
Abstract
Upper limb paresis occurs quite commonly after stroke and may result in the affected limb’s disuse or learned non-use. As a result, its cortical representation may be suppressed, further inhibiting its spontaneous utilization, resulting in motor function deterioration, increase in spasticity, joint stiffness and pain.
The aim of this work was to involve stroke survivors in a qualitative study within a user centred design process to better understand the perspectives of stroke survivors on virtual reality - based serious games (SG) for upper limb rehabilitation during the chronic phase and use those insights to design a VR-based serious games which promotes activation of the affected cortical area.
A qualitative research method was performed using a multi professional focus group discussion, including a representative group of stroke survivors.
With the insights of this work, the authors initiated the design of a VR-based SG prototype for upper limb rehabilitation with two modes, one version to be played with any arm to pick a virtual hammer and hit targeted objects, and other version, a mirror version based on mirror therapy.
Keywords
Introduction
Every year, over a million Europeans suffer from stroke, with around two-thirds of survivors suffering from upper limb paresis. 1 With the increase in life expectancy of stroke survivors, it is necessary to pay more attention to the psychological, social and physical handicaps in the chronic phase, equally important to the quality of life. Since there is no clear consensus on when the chronic stage after a stroke begins, in this study the authors define it as beginning 6 months after the stroke. 2
Patients with upper limb paresis frequently learn to conduct activities of daily living (ADLs) with just one limb, resulting in a learned non-use phenomenon of the paretic limb, 3 gradual loss of motor function, increased spasticity, joint stiffness, and increased pain. Activating the affected upper limb cortical area is beneficial. Liepert et al. 4 have reported good results with intensive constraint-induced movement therapy (CIMT) of stroke patients, reporting an enlarged cortical motor representation. However, CIMT could have motivation and adherence concerns, which may sometimes make patients apprehensive about participation. 5 On the other hand, an inclusion criterion for CIMT is a voluntary wrist extension and a minimal extension at the metacarpophalangeal and interphalangeal joints. 6 For patients without any movement in the paretic hand, activation of the correspondent cortical area could be accomplish with other techniques, such as mirror therapy. 7 VR could use mirror therapy principles for upper limb paresis after stroke 8 with the advantage of enhancing the patient´s engagement. 9
Besides the physical problems, with the increasing prevalence of chronic conditions, such as stroke impairments, a holistic, bio-psycho-social, approach must be taken into consideration in healthcare systems, including finding solutions for self-management.10,11 Social isolation and depression are very common among stroke survivors, 12 therefore measures that promote entertainment and socialization, while helping the rehabilitation process, are of paramount importance.
SG using VR technologies for serious purposes, such as education or health, could be a solution to motivate the use of the paretic upper limb and/or activate the affected cortical area while promoting entertainment and socialization. With technological advancements, device cost reductions, and the broad availability of high-speed internet connections, their use is expected to grow. 13 VR provides a simulation of an environment, scenario or activity, in real-time; it uses a user-computer interface in an immersive or non-immersive way and has the capability of increasing motivation and adherence to rehabilitation activities. 14 In stroke rehabilitation, VR-based SG enhances neuroplasticity at an early stage and activates sensory regions that gradually degenerate due to inactivity in the chronic phase 15 ; It also helps with pain management and depression treatment.16,17
Meta-analysis of stroke rehabilitation therapies found that using VR in combination with traditional therapy improved upper limb motor function and quality of life on gait and balance.18,19,20 Despite the promising results of VR on stroke rehabilitation, the post stroke phases (acute or chronic) were not analysed separately. 18
SG and gaming devices also allow patients to practice at home through telerehabilitation.21–25
Considering the potential benefits of SG identified in the literature, the research question of this study is: how to design SG which are persuasive to promote the use of the paretic upper limb or to activate the cortical area in the chronic phase after stroke?
