
Abstract
Objectives: The patient safety culture includes a systematic approach that promotes safe care for patients and the leadership that supports it. Medical errors threaten patient safety. A significant portion of medical errors is committed by nurses. Although error-reporting provides valuable information to prevent errors, most nurses do not report their errors due to their high level of stress. This study was to investigate the effect of electronic error-reporting forms on nurses’ stress and the rate of error-reporting. Methods: The nurses’ level of stress was compared when using paper error-reporting and 6 months after using electronic forms. A revised version of the Coudron questionnaire was completed by 186 nurses. Data were analyzed by SPSS 23 using Wilcoxon test. The number of reported errors in paper and electronic media was compared over the same period. Results: Implementation of the electronic error-reporting form reduced the job stress of nurses by 22.22 points (p=.00) and increased the error-reporting rate by 12.86% (p<.05). Conclusions: Although nurse’s stress significantly decreases after implementing electronic error-reporting forms, their level of stress is still high and they are still at risk for physical and mental problems. Using methods like modifying the error-reporting form will increase the error-reporting rate.
Introduction
Patients can be harmed while receiving care. Patient harm during care is a leading cause of morbidity and mortality internationally.1,2 Patient safety culture as the first dimension of quality improvement, reduces the risk of patient harm. 3 Patient safety means that a patient does not suffer any unnecessary harm, nor is exposed to any potential harm related to healthcare. 4 The patient safety culture includes risk assessment, preventive and corrective measures, and ongoing development of activities. 5 According to studies, Empowering nurses and supervisors, 6 developing skills in communication, leadership, and teamwork, 7 health policies and their annual assessments, and Staff Well-Being 8 will improve patient safety culture. One of the factors that threaten patient safety is medical errors.9,10 Medical errors are the third leading cause of death in the United States, 11 and annually 44,000–98,000 Americans die as a result of preventable medical errors. 12 Health care errors affect one patient in every 10 patients, 13 while many of them are preventable. 14 Nurses are one of the biggest human resources in the health sector. 15 A significant portion of medical errors occurs by the nursing staff while providing care services. 16 In the United States, 2000 deaths in 10,000 patients have occurred due to nursing errors. Nursing errors may lead to irreversible consequences, increase mortality, and raise the cost of treatment. 17 Due to lack of an official source for reporting medical errors in Iran, no accurate data exist on the errors occurring, but according to the Ministry of Health, annually several billion Dollars are spent on additional hospital fees due to medical errors. 18
Some countries use CPOE (Computerized Physician Order Entry), 19 EHR (Electronic Health Record), 20 RFID (Radio Frequency Identification), 21 CDSS (Clinical Decision Support System), 19 and HIS (Hospital Information Systems)21–23 to reduce medical errors. Because of the importance of medical errors, the IOM (Institute Of Medicine) has proposed solutions to reduce the amount of these errors, including the development of a medical error-reporting system and encouraging individuals to report errors voluntarily. 24 Reporting errors provide valuable information that helps prevent future errors and correct and mitigate errors to enhance patient safety.24–26 Also, by encouraging individuals to report errors, the frequency of error-reporting can be increased. 25
A study in Australia showed that although 98.3% of the medical and nursing staff knew the error-reporting system, most of them declared that lack of proper feedback is the greatest impediment to reporting errors. 27 In Iran, nurses are required to report medication errors honestly, 28 but they do not report most of the medical errors.29,30 The reasons for under-reporting include personal factors such as fear of losing honor and dignity; poor knowledge, skill, accountability, and commitment; and organizational factors such as inappropriate reactions of managers, doctors, and colleagues; retribution from patients’ families and administrators25,31; and fear of legal responsibility, losing the job, reduced salaries and benefits.29,32–35 Nurses feel stressed when reporting their own mistakes. The stress due to reporting error-reporting is an exacerbating factor. Error-reporting initiatives such as anonymous reporting systems can be used to prevent under-reporting.31,35 Many hospitals began to implement anonymous electronic error-reporting forms. However, it’s unclear if the anonymous electronic form would increase the nurses’ error-reporting rate and reduce their stress. Studies36,37 have been carried out on error-reporting in the medical field, but so far no study has examined the effect of electronic error-reporting forms on the error-reporting rate and the stress level of individuals. The objective of this study was to examine the effect of electronic error-reporting forms on decreasing nurses’ stress and increasing their error-reporting rate.
