
Abstract
Since the COVID-19 pandemic, the use of mobile health apps has been increasing significantly. Many have started using mobile health apps to manage their health and well-being. People need to develop healthy habits that will increase their job productivity, life expectancy and improve their social relationships. This study tests the Health Belief Model with adults in China in influencing health motivation and in turn improving their health behavior. A mobile and online survey was developed, and 120 usable responses were collected. A structural equation modeling was used to test the relationships between perceived benefits, perceived susceptibility, perceived barriers, health motivation, and health behavior. We found perceived self-efficacy, perceived benefits, and perceived susceptibility predicts health motivation, and health motivation predicts health behavior. We did not find that perceived barrier is a predictor for health motivation. We conclude that to encourage behavioral change, it is important to enhance self-efficacy and address the benefits; in the meantime, educating people on susceptibility is also important.
Introduction
The mobile app market grew 65.7% compared to pre-Covid (Fortune Business Insight 2020). 1 China's revenue in the Digital Health market is projected to reach US$46.00bn in 2022 with an annual growth rate of 12.98% till 2027. IQVIA reports that over 90,000 digital health apps were marketed last year, with an average of 250 apps per day (2021). Health mobile apps play an important role in health promotion and motivation. Harvard Medical Publishing (2015) 2 claims that downloadable smartphone apps can coach people to check and improve their health. Current evidence shows that individuals and families practicing self-management behaviors improve their health outcomes. 3 Mobile health apps can be used to educate patients, and the public about health and even serve as interventions for disease treatment and recovery. Increase in demand for healthcare services during covid, inability of people to visit health care facilities due to social distancing measures, different regions within China having different COVID-19 policies highlighting the need for communication, increased awareness of maintaining good general health have all heightened the need to study mobile health apps adoption in China. It was interesting to find that the apps were mostly used for “accessing information on COVID-19.” Chinese respondents overwhelmingly identified “information” as the most valuable feature of COVID-19 apps. 4 In addition, it is believed that the pandemic has accelerated the adoption of health apps in China 7 and this trend may continue thus having a significant long-term impact. That is evidence that mHealth apps are an effective health care approach gaining in popularity among the Chinese population following the COVID-19 outbreak. 5 The next step after recognizing the importance mobile applications is to explore the factors that initiates or improves adoption of mobile apps in China using established theoretical models. Such an understanding can not only improve the adoption of mobile apps by suggesting ways to improve both usage and adoption.
Theory-guided research is needed to understand health beliefs and attitudes toward technological interventions such as mobile health apps. The Health Belief Model (HBM) is widely accepted and used in explaining people's health beliefs and behaviors. It has been tested extensively in different countries and cultures. 6 The classic Health Belief Model contains six constructs perceived seriousness, perceived threat, perceived susceptibility, health motivation, cue to action, and the likelihood of behavior change. Over the years, many researchers have modified the health belief model by adding moderators and mediators. 7
The Pandemic has affected every people’s lives in unprecedented ways. Many people's health behaviors have changed. According to Statistica, China is ranked second in the mobile health app user share globally. 8 The COVID-19 pandemic pushed patients and providers to adopt digital health tools as care moved outside the doctor's office. Despite the pandemic triggering an explosion of new digital health apps, its user acceptance is still an area for further investigation.
It's projected that the mobile platform will deliver more health services. A study compares age differences in users' adoption of mobile health services in China and finds that perceived value, attitude, perceived behavior control, and resistance to change predict the intention to use mobile health services for the middle-aged group. Compared to old users, perceived value, attitude, perceived behavior control, technology anxiety, and self-actualization need positively affected the behavior intention of older users. 9 Though the limited studies in China on mobile apps provide some useful results, in general, studies on mobile health apps in China are limited. 10 More studies are needed to further validate HBM in China contexts and people's beliefs and behavior change over time.
The aims of this study are to (1) apply the health belief model to mobile health apps in China context, (2) examine important predictors of health behavior, and (3) discuss implications. We intend to explore the users' adoption of mobile health apps and their attitudes toward mobile health apps, health beliefs, and health behavior. The remainder of this paper is organized as follows. We first provide an overview of mobile health apps and conduct a literature review on the health belief model. The Methods section describes instrument development, translations, and implementation. The analysis section explains analysis methods and model testing. The final two sections report the results of our analysis and a discussion of our findings.
Health belief model
Mobile health apps
Mobile health has a promising future in the healthcare system in patient education, treatment access, and recovery support. Harvard Medical Publishing (2015) 2 claims that downloadable smartphone apps can coach people to check and improve their health . Mobile messaging is a feasible addition to church-based programs to improve dietary and physical activity behaviors. 7 Medical professionals often find it challenging to alter patients’ habits 11 for a variety of reasons. As an example, physicians do not want to engage in a weight-loss conversation for fear of damaging patient-physician relationships. Patients' self-awareness, self-education, self-regulation, and self-motivation are the starting points for better health.
Research shows that counselling services with frequent contact with patients provided by healthcare professionals can make patients change their health-related behavior and lifestyle. 12 Chisholm et al. 11 suggest that the barriers to behavioral change are context factors, motivational stance, and awareness of the need to change. Mobile health apps can provide counselling and frequent contact at the most convenient time and location. Whenever a patient is available, they can use health apps to self-manage their health-related needs.