Conceptual framework
A participatory design approach has been proposed by several authors to design a SG which meets the user’s needs and expectations, resulting in increased engagement. 26
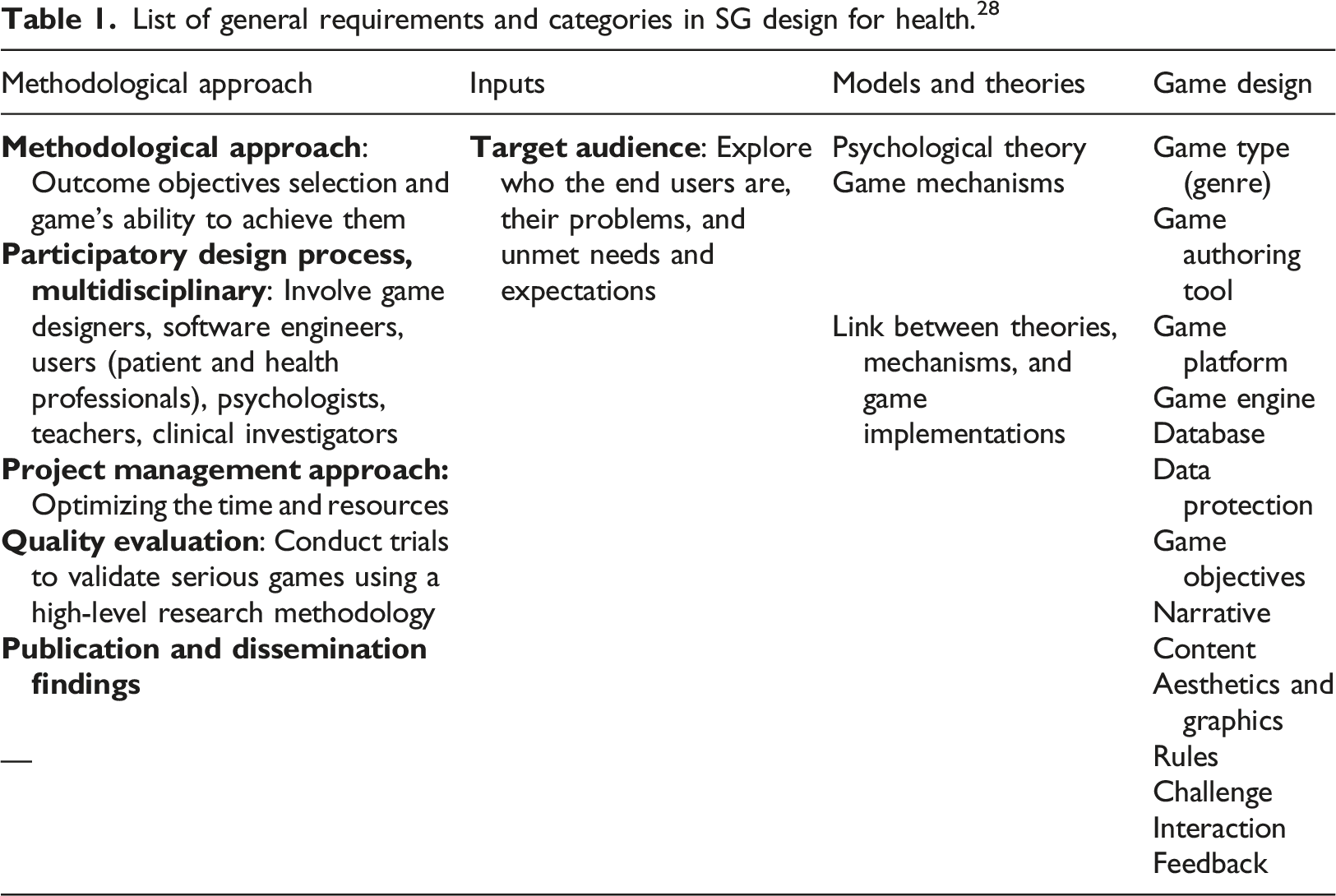
List of general requirements and categories in SG design for health. 28
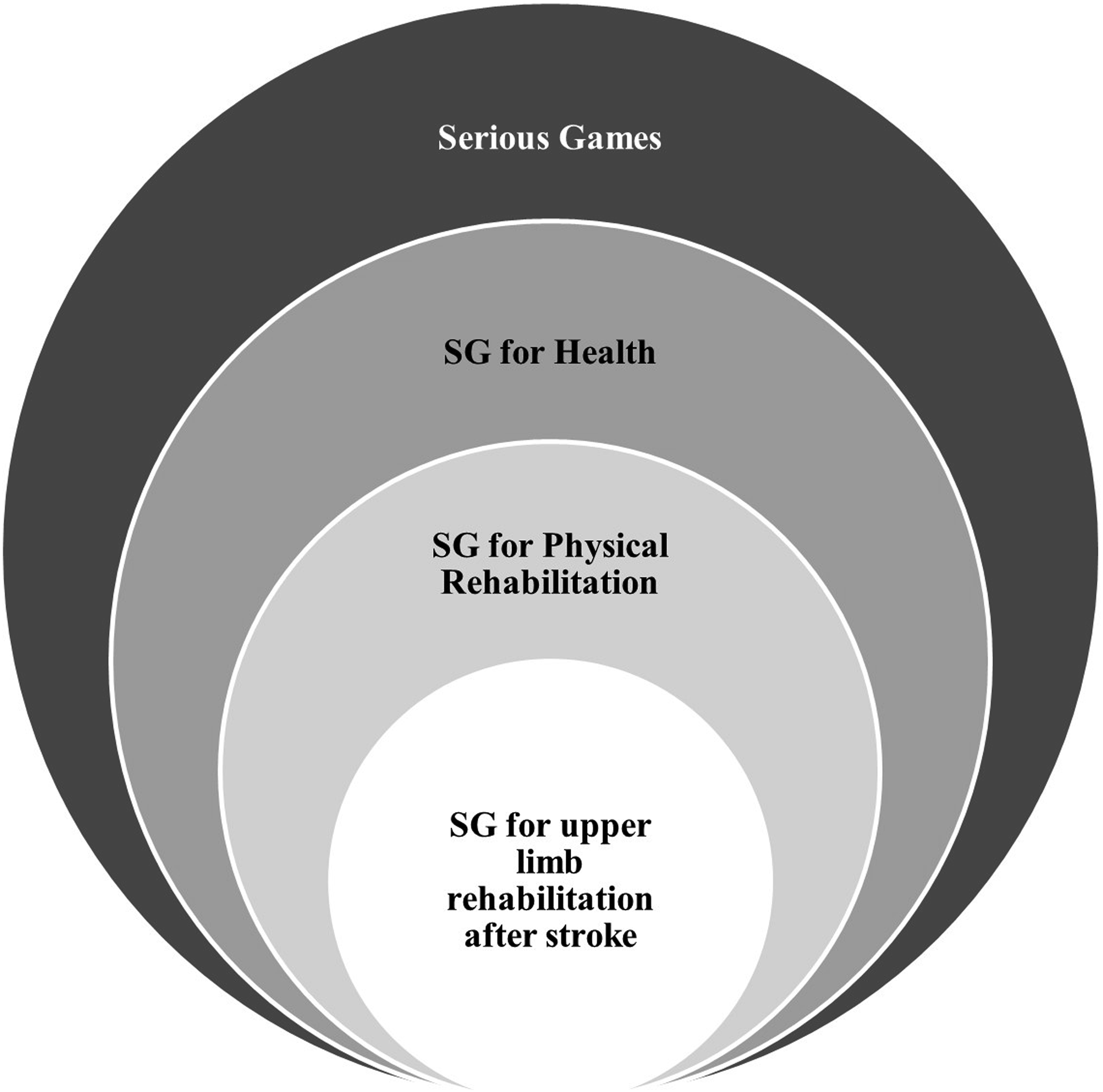
Levels of Serious Games requirements according to the purpose 150x87mm (330 x 330 DPI).
Several studies have developed SG frameworks for rehabilitation purposes.27,29–33 One of the most recent framework for physical rehabilitation was published by Beristain-Colorado et al.,
34
and is based on three fundamental concepts: structural activities in software engineering, user centred design (UCD), and gamification (Figure 2). Conceptual elements of the Beristain-Colorado framework31 144x71mm (330 x 330 DPI).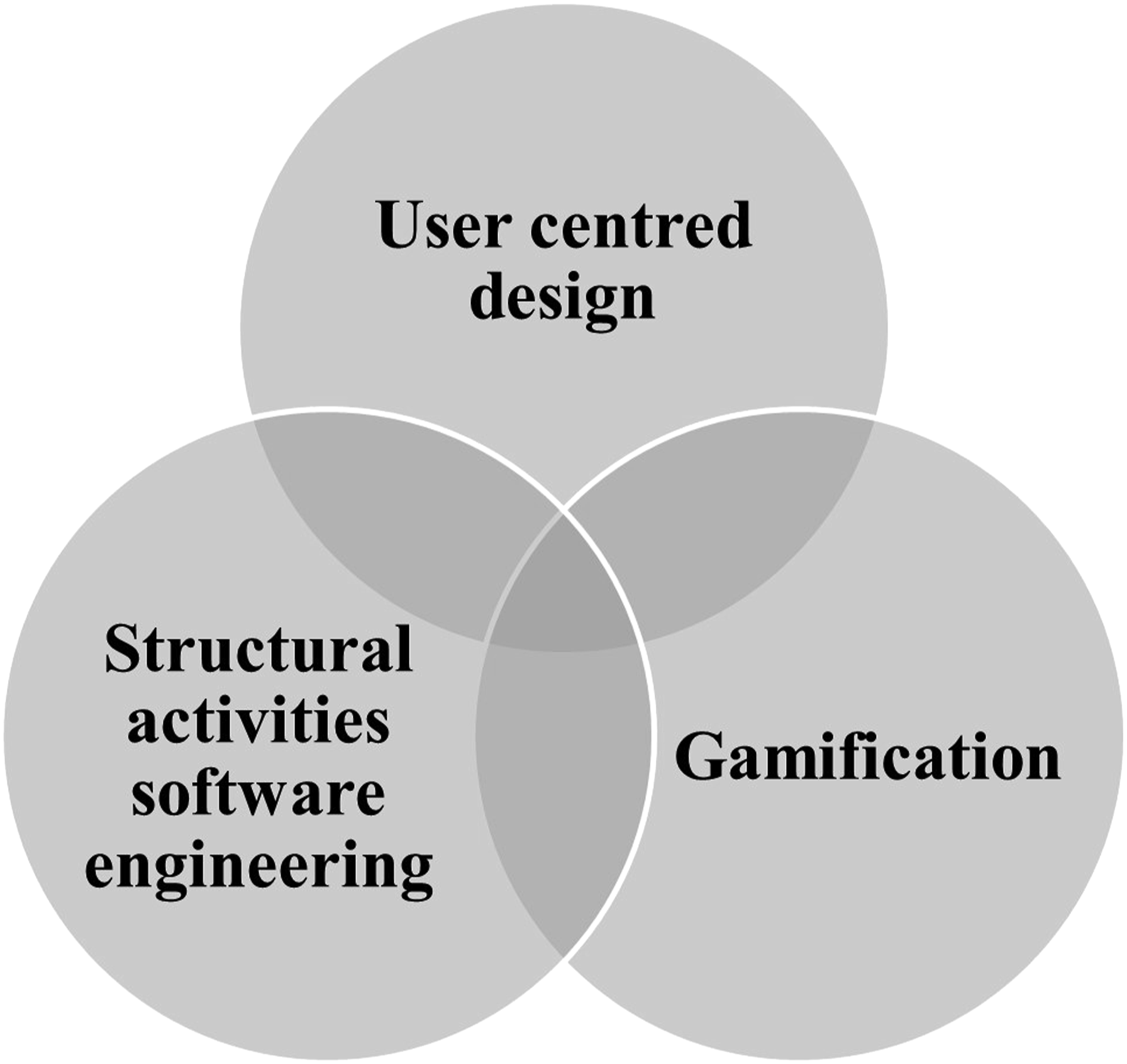
Other SG frameworks30–33 were proposed previously in physical rehabilitation and education; all of them included a structural activity component but they were not always used to a UCD. Physical rehabilitation-oriented gamification elements were a common feature in the majority of them. Few included the development of a data acquisition interface to process the patient’s motions when commercial equipment do not adapt to the rehabilitation process. 34
In the Beristain-Colorado et al. 34 framework, the structural activities applied to UCD include the communication between the development team and the users focused on determining the system’s context and essential needs. The work is based on planning the requirements and developing resource estimates, modelling and construction of a prototype and finally deploying the prototype to the end user, followed by obtaining feedback on the project to make the necessary changes.