Methods
Study design
This research was a pre and post-intervention study that measured the effect of electronic error-reporting forms on nurses’ stress and the rate of error-reporting during the 6 months before and 6 months after implementing electronic error-reporting forms. This study was performed on nurses at one of the teaching hospitals affiliated with Kerman University of Medical Sciences (KUMS). In this setting, nurses have a bachelor’s or master’s degree in nursing. The employment status of nurses is permanent employment, fixed term contract, or freelance contract. Nurses are present in the hospital in three shifts, morning (6 h), evening (6 h) and night (12 h). To hand the shift over, the nurses of the next shift take the shift and visit the patients and check their medical records half an hour before the end of the previous shift. Nurses’ work is monitored by supervisors and the quality improvement unit of hospitals. One of the methods to monitor the nurses’ work, identify their errors, and correct and mitigate errors to enhance patient safety is implementing an error-reporting form. To improve the skill level of nurses and correct their errors, the quality improvement unit examines the reported errors and provides the necessary training courses for nurses.
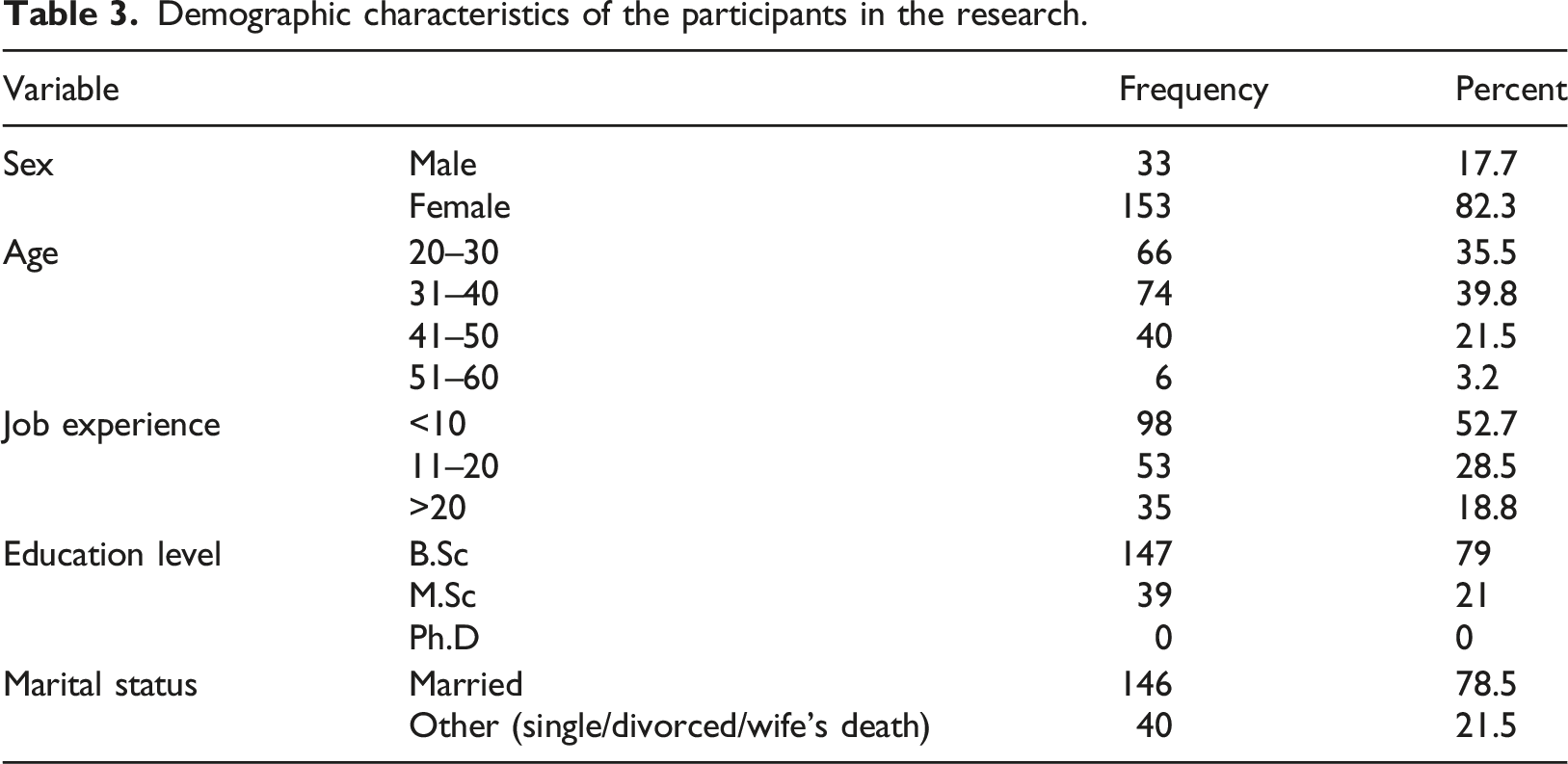
Out of 357 nurses, working in the study setting, a sample of 186 nurses was calculated using Cochran’s formula and participated in the study. Due to the non-identical distribution of nurses in the hospital departments, the research population was divided into clinical and para-clinical sections using stratified sampling. Subsequently, according to the number of nurses working in each stratum, the samples of nurses from each stratum were determined by simple random sampling. The selected nurses were asked to express their informed consent to participate in the study verbally.
