
Abstract
Objective
The study aims to investigate how wearable fitness devices (WFDs) influence health-promoting behavior in the Chinese context, particularly by examining two distinct affordances—health technician affordance and health consultant affordance—derived from affordance theory.
Methods
Drawing on affordance theory and integrating health communication and technology models (including Unified Theory of Acceptance and Use of Technology, Protection Motivation Theory, Technology Acceptance Model, Theory of Planned Behavior, Social Cognitive Theory, and Pender's Health Promotion Model), we developed a theoretical model that incorporates three mediators relevant to individual technology use. We collected 615 valid responses through a questionnaire survey across China via QR codes and links on social platforms, and used SPSS and SmartPLS for data analyzing to validate our research model.
Results
Our findings indicate that performance expectancy and exercise self-efficacy are positively associated with health-promoting behavior. Moreover, the relationship between both health technician and health consultant affordances and health-promoting behavior is mediated by performance expectancy and exercise self-efficacy. In addition, prior exercise behavior significantly influences health-promoting behavior.
Conclusion
The study advances our understanding of how WFDs contribute to health-promoting behavior by delineating both the technical and consultative roles of these devices. The results provide important theoretical insights and practical implications for enhancing health communication strategies and optimizing the use of wearable fitness technology.
Keywords
Introduction
Health-promoting behavior is defined as “proactive responses to the environment that enable individuals to achieve a higher level of health.”1 Originally proposed by Pender and Pender2 this concept encompasses activities such as regular physical exercise and comprehensive health management, aiming to maintain and enhance overall wellbeing rather than addressing specific diseases. In the postpandemic era, individuals, particularly in China, are increasingly engaging in various activities to stay healthy. The traditional Chinese practice of “regimen” or “Yangsheng,” once popular among the elderly, is now gaining traction among younger generations who are adopting healthy diets and physical activity regimens. 3 According to a survey by i-Research, 3 about 43.3% of millennials and 37.9% of Gen Z engage in regular health-promoting behaviors, such as daily physical activities like jogging and aerobic exercises.
As individuals engage in health-promoting behaviors, wearable fitness devices (WFDs) have become popular tools for tracking biometric data, seeking exercise feedback, and planning future regimens. WFDs, including smartwatches and fitness bands, 4 provide technological affordances that support users in achieving their health goals, thereby significantly and positively intervening in the formation of healthy exercise behaviors. 5 The function of WFDs is similar across cultures, as they serve as tools to monitor health and provide personalized feedback. However, in China, WFDs have seen widespread adoption, with the shipment rate of wearable devices steadily increasing since 2023. 6 In the first-quarter of 2024, shipments of wearable devices reached 33.7 million units, with the smartwatch market growing by 54.1% year-on-year and the wristband market growing by 29.6% year-on-year. 7 Given the high prevalence of WFD usage in China, examining how these devices influence health-promoting behaviors within this population can serve as a representative example. The findings from our study conducted in the Chinese context may provide insights that could be relevant to other sociocultural settings, as further research explores how WFDs impact health behaviors in different populations.
Despite the widespread use of WFDs and the increasing engagement in health-promoting behaviors in China, systematic scholarly research on this phenomenon is lacking. Existing literature tends to focus on affordances from a user design perspective, emphasizing customization, and personalization. 8 However, the specific affordances of smartwatches and their impact on users' health-promoting behaviors have not been thoroughly investigated. With advancements in smart technology, users are more inclined to engage in activities independently, necessitating an exploration of individual users' interpretations of technological affordances. Smart technology, such as WFDs, enables users to self-monitor and manage their health-related activities more effectively, fostering a more personal and reflective interaction with the technology. This shift highlights the need to understand how individuals perceive and utilize these affordances on a personal level. Additionally, while perceived performance, effort expectancy, and self-efficacy have been extensively studied within the framework of health communication, their roles as mediators between technology affordance and health-promoting behavior remain underexplored. Understanding these mediating mechanisms can provide deeper insights into the processes and effectiveness of health-promoting behaviors.
This study contributes to the health communication literature by conceptualizing the unique affordances of WFDs, specifically “health technician affordance” (HTA) and “health consultant affordance” (HCA), which enhance users' self-efficacy and health-promoting behaviors. Drawing on Gibson's affordance theory and the extended work introduced by other researchers, this research explains how WFDs function both as tools for health management (HTA) and as interactive guides offering personalized feedback (HCA). Current literature on affordance tends to mainly focus on the “technical side” of affordances, and might overlook the potential of devices to serve as virtual consultants. In contrast, our study attempts to unify the “technological” affordance and the “virtual expert or consultant” affordance by distinguishing between their “technical possibilities” (technology-side) and their “guidance” potential (human-side), thus expanding the current understanding of affordance.
Furthermore, our study integrates and applies theories of human–technology interaction, including Unified Theory of Acceptance and Use of Technology (UTAUT), Protection Motivation Theory (PMT), Technology Acceptance Model (TAM), Theory of Planned Behavior (TPB), Social Cognitive Theory (SCT) and Pender's Health Promotion Model (PHPM), to provide a comprehensive understanding of how WFDs influence health behaviors. These theories address users' perceptions of usefulness, ease of use, self-efficacy, and control. By integrating these models, this study explores how HTA and HCA drive health-promoting behaviors, offering practical implications for manufacturers, health professionals, and policymakers in optimizing WFDs to support health behavior change.
Theoretical conceptualization and hypotheses development
Conceptualizing health affordances in WFDs
Affordance refers to the human perception of the utility of an object,9,10 defined as “a relationship between the properties of an object and the capabilities of the agent that determine just how the object could possibly be used.” 11 Affordances vary among individuals based on how they interpret the qualities of the object and perceive its potential uses. 10 In the context of technology, affordance is a user's subjective interpretation of the functions of a given technology and perceptions about what the technology enables them to do. 10 Wearable technologies are lightweight devices designed to provide technical solutions and act as embodied companions that become extensions of the self. 4
Building on the understanding of affordances in information technology, Luo and Yang 8 examined affordances in IT-based self-monitoring (ITSM) functionalities, categorizing them into customization and personalization affordances. They classified preparation and data collection as customization affordances, and reflection and social connection as personalization affordances, with these conceptualizations primarily proposed from the perspective of business design interfaces for smartwatches. Expanding upon this framework, we incorporate the concept of IT guidance affordance, as introduced by Zhang et al., 12 to explore the role of WFDs in health communication, particularly in health promotion and activation. Grounded in Gibson's affordance theory, 9 which emphasizes the actionable possibilities offered by an object's properties, we argue that wearable technologies can be understood through two distinct affordances: health technician affordance and health consultant affordance.