China has made significant investments in its mobile technology infrastructure in the past decade. Mobile health apps hold the promise of patient education, disease prevention, disease management, and improved communication with providers. In general, mobile health app users in China are younger, better educated, and living in urban areas. 13 A descriptive study of China's mobile health market concludes that clinician-facing apps feature education and peer-reviewed papers. In contrast, consumer-facing apps contain features like scheduling appointments, exercise, diet, or disease-specific apps. 14
The use of mobile health apps could improve patient experience, such as accessing health information, making physician-patient communication more convenient, ensuring transparency in medical charges, and ameliorating short-term outcomes. 13 A recent study on ankylosing spondylitis health apps finds that most apps lacked comprehensive functions for ankylosing spondylitis management. This calls for the room for improvement for disease-specific apps. A fully-functional and patient-centered apps need concerted effort among healthcare providers, patients, and app developers to develop high-quality, evidence-based apps. 15
Health belief theory
Health belief theory states that individuals' beliefs determine health behavior about disease and strategies available to decrease its occurrence. 16 It postulates that an individual's likelihood of engaging in a health-related behavior is determined by his/her perception of perceived susceptibility, perceived severity, perceived benefits and risks, and cues to action. 17 Later, variables from Social Determination Theory (e.g. motivation) 18 and Social Cognitive Theory (self-efficacy) were added to HBM to increase the predictive power of HBM. 19 The Health Belief Model (HBM) is one of the most popular models used to prevent diseases with social, psychological, and behavioral underpinnings. HBM is the most widely used model explaining health beliefs and behavior validated in many cultures and contexts.20–22
Health Belief Model has a great impact on health education, designing both long and short-term health behavior interventions and health promotion.23,24 Although this model is useful in general, prior findings report the model only explains 20% of variances in behavior change. 25 Recently, a systematic review of COVID-19-related preventive behavior shows a 25% predictive validity, and the explained variance for HBM ranged from 6.5% to 90.1% from the global studies of HBM. 20 However, studies have used a varied number of HBM constructs. Some did not include perceived benefits, whereas others did not incorporate self-efficacy into their model. In general, perceived benefits and self-efficacy are the two most frequently used constructs in all HBM studies. 20
In our study, we intend to survey adults' attitudes and perceptions towards mobile health apps, we deem perceived barriers, perceived benefits, perceived susceptibility, and self-efficacy are important predictors to motivate individuals to engage in healthy behaviors. We did not include perceived severity in our model as prior studies show no significant difference was observed between the two groups regarding perceived severity. 6 Harrison et al. 26 suggested severity might not vary as much as some of the other variables because few people consider outcomes like breast cancer as anything other than extremely severe. 27
Figure 1 shows the constructs and relationship between constructs in the Health Belief Model. Research model.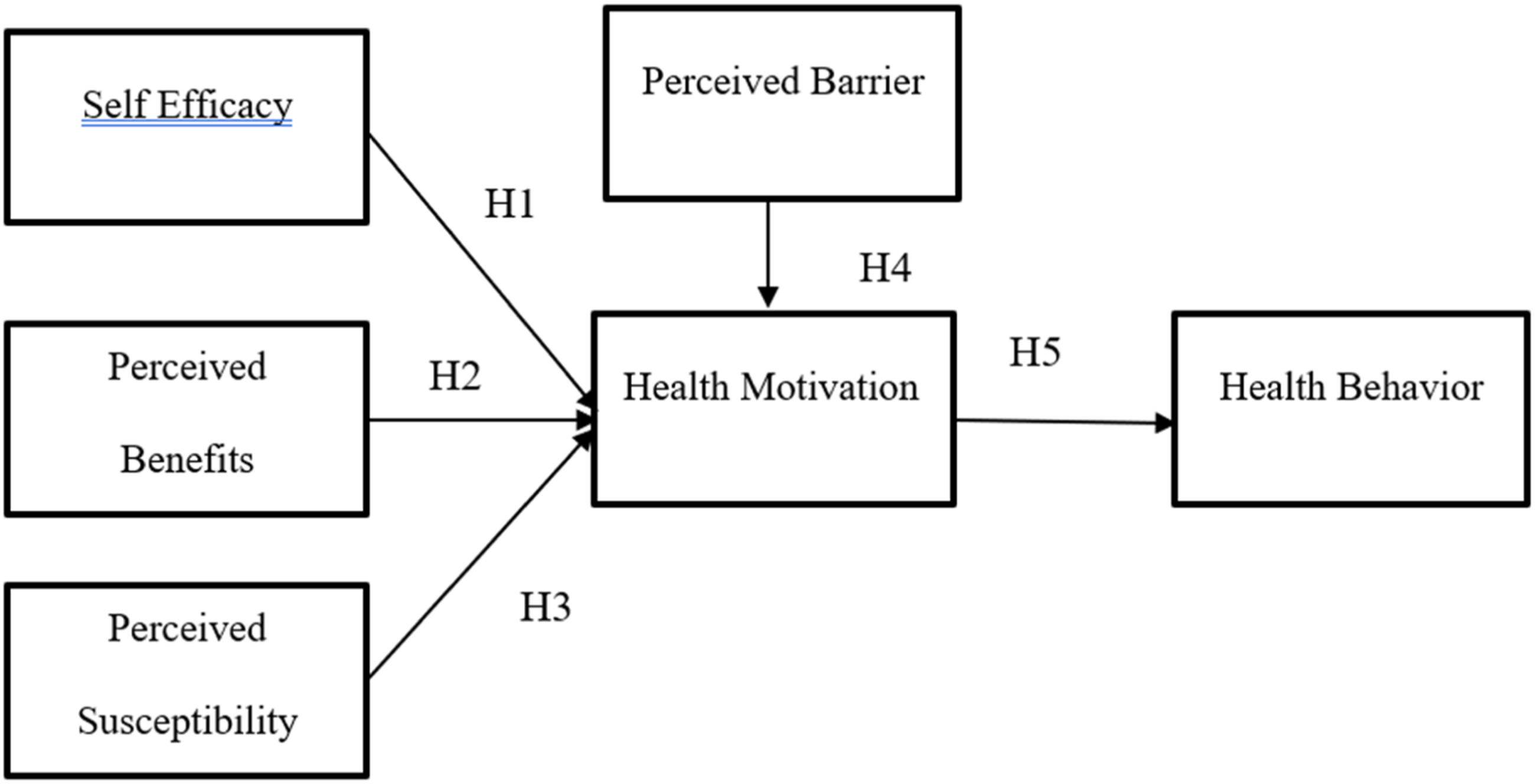
Research model
Self-efficacy refers to the belief that a person can control challenging environmental demands by taking adaptive action. 28 It is perceived to be domain specific. In the past, many self-efficacy scales have been developed, for example, computer self-efficacy 29 breast cancer self-efficacy, 30 and generalized self-efficacy scale.31,32 revealed that self-efficacy was the most important predictor in the HBM constructs to predict breast self-examination behavior in female students. In a quasi-experimental study of mobile health app intervention on women's health beliefs on breast self-examination, self-efficacy, and health motivation were significantly higher in the intervention group compared to the control group. 6 The relationship between self-efficacy and motivation has also been established in the literature. For example, a recent study on a university gym evaluation program explores how perceived changes in health and motivation are related to changes in self-efficacy by age. 33 Motivation could be intrinsic and extrinsic. Intrinsic motivation refers to "people's spontaneous tendencies to be curious and interested, to seek out challenges and to exercise and develop their skills and knowledge, even in the absence of operationally separable rewards". 18 Drawing from studies on computer usage, researchers have theorized that higher self-efficacy leads to easier use and lower resistance to adoption. 34 Although intuitively it appears that such a theorization is plausible, results from other mobile app studies are conflicting. Alharbi et al. 35 found a strong support perceived benefits and self-efficacy to be the strong predictors of mobile health applications. However, Vancouver et al., 36 describe other studies where the evidence is conflicting. To further test the role of self-efficacy we posit
H1: Self-efficacy is positively associated with health motivation. Perceived benefits refer to individuals' opinions or values of a new behavior’s benefits.
37
Perceived benefits play an important role in adopting preventive behaviors.
27
Graham
38
found that women who perceived the benefits of breast self-examination had higher odds of performing the screening than those who did not. Interventions based on perceived benefits are recommended to increase women's regular breast cancer screening.
32
People who perceive the benefits are more motivated to engage in certain health behavior. While there are some studies that support the influence of perceived benefits on motivating behavioral change,
39
there is some doubt cast by others whether the motivation will lead to lasting change in behavior Borland et al., 2010).
40
To test this relationship further, we include perceived benefits in the model and posit that
H2: Perceived benefits are positively associated with health motivation. Perceived susceptibility/risk refers to the likelihood of an individual developing a health condition. People will be more motivated to seek healthy behavior if they believe they are at risk for developing a specific negative health outcome.
41
Usually, the higher the perceived risk is, the higher the likelihood of an individual engaging in behavioral changes to reduce the risk. Increased belief in risks will motivate people to take action.
42
For example, Mullens et al.
43
report behavior changes in colon cancer survivors. We therefore posit:
H3: Perceived susceptibility is positively associated with health motivation. Perceived barriers mean the obstacles an individual perceives to adopting a new behavior. It is the most significant
44
and strong predictor
45
in behavior change. When individuals feel the barriers are high, they are less motivated to participate in behavior-change activities. We therefore posit:
H4: Perceived barriers are negatively associated with health motivation. Motivation is the general desire to do something. Motivation is driven by our needs, and affects how we think, feel, and act. Each of us is unique in our needs, wants, and desires which drive us to achieve better health, and well-being, live a purposeful life, or grow professionally. Becker
46
proposed that overall motivation to pursue healthy behavior should be included in HBM. Motivation helps us understand human nature as it explains why we set goals, strive for achievement and power, and why experience emotions like fear, anger, and compassion. Health motivation is important in changing behavior, as numerous studies show intention and motivation drive behavior.