System and setting
In order to motivate nurses to report errors, supervisors of hospital departments explain the advantage of the reporting errors and then asked the nurses report their errors to correct and reduce errors and increase patient safety.
Before this study, a paper form in Persian was used to report nursing errors in the setting. Above this form, it was said that it is not necessary to report the name. Although this form was filled out anonymously, there was a possibility of identifying the offender from the completion of the form to the delivery to the quality improvement unit of the hospital. This paper form has been available in the required number in all departments of the hospital and was collected monthly and delivered to the quality improvement office of the hospital by supervisors of hospital departments. In this study an electronic error-reporting form was developed and placed on the hospital website after confirmation by the hospital manager and the quality improvement unit. It was also announced through a letter to all head nurses that the errors should be reported electronically. Thus, nurses could report the errors in full detail and anonymously whenever they want, through any devices and without the stress of being identified. A computer expert through the hospital website delivers monthly the reported errors to the quality improvement office.
Data collection
To collect the reported errors, the errors of 6 months before and after the implementing electronic error-reporting forms were received from the quality improvement office.
To collect the data on nurses’ stress, the modified version of the Persian questionnaire of Coudron stress 38 was used (Additional file 1). This questionnaire contains four tests and evaluates the stress in different fields. The first test examines the job as the source of stress, the second test examines the health of life, the third test examines personal life, and the fourth test examines the personality and the individual’s habits.
A number of questions from each of the tests were selected by one of the psychiatrists of the hospital according to the research objectives and some of them were edited. This psychiatrist had 10 years of experience working in the hospital and was very familiar with the nurses and their working conditions.
The questionnaire consisted of three sections. (1) Demographic information of participants, including age, work experience, sex, education degree, marital status, and type of employment (six questions). In this section, except for two open-ended questions, the other questions were multiple-choice. (2) Open questions were related to the number of errors made, the number of unreported errors, and the reasons for not reporting the error (two questions). (3) Questions to evaluate the stress in different fields. This section includes questions about the job as the source of stress (32 questions), the health of life (6 questions), personal life (13 questions), personality, and the individual’s habits (13 questions). All questions in this section were dichotomous.
Three psychiatrists confirmed the content validity of the questionnaire. Its reliability was also evaluated by calculating Cronbach’s alpha through SPSS 23. For this purpose, based on the internal coordination of the items and calculating the alpha coefficient, the items were provided to 30 random samples of nurses. To prevent errors, these 30 nurses did not participate in the final study. Cronbach’s alpha was 0.81; therefore, the reliability of the questionnaire was confirmed.
A paper questionnaire was used to collect data. The questionnaire was distributed by one of the researchers among 186 nurses 6 months before and 6 months after the implementation of the electronic error-reporting form.
Data analysis
To check the error-reporting rate, the number of errors reported in paper form within 6 months before the implementation of electronic error-reporting forms and the number of errors reported electronically within 6 months after implementing electronic error-reporting forms were compared.