Health technician affordance refers to the device's inherent technological features, such as goal setting and systematic data collection, which enable users to engage in precise self-monitoring. These capabilities empower users to track and measure their health metrics, supporting objective health management. In contrast, health consultant affordance reflects the device's guidance dimension, enabling it to provide personalized feedback and foster an interactive connection with the user. This consultative role allows the device to help users interpret their data, make informed health decisions, and engage in sustained health-promoting behaviors. By combining both the functional and guidance roles, WFDs serve a dual purpose: they not only collect and process data but also offer expert-like guidance, supporting users in managing their health in a comprehensive and personalized manner (see Figure 1).

HTA (left) and HCA (right) interactive interface. HCA: health consultant affordance; HTA: health technician affordance.
Health technician affordance specifically refers to the technological capabilities embedded in WFDs. 13 This affordance enables users to set tailored exercise goals and develop precise health plans, while also facilitating the continuous tracking and accurate recording of biometric data. In this context, the “preparation” function involves configuring the device to align with personal health objectives, and the “data collection” function ensures that detailed physiological metrics are captured in real time. This affordance enables users to set personalized exercise goals and develop tailored health plans while facilitating continuous tracking and precise recording of biometric data.8,13 In this context, the “preparation” function involves configuring the device to align with personal health objectives, while the “data collection” function ensures that detailed physiological metrics are captured in real time. These technical features emphasize the device's role as a reliable, objective tool for achieving specific health outcomes. The technological nature of health technician affordance is evident in the structured, data-driven processes that support these functions, highlighting the device's functionality and efficiency in tracking and managing health-related information.
Conversely, health consultant affordance reflects the device's capacity to function as a virtual health expert, translating raw data into actionable, personalized health insights.8,13 This affordance is expressed through two core functions: reflection and social connection. The “reflection” function allows the device to analyze and interpret the gathered data, providing users with customized feedback and actionable recommendations that guide health-related decisions. 14 Meanwhile, the “social connection” function reflects the dynamic, responsive relationship between the user and the device, where the device acts as a caring figure—offering expert-like advice and fostering a sense of trust and companionship. 14 This guidance affordance highlights how the device not only communicates information but also engages users in an intimate, advisory manner, enhancing their confidence and motivation to pursue health-promoting behaviors.
In our study, we examine the usage of WFDs, focusing on how users perceive these devices as extensions of themselves and as embodied companions. WFDs serve dual roles as health technicians and health consultants, offering both technical support and expert guidance, which ultimately enhances users' health management and promotes sustained engagement in health-promoting behaviors.
Integration of theoretical models
Our primary research question is to explain how WFDs influence health-promoting behavior, and to do so, we integrate several theoretical models—UTAUT, PMT, TAM, TPB, SCT, and PHPM. These theories specifically explore human–technology interactions, with TAM and UTAUT focusing on performance expectancy (perceived usefulness) and effort expectancy (ease of use), which are enhanced by both health technician and health consultant affordances. TPB emphasizes how perceived control over the technology influences behavior, linking effort expectancy with greater user engagement. SCT and PMT focus on self-efficacy, where both affordances increase users' confidence in their ability to perform health-related tasks, ultimately promoting sustained health behavior. Together, these models highlight the interrelated ways in which WFDs influence health-promoting behavior by addressing motivation, perceived value, ease of use, and self-confidence.
Affordance and performance expectancy
Performance expectancy refers to the degree to which an individual believes that using a system will help them achieve their performance goals. This concept is primarily derived from the perceived usefulness of the system, which is a key component of performance expectancy.
15
Health technician affordance offers users straightforward biometric data, thereby fulfilling their need to actively learn about their infometrics. This increased access to and understanding of their biometric data enhances the perceived usefulness of the WFDs, subsequently improving performance expectancy. Similarly, health consultant affordance provides users with feedback and health management suggestions, empowering them to effectively utilize health-related initiatives. This empowerment increases the perceived usefulness of the WFDs, further enhancing performance expectancy. Therefore, we propose the following hypotheses: H1a: Health technician affordance is significantly positively associated with performance expectancy. H1b: Health consultant affordance is significantly positively associated with performance expectancy.
Health promotion behaviors are defined as “proactive responses to the environment that enable individuals to achieve a higher level of health.” 1 Pender's and Pender 2 posit that these behaviors do not aim to address specific diseases or problems. Rather, they encompass activities such as regular physical exercise and comprehensive health management, which are undertaken to maintain and enhance individuals' overall wellbeing. Through these activities, individuals can ultimately achieve self-actualization and self-fulfillment. 1
Based on the Health Belief Model (HBM), an individual's decision to engage in health-related actions is influenced by their perception of the perceived threat of not taking action and the perceived benefits of taking action.
16
The greater the perceived net benefits, the more likely individuals are to engage in health-promoting behaviors. Performance expectancy, a key construct in the UTAUT model, refers to the perceived usefulness of a technology and the benefits it provides.
15
A useful device implies higher data quality, which can influence an individual's exercise performance through activity adequacy mindsets, leading to positive interventions in emotional states.
17
Previous studies have shown that the direct effect of the performance expectancy on habitual use of wearable devices was greater than that of intention to continue use,
18
indicates the crucial role of performance expectancy in fostering habit formation. When individuals perceive technological usefulness and anticipate positive outcomes from using such technologies, they are more likely to adopt behaviors that promote their health. Therefore, we propose the following hypothesis: H2: Performance expectancy is significantly positively associated with health promotion behavior.
