHC by improving the operational efficiency and workflow of CHWs. Within these contexts, CHWs have successfully utilized mobile technology to address a wide range of health issues, including maternal and child health, sexual and reproductive health, family planning, general health, acute respiratory infections, infectious diseases, and injury and trauma. 32 These successes resonate with Brazilian policy initiatives aimed at broadening the CHWs’ scope of action, indicating potential future enhancements for apps related to data recording and sharing among healthcare teams. Monitoring families and households must be conducted consistently by the CHW responsible for the designated territory. The process of territorialization is both a planning and management technique and a foundational element of family and community care in Brazil. Strategies and tools such as georeferencing and map creation support this process. 33 The e-SUS Território app’s map visualization feature is designed to promote the principles of territorialization in the day-to-day activities of PHC.
The cities leading in the number of app users are the capital cities of Brazilian states, characterized by their larger population sizes. This illustrates the app’s capability to serve the needs of major urban centers, which present additional layers of complexity in territorial organization. Furthermore, metropolises generally have more developed health service infrastructures, potentially offering better technological infrastructure and incentives for health teams to adopt technologies, such as the e-SUS Território app. Another significant aspect is the use of mobile applications beyond the health unit premises, facilitating the easy and timely recording of information. The contexts of remote populations are shaped by various distinct factors, such as geography, environment, politics, economy, history, culture, and society, all of which are deeply interconnected. These factors create a complex backdrop that influences practice development and access to health services. 34 Moreover, research has described challenges associated with smartphone use by CHWs, including lack of training and technical support. Additionally, barriers to adopting mobile solutions are apparent, including the unsustainable nature of pilot projects and the high investment costs. 32 Therefore, the success of the e-SUS APS strategy, which encompasses the PEC e-SUS APS electronic medical record and the e-SUS Território app, stands out for offering user technical support services and for the evolution of government tools developed over a decade.
This study has limitations related to the selection of data for analysis, as inclusion and exclusion criteria were not applied, nor was a calculation performed to define the sample. Usability data was extracted from ready-made Google Analytics dashboards, which may limit the analysis of the use of the e-SUS Território application. Another limitation of this study is the lack of comparative statistical calculations, such as t-tests to compare average usage between different regions and variance analyses.
Conclusion
The e-SUS Território application is an essential tool used by community health workers, contributing to their productivity, work process, and the management of care provided by the team. Adherence to the use of the application has been growing exponentially since its implementation, and its functionalities have been improved. The contributions of the CHWs in Brazil have been widely recognized in the literature, thereby highlighting the importance of national health policies and programs in promoting the performance of these professionals. These results highlight the support of mobile applications to community health workers, along with the importance of structuring policies and programs to promote the development of these technologies.
Footnotes
Acknowledgements
We would like to thank the members of the agile software development team responsible for the e-SUS Territótio application for assisting us with extracting data from Google Analytics and preparing the application’s screenshots.
Author contributions
I.C. Celuppi: conception and design; analysis and interpretation of data; article writing and relevant critical review of intellectual content; responsible for all aspects of the work in ensuring the accuracy and integrity of any part of the work; final approval of the version to be published. R.L.C. Prado: conception and design; analysis and interpretation of data; article writing and critical review of intellectual content; final approval of the version to be published. E.T.B. Mohr: analysis and interpretation of data; article writing and relevant critical review of intellectual content; final approval of the version to be published. F. Mioto: analysis and interpretation of data; article writing and relevant critical review of intellectual content; final approval of the version to be published. J.M.D. Oliveira: analysis and interpretation of data; article writing and relevant critical review of intellectual content; final approval of the version to be published. M. Felisberto: analysis and interpretation of data; article writing and relevant critical review of intellectual content; final approval of the version to be published. J.F. Hammes: analysis and interpretation of data; article writing and relevant critical review of intellectual content; final approval of the version to be published. R.S. Wazlawick: content review; responsible for all quality aspects of the manuscript and its compliance with the journal’s rules; as general coordinator of the e-SUS APS project, he is ultimately responsible for the integrity and accuracy of the information; final approval of the version to be published. E.M. Dalmarco: content advisor; article writing and relevant critical review of intellectual content; responsible for all aspects of the work in ensuring the accuracy and integrity of any part of the work; final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed, in part, by the Coordination for the Improvement of Higher Education Personnel (CAPES) – Financial Code 001 and by the Brazilian Ministry of Health, through the Decentralized Execution Term (MS/UFSC). RSW and EMD are productivity fellows in technological development and innovative extension from the National Council for Scientific and Technological Development (CNPq).