47
H5: Health motivations are positively associated with health behaviors.
Research methods
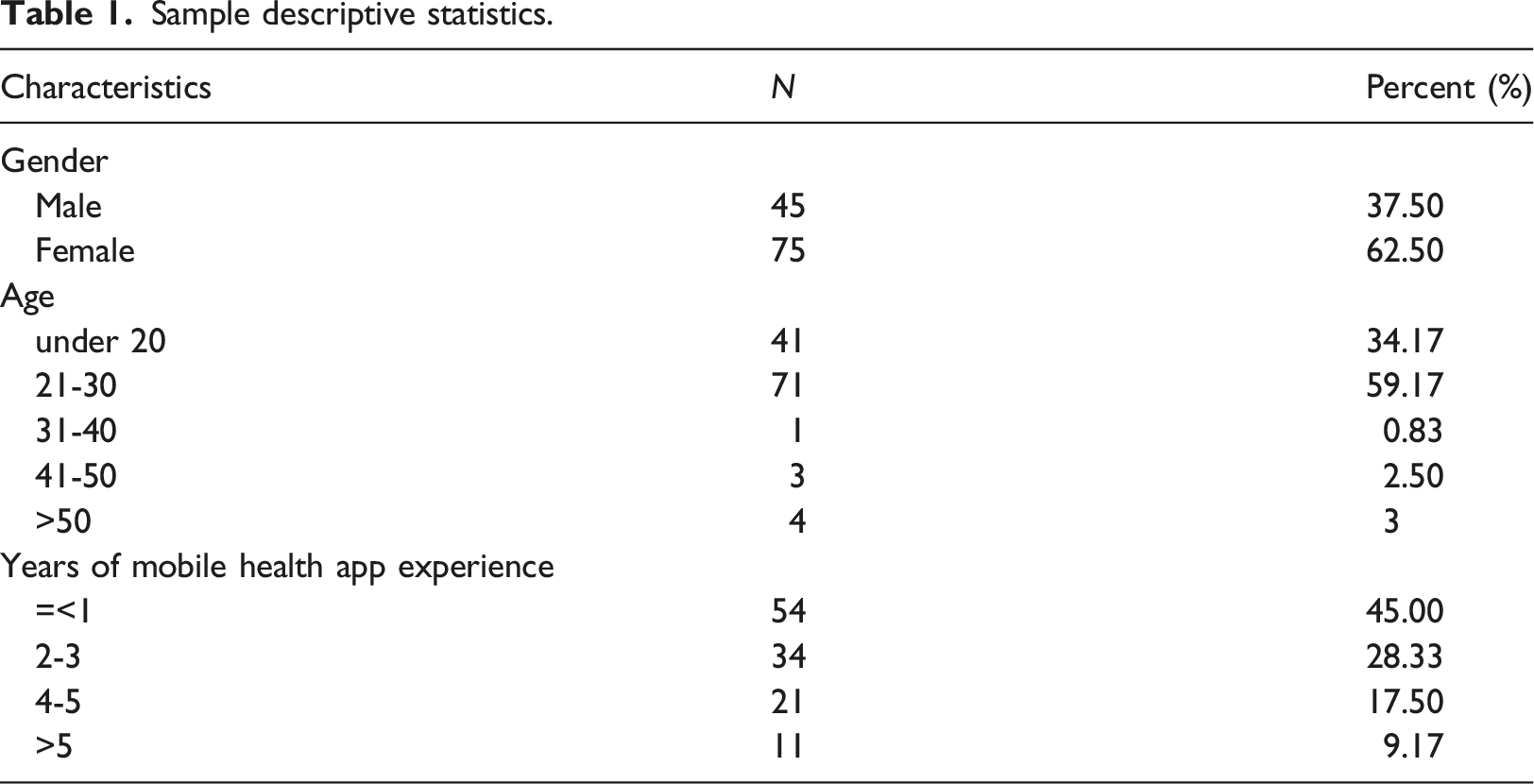
The authors’ Institutional Review Board approved this study. To examine the relationships among constructs in the Health Belief Model, we used a survey method. Data were collected in a fitness club near a university in Hangzhou, China. Most of the club members are young adults. We recruited five college students to collect data for us. The five students went to the fitness club asking for consent for participation in this survey. Two survey delivery methods were used to provide convenience to the study participants: a mobile survey and an online survey. The same survey was used in both the delivery methods. Once the consent was obtained, a bar code containing a link to the survey was texted to WeChat on their mobile phone and emailed to the study participants. The data collection lasted about 2 months between Oct. 1.2021 – Nov. 30, 2021. A total of 122 surveys were collected, 120 were usable surveys.
Measures
All measures were adapted from existing literature. The self-Efficacy scale was adapted and based on the theoretical perspectives proposed by Bandura. 28 Perceived benefits, perceived seriousness, perceived susceptibility, health motivation, and barriers were adapted from. 48 For health behavior, we use three items eating, exercise, and body weight index, to measure behaviors.
An English version of health belief model questions specifically targeting mobile health apps was developed. Questions were measured on a seven-point Likert scale (with one indicating strongly agree and seven indicating strongly disagree). The questionnaire contains four questions related to susceptibility, four about seriousness, six about benefits, seven about barriers, three about self-efficacy, three about health behavior, and six about health motivation. Low scores indicated high levels of perceived dimensions. Two researchers translated the English version into the Chinese version. A back translation was also conducted 49 from Chinese to English to ensure equivalency and reliability between the English and Chinese versions. Participants then completed a Chinese version of the HBM questionnaire. Appendix 1 contains our survey.
Results
Descriptive statistics
Sample descriptive statistics.