Affordance and effort expectancy
Effort expectancy refers to the degree of ease associated with using a system, encompassing three key components: perceived ease of use, complexity, and ease of mastery. These components are interrelated and collectively contribute to the overall ease of use of the system. At its core, effort expectancy emphasizes the simplicity and user-friendliness of the technology. Scholars have categorized the interaction technology of wearable devices into two types: explicit interaction and implicit interaction. The former focuses on personal information consciously and voluntarily input by the user (e.g., previous health habits, goal setting, etc.), requiring higher levels of user attention and initiative. The latter, on the other hand, focuses on the intelligent analysis of unconscious bodily data, emotions, and perceptions, without relying on the user's active operation of the device. Health technician affordance improves perceived ease of use by delivering clear and easily accessible biometric data, thus simplifying the technology and lowering the learning curve. However, it presents autonomy challenges in explicit interactions such as goal setting and personalized program adjustments. In a similar vein, health consultant affordance boosts perceived ease of use by supplying intuitive feedback and health management advice, which further elevates effort expectancy, as it relies heavily on implicit interactions between the user and the device, requiring minimal user initiative.
Researchers have integrated the UTAUT and TTF (Task-Technology Fit) models to investigate the impact of technical characteristics on user acceptance. Their findings validate the significant influence of effort expectancy on usage intention and demonstrate that technical characteristics positively affect effort expectancy and contribute to TTF. In other words, improvements in a system's technical features can better align with users' complex task goals, enabling them to use the technology more effectively to meet their needs.
19
As a manifestation of technological affordance, when technical features reduce the difficulty of using the device, technological affordance positively impacts effort expectancy. Therefore, the following hypotheses are proposed: H3a: Health technician affordance is significantly positively associated with effort expectancy. H3b: Health consultant affordance is significantly positively associated with effort expectancy.
Effort expectancy, a key concept in the TAM, refers to “the degree of ease associated with the use of the system.” Users perceive the ease of using technology as an enabler for perceived control. According to the TPB, perceived control can increase the perceived behavioral control of users, which results in taking actions to achieve their goals.
20
This suggests that when individuals find a system easy to use, they feel more in control and are more likely to engage in behaviors that promote their health. Therefore, we propose the following hypothesis: H4: Effort expectancy is significantly positively associated with health promotion behavior.
Affordance and exercise self-efficacy
Exercise self-efficacy refers to an individual's belief in their ability to engage in exercise despite potential barriers such as fatigue, a busy schedule, or other constraints. Higher levels of exercise self-efficacy are associated with a greater likelihood of participating in physical activities. This concept is grounded in Bandura's SCT, which posits that self-efficacy beliefs influence motivation and behavior.21,22 According to this theory, personal, environmental, and behavioral factors interact through reciprocal mechanisms. Specifically, situational factors (environment) play a critical role in shaping individuals' self-efficacy perceptions. The more positive reinforcement provided by situational factors, the stronger the individual's belief in their ability to complete the task.
Health technician affordance creates an environment where users can manage their goals according to personal needs, fostering a sense of control and achievement. This process enhances exercise self-efficacy by enabling goal-setting, a key component of self-regulation that is crucial for maintaining motivation and achieving desired outcomes. 23 The tracking of activities enables of autonomy and confidence, and autonomy influences personal willingness to use health technologies. 24 By allowing users to monitor their progress and adjust their goals, health technician affordance reinforces a sense of control and accomplishment, thereby strengthening exercise self-efficacy.
Health consultant affordance provides an environment where users can receive feedback and health suggestions, encouraging them to engage more effectively in future exercises. This feedback mechanism not only enhances exercise self-efficacy but also provides guidance and support, helping users overcome obstacles and maintain their exercise routines. Such positive reinforcement further strengthens their belief in their ability to succeed. Therefore, we propose the following hypotheses: H5a: Health technician affordance is significantly positively associated with exercise self-efficacy. H5b: Health consultant affordance is significantly positively associated with exercise self-efficacy.
According to PMT, individuals' decisions to take action are related to their perceptions of threat appraisals, such as perceived vulnerability and perceived severity, and coping appraisals, such as response efficacy and self-efficacy.
16
Coping appraisals pertain to how individuals adopt coping responses to address threats or influencing factors, thereby increasing the likelihood of initiating an adaptive response, such as following behavioral advice.
25
The capability to perform the recommended behavior (self-efficacy) can significantly increase the probability of an adaptive response.
25
In the context of health promotion, exercise self-efficacy can be categorized as a perceived coping appraisal that enhances adaptive behavioral responses, leading to health promotion behavior. Therefore, we propose the following hypothesis: H6: Exercise self-efficacy is significantly positively associated with health promotion behavior.
The theoretical framework depicted in Figure 2 illustrates the analysis of how health technician and health consultant affordances impact health-promoting behaviors, mediated by expectancy and self-efficacy.

Theoretical model.
Method
Selection criteria
Our study deliberately focused on the core mechanisms underpinning health-promoting behavior by emphasizing the technological affordances of wearable fitness devices—specifically, HTA and HCA—and their impact via performance expectancy, effort expectancy, and exercise self-efficacy. This focus was guided by established theoretical frameworks (e.g., UTAUT, TAM, TPB, PMT, SCT, and PHPM), which highlight these individual-level constructs as key determinants in the context of self-monitoring technologies. Besides, previous studies found that the effect of the sharing feature on wearable devices does not significantly change with differences in autonomous motivation, indicating that the importance of social mechanisms, such as sharing with others, diminishes during the process of forming exercise habits. Therefore, we minimized the interference of such factors in our model and study. 26 Moreover, including these additional variables would have complicated the model without yielding clear theoretical or empirical benefits. We do acknowledge, however, that social influences are important in shaping health behaviors. As we'll note in the manuscript's limitations, future research should explore these factors more deeply to provide a more holistic view of health promotion.
Measurement
The multi-item scales used in this study are grounded in theoretical and empirical literature and have been validated by experts to ensure logical and rigorous item design. We then extracted and adapted items from previous validated measurement scales to create the survey for our study.