In each phase of the design process, the UCD method focuses on users and their demands. It starts with the understanding of the context and users, followed by the specification of user requirements, then the design and, finally the evaluation. Depending on the results, it might be necessary to repeat phases until a satisfactory response is given by the users (Figure 3). UCD process phases31 150x55mm (330 x 330 DPI).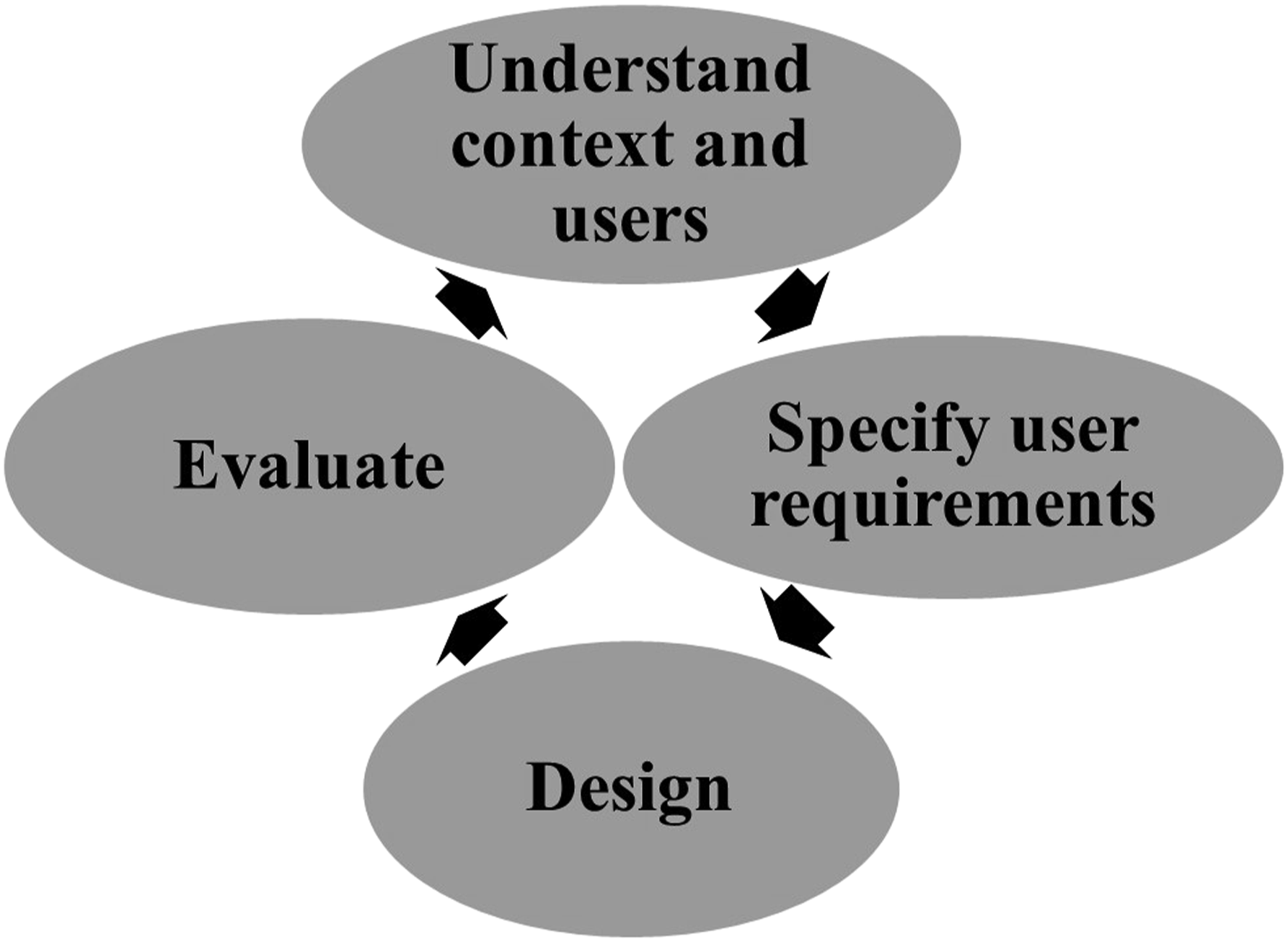
Gamification applies game mechanisms in many circumstances to entice people to ordinary but enjoyable activities with motivational and cognitive advantages. 35 The gamification elements include: challenge – the game must be challenging enough for the user’s skill level to avoid boredom and adapt to the users´capabilities; 36 accessibility –adaptability to the user´s disabilities, and the users’ interests; experiences and skills, 36 player skill – with progress, the user develops more skills that encourage him/her to continue playing; rewards which indicate the users’ progress; real-life simulation to allow users with physical limitations to fully involve themselves in the game concentration on the game avoiding distractions from the main task; feedback to the patient (about the progress, the correct performance and through rewards, and difficulty adjustments to the rehabilitation exercises).
The UCD process and gamification elements are essential to design persuasive SG. With fun experience, SG can persuade stroke patients in shaping a positive attitude and behaviour through their rehabilitation therapy. 37