Analysis
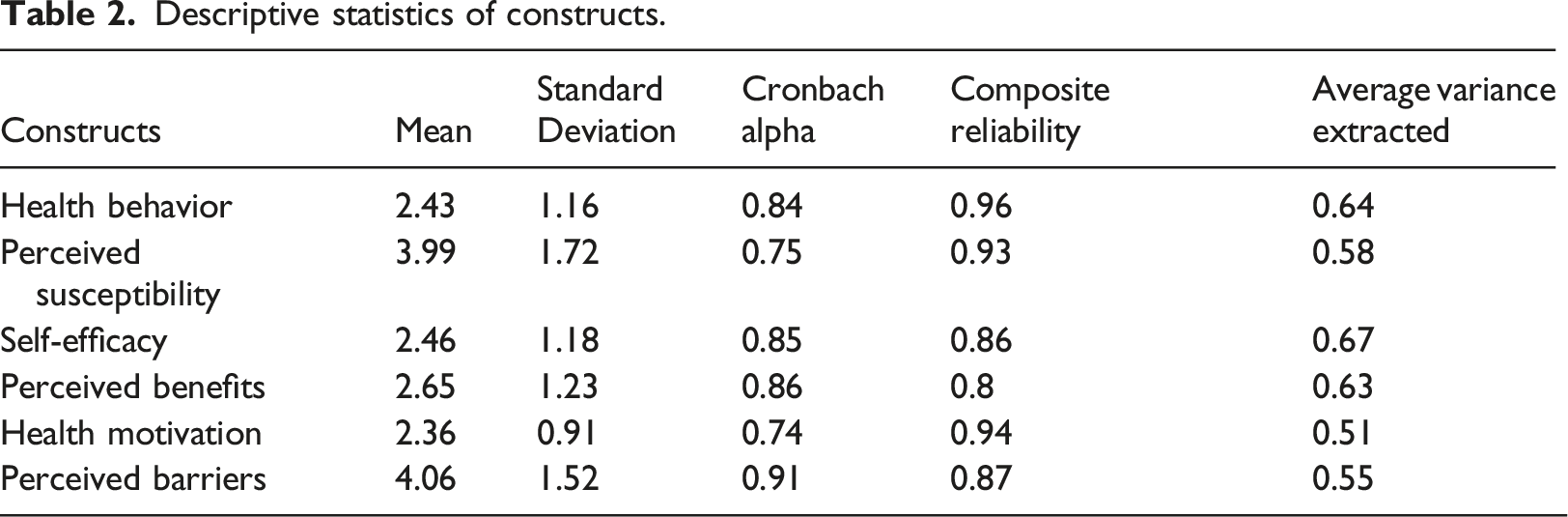
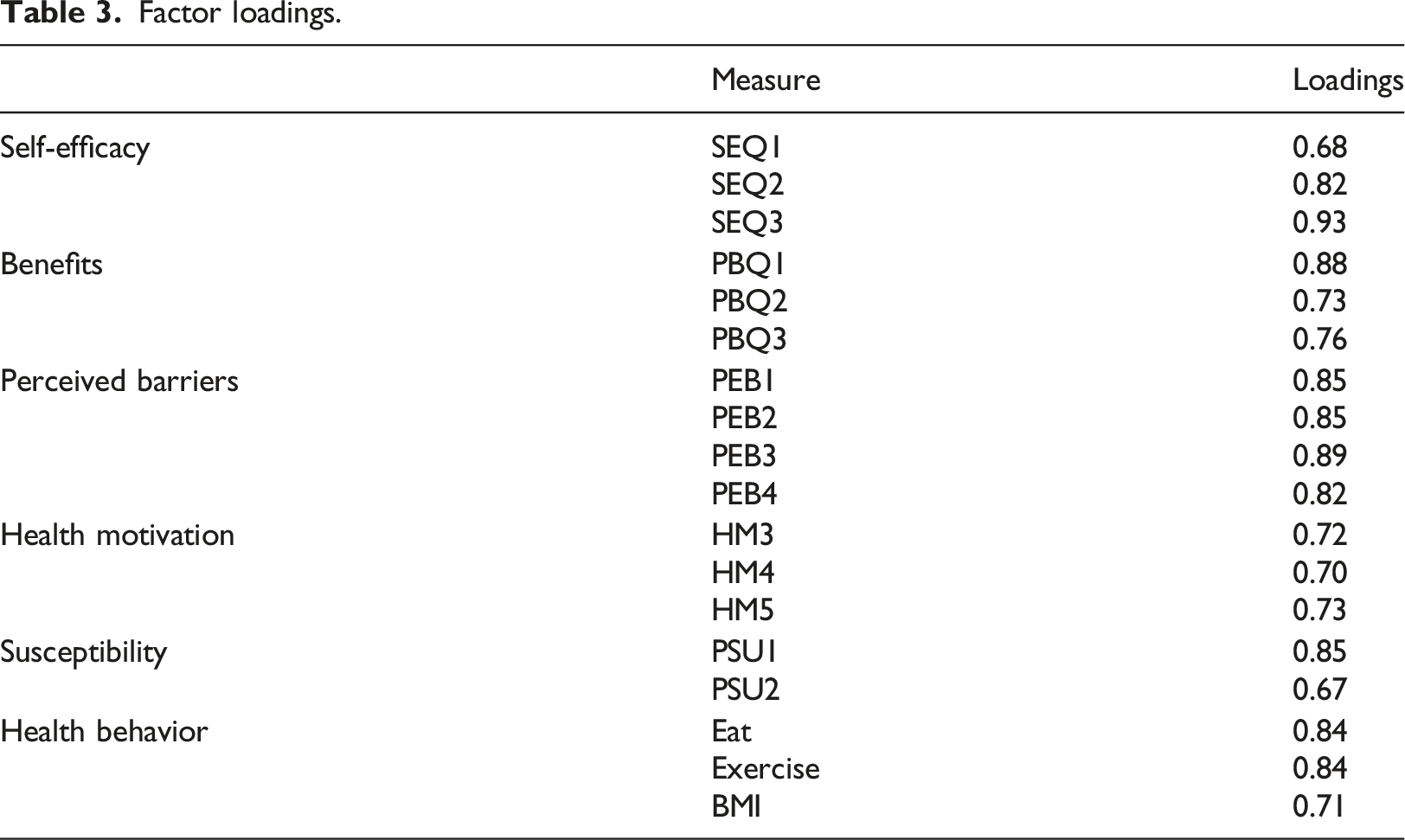
A confirmatory factor analysis using Stata 17 was used to test the measurement model.
Descriptive statistics of constructs.
Factor loadings.
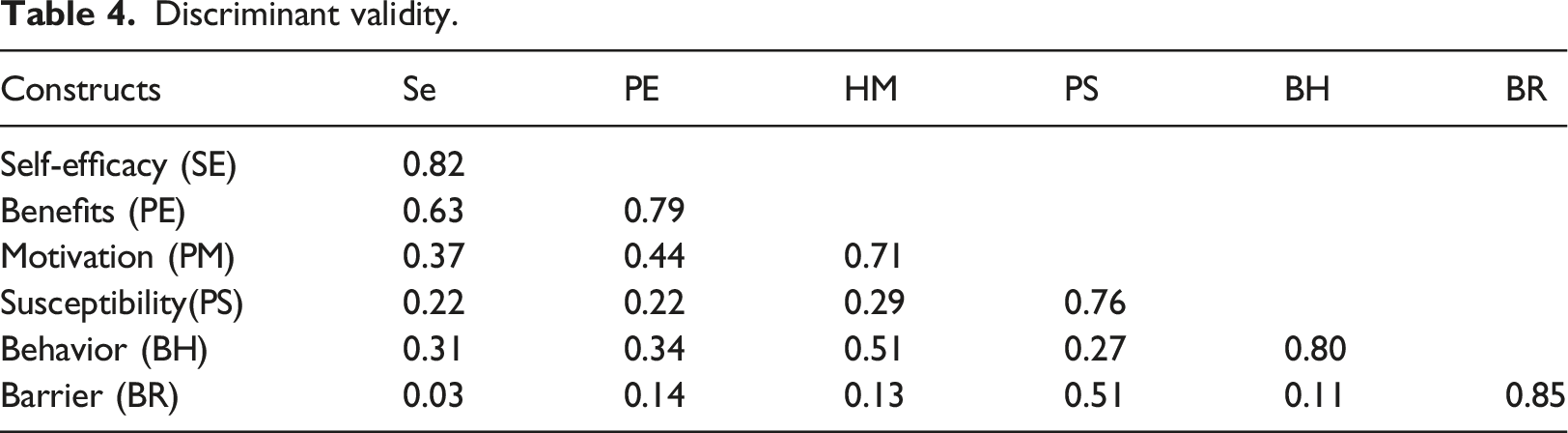
To test discriminant validity, we used two well-established methods: item-to-construct correlation, 53 and Fornell-Larcker's method on correlation and AVE, which requires the square root of the AVEs of each latent variable must be greater than its correlations with any other constructs. 51 Appendix 2 shows item-to-construct correlations, which provide evidence that all items correlated highly with their intended constructs.