HTA and HCA are conceptualized as second-order reflective-formative constructs based on Luo et al., 8 with HTA and HCA being higher-order variables. HTA is formative with two dimensions: information preparation (original scale Cronbach's alpha = 0.742) and data collection (original scale Cronbach's alpha = 0.705), while HCA synthesizes the two lower-order dimensions of reflection (original scale Cronbach's alpha = 0.709) and social connection (original scale Cronbach's alpha = 0.782). All of the second-order variables are composed of three items each.
Four items that construct performance expectancy (original scale Cronbach's alpha = 0.844) and three items that construct effort expectancy (original scale Cronbach's alpha = 0.849) are mainly based on Venkatesh et al. 15 and Gao et al. 27 We added 1 item to the performance expectancy scale from Gao's version based on Venkatesh's original scale, aiming to better measure the usefulness of WFDs in enhancing health management opportunities.
Exercise self-efficacy was adapted from Kroll et al. 28 (original scale Cronbach's alpha = 0.828), we use five items to construct the variable, measuring the level of confidence and autonomy when individuals having physical exercise.
Based on the previous research from Walker and Hill-Polerecky, 29 four items were used for health-promoting behavior (original scale Cronbach's alpha = 0.793–0.872). We selected items from the original scale related to an individual's planning of exercise and engagement in activities of varying intensities, in order to comprehensively measure the formation of exercise habits. A higher score indicates a greater likelihood of practicing corresponding health-promoting behaviors.
Prior exercise behavior was included as a control variable. We referred to Oh's 30 measurement of prior habits using a single-item scale and adapted and expanded it based on the specific context of our research. This variable was measured from three aspects: individuals' exercise habits, exercise data tracking, and WFD usage habits for exercise, consisting of a total of three items.
All items above were graded on a 5-point Likert scale, with “1” denoting “strongly disagree” and “5” denoting “strongly agree.” Additionally, a pilot study was conducted with 90 WFDs users to enhance the measurement scales' construct validity and reliability. Due to the poor reliability of some variables after the pretest, we modified the wording of the questionnaire items to improve the quality of the subsequent data collection.
A health status scale and a prior exercise scale were used to assess personal health and exercise-related conditions. Moreover, demographic variables such as age, gender, income, and region were controlled to observe their potential impact on health promotion.
Participants and procedure
The questionnaire was distributed through two Chinese professional survey platforms: Wenjuanxing [https://www.wjx.cn/] and Diaoyanjia [https://www.surveyplus.cn/]. We shared the survey via QR codes and links on social platforms such as WeChat Moments and Weibo, as well as in several health communities and groups on social media. The questionnaire collection adhered to the principles outlined in Duncan 31 Declaration of Helsinki, ensuring the questionnaire data anonymized during collation and statistical analysis. All participants voluntarily filled out the questionnaire and were informed of and agreed to the purpose of the survey.
To ensure data quality, the first page of the questionnaire included a screening question: “Have you ever used a wearable fitness device?” Participants who answered “yes” proceeded to the subsequent questions, while those who answered “no” were considered invalid samples.
According to a report by Deloitte, 32 young people are more adept at discovering and using the health monitoring functions of smart devices. Over 60% of the 18 to 34 age group pay attention to their step count and heart rate, while this figure drops to about 50% among those aged 35 and above. Therefore, this study expanded the sample of Generation Z to obtain more representative data.
The survey was conducted from 8 January to 25 April 2024, and 833 questionnaires were received. Since our research focuses on the health behaviors of WFD users, samples without prior experience using WFDs were excluded, leaving a final sample of 654 that was consistent with the target population. Furthermore, to ensure the quality of the survey, we excluded responses with duplicate answers or high response consistency (e.g. selecting the same option for all questions). This resulted in 615 valid samples, leading to an effective response rate of 94%. Previous study indicated that having at least 10 cases per item is a reasonable target, with more complex models requiring larger samples. Our questionnaire have 31 measurement items in total, therefore, 615 valid samples are reasonable and worth analyzing. 33
Descriptive statistics show that all participants in our research were Chinese, and the gender and age distributions were balanced, as we applied quota sampling criteria based on Report on China's Fitness Industry by STYD. 34 The number of females slightly exceeded that of males, and more than 80% of participants were young and middle-aged individuals under 40. Furthermore, the income and regional distribution of the sample were also fairly even. This aligns with the conclusion in Deloitte's report regarding the enthusiasm of Chinese youth for physical monitoring, reflecting the principle of random and broad sampling (Table 1).
Descriptive statistical analysis of respondents.

WFD: wearable fitness device.
Results
Measurement model result
This study employed SPSS 26 for data organization, eliminating invalid items, and performing descriptive statistics. The data was then imported into SmartPLS 3 for reliability and validity tests, as well as structural equation modeling (SEM) analysis, yielding results such as model fit, path coefficients, and mediation effects. All analyses were conducted using the two-step approach recommended by Anderson and Gerbing 35 to evaluate the research model. The measurement model was assessed for reliability and validity of all first-order variables. The results indicated good reliability, with the Cronbach's alpha coefficients and composite reliability for all variables exceeding the standard of 0.7. The average variance extracted (AVE) values were greater than the standard of 0.5, indicating excellent convergent validity (see Table 2). Furthermore, the square root of the AVE for each construct was larger than the corresponding correlations, demonstrating reasonable discriminant validity (see Table 3).
Reliability and validity measurement.

A Cronbach's alpha and composite reliability above 0.7 indicate good reliability; factor loadings above 0.7 and an AVE greater than 0.5 indicate good convergent validity.
AVE: average variance extracted; CR: composite reliability; DC: data collection; EE: effort expectancy; ESE: exercise self-efficacy; HPB: health-promoting behavior; PE: performance expectancy; PR: preparation; RE: reflection; SC: social connection.
Discriminant validity Fornell-Larcker criterion.

A construct shows good discriminant validity if the square root of its AVE exceeds the corresponding correlations.
DC: data collection; EE: effort expectancy; ESE: exercise self-efficacy; HPB: health-promoting behavior; PE: performance expectancy; PR: preparation; RE: reflection; SC: social connection.