According to Bogost, 38 the ability of digital games to explain processes through interactions was a powerful persuasive characteristic.
Teresa de la Hera 39 provided a theoretical model that explains how other aspects of a game, such as aesthetics, music, plot, or audio, visual treatment, might affect how players understand game material.
Although research on persuasive gaming is going in multiple directions, and gamification has become a common way to increase patient´s engagement and affect their result positively in SG applied to health, there is little research on designing persuasive games for stroke patients. A conceptual design model of a persuasive game for upper limb rehabilitation after stroke was proposed by Omar et al., 40 aligned with the Persuasive System Design (PSD) Model. 41
The authors took into account the general and more specific frameworks related to SG design in health and in rehabilitation to design this study.
Methods
In this section, it is described the study and the methods used to gather information regarding the development of engaging SG for upper limb rehabilitation. The study was approved by the University of (anonymized information) Ethics Committee. Participants were invited to take part in the study by an email from the president of an association of stroke survivors. Further details and an informed consent form were sent to those who agreed to participate. All participants were informed that any data they provided that might identify them would be confidential and would not be published. Those willing to participate were emailed more information and a consent form. All participants were informed that any information given would be kept anonymous and that any details that may identify them would not be published. The participants were also asked if they would consent to the recording of the meetings. The meetings only occurred after written consent was obtained.
The authors used the SPIDER tool 42 for a qualitative study: Sample, Phenomenon of Interest, Design, Evaluation and Research Type.
Sample (S)
The inclusion criteria for participants were: (1) representative from rehabilitation experts; (2) representative from SG designers; (3) representative from stroke survivors, adults, with more than 1-year post stroke, who understand the purpose of the study and know how to use a computer. Four of the authors (three engineers and one rehabilitation physician) were active participants and a convenience sampling 43 from a stroke survivor association was used. The authors contacted the stroke survivor’s association president, who is also a stroke survivor, and explained the purpose of the research. A group of eight stroke survivors was selected by the association president, because they were thought to give richer information on the subject. There were no restrictions regarding the participants’ sex or age. The participants were five males and three females, all with at least 1 year past since their stroke, and with ages ranging between 30 and 70.
Phenomenon of interest (PI)
Authors' aim was to investigate what chronic stroke survivors thought about custom-made VR-based SG.
Design (D)
Thematic analysis or content analysis 44 was used in order to analyse the themes and patterns from the narrative content of the qualitative study.45,46
Evaluation (E)
Subjective outcomes (attitudes, opinions, experiences, expectations, preferences).