Discriminant validity.
Structural model
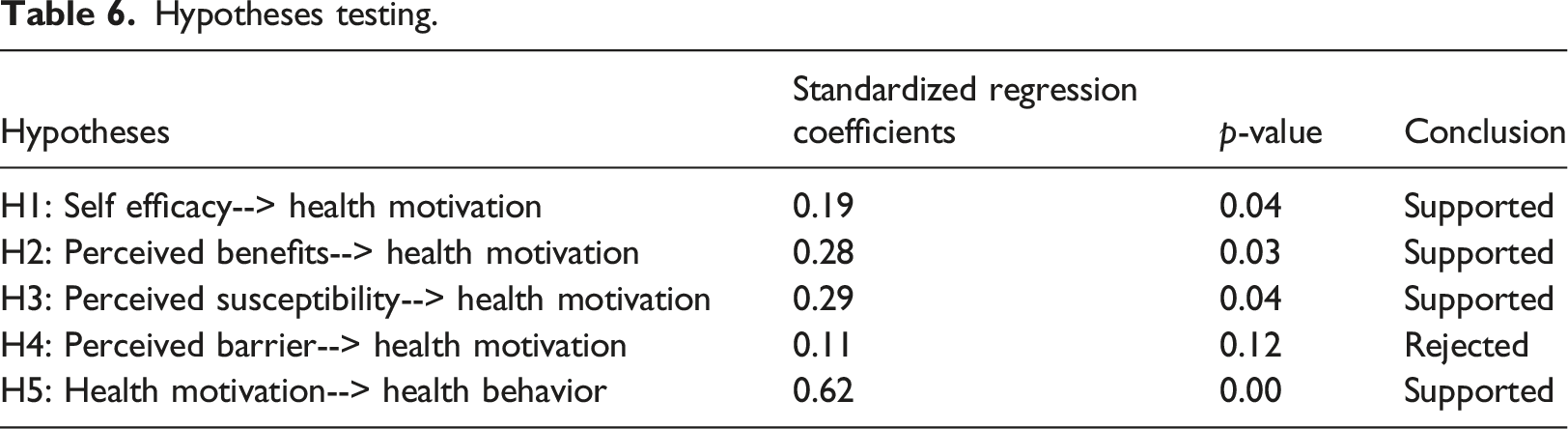
After validating the factor structure of the constructs, we proceed to test the structural relationships using a confirmatory approach. Stata 17 was used to conduct a CFI on our research model. Stata provides CFI, RMSEA, and TLI for model evaluation. Our model shows CFI=0.92, RMSEA 0.07, TLI =0.90. These fit indices satisfy the criteria for a good model fit (Bentler, 1990). 54 Our RMSEA is 0.07, which is an acceptable fit level (Browne and Cudeck, 1992). 55 The diagram below shows significant paths in the model. As shown in the diagram, when four variables are used to predict health promotion, only three are significant: self-efficacy perceived benefits and perceived susceptibility. The perceived barrier is not a significant predictor. Collectively the three constructs perceived efficacy, perceived benefits, and perceived susceptibility, explain 34.5% of the variance. The path coefficient from perceived efficacy to health motivation is 0.19 (p < 0.01). The path coefficient from perceived benefits to health motivation is 0.28 (p < 0.01). The path coefficient from perceived susceptibility to health motivation is 0.29 (p < 0.01). The path coefficient from health motivation to health behavior is 0.62 (p < 0.001) and health motivation explains 39.5% of the variance in health behavior.
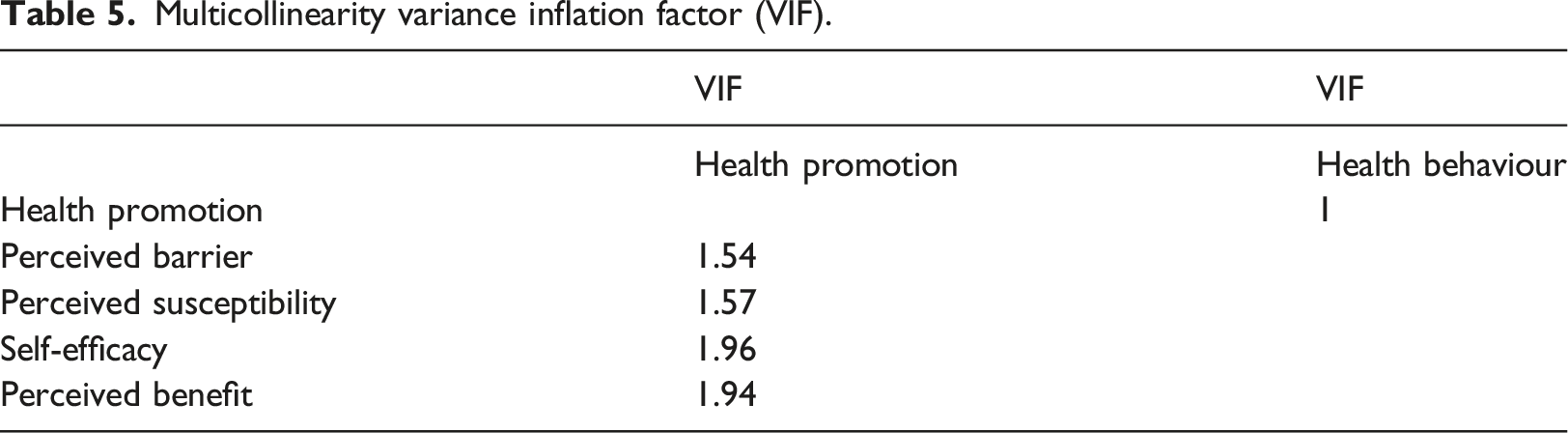
Multicollinearity variance inflation factor (VIF).
Hypotheses testing.