Given the distribution method of the questionnaire, common method variance might influence the analysis results. Harman's single-factor test indicated that the largest factor accounted for 38.66% of the total variance, below the 40% threshold, confirming no common method bias. The reflective-formative model analysis of HTA and HCA required a two-step analysis using the repeated indicators approach. The results indicated that the weights of first-order constructs were significantly weighted by the second-order formative constructs (p < 0.05), and the variance inflation factor (VIF) values for each variable were less than the recommended threshold of 3 (see Table 4), indicating no multicollinearity among the dimensions.
First- and second-order construct relationship.

A valid second-order variable should significantly load on first-order variables, with no multicollinearity present (VIF < 10).
DC: data collection; HCA: health consultant affordance; HTA: health technician affordance; PR: preparation; RE: reflection; SC: social connection; VIF: variance inflation factor.
Hypothesis testing
We use Smartpls for hypothesis testing. After processing with the PLS algorithm, we obtained the results of path coefficients for each hypothesis (Table 5), the coefficient of determination R2and effect size f2 (Table 6), the total indirect effects (Table 7), and the mediation effects (Table 8).
Direct effect hypothesis testing.

CI: confidence interval; EE: effort expectancy; ESE: exercise self-efficacy; HCA: health consultant affordance; HPB: health-promoting behavior; HTA: health technician affordance; LLCI: lower limit of the confidence interval; PE: performance expectancy; ULCI: upper limit of the confidence interval.
The explanatory power R2 and the effect size f2 of the model.

R2 value interpretation (≥0.75—significant, ≥ 0.50—moderate, ≥ 0.25—weak).
f2 value interpretation (≥0.35—substantial effect size, ≥ 0.15—medium effect size, ≥ 0.02—small effect size, and <0.02—trivial effect size).
EE: effort expectancy; ESE: exercise self-efficacy; HCA: health consultant affordance; HPB: health-promoting behavior; HTA: health technician affordance; PE: performance expectancy.
The total indirect effect of technological affordance.

When VAF < 20%, it is a no-mediation effect, when 20%≤VAF ≤ 80%, it is a partial-mediation effect, and when VAF > 80%, it is considered to be a full-mediation effect.
CI: confidence interval; HCA: health consultant affordance; HPB: health-promoting behavior; HTA: health technician affordance; LLCI: lower limit of the confidence interval; ULCI: upper limit of the confidence interval; VAF: Variance Accounted For.
The mediation effect of perception.

CI: confidence interval; EE: effort expectancy; ESE: exercise self-efficacy; HCA: health consultant affordance; HPB: health-promoting behavior; HTA: health technician affordance; LLCI: lower limit of the confidence interval; PE: performance expectancy; ULCI: upper limit of the confidence interval.
In the SEM model, when the p value of the path analysis results is less than 0.05 and the confidence interval (CI) does not include 0, the path can be considered significant. The R2 value is used to assess the model's explanatory power, ranging from 0 to 1. Endogenous latent variables with R2 values of 0.75, 0.50, and 0.25 are considered to have strong, moderate, or weak explanatory power, respectively. 36 The effect size, represented by f2, is classified as trivial (<0.02), minor (≥0.02), medium (≥0.15), and substantial (≥0.35). 36 Additionally, the Variance Accounted For (VAF) value is used to measure the mediation effect. When VAF is less than 20%, it is considered to have no mediation effect; when (20%≤VAF ≤ 80%), it is considered to have partial mediation; and when VAF is greater than 80%, it is considered to have full mediation. 37
Theme 1: Complex affordances—a battle between technician and consultant role
As the main findings of our research, affordances show different influence in different individuals' perception. Technological affordance significantly and positively influences personal perception, with a better explanatory power in performance expectancy (R2 = 0.546) follow by exercise self-efficacy (R2 = 0.472) and effort expectancy (R2 = 0.384). Moreover, HCA having a better predictive effect than HTA. Regarding the influence of different affordances on single perceptions, performance expectancy, and exercise self-efficacy are more greatly influenced by HCA compared to HTA, while effort expectancy is more influenced by HTA. Overall, from the path coefficient and effect size, HCA showed an advantage in influencing personal perception.
Specifically, focusing on the influence of single affordance on different perceptions, HTA has the greatest impact on effort expectancy (coefficient = 0.379, CI: [0.273, 0.485], p < 0.05), indicating that ease of system operation is the primary consideration for users when engaging with WFDs, followed by exercise self-efficacy (coefficient = 0.294, CI: [0.184, 0.395], p < 0.05) and performance expectancy (coefficient = 0.282, CI: [0.176, 0.390], p < 0.05). Meanwhile, HCA has the greatest impact on performance expectancy (coefficient = 0.510, CI: [0.411, 0.604], p < 0.05), suggesting that obtaining effective and practical health information from WFDs is crucial for achieving exercise goals. This is followed by exercise self-efficacy (coefficient = 0.445, CI: [0.350, 0.541], p < 0.05) and effort expectancy (coefficient = 0.289, CI: [0.183, 0.392], p < 0.05). To sum up, in the comparison of the two affordances, HCA shows stronger competitiveness and plays a greater leading role in influencing an individual's sense of purpose and confidence.
Theme 2: Direct effect on healthy outcomes—the role of device perception and self-psychology
Consistent with our expectation, personal perceptions show a high explanatory power and has a significantly positive influence on health-promoting behavior (R2 = 0.658). Specifically, performance expectancy (coefficient = 0.185, CI: [0.086, 0.277], p < 0.05) and exercise self-efficacy (coefficient = 0.405, CI: [0.307, 0.501], p < 0.05) significantly impact health-promoting behavior. With the digital health intervention of WFDs, individuals tend to gain effective management of physical activities and receive more confidence in exercising when facing difficulties. The value of the device is thereby manifested, thus forming the behavior of health promotion.
However, the hypothesis regarding effort expectancy influencing health promotion was not supported (coefficient = 0.076, CI: [−0.005, 0.153], p = 0.058; see Figure 3). This is an interesting finding, proving that the effort expectancy of WFDs no longer has a significant impact on an individual's exercise behavior. The small effect size of the hypothesis result also reflects that the difficulty of using the device is not crucial in contributing to health behaviors.
