
Abstract
Objective
Health self-monitoring technologies are gaining popularity worldwide, but they face low adoption rates in emerging countries. There is a deficiency in studies that have applied the value-belief-norm (VBN) model to understand the adoption of IoT-enabled wearable healthcare devices (WHDs). This study investigates the adoption of IoT-enabled WHDs among older adults in China, using the VBN model as a theoretical framework.
Methods
Using a convenience sampling method and a web-based cross-sectional survey method, we collected data from 476 respondents, which we analyzed using partial least squares structural equation modeling using Smart PLS version 3.3.5.
Results
The findings highlight the significance of health values and motivation in shaping personal health beliefs, which, in turn, influence personal norms and awareness of consequences. Particularly, awareness of consequences and attributions of responsibility significantly impact personal norms. Personal and social norms, in turn, strongly affect the intention to adopt IoT-enabled WHDs, ultimately driving their actual adoption.
Conclusion
This research contributes novel insights into the behavioral dynamics surrounding the adoption of IoT-enabled WHDs, providing valuable guidance for marketers and policymakers. Marketers can leverage these insights to develop tailored marketing strategies within the IoT-enabled WHD industry. Additionally, policymakers are urged to prioritize campaigns aimed at enhancing awareness and understanding of self-healthcare monitoring, with a focus on promoting the unique health benefits of IoT-enabled WHDs.
Keywords
Introduction
Ensuring that individuals live actively and healthily as they grow older is one of the most important issues in society. 1 Noncommunicable diseases (NCDs), which include cardiovascular abnormalities, hypertension, respiratory illnesses, cancers, kidney diseases, and diabetes, are the leading causes of mortality worldwide. According to the World Health Organization, 2 there were 41 million deaths globally due to NCDs in 2020. Healthy lifestyle habits can significantly prevent approximately 75% of heart disease, brain stroke, heart failure, and type II diabetes risks, as well as 40% of cancer risks. 3 This phenomenon can be addressed and controlled by lowering lifestyle risk factors, such as restricting the intake of unhealthy diets, nicotine, and alcohol; promoting physical exercise; and, most importantly, regular monitoring of health status (e.g., glucose level, hypertension, and blood cholesterol level). 4
Internet-of-Things (IoT)-enabled wearable healthcare devices are becoming increasingly popular. 5 These devices offer a variety of solutions, such as fitness trackers, smartwatches, remote patient monitoring devices, specialized monitors (i.e., electrocardiogram and electroencephalography monitors), and smart clothing with built-in sensors.6,7 Wearable technologies allow on-body real-time scanning and computation of personal physiological data. 8 IoT-related healthcare systems use remote monitoring to aid users with physical and psychological challenges by detecting and analyzing numerous body functionalities, such as blood pressure, blood oxygen level, heart rate, and body temperature. 9 Several IoT devices and services in healthcare (e.g., monitoring physical parameters, diet-activity-weight-sleep tracking, fall detection, anomalous activities, location detection, emergency assistance, and medical expert advice) have been established to address the needs of senior adults by stabilizing their deficiencies and minimizing predictable health issues. 6 The adoption of IoT-enabled healthcare devices may bridge the gap between doctors and patients by allowing them to communicate regularly by sharing real-time health records. Such devices can benefit older patients by providing them with high-quality health monitoring data and necessary treatments at lower costs. 10
The increase in the elderly population has driven the demand for digital healthcare systems to constantly monitor these senior adults. 8 Recent studies have highlighted IoT as the latest technology that may cause a few challenges. 11 One of the major challenges for senior adults (middle-aged and elderly) is their lack of familiarity with digital-age technologies, forcing them to put in extra effort to cope with new technologies, such as the IoT. 12 Consequently, potential users may be skeptical of the benefits and disinclined to use IoT healthcare systems, perceiving product value as a barrier. 13 Apart from these challenges, providers of IoT-enabled wearable health devices (WHDs) must also consider the technical hurdles inherent in such concepts. These include the seamless integration and comprehensive data collection from these devices, with a paramount focus on ensuring their reliability, particularly in healthcare settings.14,15 Furthermore, within the realm of challenges crucial to the healthcare domain lies the paramount concern of data privacy and anonymity.16,17 Ensuring the secure transmission of data from IoT-enabled WHDs is another ubiquitous challenge that adults are deeply concerned about. 18 Providers of IoT-enabled WHDs must bridge this gap by extensively exploring user behavioral and decision-making factors that induce their intention to adopt these devices.
A literature review reveals a demographic gap in adults’ behavioral attitudes toward the adoption of IoT-enabled WHDs. Younger individuals and those with higher health consciousness are more inclined toward adoption,19–21 while concerns over privacy and individual values vary across demographic groups. 22 Reasons for and against adoption influence the adoption of IoT-based wearables for older adults’ healthcare, revealing demographic gaps in age and health status. Additionally, values impact attitudes toward innovation, varying across demographic segments.23,24 Also, there is a possibility of higher death rates among the aging population in the forthcoming years. According to the WHO, 25 NCDs were responsible for 89% of all deaths in China in 2016, which increased to 90% by 2019. 26 It is anticipated that by 2030, China's aging population will be responsible for a 40% increase in the incidence of chronic illnesses. 27 This high mortality rate emphasizes the need for adults to regularly monitor their health status to receive the necessary attention and treatment on time and avoid regrettable fatalities. To address this demographic gap, this study targets Chinese senior adults (aged 40 years and above) to determine the key determinants influencing their adoption of IoT-enabled WHDs for regular health monitoring.
In the current literature, both the theory of reasoned action (TRA) and the theory of planned behavior (TPB) have been extensively implemented to understand and predict a wide array of health-related activities, including physical activities, 28 glucose monitoring, 29 blood pressure monitoring, 30 and individual health behaviors during the pandemic. 5 Several studies have adopted the health belief model (HBM) due to its effectiveness in elucidating healthcare behaviors.19,31 Many studies have combined and added to other theories, such as the unified theory of acceptance and use of technology (UTAUT), the technology acceptance model (TAM), the health monitoring behavior (HMB), and the technology acceptance theory (TAT), to try to explain why information technology (IT) is being used in healthcare and with health monitoring equipment.32–35 Only a few studies have included norm activation theory in conjunction with other theories to study healthcare practices and personal health monitoring device adoption.36,37 To the best of our knowledge, we have not yet completely implemented the value-belief-norm (VBN) model to empirically explore users’ decision-making processes involving healthcare and health-monitoring gadgets. Individual components of the VBN model, such as health interests, 29 personal health values, 38 health beliefs, 39 health motivation, 40 awareness of consequences, 37 personal responsibility in the form of an ascription of responsibility 41 and moral considerations, 42 have been investigated in various prior studies within the context of health monitoring activity and technology adoption. However, previous studies did not thoroughly examine these components.
This study addresses several theoretical gaps in the literature on the adoption of IoT-enabled WHDs. First, intrinsic factors that drive user decision-making regarding the adoption of IoT-enabled WHDs, such as health values (HVs) and health motivation (HM), have been inadequately theorized. Second, the influence of social norms on users’ intentions to adopt IoT-enabled WHDs has remained largely unknown. Third, empirical studies on users’ actual behavioral responses based on the VBN model are limited. This study aims to address these gaps by developing and testing an expanded VBN model to enhance the existing knowledge of users’ adoption of IoT-enabled WHDs. The significance of this study lies in the fact that this research notably advances the understanding of technology adoption behavior within the context of I WHDs, bridging the gap between technical aspects and user decision-making processes. By integrating theories from both the technological adoption and health behavior domains, it offers a comprehensive framework for elucidating the complex factors influencing adoption behavior, particularly among older adults in China. Furthermore, the study's empirical validation of the extended VBN model underscores its practical relevance in guiding interventions aimed at promoting the adoption of IoT-enabled WHDs and fostering positive health behaviors. Moreover, the study's insights can empower healthcare practitioners and older populations to recognize the effectiveness of IoT-enabled WHDs, ultimately contributing to the improvement of the country's overall health service status in the long term. Furthermore, the findings can inform related firms in developing relevant product features for IoT-enabled WHDs and devising market strategies by offering valuable insights into user decision-making and behavioral characteristics.