Research type (R)
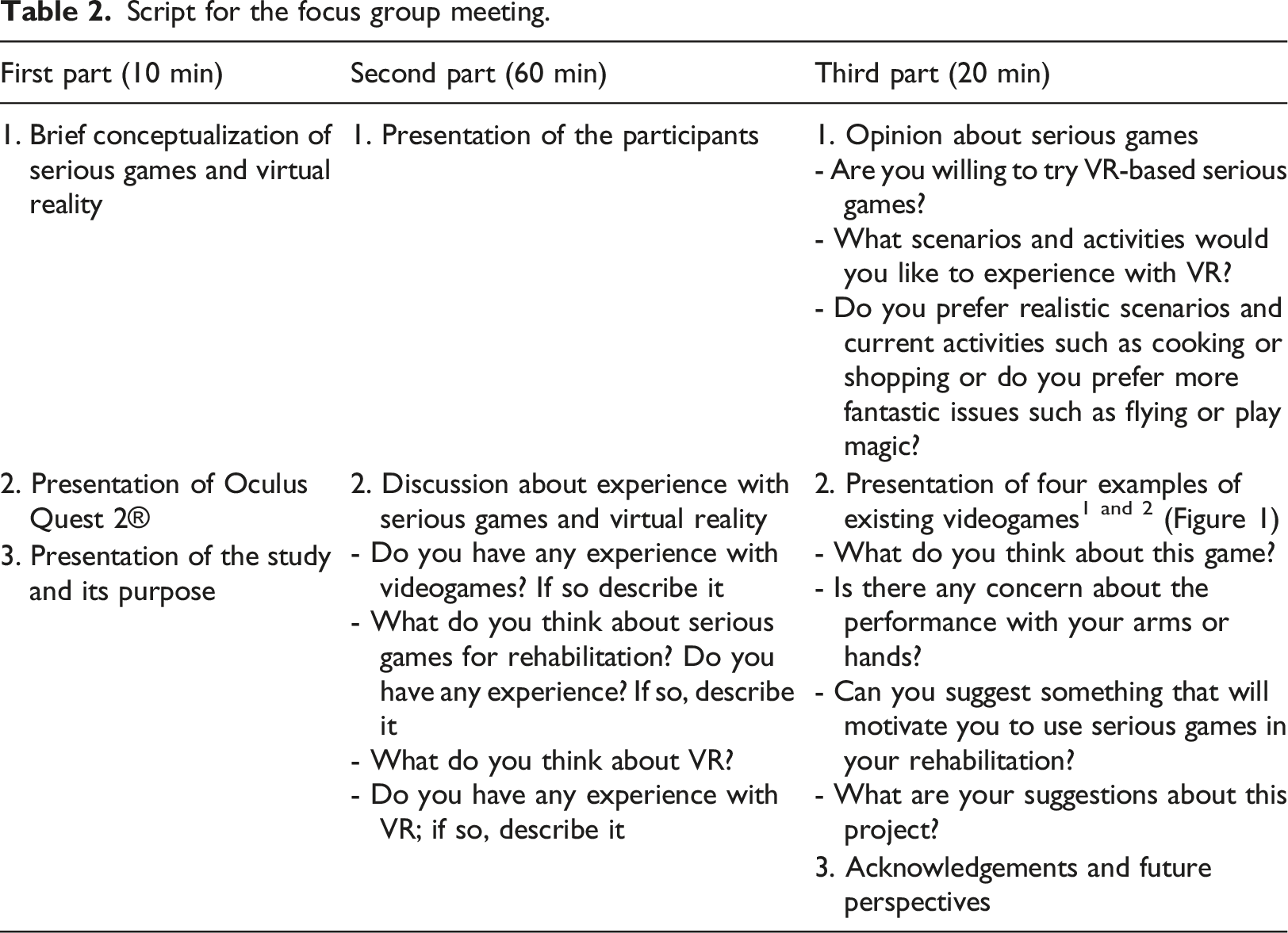
After selecting the convenience sampling, a qualitative data collection method was performed based on two focus group online meetings between May and June 2021, the first between four of the authors and the stroke association president to introduce the study. The second was a 90-minute-long meeting that included the same participants of the first meeting plus seven members of the same association. In both meetings one of the authors was the moderator.
Script for the focus group meeting.
The authors also selected four existing videogames (Figure4) to show and stimulate discussion during the focus group meeting. Existing videogames shown to participants as examples 92x72mm (220 x 220 DPI).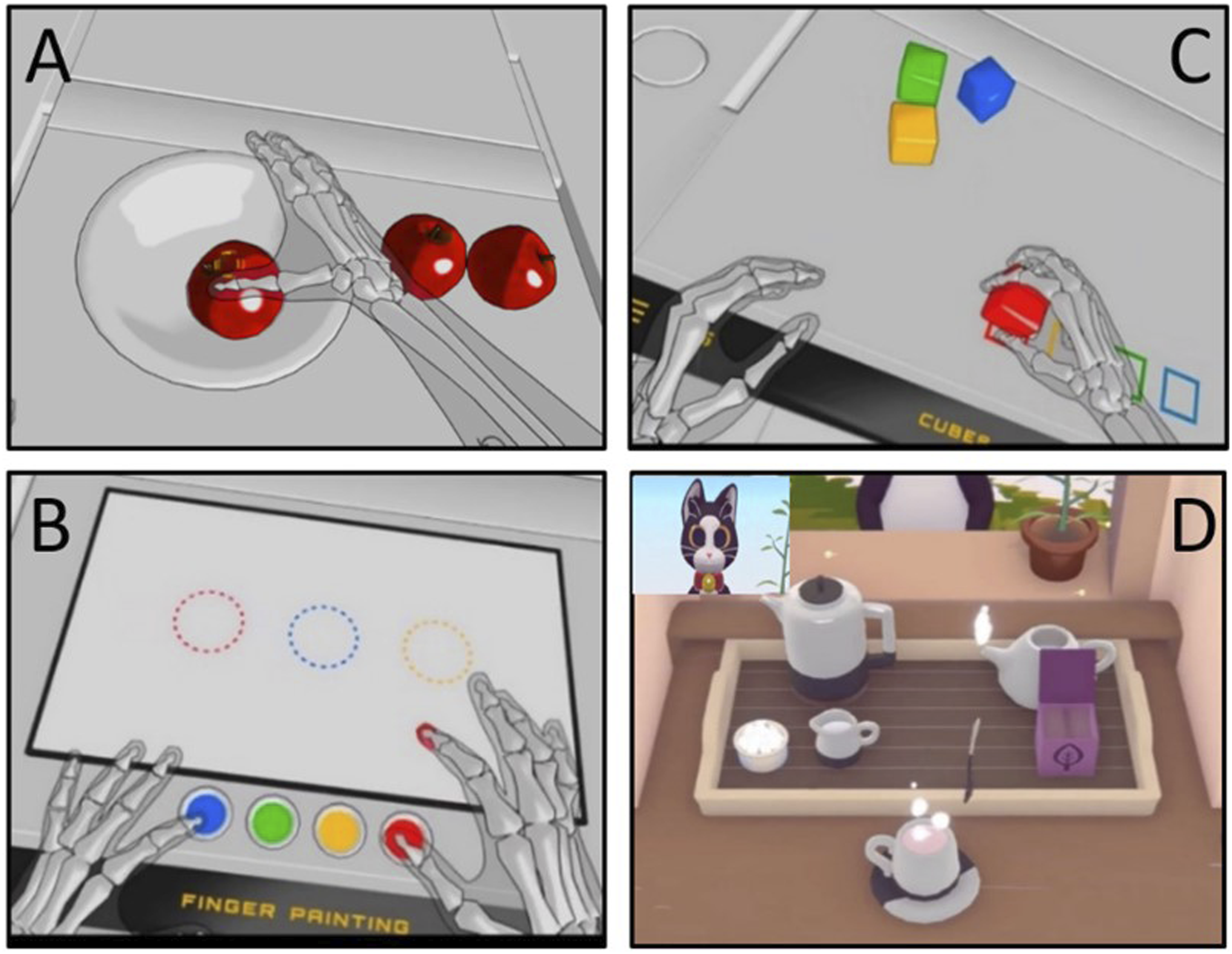
Thematic analysis was made starting with transcription of the focus group discussion, as well as the notes that the moderator took during the meetings, followed by a themes' review refinement, following a narrative research approach. 47 Two of the authors were involved in data analysis using investigator triangulation to provide multiple observations and conclusions.
Results
From the eight stroke survivors, two had already experienced non-immersive VR-based serious games (with Nintendo Wii® and Armeo®) during the acute phase; those two survivors are between 35 and 44 years old, one was a woman and one was a man. None had experienced immersive VR. A third patient, a 49-year-old man, usually played simple computer videogames on his mobile phone for entertainment but found most commercial videogames difficult to play and presented accessibility issues. When asked about their opinion regarding commercial videogames, one participant answered: «The normal videogames unnerve me, as they are too fast and noisy».
Some stroke survivors had doubts about SG suitability considering their clinical characteristics: «I have visual hemineglect. Can those games (SG) help me? Can you alter the game for that purpose?» «I get scared easily since the stroke. Are immersive SG appropriate for me?» «I had seizures when I had the stroke and during the first year, I had to take medication to avoid them. Is it safe for me to play SG?»
The stroke survivors who didn´t have experience with videogames or SG were curious and preferred to try SG rather than commercial videogames. «We have a lot of free time and nothing to do. If we play games just to spend time, it would be better to play games which are helpful for us».