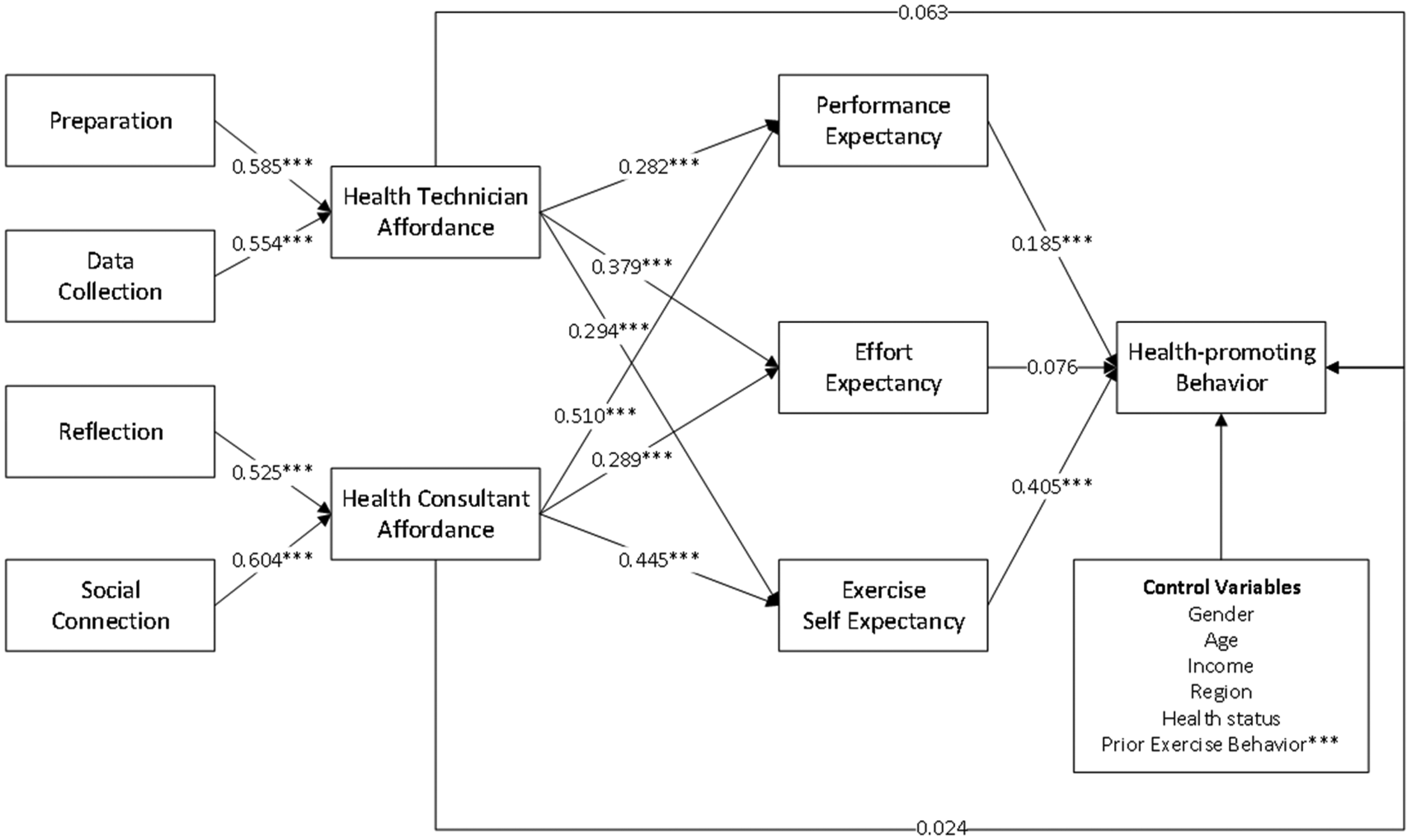
Results of model testing. Note. *p < 0.05, **p < 0.005, ***p < 0.001.
Theme 3: Powerful mediation effect—a crucial bridges in the behavioral chain
In this study, personal perception serves as the mediating variable between technological affordance and health-promoting behavior, with significant indirect effects (HTA indirect effect = 0.263, CI: [0.135, 0.263], p < 0.05; HCA indirect effect = 0.320, CI: [0.230, 0.370], p < 0.05). These results indicate that the capabilities provided by technology can stimulate health-promoting behavior through personal perception. Specifically, personal perception partially mediates the impact of HTA on health promotion (20%≤VAF ≤ 80%) and fully mediates the impact of HCA on health promotion (VAF > 80%). Both mediating factors share a significant positive effect on the direct impact of affordances on health-promoting behaviors, acting as crucial bridges in the behavioral chain. Their interplay enhances the overall influence of WFDs on encouraging healthy behaviors. Additionally, the total effect of HCA on health promotion is slightly higher than that of HTA. This suggests that technological affordance cannot directly impact health promotion. Compared to technician-driven affordance over the device, the emotional consultant-driven affordance has a more positive impact on health-promoting behavior, which is exerted through human perception (Table 7).
Specifically, apart from the path mediated by effort expectancy (HTA indirect effect = 0.029, CI: [−0.002, 0.062], p = 0.074; HCA indirect effect = 0.022, CI: [−0.002, 0.047], p = 0.047), both performance expectancy (HTA indirect effect = 0.052, CI: [0.021, 0.090], p < 0.05; HCA indirect effect = 0.095, CI: [0.044, 0.145], p < 0.05) and exercise self-efficacy (HTA indirect effect = 0.119, CI: [0.072, 0.169], p < 0.05; HCA indirect effect = 0.180, CI: [0.124, 0.246], p < 0.05) can mediate the effect of technological affordance on health-promoting behavior. This is because, as indicated by the hypothesis testing, effort expectancy does not impact health promotion, resulting in its inability to act as a mediator between affordance and health promoting behavior. Additionally, exercise self-efficacy is the most influential factor in mediating the effects of both HTA and HCA. Its strong mediating role suggests that affordance needs to inspire individuals' confidence in completing exercises to better achieve health-promoting behavior (see Table 8).