There are seven separate parts to this research: first an introduction, followed by a section on theoretical background and hypothesis development, then the section on methodology , and the fourth section on data analysis and presentation of findings. The fifth section covers critical discussion, and the sixth section discusses practical and theoretical implications. Finally, we have the section on conclusion and acknowledgment of limitations.
Literature review
Theoretical background
According to Stern et al., 43 the VBN theory suggests that individuals who uphold the core values of a movement perceive a threat to those values, believe that their actions can help restore and uphold those cherished values, and feel a personal obligation to take promovement action. Schwartz's 44 theory proposes that actions relevant to norms involve three key concepts: acknowledging an individual's specific values, recognizing a threat to something important to those values, and believing that one's behavior can mitigate the threat and restore value, known as personal norms (PNs). Schwartz 45 categorized values into three types: biospheric, altruistic, and egoistic. Beliefs encompass an ecological worldview (EW), awareness of consequences (AOC), and ascription of responsibility (AOR), which together influence behavioral intention. Values, in particular, influence the adoption of EW, which in turn heightens AOC and AOR, leading to PNs and social norms (SNs) that can predict behavior or behavioral intentions. 46
The VBN theory has demonstrated its efficacy as a reliable predictor of sustainable behaviors across various contexts, finding widespread application in elucidating proenvironmental behaviors. These include areas such as residential energy savings, 47 sustainable tourism, 48 climate-conserving behavior, 49 environmentally friendly cruise travel, 50 reduction of household environmental pollution, 51 human proenvironmental behavior, 52 and organic food composting. 53
Moreover, scholars have expanded the VBN theory by incorporating additional variables such as SNs and perceived behavioral control, 54 emotion, 55 and factors like trust, satisfaction, and past behavior incidence. 56 While the original model focused on PNs as a single dimension of norms, de Groot et al. 57 and Kim et al. 58 argue that PNs should be expanded to include SNs to establish a comprehensive norm that encompasses both internal and external influences. Scholars also advocate for the inclusion of HVs 38 and HM, 40 as well as health beliefs. 39 Thus, the present study incorporates HVs and HM as factors related to health beliefs, which in turn affect intention to adopt IoT-enabled WHDs (IWHD) and actual adoption of IoT-enabled WHDs (AWHD) through SNs and PNs.
Hypothesis development
Health values (HVs)
HVs refer to one’s proclivity to implement health initiatives,
31
exhibiting the qualities of being sensitive to physical health risks and hazards.
59
HVs typically represent individuals’ views on the significance and priority of health, as well as the perceived value or efficacy of adopting healthy behaviors.
60
These values serve as motivating factors, encouraging individuals to strive for their health-related objectives and aiding in the synchronization of these objectives with their physical and mental well-being.
61
Furthermore, HVs can influence individuals’ beliefs about various health issues and behaviors, encompassing both cognitive and affective aspects such as the benefits of disease prevention and management, maintaining a healthy weight, and adopting healthy habits to improve longevity.
60
Individuals who value their health adopt self-tracking devices to consciously and purposefully measure their health status (e.g., pulse rate, sleeping time, daily exercise, calorie burns, somatic symptoms, anxiety, and recovery) to evaluate and transform their lives accordingly.
62
Zhang et al.
36
empirically demonstrated the higher tendency of individuals concerned about their health to acquire new health-related technologies, the higher level of perceived health value leads to a relatively higher level of belief and confidence in effectively managing health status from any health hazard.
39
A recent study found a consistent link between personal health values and healthy eating views.
63
Based on this argument, the following hypothesis is proposed:
Health motivation (HM)
HM is characterized by a high aspiration to engage in positive behaviors, such as eating well, living in a healthy environment, and monitoring health conditions, to prevent health complications.
64
HM can drive consumers to actively seek out and engage with health-related information, thereby enhancing their comprehension and awareness of health and healthy living practices. Additionally, it can foster the formation of steadfast and persistent attitudes and behaviors toward health.
65
Scholars identified that HM has an impact on self-tracking device continuation intention,
66
self-tracking enables users to achieve their fitness goals,
67
the intention to use wearable fitness gadgets,
68
and the use of wearable self-tracking tools.
69
Attig and Franke
40
observed that individuals with significant extrinsic motivation become heavily reliant on monitoring devices. Ivanov et al.
70
examined the factors influencing patients’ willingness to share health-tracking data with professionals and reported a significant influence of patients’ HM on their beliefs in sharing health data with clinicians. According to the latest findings by Yang et al.,
53
individuals who possess robust HM tend to hold more favorable beliefs regarding healthy eating. Thus, the following hypothesis is postulated:
Personal health beliefs (PHBs)
Individuals’ personal beliefs on the effectiveness of specific activities in improving their overall health status are called “health beliefs.”
36
A high degree of personal health belief about the utility of WHDs leads to awareness of the devices’ benefits and consequences for health management, which, in turn, drives the intention to adopt WHD.
35
Consumers with higher PHBs who also actively explore solutions to improve their health state are more likely to make efforts to gain further knowledge about the utility of wearable healthcare technologies,
34
resulting in higher PNs. Prior empirical studies have supported the significance of PHBs in improving users’ inclination to adopt fitness-tracking technologies.36,71 PHBs about the health risks and health consequences of any adverse activity minimize the possibility of engaging in careless health habits.
72
Cognitive and emotional beliefs about online health information are critical for individuals who believe that their health is compromised.
32
Yang et al.
63
demonstrated that personal healthy eating beliefs have a significant influence on PNs and awareness of the consequences. Accordingly, the following hypotheses were postulated, linking personal health beliefs with awareness of consequences and PNs:
Awareness of consequences (AOC)
Individual viewpoints on the positive effects of any behavior on others are referred to as the awareness of consequences.
73
Awareness of consequences has a highly significant relationship with ascribing responsibility
74
and triggers PNs.
75
Individuals with high awareness of the consequences of chronic diseases may communicate with their trusted others about taking the necessary health measures, such as using self-monitoring health tools, to lessen their despair, anxiety, and panic when they witness the suffering of others.
33
Shanka and Kotecho
37
empirically demonstrated that awareness of the negative consequences of breaching COVID-19 safety measures is a key driver of moral and practical transformations that ultimately lead to compliance. Individuals have become more aware of the consequences of health hazards and chronic illness complications because of their persistent health issues, promoting the use of fitness and health monitoring technologies.
33
In line with the findings of Yang et al.,
63
we can conclude that awareness of consequences has a major impact on the assignment of responsibility and PNs. The following hypotheses are generated based on the preceding discussion:
Ascription of responsibility (AOR)
AOR is a sense of individual accountability for the consequences of prosocial initiatives.
73
It refers to the strong belief that even minimal effort can potentially prevent harmful effects.
76
Individuals commonly develop morality when they feel responsible for the negative consequences of their activities, and those who refuse to be accountable for the resultant adverse consequences are less likely to form PNs.
77
E-healthcare focuses on shared decision-making and enhances one’s sense of self-responsibility, which is especially suited for those with chronic conditions where health improvement patterns are both incremental and complex.