Analysis
Mediation test
According to Williams and MacKinnon,
57
bias-corrected bootstrapped confidence intervals (CIs) are considered more favorable compared to traditional theorem estimates. Using Stata, we applied bias-corrected bootstrapping techniques (1,000 bootstrap samples) and tested for biased-corrected two-tailed significance to confirm that the indirect effect was present Figure 2. Path results.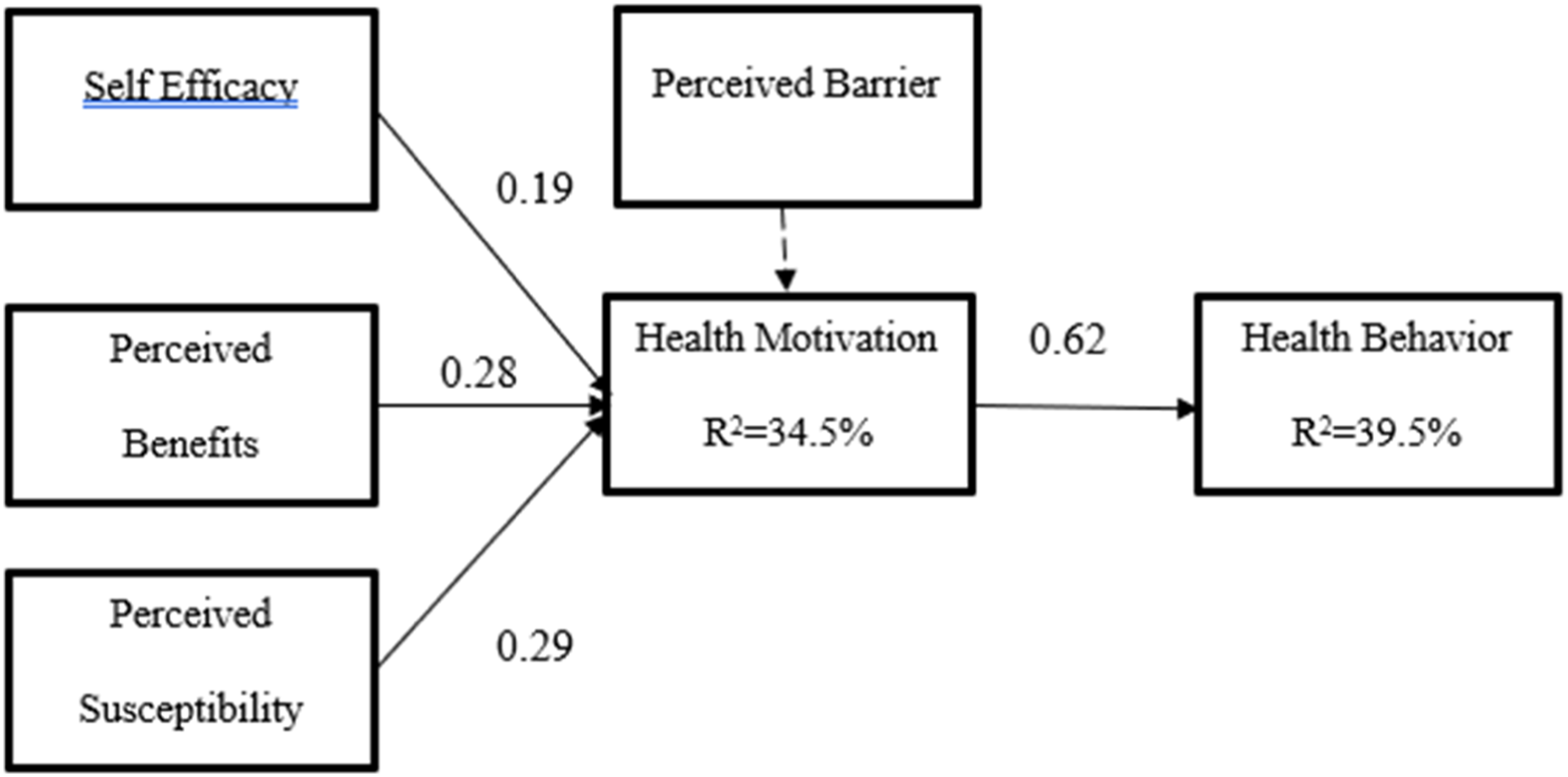
Direct and Indirect effects of Mediation.
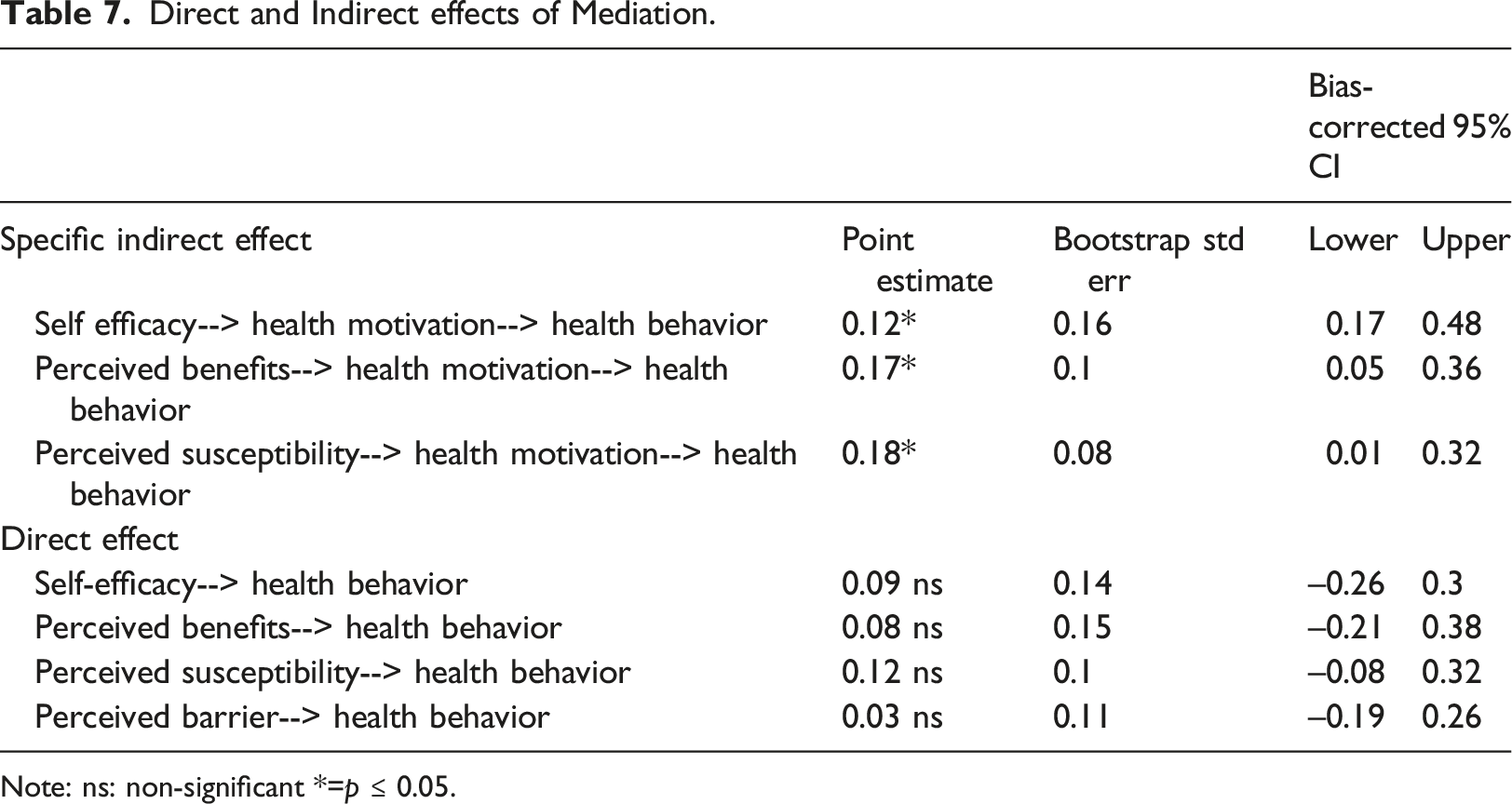
Note: ns: non-significant *=p ≤ 0.05.
Discussion
China's Ministry of Education reports that about 30% of Chinese college students failed to reach the “qualified” level of physical health as of 2020. 58 This calls for urgency in educating young people about health. The health of people determines their productivity. The Pandemic has made more people more conscious about their health, resulting in more extensive adoption of mobile health apps. Mobile apps promote health and wellness. 59 The health belief model has been validated in many contexts. Mobile health (m-health) apps can bring health prevention and promotion to the general population. 60 This study assesses adults' health perceptions, self-reported health attitudes toward using mobile health apps, and their behaviors. Built on Health Belief Model and Self Determination theory, this study tests a structural equation model of user perceptions of mobile health apps with motivation as a mediator which predicts health behaviors.