Theme 4: Robustness testing—interference effect of prior exercise behavior
A robustness test is conducted to ensure that research findings remain valid under varying conditions or situations. In this study, prior exercise behavior was initially included as a control variable to eliminate the influence of an individual's previous exercise experience on health promotion behaviors. This approach was intended to isolate the influence of these affordances thus preserving the purity of the research results.
We included prior exercise behavior as a variable for robustness testing for two main reasons. On one hand, during hypothesis testing, prior exercise behavior was found to be the only significant control variable, confirming that varying levels of exercise experience can indeed interfere with the path relationships in the model. On the other hand, existing research suggests that prior technical and exercise experiences and behaviors can automatically influence health-promoting behavior,38,39 and previous successful experiences can enhance self-efficacy.21,40 As individuals accumulate more experience with a certain technology over time, their usage becomes less influenced by conscious decision making, ultimately becoming a dominant predictor of behavior. Therefore, to further explore the potential impact of prior exercise behavior, robustness testing involved repositioning prior exercise behavior from a control variable to an independent variable.
By examining the relationships between prior exercise behavior, mediating variables, and the dependent variable, the results revealed that these added paths were significant (p < 0.05), and importantly, the significance of the original paths remained consistent with prior hypothesis results (Figure 4). This confirms that our research model remains valid even under the interference of prior exercise behavior, and affirms the critical role of prior exercise behavior in the health promotion process facilitated by WFDs. The result of robustness testing provides empirical evidence for further refinement of the model—demonstrating that the external technological intervention effect is strong and its significance is not influenced by intrinsic individual experience. However, the potential interaction between the two factors in shaping the formation of health-promoting behaviors is worth further investigation in future research.

Results of robustness testing. Note. *p < 0.05, **p < 0.005, ***p < 0.001.
Discussion
Theoretical implications
In the contemporary digital era, technology and daily life are inextricably intertwined, necessitating not only the utilization of technology's inherent capabilities but also an exploration of its human-centric dimensions. In the postpandemic landscape, the emphasis on accuracy and reliability of technology 41 is now complemented by a growing need for digital tools that serve as caring figures. Prolonged social distancing and heightened social isolation have led individuals to take more proactive initiatives in caring for their bodies. In this context, WFDs, as an electronic health device, can significantly and positively intervene in the formation of health-promoting exercise behaviors. 5 It might not only provide precise biometric data but also offer personalized guidance and support to encourage and sustain health-promoting behaviors.
Building on this understanding, our study expands the concept of affordance by introducing two dimensions: HTA and HCA. Drawing on Gibson's affordance theory and its subsequent extensions, we posit that HTA reflects the technological, data-driven capabilities of WFDs—such as personalized goal setting and systematic data collection—that empower users to engage in precise self-monitoring and achieve a sense of control. In contrast, HCA embodies the guidance dimension, whereby WFDs transform raw biometric data into actionable, personalized health insights and establish an interactive, advisory relationship with users. This dual-process framework moves beyond a unidimensional view of human–technology interaction to capture the dynamic interplay between user autonomy and dependency—a phenomenon we refer to as the independence-dependence paradox. 42
Our findings indicate that HCA exerts a stronger influence on performance expectancy and exercise self-efficacy, suggesting that users tend to rely on the consultative, expert-like functions of WFDs to enhance their competence in health management. Conversely, HTA more significantly affects effort expectancy, as users value the ease of use provided by the device's technical functions. These results align with key tenets of SCT, 21 that personal accomplishment and emotional arousal can lead to self-efficacy, highlighting how both autonomy (via HTA) and relatedness (via HCA) are critical for sustaining long-term health behavior change. Overall, this theoretical framework not only deepens our understanding of how WFDs contribute to health-promoting behaviors by integrating both functional and guidance roles but also underscores the emerging need for technology that serves as a caring, supportive virtual health consultant in the postpandemic era.
Secondly, we advance the mediation mechanism between affordance and health-promoting behavior. Our findings indicate that performance expectancy and exercise self-efficacy significantly mediate this relationship. This is consistent with the UTAUT, which posits that perceived usefulness is a primary driver of technology adoption and continued use. 43 Our study extends UTAUT by demonstrating that perceived usefulness also sustains health-promoting behavior. Additionally, technology affordance boosts users' self-belief in their abilities, and higher levels of self-efficacy have a more significant impact on the effectiveness of electronic health interventions, 44 leading to positive health outcomes, which aligns with Bandura's SCT that highlights self-efficacy as crucial for behavior change. 21 Notably, effort expectancy does not significantly promote health-promoting behavior. One possible explanation lies in the increasing digital literacy and the decreasing digital divide in China, 45 where the majority of WFD users are becoming more adept at managing digital technologies. As users become more familiar with wearable devices, their perceived difficulty in using these devices diminishes. Modern WFDs, with their user-friendly interfaces and intuitive designs, have reduced cognitive load and made the technology more accessible. 8 This ease of use is likely to be less of a barrier for most users, particularly among younger generations who are more accustomed to interacting with digital technologies. Additionally, as users grow more experienced with WFDs, their focus may shift away from concerns about effort expectancy and toward more intrinsic motivators, such as autonomy, competence, and self-esteem. These factors are more directly related to users' ability to achieve their health goals and maintain long-term engagement with health behaviors, as demonstrated in our study. Moreover, the cross-sectional data used in our research was mainly collected from people who have experience in using WFDs. These individuals already have the habit of using WFDs, so the difficulty level of using the device has met their satisfaction, and therefore the ease of use of the device has become irrelevant to the cultivation of healthy habits. 46
Thirdly, our results indicate that prior exercise behavior significantly impacts users' health-promoting behavior, a finding that aligns with Pender's Health Promotion Model. This model suggests that previous engagement in health-promoting activities serves as a critical antecedent for current behavior, reinforcing the idea that past experiences shape future actions. Our findings confirm that prior exercise behavior, which represents self-initiated decisions independent of technological guidance, is an important predictor of sustained health promotion. This underscores the theoretical need to integrate historical behavioral patterns into the design and implementation of health interventions. Although our study primarily focuses on the roles of HTA and HCA in shaping health behaviors, including prior exercise behavior as a control variable enables us to better isolate the influence of these affordances. Furthermore, the interplay between self-initiated exercise behaviors and the guidance provided by WFDs suggests that the interaction between intrinsic motivation and technology-mediated support could be a fertile area for future research. Such exploration may reveal how these factors synergistically contribute to long-term health behavior change.