78
In a previous qualitative study, McBride et al.
30
reported that numerous interview participants expressed that their enhanced sense of personal responsibility forced them to take corrective initiative when their blood pressure records consistently and repeatedly exceeded the threshold. According to Sharon,
41
the overall health of a community can be strengthened if the community members develop a sense of personal responsibility to maintain their health. Carfora et al.
61
identified that ascription of responsibility and PNs are positively connected. Considering the significant influence of the AOR on the development of PNs in the context of healthcare monitoring, the following hypothesis is proposed:
Personal norms (PNs)
PNs determine whether an individual should engage in a specific activity to reduce adverse consequences.
76
PNs are triggered when individuals perceive that social action has a favorable influence on others and when they feel responsible for the negative ramifications of their passivity.
74
For example, health professionals may instill feelings of moral obligation to exercise by offering self-management assistance and advising patients with type II diabetes to participate in physical exercise.
28
With regard to medicine adoption, moral norms were identified as having a major impact on individuals’ vaccination uptake intention compared with other behavioral aspects.
79
Individual adoption of an artificial intelligence system in healthcare necessitates evaluation from a moral perspective.
80
Hence, the characterization of moral norms in healthcare monitoring is highly justified. Physical indolence, in the context of being overweight or obese, is subject to personal and moral condemnation in a society where a higher degree of physical exercise is recognized as a moral norm.
81
Yang et al.
53
concluded that strong personal norms had a significant impact on the consumption of organic foods. Based on this rationale, this study develops the following hypothesis:
Social norms (SNs)
SNs are individuals’ assessments of whether important others around them feel that they should (or should not) engage in a particular initiative.
82
For instance, individuals are willing to accept and embrace WHDs when they observe a prominent personality and endorse their use.
35
Given that the judgments of family members and friends significantly influence user behavior, social norms are recognized as important factors that motivate patients’ behavior in the uptake of ICT-based healthcare services.
83
Lee and Lee
35
found that patients with optimal health improvement experience with wearable health technologies were more willing to recommend them to their acquaintances. Although it was empirically revealed to have no substantial impact on end users’ intentions to use, Ben et al.
13
highlighted social influence as a key element in influencing users’ intention to adopt IoT-enabled healthcare devices in France. Individuals may also be inspired to become potential users of wearable healthcare devices based on their acceptance in society.
35
Focusing on the context of mobile healthcare services with IoT devices, Liu et al.
84
identified social norms as a crucial element in consumers’ adoption of such technology in China. Based on the preceding observations, this study proposes the following hypothesis:
Intention and adoption of IoT-enabled WHDs
Behavior can be defined as an intentional activity performed as a consequence of various processes.
43
The desire to engage in an activity is a decisive element in the explosion or nonexplosion of a certain behavior.
85
Intention affects behavior, as individuals are thought to be rational, intend to attain a certain goal, and act accordingly.
86
According to Ahmed et al.,
87
consumers are significantly impacted by the materialistic intent to use IoT as well as the actual usage of IoT. An individual’s intention to use an e-health device positively impacts actual device utilization.
42
Although WHDs share many properties with other technology-related products and services, these devices differ in a number of ways (e.g., public perception of physical health impact), making it imperative to explore the factors that influence users’ adoption of these devices.
35
Based on these arguments, the following hypothesis is proposed for testing:
Perceived product value as moderating variable
According to Yang et al.,
88
perceived value is linked to four aspects: (a) comparatively low cost; (b) user expectations of the product; (c) expected product quality; and (d) what users truly acquire in terms of patching up. The cognitive tradeoff that users make between the perceived benefits of employing new technology and the monetary expense of doing so is referred to as the perceived price value.
89
According to Lee and Lee,
90
users tend to analyze the product value and intended benefits of healthcare technologies for adoption. Users’ assessment of product usability influences their satisfaction, while users’ perspectives on the value of utilizing mobile healthcare services reflect the objective dimension that influences their intention to adopt such services.
84
Kim and Kim
91
postulated that discrepancies in the functionality of IoT healthcare services, specifically the usefulness of features and performance, may lead to variances in perceived value among users. In other words, direct or indirect experiences or predicted values constantly influence one’s desire to use wearable devices and applications.
35
Hossain et al.
29
recognized perceived value as a key element and empirically evaluated its influence on the adoption of wearable devices for continuous glucose level monitoring. Considering the support for the significance of perceived product value in earlier studies, this study proposes its moderating effect on the relationship between IWHD and AWHD.
All hypothesized relationships in this study are illustrated in Figure 1.

Research framework.
Methodology
This study quantitatively examines the hypothesized relationships among these constructs. Partial least squares structural equation modeling (PLS-SEM) was used to measure and assess the structural models using SmartPLS (V.3.3.5) software. PLS-SEM is a nonparametric and multivariate approach commonly employed to assess path correlations with latent variables. 92 PLS-SEM is often suggested for exploratory research, particularly when the research framework is sophisticated and contains mediating and moderating variables. 93 This exploratory study examines the intention to adopt and actual adoption of IoT-enabled WHDs. Furthermore, the research framework comprises multiple independent factors and a moderating variable. This study conducts a sex multigroup analysis. Furthermore, based on numerous studies in similar research, 94 PLS-SEM is regarded appropriate for this investigation.
Population and sample size
To test the research hypothesis, we conducted an online survey among middle-aged and elderly populations in China (Figure 2). According to the age groups provided by the WHO, individuals below 44 years are considered young, those between 45 and 59 years are middle-aged, and those above 60 years are classified as elderly. However, considering China's research background and to ensure that the study results have more practical significance, age groups should be closer to the actual situation in China. Based on the Civil Code of the People's Republic of China and the Chinese National Youth Federation, the age groups were defined as follows: individuals aged 18–40 were considered young, whereas those aged 41 years and above were classified as middle-aged and elderly. For this study, the target population was restricted to individuals aged 40 and above. Due to China's large population, it was impossible to obtain a detailed list of age distributions by region. Consequently, this study did not employ probabilistic sampling, and a nonprobability sampling method was chosen instead. 95 A convenience sampling strategy was employed, and a purposive selection of middle-aged and elderly individuals was conducted during the questionnaire distribution phase. A conventional equal-interval scale was used to avoid potential data collection bias related to the sensitive nature of age questions in the survey. 96 The age intervals started at 20 years, with each interval spanning 10 years. Of the 496 collected samples, 476 were relevant to the research background. Following the guidelines proposed by Faul et al., 97 G*Power was used to estimate the appropriate sample size. Consequently, this study required a minimum of 114 respondents to investigate the expected effects based on the following parameters: effect size (f2) of 0.15; α error probability of 0.05; power (1–β error probability) of 0.80; and nine predictor variables. The final data collection yielded a sample size that satisfied the minimum requirements.

Flowchart of research methodology.
Data collection
This study uses an online survey approach, with respondents accessing the questionnaire via WJX site (https://www.wjx.cn/). An online questionnaire was distributed via platforms such as WeChat. Before participating in the survey, the respondents were informed about the objective of the research, the ultimate use of the data, and the noncommercial nature of data collection. Subsequently, the respondents read and agreed to an informed consent form that explained their right to participate and withdraw from the survey at any time. At this stage, all respondents were reminded that there were no right or wrong answers and were encouraged to provide genuine responses to minimize potential bias due to data collection. Considering that WHDs involve specialized academic vocabulary, this study provides a detailed explanation of the meaning, utility, common functionalities, and devices available in the market to help respondents better understand the background of the research. After signing an informed consent form, the respondents entered the data collection phase. Ultimately, 496 responses were received. Based on the age-related background questions, samples with age options below 40 years were excluded, resulting in a final set of 476 samples aligned with the research background.