Several key findings are developed. First, this study finds that self-efficacy positively influences health motivation. This finding is consistent with what the literature reports.32,21,61 For example, people who are more knowledgeable about breast cancer self-examination are more motivated to conduct the self-examination 32 Another study on the obese population also reports that education is a significant predictor of the performance of health promotion. When applying this finding to practice, education and training is the key. When people gain knowledge and skills, they are more confident and motivated to change their behavior.
Second, this study also finds the positive influence of perceived benefits on health motivation. Intuitively, this relationship is expected. When the benefits are tangible or can be visualized, people are motivated to change their behavior. 42
A recent systematic review of the COVID-19 study 20 concludes that perceived benefits are the most significant predictor of behavior. Thus, any education materials for disease prevention or treatment should start with potential benefits. Letting people know the benefits would motivate them to engage in desired health behavior.
Third, this study confirms the positive relationship between perceived susceptibility and motivation. When people are worried about something or feel vulnerable to health-related issues, they are more likely to want to change their behavior. The worry or perceived risk is sufficient for people to change their behavior. 42 In a recent COVID-19 study on nursing students, 21 increased susceptibility will increase nursing students' intention to change their behavioral intention to prevent the spread of COVID-19.
Lastly, unlike prior studies, 21 this study did not find perceived barriers a predictor for motivation. This could be due to our study participants being familiar with mobile apps and how to use them, and they do not feel any extra effort or risks in using mobile apps. Furthermore, we confirm motivation is a very strong predictor of health behaviors. Thoughts and beliefs drive one's actions; in essence, changing people's beliefs will lead to changes in behaviors. 42 Access to smartphone applications improves one's beliefs of perceived susceptibility, self-efficacy, and health motivation. 6
Conclusion
Health has been a focused concern since the Pandemic. Mobile health apps have become an important platform for healthcare and gained popularity during the Pandemic. This study applied Health Belief Model to assess users' acceptance and attitudes toward using mobile health apps for health interventions. Our study focuses on the consumer-facing mobile health apps, which could be a useful health intervention for people to change their behavior. Healthcare mobile apps can satisfy our health-related needs and empower us to manage our health any time anywhere with an intuitive interface that is easy to learn and use for most consumers. Moreover, this study further confirms the importance of self-efficacy and perceived benefits in changing consumers' behavior. In practice, mobile health app vendors should target the benefits when promoting their health apps; it is also essential to tackle self-efficacy issues when addressing behavior change. Yet, long-term sustainability, user behavior, and engagement with mobile health apps continue to be important research areas. Our future studies will address the health belief model in different cultures and contexts.
Limitations
We recognized a few limitations with our research. First, we collected data in China to test our model. The literature documented evidence of cultural differences in people's attitudes and behavior 28 Thus, generalization should be applied to similar contexts. Future studies could test our model in a different cultural context. Second, we did not use a random sampling strategy. Though our sampling method is not random, the selection of the study participants suits the purpose of this study. Future studies will use the random sample to test the same model to examine the predictive validity of the model. It should be borne in mind that the survey results are not generalizable across the entirety of the Chinese population. Third, our questionnaire on mobile health apps did not target a particular disease category. There are many disease-specific mobile apps on the market. It will be helpful to expand our study to disease-specific apps and mobile health apps that are recommended by clinicians. Cross-validation of the results is useful in knowledge transfer and generalization. Future studies may tailor questions to disease types to further validate the health belief model.