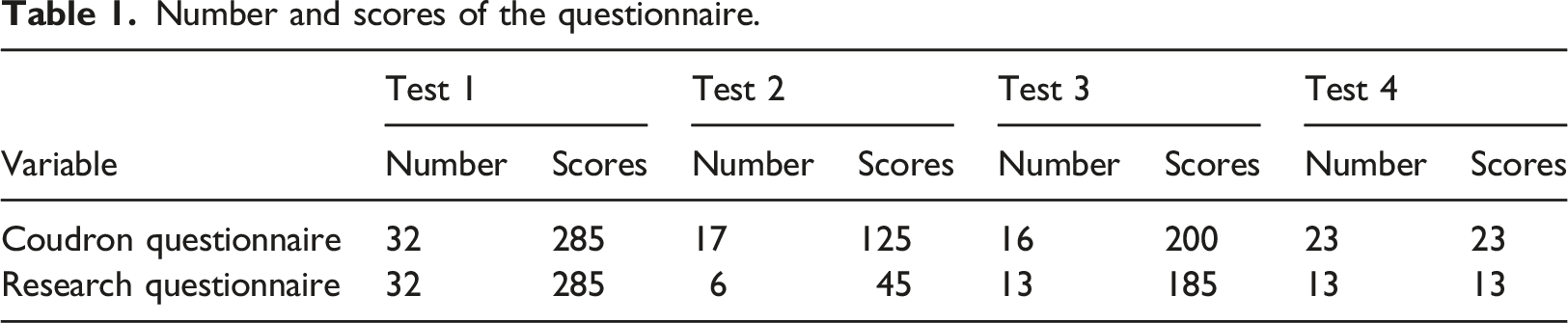
To examine the effect of electronic error-reporting forms on decreasing nurses’ stress, a score of 0–40 was assigned to each question of this questionnaire. Based on the answers given to the questions in each test of the questionnaire four distinctive total scores were calculated for each nurse. The four total test scores of each nurse before and after implementing the electronic error-reporting form were analyzed by SPSS 23.
Number and scores of the questionnaire.
Interpretation of the tests
Test 1: Self-assessment of job stress
According to the calculations performed to obtain the expected range for the interpretation of the job stress, a score ranging from 0 to 30, indicates natural stress that stimulates a nurse to be active, and grow his/her abilities without being aggressive at the same time. A score from 31 to 60 shows that the nurse is struggling with job stress that makes his/her life unbalanced, and threatens physical and mental health. A score higher than 60 means that the person is having very intense job stress.
Test 2: Self-assessment of life health
According to the calculations, if the person’s score on the second test ranges from 0 to 10, it means that the person has a healthy life. If the score is between 11 and 20, it indicates that the person cannot control the stress. A score higher than 20, shows that this type of life health has prepared the person for any kind of discomfort.
Test 3: Self-assessment of personal life
According to the calculations, if the person’s score in the third test ranges from 0 to 15, it means that the individual’s personal life is not difficult. If the score is between 16 and 35, it indicates that the person is not satisfied with his/her personal life. A score higher than 35, reveals that the person’s life is stressful and it is likely to get worse soon.
Test 4: Self-assessment of personality and Intellectual habits
According to the calculations, if the score of a person on the fourth test is between 0 and 3, it means that the person’s personality and intellectual habits have no problem. A score higher than three indicates that the person’s personality is the source of stress and does not allow the events to be realistic.