Measurement items
Apropos the objectives of this study, the questionnaire was developed based on previously validated instruments with minor modifications (as presented in Supporting Material 1: Survey Instrument). Clear, straightforward, and unbiased phrasing was employed to ensure respondents’ engagement in completing the survey accurately and easily. Four items were adapted from Yang et al. 53 to measure HVs, and five items were derived from Li et al. 98 to measure HM. We adopted five items from Yang et al. 53 to measure PHBs. In this study, AOC, AOR and PNs were evaluated using five items each, which were adopted from Al Mamun et al. 99 and five items were derived from Yang et al. 100 to measure social norms (SNs). Additionally, this study adopted five items from Kim et al. 101 to assess perceived price value. In this study, IWHD was evaluated using five items from Hayat et al. 102 Lastly, one item was included to assess AWHD. Respondents were required to provide responses that best reflected their views on a seven-point Likert scale. All items used in this study adopted from papers used CC BY-4 license, which permits the adoption of materials without any permission.
Results
First, the demographic characteristics of the respondents and other relevant activity information were descriptively analyzed. Next, the obtained data were subjected to SEM using the SmartPLS software. The following sections explain the demographic characteristics of the respondents and SEM results.
Demographic characteristics of respondents
Table 1 presents the demographic characteristics of the respondents. Particularly, 52.1% of the respondents were women, and the remaining 47.9% were men. Most respondents (37.2%) reported having a bachelor's degree, followed by a diploma (20.0%), high school certificate (20.6%), master's degree (19.1%), and PhD (2.1%). Additionally, most respondents were between 40 and 49 years (91.8%), and the rest were above 50 (8.2%). In terms of monthly income, 26.3% of the respondents reported earning a monthly income between CNY 2001 and CNY 4,000, followed by CNY 4001 and CNY 6000 (22.1%), CNY 2000 (16.8%), CNY 6001 and CNY 8000 (14.5%), CNY 10,000 (12.8%), and CNY 8001 and CNY 10,000 (7.6%). Approximately 83% of the total respondents reported purchasing IoT-enabled products, and 51.1% of the total respondents indicated using IoT-enabled WHDs.
Demographic characteristics.

Note: 1 USD = 7.25 CNY (Chinese Currency), WHDs: IoT-enabled Wearable Healthcare Devices.
Common method bias (CMB)
Harman's single-factor test confirms that a single component explained 49.23% of the total variation and did not exceed the 50% threshold recommended by Podsakoff et al. 103 In other words, CMB was not an issue in this study. Moreover, as Kock 104 has recommended, this study conducted a full collinearity test (see Table 2) for all model components. The results revealed that all values of the variance inflation factor ranged from 1.053 to 2.873, which did not exceed the maximum threshold value of 3.3, as specified by Kock, 104 thus confirming a lack of CMB.
Full collinearity test.

Note. HV: Health values, HM: Health motivation, PHB: Personal health beliefs, AOC: Awareness of consequences, AOR: Ascription of responsibility, PNs: Personal norms, SNs: Social norms, PPV: Perceived product value, IWHD: Intention to adopt IoT-enabled WHDs, AWHD: Actual adoption of IoT-enabled WHDs.
Source. Author's own data analysis.
Multivariate normality, internal consistency and convergent validity
The multivariate normality results showed that the multivariate kurtosis and skewness p-values were lower than 0.01, indicating the nonnormality of the data. 105 The internal consistency and convergent validity of the model components were evaluated using Dijkstra-Hensele's ρ, Cronbach's α, and composite reliability, with values exceeding the threshold value of 0.70, indicating significant internal consistency and reliability. 93 The results in Table 3 demonstrate that the values of more than 0.7 for all components. These results indicate the robust reliability and internal consistency of the model. Additionally, Hair et al. 92 suggested that the values of average variance extracted (AVE) should exceed 0.5 to ensure that the model and its components possess strong convergent validity. Referring to Table 3, the AVE values range from 0.600 to 0.804, thus confirming significant convergent validity.
Validity and reliability.
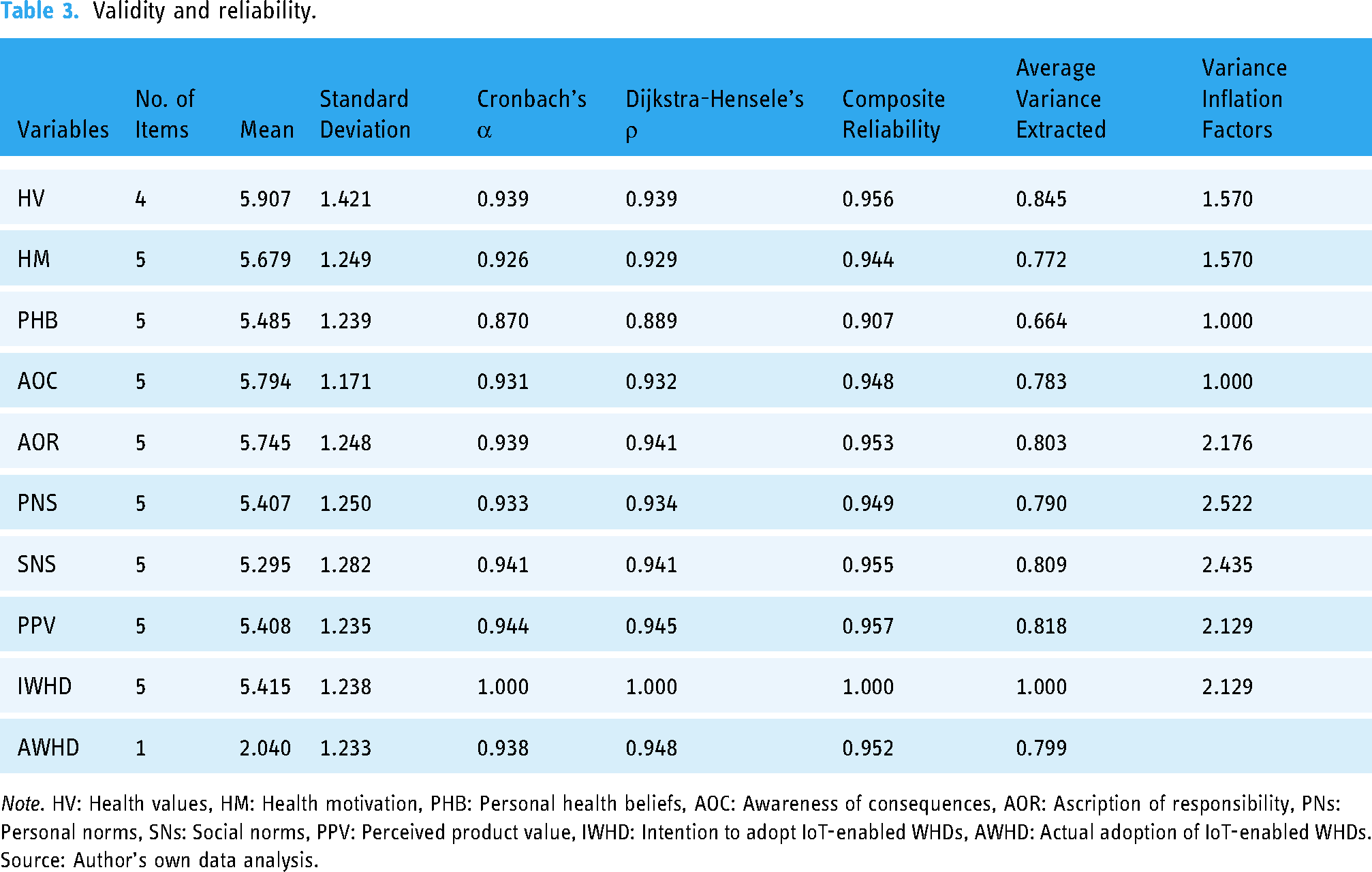
Note. HV: Health values, HM: Health motivation, PHB: Personal health beliefs, AOC: Awareness of consequences, AOR: Ascription of responsibility, PNs: Personal norms, SNs: Social norms, PPV: Perceived product value, IWHD: Intention to adopt IoT-enabled WHDs, AWHD: Actual adoption of IoT-enabled WHDs.