Footnotes
Acknowledgments
The authors would like to thank all people who participated in this study.
Author contributions
The first and second authors conceptualized the paper and developed the research model. The second author developed the survey instrument. The first author performed the analysis and drafted the paper. The third author collected data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Zhejiang National Science Foundation (PI: Xueyan Yang, No. LY 20G02001).
Ethical Statement
The institution Review Board at Northern Kentucky University approved this study (IRB#344). Zhejiang National Science Foundation (LY 20G02001) in China approved this study. Online consent was obtained prior to data collection.
Appendix 1
Survey questions.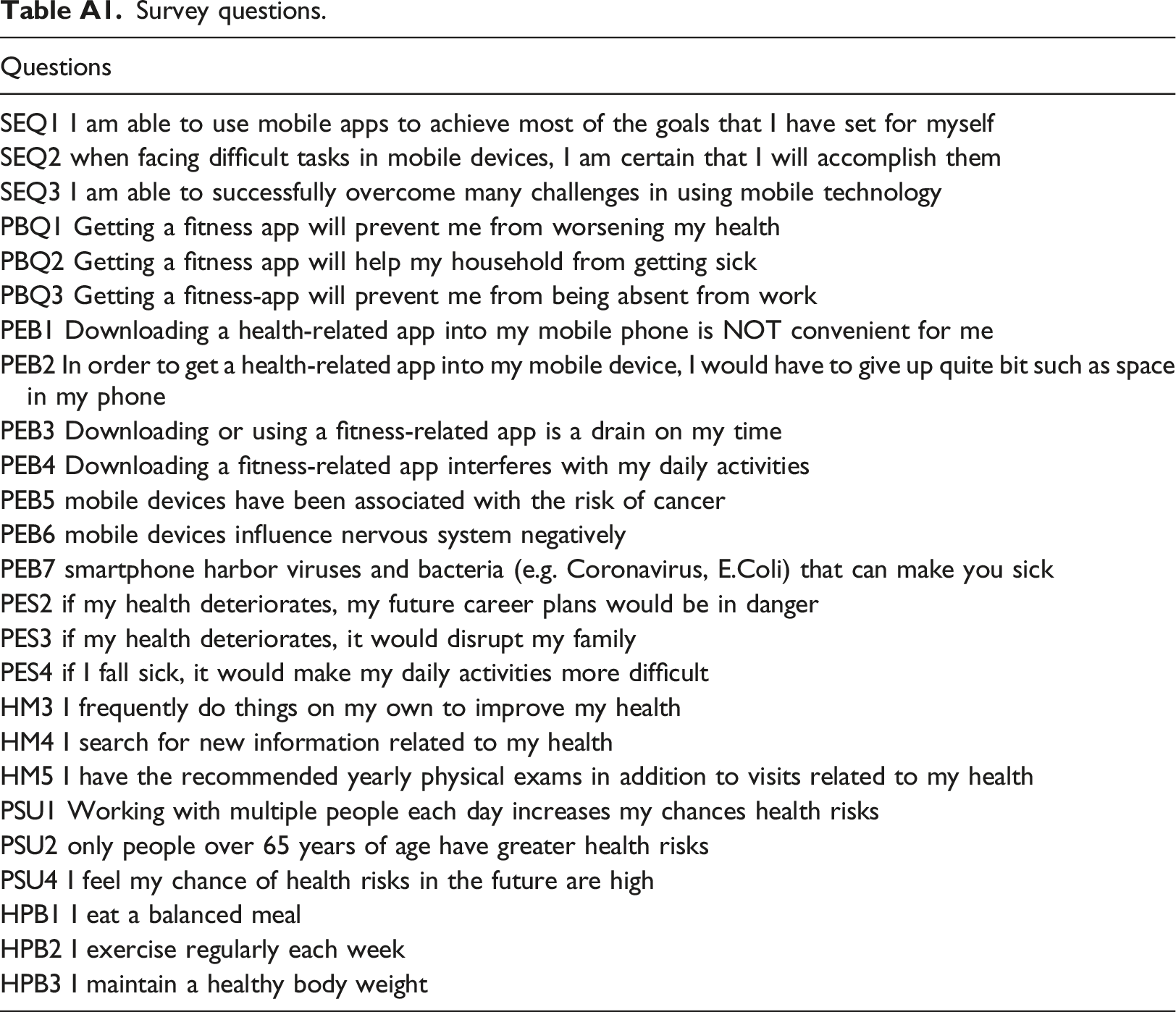
Questions
SEQ1 I am able to use mobile apps to achieve most of the goals that I have set for myself
SEQ2 when facing difficult tasks in mobile devices, I am certain that I will accomplish them
SEQ3 I am able to successfully overcome many challenges in using mobile technology
PBQ1 Getting a fitness app will prevent me from worsening my health
PBQ2 Getting a fitness app will help my household from getting sick
PBQ3 Getting a fitness-app will prevent me from being absent from work
PEB1 Downloading a health-related app into my mobile phone is NOT convenient for me
PEB2 In order to get a health-related app into my mobile device, I would have to give up quite bit such as space in my phone
PEB3 Downloading or using a fitness-related app is a drain on my time
PEB4 Downloading a fitness-related app interferes with my daily activities
PEB5 mobile devices have been associated with the risk of cancer
PEB6 mobile devices influence nervous system negatively
PEB7 smartphone harbor viruses and bacteria (e.g. Coronavirus, E.Coli) that can make you sick
PES2 if my health deteriorates, my future career plans would be in danger
PES3 if my health deteriorates, it would disrupt my family
PES4 if I fall sick, it would make my daily activities more difficult
HM3 I frequently do things on my own to improve my health
HM4 I search for new information related to my health
HM5 I have the recommended yearly physical exams in addition to visits related to my health
PSU1 Working with multiple people each day increases my chances health risks
PSU2 only people over 65 years of age have greater health risks
PSU4 I feel my chance of health risks in the future are high
HPB1 I eat a balanced meal
HPB2 I exercise regularly each week
HPB3 I maintain a healthy body weight
Appendix 2
Item-to-construct correlation: discriminant validity.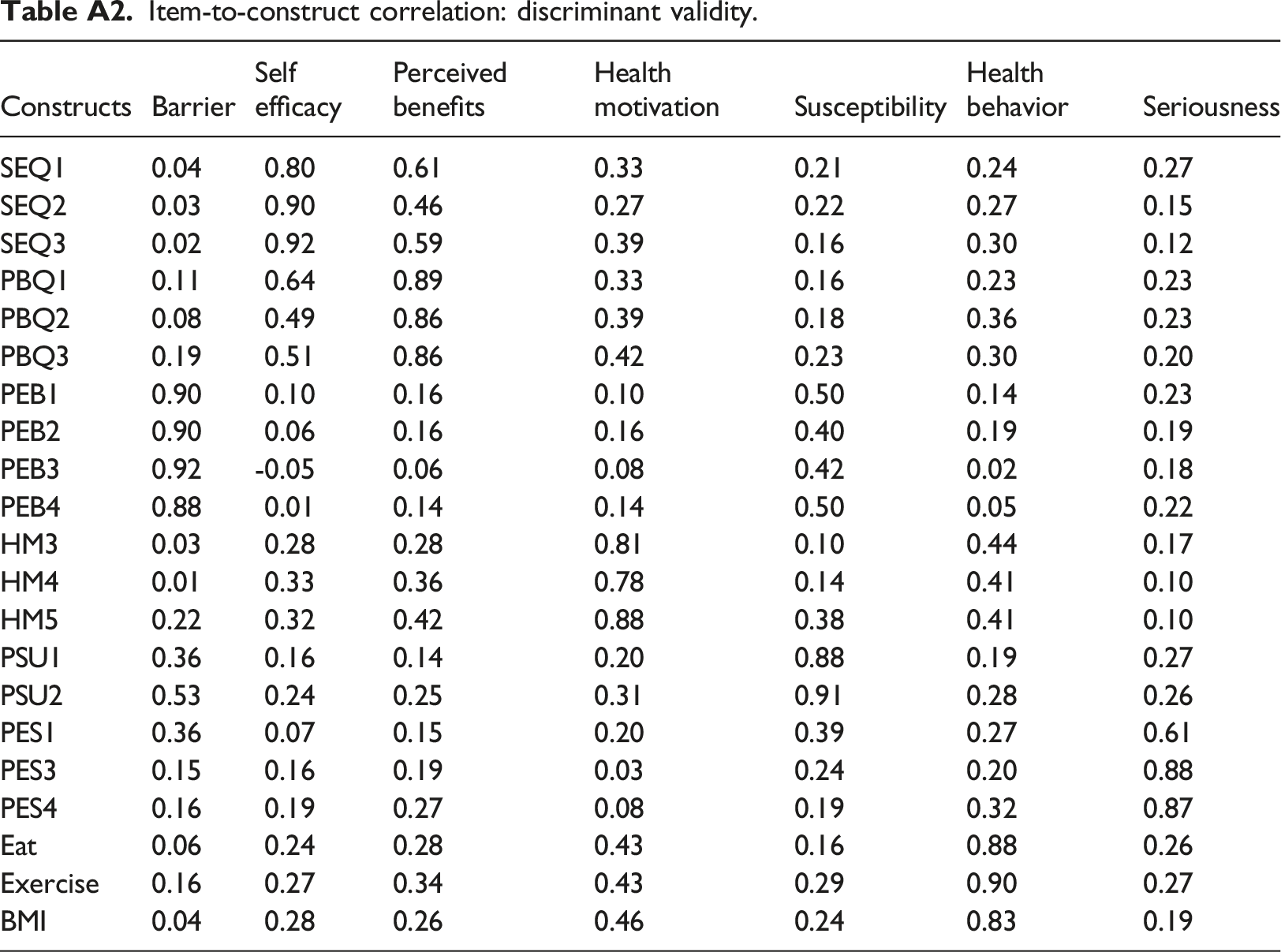
Constructs
Barrier
Self efficacy
Perceived benefits
Health motivation
Susceptibility
Health behavior
Seriousness
SEQ1
0.04
0.80
0.61
0.33
0.21
0.24
0.27
SEQ2
0.03
0.90
0.46
0.27
0.22
0.27
0.15
SEQ3
0.02
0.92
0.59
0.39
0.16
0.30
0.12
PBQ1
0.11
0.64
0.89
0.33
0.16
0.23
0.23
PBQ2
0.08
0.49
0.86
0.39
0.18
0.36
0.23
PBQ3
0.19
0.51
0.86
0.42
0.23
0.30
0.20
PEB1
0.90
0.10
0.16
0.10
0.50
0.14
0.23
PEB2
0.90
0.06
0.16
0.16
0.40
0.19
0.19
PEB3
0.92
-0.05
0.06
0.08
0.42
0.02
0.18
PEB4
0.88
0.01
0.14
0.14
0.50
0.05
0.22
HM3
0.03
0.28
0.28
0.81
0.10
0.44
0.17
HM4
0.01
0.33
0.36
0.78
0.14
0.41
0.10
HM5
0.22
0.32
0.42
0.88
0.38
0.41
0.10
PSU1
0.36
0.16
0.14
0.20
0.88
0.19
0.27
PSU2
0.53
0.24
0.25
0.31
0.91
0.28
0.26
PES1
0.36
0.07
0.15
0.20
0.39
0.27
0.61
PES3
0.15
0.16
0.19
0.03
0.24
0.20
0.88
PES4
0.16
0.19
0.27
0.08
0.19
0.32
0.87
Eat
0.06
0.24
0.28
0.43
0.16
0.88
0.26
Exercise
0.16
0.27
0.34
0.43
0.29
0.90
0.27
BMI
0.04
0.28
0.26
0.46
0.24
0.83
0.19