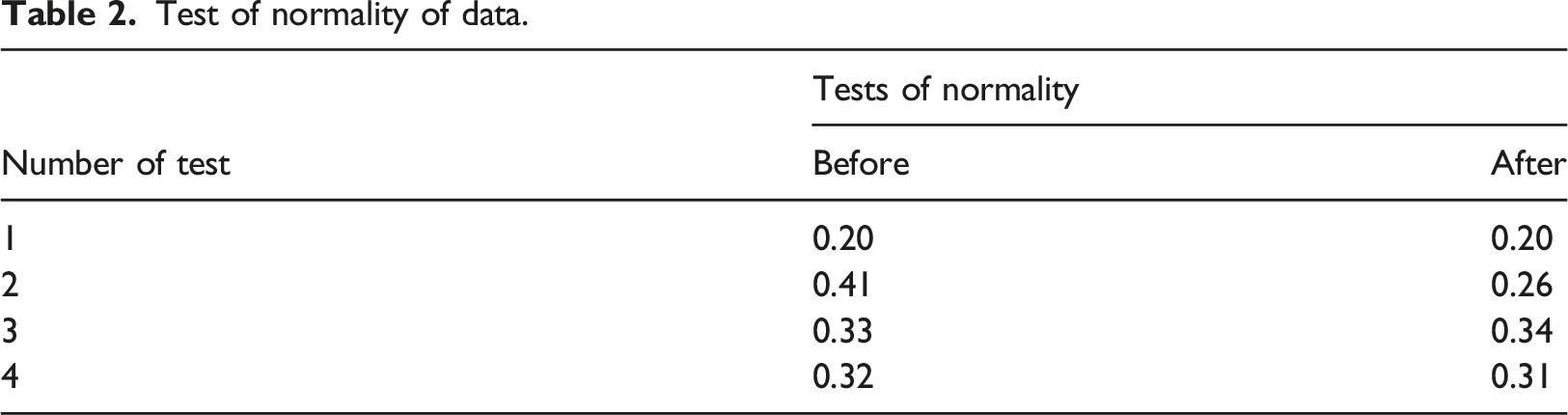
Test of normality of data.
Results
Test results
Demographic characteristics of the participants in the research.
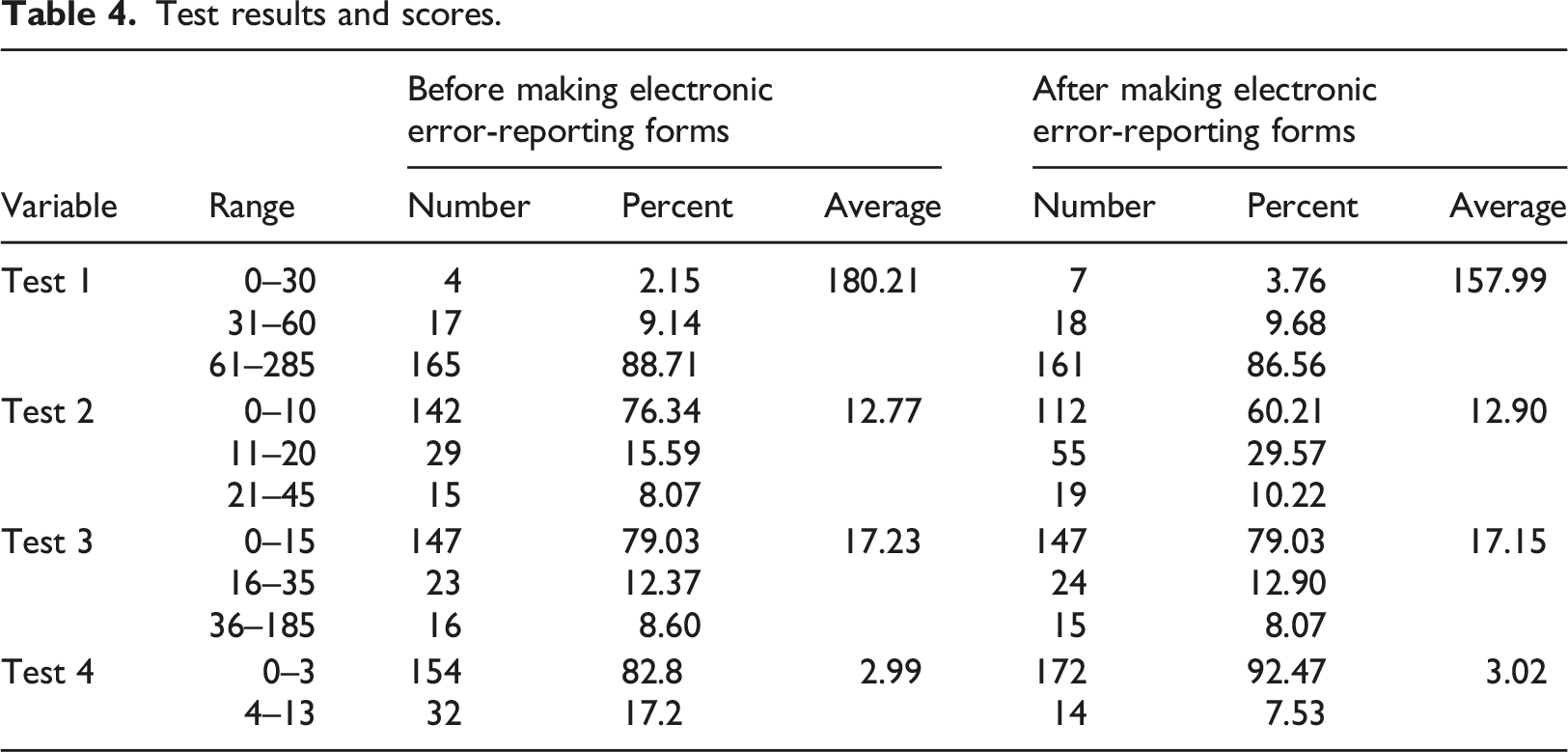
As shown in Table 4, the results of nurses’ stress before and after implementing electronic error-reporting forms are as follows:
Test 1: Self-assessment of job stress
This test examines the stress of an individual’s job. The mean score of nurses’ job stress before making electronic error-reporting forms was 180. It significantly decreased to 158 after making electronic forms (p = .00, z before = 0.88, z after = 0.89).