Source: Author's own data analysis.
Discriminant validity
The Fornell–Larcker criterion, heterotrait-monotrait (HTMT) ratio, and cross-loadings were used to obtain a comprehensive description of the model's discriminant validity. As shown in Table 4, the recorded values of the Fornell-Larcker criterion (in bold font) exceeded the recorded correlations. According to Henseler et al., 106 to achieve strong discriminant validity, all HTMT values should be lower than 0.85. The results in Table 4 demonstrate that the HTMT values (ranging from 0.069 to 0.777) for all the constructs met the criterion. Finally, as shown in Table 5, all factor loadings (in bold and italics) ranged from 0.629 to 1.00, meeting the stipulated criterion. 107
Discriminant validity.
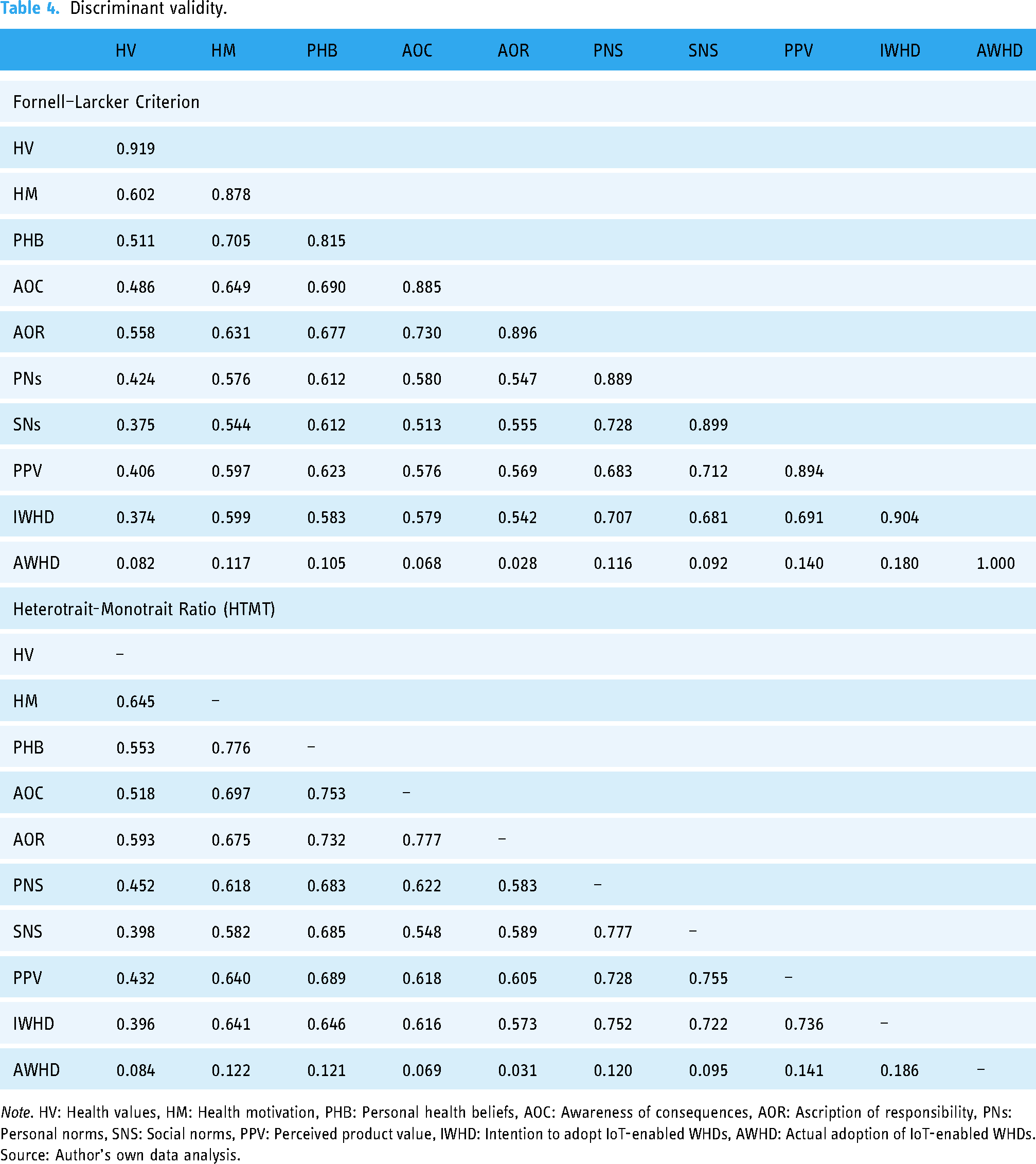
Note. HV: Health values, HM: Health motivation, PHB: Personal health beliefs, AOC: Awareness of consequences, AOR: Ascription of responsibility, PNs: Personal norms, SNS: Social norms, PPV: Perceived product value, IWHD: Intention to adopt IoT-enabled WHDs, AWHD: Actual adoption of IoT-enabled WHDs.
Source: Author's own data analysis.
Loading and cross-loading.

Note. HV: Health values, HM: Health motivation, PHB: Personal health belief, AOC: Awareness of consequences, AOR: Ascription of responsibility, PN: Personal norm, SN: Social norms, PPV: Perceived product value, IWHD: Intention to adopt IoT-enabled WHDs, AWHD: Actual adoption of IoT-enabled WHDs.
Source: Author's own data analysis.
Hypothesis testing
Based on the results presented in Table 6 and Figure 3, HVs significantly positively influenced PHBs (β = 0.135, t = 2.620, p = .005). In other words, H1 was supported. Likewise, H2 was supported. Health motivation exhibited substantial positive influence on PHBs (β = 0.624, t = 13.625, p = .000). The results further confirmed the significant and favorable influence of PHBs on both awareness of consequences (β = 0.690, t = 23.616, p = .000) and PNs (β = 0.589, t = 15.862, p = .000). Thus, H3a and H3b were supported. Furthermore, awareness of consequences significantly influenced the AOR (β = 0.730, t = 21.296, p = .000) and PNs (β = 0.331, t = 5.095, p = .000). Thus, H4a and H4b were accepted. Concurrently, AOR exhibited a substantial positive influence on personal norms (β = 0.131, t = 2.056, p = .020), confirming H5. Additionally, PNs (β = 0.450, t = 7.682, p = .000) and SNs (β = 0.353, t = 5.773, p = .000) exhibited significant and favorable influences on IWHD. In other words, H6 and H7 were accepted. Finally, IWHD had a considerable positive influence on AWHD (β = 0.161, t = 2.737, p = .003). Thus, H8 was verified.

Final model.
Hypothesis testing.

Note. HV: Health values, HM: Health motivation, PHB: Personal health beliefs, AOC: Awareness of consequences, AOR: Ascription of responsibility, PNs: Personal norms, SNs: Social norms, PPV: Perceived product value, IWHD: Intention to adopt IoT-enabled WHDs, AWHD: Actual adoption of IoT-enabled WHDs.