Practical implications
For WFD manufacturers, enhancing the accuracy of data and the human-like expert roles of the technology is crucial. WFDs have a strong influence as health consulting experts, and humanizing the devices can help reduce usage effort. However, issues with measurement reliability and validity persist. 47 Users tend to trust the health information provided by these devices, indirectly demanding improved data accuracy from manufacturers. Improved data accuracy is directly linked to increased trust. 48 Therefore, manufacturers should prioritize the expert-like aspect of WFDs, emphasizing warmth, trustworthiness, and emotional arousal. Compared to attending standalone offline expert consultations, WFDs are more effective in motivating individuals to achieve health behavior changes. Additionally, artificial intelligence (AI)-based WFDs provide unwavering support and real-time guidance, which is crucial for individuals in maintaining fitness habits. 49 This will help users make informed health decisions and manage their exercise routines more effectively. The humanization of these devices highlights the need for deeper interactions with users, which in turn requires manufacturers to ensure comprehensive electronic health literacy in users, enabling them to identify inaccurate or ineffective information. Existing research suggests that wearable devices should incorporate more gamified exercise methods to facilitate behavior management, 50 especially for individuals with low self-efficacy, enhancing interactivity could lead to a greater willingness to continue usage. 51 WFDs manufacturers can consider creating digital avatars of experts to build a personal data analysis framework with the help of health professionals, and by developing gamified health challenges, reduce the difficulty of interpreting and applying device data, thus enhancing users' motivation and sense of involvement in exercise. Moreover, as effort expectancy is no longer a significant factor, manufacturers should focus on improving WFDs' performance in promoting sustained health habits, highlighting their unique advantages in the health sector.
For health professionals, they should collaborate with WFD manufacturers to prioritize the usefulness of technology and the improvement of self-efficacy when promoting WFDs. With the additional support of human expert consultations, the cultivation and change of health behaviors will achieve maximum results and accelerate the positive transformation of health behaviors. 52 Rather than emphasizing ease of use, health professionals can work to ensure that WFDs are integrated with diverse health scenarios that enhance users' self-efficacy in health-promoting behaviors. By focusing on the health consultant affordance (HCA) of the technology, health professionals can support users in applying the feedback and recommendations provided by the devices to improve health outcomes. Additionally, health professionals can encourage the use of HTA by integrating scenarios that emphasize the usefulness of the technology, helping users see the benefits of data collection and self-monitoring for their health.
For policymakers, advancing the integration of personalized exercise scenarios and cloud databases through AI, 5G, and information and communication technologies will become increasingly important. This requires a comprehensive analysis of body data to build robust systems that foster sustained use of WFDs. Policymakers should support the development of integrated personal information portals and facilitate the collection and use of health data to inform health interventions. Additionally, they should also focus on the integration of prior exercise behavior as a motivational tool to enhance the formation and sustainability of health-promoting behaviors among users. Policymakers can expedite the development of governance guidelines for the use of AI-assisted cloud computing, helping to ensure that more AI and multimodal algorithms are applied in the development of personal information portals. These technologies can provide deeper and richer insights for interpreting health data, aligning more closely with individual experiences and unique needs, which in turn can result in more effective and sustainable behavior change, leading to improved health outcomes. 53 Moreover, policymakers could provide channels for integrating exercise and health information from WFDs into healthcare institutions and service platforms, collaborate with manufacturers and health professionals to design systems that tailor WFDs' feedback and recommendations to users' prior exercise experiences. Leveraging the professional knowledge of national health experts to intelligently interpret body data and design more scientific exercise plans, can help users become more familiar with health-promoting activities, increasing their confidence and likelihood of engagement. By emphasizing the importance of past behaviors in health interventions, policymakers can promote the effective and long-term use of WFDs for health behavior change.
Limitations
Firstly, this study focused on adults, and future research should consider users with a more diverse demographic range. For example, WFDs are widely used among teenagers, and further studies could explore whether WFDs can help address obesity issues in this age group. Additionally, the current study primarily examines Chinese users. Future research could explore users from different cultural backgrounds to compare how WFDs are used across various cultural contexts. Furthermore, the current study relies mainly on self-reported data. Future research could incorporate biometric data to provide more objective insights.
Secondly, this study does not incorporate social factors into the research model, aside from performance expectancy, effort expectancy, and exercise self-efficacy. Given that humans are inherently social beings, neglecting the social context may overlook significant factors that influence health-promoting behaviors. Future studies should place greater emphasis on social variables and target specific groups to conduct more comprehensive health promotion research.
Additionally, while effort expectancy was found to be insignificant in predicting health-promoting behaviors, this result suggests that as digital literacy improves and users become more familiar with technology, effort expectancy may have a diminished role in motivating users. This offers an important direction for future research, which could examine how the relationship between effort expectancy and behavior change evolves as users gain proficiency with wearable fitness devices.
Lastly, the potential impact of WFD malfunctions has not been discussed, despite the frequent occurrence of device failures. The “incomplete intelligence” state that arises during such failures presents a new challenge in human–machine interaction and warrants further in-depth investigation in future studies.
Conclusion
The study extends current affordance theory by demonstrating that WFDs contribute to health-promoting behavior not only through their technical capabilities but also by serving as interactive guides that enhance users' self-efficacy and perceived usefulness. These insights have implications for both theoretical advancement and practical application in designing digital health interventions in the postpandemic era.
Footnotes
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Academic Committee Members of School of Journalism and Communication (August 28, 2024) for studies involving humans.
Author contributions
GH contributed to the conceptualization of the study. WH was responsible for the data collection and analysis. FQ contributed to the writing of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Guangdong Basic and Applied Basic Research Foundation, and National Social Science Fund of China (grant numbers 2023A1515010670 and 22BXW024).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.