Test 2: Self-assessment of life health
This test examines the stress associated with the health of a person’s life. The mean score of nurses’ stress concerning life health before implementing electronic error-reporting forms was about 13, which did not significantly differ from the mean score after implementing electronic forms (p = .61, zbefore = 0.65, zafter = 0.83).
Test 3: Self-assessment of personal Life
This test examines the stress of nurses in their personal lives. The score of nurses’ stress in their personal life before implementing electronic error-reporting forms was about 17 and had no significant difference from the mean score after the implementation of electronic reporting forms.(p = .79, zbefore = 0.61, zafter = 0.60).
Test 4: Self-assessment of personality and Intellectual habits
Test results and scores.
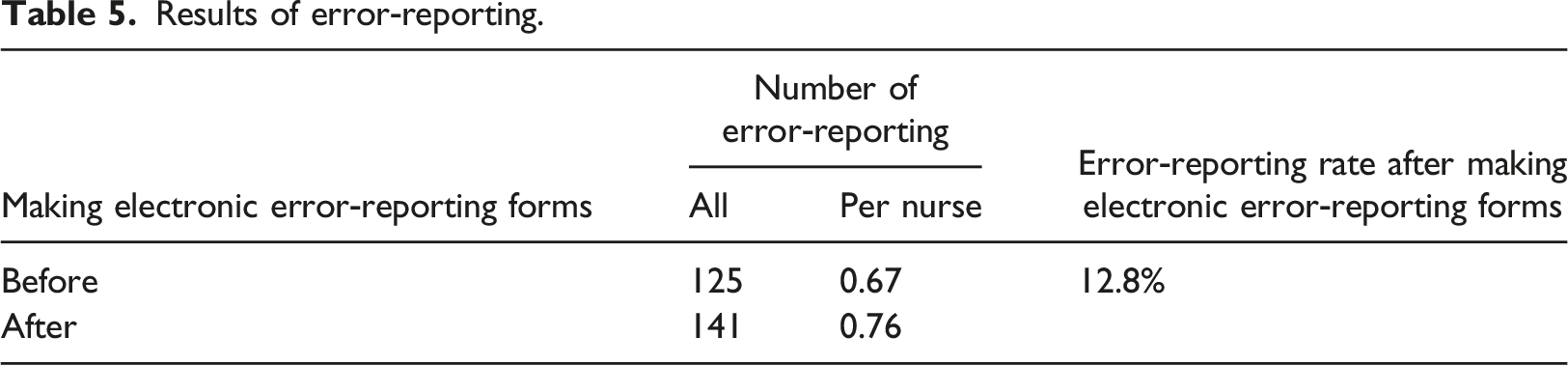
Results of error-reporting rate
Results of error‑reporting.
Discussions
In this research, the same paper-based error-reporting form was designed in electronic form. The implementation of the electronic error-reporting form significantly increased the error-reporting rate by nurses. The results of nursing stress assessment in four phases of job stress, life health, personal life, personality, and intellectual habits indicate that a high percentage of nurses suffered from job stress before making electronic error-reporting forms. This stress increased the possibility of making errors. After making electronic error-reporting forms, the stress level of nurses decreased, significantly.