Source: Author's own data analysis.
Coefficient of determination (R2)
The coefficient of determination (R2) denotes the degree of explained variance or, in other words, the proportion of variation in the dependent variable explained by a linear model. Endogenous latent variables that were significant, moderate, or weak record R2 of 0.75, 0.50, and 0.25, respectively. 93 Table 7 presents the recorded values of R2 of the endogenous constructs. PHBs recorded R2 of 0.507 suggesting that HVs and HM as exogenous constructs explained 50.7% of the total variation in PHBs (moderate explanatory power). Similarly, the remaining constructs in this study demonstrated moderate to poor explanatory power: PNs (R2 = 0.426), AOC (R2 = 0.475), AOR (R2 = 0.531), IWHD (R2 = 0.557), and AWHD (R2 = 0.027).
Coefficient of determination (R2).

Note: R2 value interpretation (≥0.75—significant, ≥0.50—moderate, ≥0.25—weak). 93
Source: Author's own data analysis.
Effect size (f2)
Effect size (f2) measures the significant influence of exogenous factors on endogenous variables based on a particular variance instead of their shared variance. 92 Cohen 107 classified the effect size as trivial (<0.02), minor (≥0.02), medium (≥0.15), and substantial (≥0.35). However, it may be difficult to guarantee that the rules of thumb are adequate to produce a large effect size because they vary depending on the characteristics of the research framework and domain of interest. 92 Table 8 presents the results of the effect size evaluation. PHBs and AOC significantly affected AOC and AOR, respectively. Meanwhile, AOR and IWHD were identified as exhibiting trivial effects on PNs and the AWHD, respectively. The results further demonstrated the medium effect of HM on PHBs and the medium effect of PNs on IWHD.
Effect Size (f2).

Note 1. HV: Health values, HM: Health motivation, PHBs: Personal health beliefs, AOC: Awareness of consequences, AOR: Ascription of responsibility, PNs: Personal norms, SNs: Social norms, PPV: Perceived product value, IWHD: Intention to adopt IoT-enabled WHDs, AWHD: Actual adoption of IoT-enabled WHDs.
Note 2. f2 score interpretation (≥0.35—substantial effect size, ≥0.15— medium effect size, ≥0.02—small effect size, and <0.02—trivial effect size). 108
Source Author's own data analysis.
Predictive relevance (Q2)
The Q2 test determines whether exogenous factors outperform endogenous ones in terms of predictive power. 92 To determine the predictive relevance of the exogenous variables for the endogenous variables, the value of Q2 must be greater than zero. 92 The results in Table 9 show that all endogenous constructs in this study attained predictive relevance (Q2 > 0), suggesting the strong predictive power and validity of the model.
Predictive relevance (Q2).

Note. Q2 > 0 is significant. 92
Source: Author's own data analysis.
Moderating effect
As part of the research framework, perceived product value was postulated as a moderating variable in the relationship between the intention to adopt IoT-enabled WHDs and their actual adoption. A bootstrapping approach was used to examine the moderating effect of perceived product value. The results in Table 10 reveal no moderating effect on the perceived product value (nonsignificant p-value = .439).
Moderation effect.

Note. PPV: Perceived product value, IWHD: Intention to adopt IoT-enabled WHDs, AWHD: Actual adoption of IoT-enabled WHDs.
Source: Author's own data analysis.
Indirect effects
In addition to the direct effects of constructs, indirect effects should be explored to comprehensively comprehend the relationships among the constructs. 93 Table 11 presents the results of the indirect effects of all the constructs in this study. HVs have significant positive indirect effects on AOC (β = 0.093, p < .01), AOR (β = 0.068, p < .01), PNs (β = 0.080, p < .01), IWHD (β = 0.036, p < .01), and AWHD (β = 0.006, p < .05), whereas HM shows substantial positive indirect effects on AOC (β = 0.431, p < .01), AOR (β = 0.314, p < .01), PNs (β = 0.368, p < .01), IWHD (β = 0.165, p < .01), and AWHD (β = 0.027, p < .01). Similarly, PHB exhibits notable positive indirect effects on PNs (β = 0.229, p < .01), AOR (β = 0.504, p < .01), IWHD (β = 0.265, p < .01), and AWHD (β = 0.043, p < .01), while AOC has a significant positive indirect effect on PNs (β = 0.096, p < .05), IWHD (β = 0.149, p < .01), and AWHD (β = 0.024, p < .01). AOR shows a positive indirect effect on IWHD (β = 0.059, p < .05) but not with AWHD (β = 0.009, p > .05). PNs have a positive indirect effect on AWHD (β = 0.072, p < .01), while SNs demonstrate a positive indirect effect on AWHD (β = 0.057, p < .05).
Indirect effects.
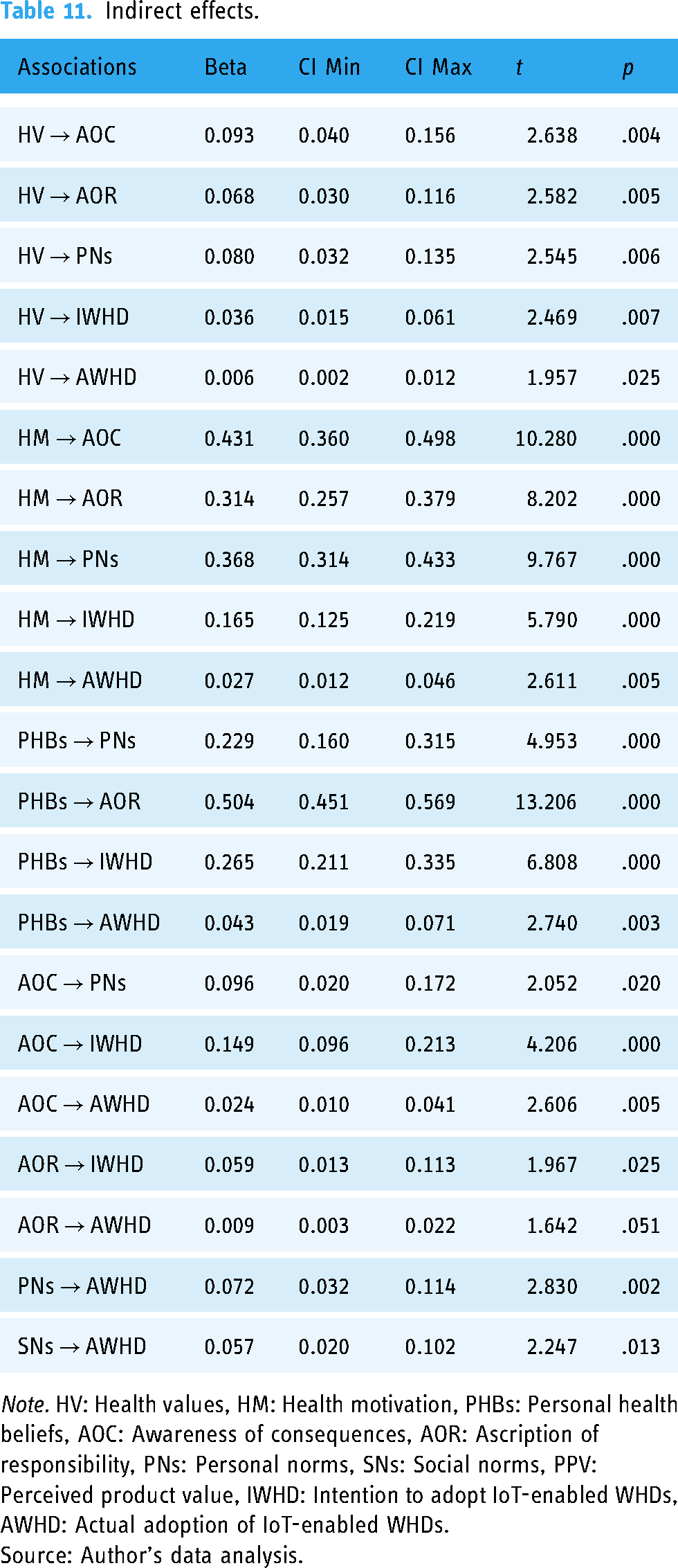
Note. HV: Health values, HM: Health motivation, PHBs: Personal health beliefs, AOC: Awareness of consequences, AOR: Ascription of responsibility, PNs: Personal norms, SNs: Social norms, PPV: Perceived product value, IWHD: Intention to adopt IoT-enabled WHDs, AWHD: Actual adoption of IoT-enabled WHDs.
Source: Author's data analysis.
Multigroup analysis (MGA)
The model was subsequently assessed using MGA for further in-depth evaluation and comprehension. PLS-MGA analyzes group heterogeneity and is one of the most effective methods for evaluating the influence of a moderating variable in multiple associations rather than just a single association. 92 Measurement invariance was established before performing PLS-MGA to confirm the validity of the effects. The measurement invariance of composite models’ approach was employed to test the measurement invariance for the two groups in this study.
The data involving male and female respondents were initially examined for measurement invariance (Group 1: male; Group 2: female). Both configurable and compositional variances were shown, validating the partial invariance of the measurement items. The permutation p-values for all factors exceeded .05, confirming measurement invariances. This study analyzed the results of the gender path coefficient from the PLS-MGA. As shown in Table 12, the results revealed that all recorded p-values of the group differences exceeded .05. Therefore, the results for these two gender groups indicated no statistically significant differences in any correlation.
Multigroup analysis—gender.

Note. HV: Health values, HM: Health motivation, PHB: Personal health beliefs, AOC: Awareness of consequences, AOR: Ascription of responsibility, PNs: Personal norms, SNs: Social norms, PPV: Perceived product value, IWHD: Intention to adopt IOT-enabled WHDs, AWHD: Actual adoption of IOT-enabled WHDs.
Source: Author's own data analysis.
Discussion
This study employed the VBN model to assess the relationship between HVs and HM with PHBs; PHBs with AOC; AOC with AOR; PHB, AOC and AOR with PNs; PNs and SNs with IWHD; and IWHD with AWHD. The moderating role of perceived product value in the hypothesized relationships between the constructs was also examined. All direct and indirect effects of the constructs in the proposed model were statistically significant and positive. Furthermore, this study found that perceived product value exhibited a nonsignificant moderating effect on the relationship between IWHD and AWHD. In light of the findings of earlier studies, logical interpretations of the results obtained are thoroughly discussed below.
HVs were found to have a significant impact on PHBs. Lee and Lee 35 and Hossain et al. 29 presented similar findings, establishing the vital role of HVs in the adoption of IWHDs. This implies that individuals have become increasingly health conscious and prioritize a healthy lifestyle. This study also shows that individuals assess healthcare monitoring tools to enhance health support benefits in illness prevention. HM has a significant and positive influence on PHBs, which is consistent with the findings of several previous studies.67,68 These results indicate that individuals who adopt self-care practices and have strong health motivations are likelier to have strong personal beliefs regarding using IoT-enabled WHDs for health tracking.
Based on these results, PHBs were found to have favorable individual relationships with the AOC and PNs. These findings are consistent with previous studies on the adoption of WHDs.34,36 This shows a preference for adopting IWHDs for consistent health monitoring. Such PHBs may inspire individuals to know the severe ramifications of illness burdens and hospitalization expenditures. Consequently, AOC and AOR were found to significantly influence personal norms. These findings agree with those reported by Shanka and Kotecho 37 regarding adherence to COVID-19 preventive measures. In other words, individuals who were aware of the detrimental consequences of unhealthy lifestyle habits and NCDs were more likely to feel morally obliged and intuitively responsible for monitoring their health and implementing appropriate initiatives.
Another noteworthy finding of this study is the substantial and favorable influence of personal and social norms on the intention to adopt IoT-enabled WHDs. Earlier studies in the context of IoT and mobile healthcare have validated these findings.35,42,84 In other words, individuals who feel morally responsible for caring for their own health and fitness and those exposed to the burden of disease and hospitalization costs are more likely to demonstrate a strong willingness to adopt IoT-enabled WHDs. Simultaneously, SNs play an active role in promoting the intention to adopt IoT-enabled WHDs, considering that individuals are more inclined to follow societal trends and are encouraged by the healthy lifestyles of significant others.
The results further demonstrate the positive influence of the intention to adopt IoT-enabled WHDs on actual adoption. Princi and Krämer 42 report similar findings in the context of IoT healthcare equipment. Another critical observation of this study is that the indirect effects of all associated constructs are statistically significant and positive, except for the relationship between AOR and AWHD. Based on these findings, it is plausible that individuals with a strong intention of adopting IoT-enabled WHDs are more likely to be apparent users. Additionally, all extrinsic and intrinsic healthy life-related values, beliefs, and norms play influential roles in the decision-making process of adopting IoT-enabled WHDs.
Interestingly, this study found that perceived product value exhibited a nonsignificant moderating effect on the relationship between IWHD and AWHD. Beh et al. 33 reported similar findings in the context of smartwatches in healthcare monitoring. However, Princi and Krämer 42 and Hasan et al. 64 reported otherwise. One possible explanation for these findings is that IoT-enabled WHDs are still new in the marketplace and have not yet been completely implemented. Consequently, respondents were unable to relate product value to anticipated advantages. Another probable explanation is that older adults over the age of 40 are generally not highly tech savvy, making it difficult for them to fully realize the benefits of adopting IoT-enabled WHDs.
In the case of indirect effects, all hypothesized relationships were statistically significant and positive, except for the indirect effect of AOR on AWHD. This indicates that HVs, HM, PHBs, AOC, PNs, and SNs significantly influence indirectly both the intention to adopt and the actual adoption of IoT-enabled WHDs. These findings highlight the importance of considering various psychosocial and motivational factors when designing interventions to encourage the adoption of such devices in healthcare contexts.
Finally, the results of the multigroup analysis revealed no significant differences in AWHD between male and female respondents. The apparent reason for such an outcome is that the relevance of health status monitoring does not necessarily depend on any particular gender because any individual can be health conscious and desire to live healthily. Both men and women have values, beliefs, and norms that minimize the significant repercussions of health disorders, driving them to take appropriate on-time measures for their health improvement through self-monitoring.
Implications
Theoretical implications
This research offers several theoretical implications. First, this study explores an underexploited conceptual foundation within the context of IoT-enabled WHDs and establishes a theoretical framework that contributes to the existing literature on technology adoption behavior. Most prior studies have focused on the technical aspects of IoT and its applications, and this study extends this knowledge by conceptualizing both the intrinsic and extrinsic elements of IoT adoption in health monitoring to interpret users’ decision-making processes. Second, this study integrates theories from both the technological adoption and health behavior domains, providing a holistic framework for understanding the adoption of IoT-enabled WHDs. By bridging these theoretical perspectives, the study offers a nuanced understanding of the factors influencing adoption behavior, thereby contributing to the interdisciplinary literature on technology adoption and health behavior change.