Studies29,31,33 have shown that fear of legal responsibility and honor; poor knowledge, job awareness, skill, accountability, and commitment; the unfavorable response of managers, doctors, and associates; loss of jobs; and reducing salaries and benefits prevents error-reporting. The results of this research confirmed the results of previous studies.
The implementation of electronic error-reporting forms provides nurses with an opportunity to report errors freely and without stress. 30 Because in the conventional way of reporting with a paper form, there was a possibility of identifying the offender from the completion of the form to the delivery to the quality improvement unit of the hospital, and the nurses did not usually report their errors due to fear of the loss of honor, legal responsibility, etc.29,32–35 However, in this study, by implementing an electronic error-reporting form and placing it on the hospital website, it’s not possible to identify nurses in any way, and the identity of the nurse will remain completely confidential. In addition, nurses can access the form in any location from the hospital website, and they can calmly report their errors in full detail whenever they are free from work and without the stress of being identified.
The results also indicate an increase of 12.86% in error-reporting after implementing electronic error-reporting forms because, in addition to the confidentiality of the identity of the individual, nurses can access the form at any time from any location for reporting errors. This result confirms the findings of a previous study 30 which showed that creating an error-reporting system increases the error-reporting rate. Error-reporting provides valuable information to prevent future errors, supports correction and reducing errors, and thereby improves patient safety. These results are in line with the results of studies39–41 that revealed increasing error-reporting improves patient safety.
Reducing the stress of nurses is important because they constitute a major part of the human resources of the healthcare system and perform most of the patient care. 15 Stress poses a threat to their physical and mental health and social function, and results in exacerbating errors. This study showed that the stress level of nurses after implementing electronic error-reporting forms decreased by 22.22 scores, but this level of stress is still high. Therefore, they are expected to remain at risk for physical and mental problems. Reducing the job stress level of nurses associated with their physical and mental health reduces their error rate, leads to a reduction in the patient’s mortality rate and the cost of treatment, and thus enhances patient safety. This result confirms the results of another study that showed reducing the nurses’ stress increases patient safety. 42
The results showed no significant difference in the life health, personal life, personality and intellectual habits of nurses before and after implementing electronic error-reporting forms, thus reduction in job stress happened only due to the change in the method of error reporting.
This study had three limitations. First, was the low response rate of nurses to the questionnaire, due to their very busy work status. This limitation was resolved by making several flexible appointments. Second, nurses were concerned about the disclosure of their identities. To deal with this concern, they were assured that their data will be analyzed cumulatively and the confidentiality of their data will be maintained. Third, the results of the study might be influenced by external variables that affect nursing stress levels and nursing error reporting. To prevent the influence of these variables, the period of data collection was shortened and the effect of these variables on the results was controlled.
This research revealed that the implementation of electronic error-reporting forms increases the rate of error-reporting by nurses and reduces their job stress. The reduction of nurses’ stress merely resulted from using electronic error-reporting forms and did not influence by factors such as life health, personal life and personality and intellectual habits. The nurses in this study had years of work experience with electronic systems like HIS and had at least a bachelor’s degree or higher. Therefore, they had no problem working with the electronic error-reporting forms. Although the organizational structure and culture are similar in all teaching hospitals in Iran, these results may not be generalizable to communities with lower levels of education or work experience with information systems.
Conclusions
The findings of this research showed that the stress level of nurses decreased significantly by implementing electronic error-reporting forms. However, their stress level is still high, and action should be taken to reduce it. Therefore, management, supervisors, and experts in the quality improvement unit of the hospital are recommended to reduce medical staff job stress and improve their physical and mental health by using a suitable reporting method. Additionally, using methods such as functional changes in questions of error-reporting form will increase the error-reporting rate. All these factors can increase the physical and mental health of nurses, reduce their errors, increase the rate of reporting and thereby improve patient safety.
In this research, an identical set of questions was used in the paper and electronic error-reporting forms. It is recommended that the researchers interested in this issue investigate the impact of changing the questions of the error-reporting form on the stress level of nurses and the impact of electronic error-reporting forms on the stress level of other medical staff.
Footnotes
Acknowledgements
The authors thank the management, educational and clinical supervisors, computer center staff, quality improvement unit staff and nurses of Shafa hospital who have been fully involved in this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.