Third, this study extends the VBN model's applicability to the context of IoT-enabled WHD adoption among older adults in China. The current study adds three new factors to the VBN model: HVs, HM, and PHBs. It does this by looking at the use of IoT-enabled WHDs to learn more about how health monitoring affects maintaining a healthy lifestyle. By incorporating factors, the study provides a comprehensive framework for understanding the complex decision-making processes involved in the adoption of such devices. Fourth, this study contributes to the existing literature by demonstrating the effective application of the extended VBN model. This study empirically shows the proposed expanded VBN model for senior adults in the context of adopting IoT-enabled WHDs in developing countries like China.
Fifth, the study's findings validate several relationships proposed by the VBN model. For instance, the positive relationships between HVs and PHBs, HM and PHBs, PHBs and AOC, and AOC and AOR are supported. This contributes to the empirical validation of the theoretical foundations of the VBN model in the context of IoT-enabled WHD adoption. Sixth, the study helps us understand the connection between behavioral intentions and actions by showing that the intention to adopt IoT-enabled WHDs is a strong predictor of actual adoption behavior. This finding underscores the importance of fostering positive intentions as a precursor to actual adoption, highlighting the need for interventions aimed at shaping individuals’ attitudes and perceptions towards these devices.
Practical and managerial implications
Based on this study's findings, several practical and managerial implications benefit marketers, practitioners, and policymakers in effectively utilizing significant factors that either favor or hinder the adoption of IoT in the healthcare field. This study empirically demonstrates that HVs and HM are important drivers of developing PHBs when adopting IoT-enabled WHDs. Based on these findings, marketers should rigorously promote the benefits of regular health monitoring using IoT-based devices through strategic promotional campaigns. Additionally, to highlight the advanced features of IoT-enabled healthcare devices, practitioners may provide users with special service offerings, such as dietary assistance, medication guidelines, and emergency treatment packages. Furthermore, IT providers should target certain user groups to instill feelings of care and a sense of comfort and stimulate their values for health-monitoring practices through the adoption of the IoT. Simultaneously, government agencies may use social media and other forms of media to convey more authoritative and strategic service information and raise users’ moral standards for high-quality medical and healthcare services. Healthcare organizations should also emphasize that the adoption of IoT-enabled healthcare devices to analyze health status allows physicians to provide contactless treatment in real-time. 5
Additionally, this study empirically exhibits the significant influence of PHBs on the awareness of consequences and personal norms. Considering these findings, providers should highlight the special features of IoT-enabled WHDs and services in developing these products, such as the early detection of critical illnesses, direct medical consultation upon detection of abnormalities, and emergency medical assistance. In fact, prompt incident management features may aid users in developing healthy perceptions and rationally adopting these devices. Furthermore, maintaining consistency in the claims of distinctive attributes of IoT devices in healthcare may strengthen users’ dependability on products and services and induce a strong attachment to these products and services. Consequently, maintaining stringent quality standards is critical for organizations to gain and maintain users’ PHBs when adopting IoT-enabled WHDs. Concurrently, government authorities should launch educational programs and public awareness campaigns to promote the benefits of IoT healthcare devices for the aged population, who are increasingly at risk of reliance, disabilities, and chronic medical conditions, as well as to raise users’ morale in support of healthy aging. Marketing professionals and brand practitioners should also consistently emphasize and reinforce the fact that IoT-based health monitoring can help users’ family members (especially the elderly) lead healthier lifestyles, thereby raising their optimistic views about regular health monitoring.
Considering the significance of social norms as one of the key factors influencing the intention to adopt IoT-enabled WHDs, knowledge alone may not be adequate to persuade users to embrace this technology if they cannot recognize the social recommendations of these alleged benefits. Advertisers and practitioners should provide relevant details on the integrated features and services of IoT-enabled healthcare devices to ensure that their claims for healthcare monitoring-related benefits are substantiated. The adoption of IoT-enabled WHDs can be widely regarded as dependable when renowned hospitals, medical service providers, and government regulatory authorities endorse the related products and services. Marketers may also consider offering multiple packages and discounts to early adopters, who may serve as real-life examples and references to build strong word-of-mouth and widespread positive reviews regarding the use of IoT-enabled WHDs. Furthermore, IoT providers and marketers should collaborate with non-profit social activist groups and a range of social media communities to increase user awareness of the rising incidence of NCDs and rehabilitation costs. Finally, the government and policymakers may consider imposing explicit standards and certifications and implementing a constant monitoring system to guarantee that the developers and producers of these products and services meet quality standards at all times.
Conclusion
The framework of this study emphasizes the core aspects that promote the intention to adopt IoT-enabled WHDs and elaborates on essential individual values, beliefs, and norms in such technology adoption among Chinese senior adults. Moreover, this study addresses substantial gaps in the literature by examining the socio-psychological aspects that influence individuals’ decisions to adopt IoT-enabled WHDs. The empirical findings supported all hypotheses as well as all projected indirect effects of related constructs. This study empirically demonstrates the need for manufacturers and markets to prioritize the influence of diverse individuals’ HVs, HM, PHBs, SNs, and PNs on practical adoption behavior to satisfy different user demands. Lastly, to achieve national public health and sustainability goals, the government and policymakers should establish specific guidelines and implement a proper monitoring strategy to ensure that all stakeholders can reap the benefits of this novel technology and its related services.
This study has a few limitations. First, the data was acquired from a few IoT-enabled device users in China, which may limit the generalizability of the proposed model to other contexts. Therefore, future studies should gather data from larger samples with diverse demographic characteristics and from different localities. This can help improve insights into the adoption of IoT-enabled WHDs and enhance the generalizability of the proposed model. Second, this study examined only a few aspects associated with values, beliefs, and norms, and it is possible that other essential factors, such as technology acceptance, were overlooked. To improve existing understanding, future studies should take into account additional context-specific elements such as perceived privacy, cost and affordability, trust in technology and providers, and security. Third, this study employed a cross-sectional approach, which limited the behavioral evaluation analysis over time. Hence, future research should employ a longitudinal approach to analyze the long-term effects of these factors and their related associations over time. Finally, to fill the intention-behavior gaps, the study examined moderating factors such as perceived product value between intention and actual behavior. Unfortunately, it turned out to be insignificant. Future research could investigate this moderating variable in other settings and come up with new moderating variables, such as technology literacy, socioeconomic status, and cultural norms, to provide a more nuanced understanding of adoption behavior.
Contributorship
Qing Yang and Farzana Naznen: Conceptualization, investigation, methodology, and writing—original draft preparation. Abdullah Al Mamun and Mengling Wu: Conceptualization, methodology, formal analysis, and writing—review and editing.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241279199 - Supplemental material for Strengthening health monitoring: Intention and adoption of Internet of Things-enabled wearable healthcare devices
Supplemental material, sj-docx-1-dhj-10.1177_20552076241279199 for Strengthening health monitoring: Intention and adoption of Internet of Things-enabled wearable healthcare devices by Qing Yang, Abdullah Al Mamun, Mengling Wu and Farzana Naznen in DIGITAL HEALTH
Supplemental Material
sj-csv-2-dhj-10.1177_20552076241279199 - Supplemental material for Strengthening health monitoring: Intention and adoption of Internet of Things-enabled wearable healthcare devices
Supplemental material, sj-csv-2-dhj-10.1177_20552076241279199 for Strengthening health monitoring: Intention and adoption of Internet of Things-enabled wearable healthcare devices by Qing Yang, Abdullah Al Mamun, Mengling Wu and Farzana Naznen in DIGITAL HEALTH
Footnotes
Declaration of conflicting interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical approval
The research ethics committee of Changzhi University, China have approved this study (Approval Number: CZ-2022-0006). This study has been performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from respondents who participated in the survey.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Abdullah Al Mamun (Corresponding Author).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.