Figure 5 shows the final four themes and categories after the focus group thematic analysis: Purpose, Scenarios, Tasks and Design Strategy. The final thematic map, showing the final four main themes 338x190mm (96 x 96 DPI).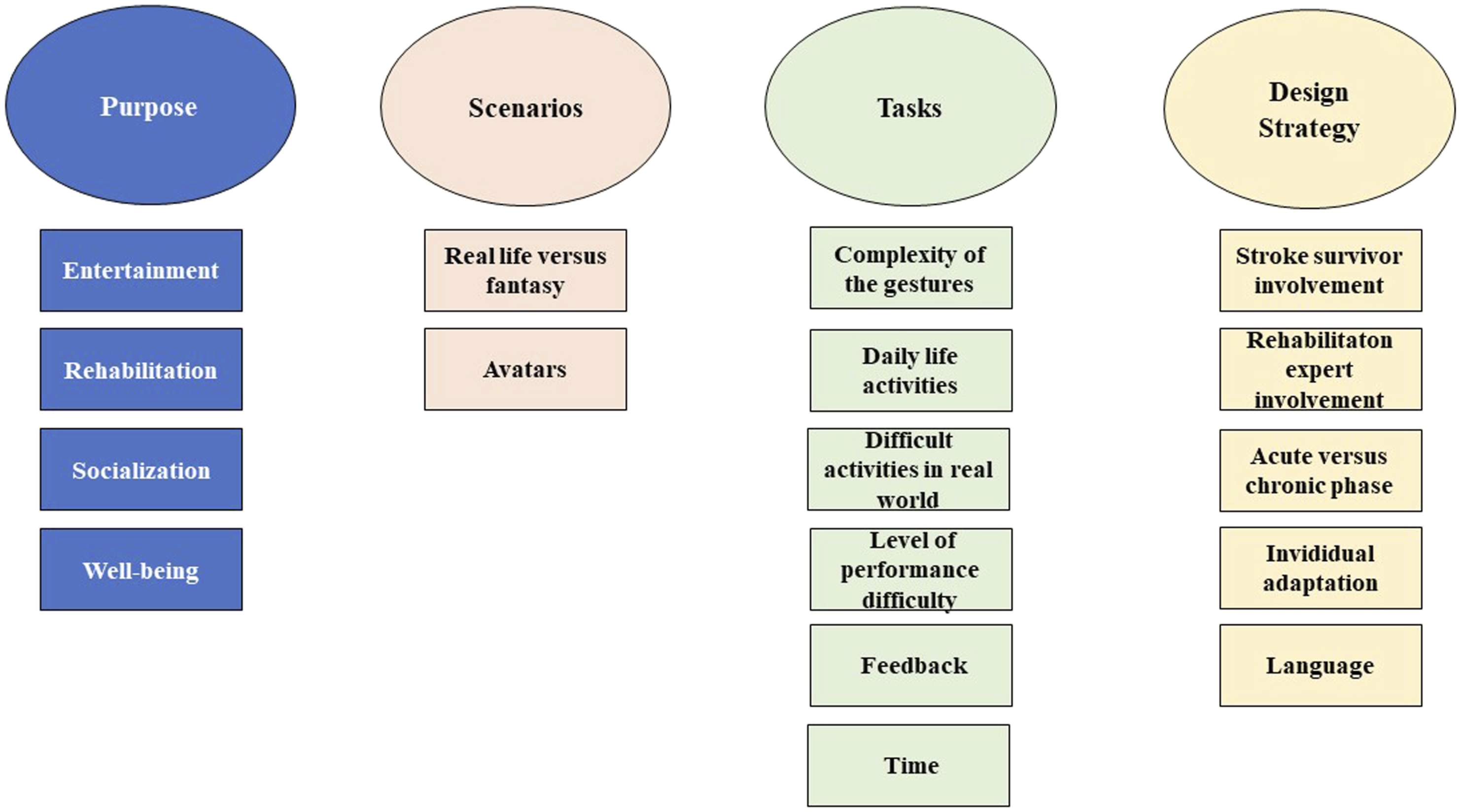
Purpose
The participants recognize that their handicaps are irreversible in the chronic period after a stroke and do not anticipate improving significantly with SG. They have knowledge of the use of SG for acute phase rehabilitation with the purpose of improving functionality. Their expectations in the chronic phase are entertainment and that SG somehow will help the conventional rehabilitation that is focused on maintenance and small gains. «Games (SG) are helpful to the rehabilitation process in an acute phase after stroke, but they could also be useful in chronic phase, with the goal of contributing to not worsening deficits and, perhaps, making minor gains».
Other aspects pointed out were socialization if SGs are played by more than one person simultaneously. «Playing in a group would be spectacular! We could help each other and even enter in small competitions».
Stroke survivors asked for the possibility to use the normal hand but see the paretic hand moving in the game.
When the engineers confirmed that possibility and the doctor explained the mirror neuron mechanism of virtual reality associated with that kind of activities (activation of the affected cerebral area), similar to mirror therapy that some stroke patients experienced in acute phase, stroke survivors showed great interest in trying this possibility. «Many of us can only move one arm. Having the illusion of moving both of them would be great! We can’t do that with commercial games».
Scenarios
The stroke survivors were unanimous about their preference of more realistic scenarios and human avatars they identified with. For instance, in the «tea making game» (Figure 4), the cat did not make any sense to the participants. «I appreciate the scenario of a kitchen, but the games should be in first person. Giving tea to a cat doesn´t make sense».
Enjoyable scenarios are another proposal, particularly real places where participants have never visited. «Simulating a walk in a nice place, in Paris, for instance, would be pleasant».
Tasks
The stroke survivors who had experienced SG in the acute phase felt that the tasks should be different in chronic phase. In acute phase simple gestures are acceptable as they are meant to improve certain movements and functionalities. In chronic phase they expect that SG would help them in daily life activities autonomy as well as experiencing feelings that they can´t experience anymore, such as running, swimming, exercising in a gymnastics class, travelling to an inaccessible destiny, seeing their hand that hasn´t move for months or years move. For instance, games such as those exemplified in Figure 4 are more suitable for the acute phase. «Those exercises remind me of the acute phase. They are too simple and not for us now».
An issue that was raised several times during the meeting was the preference for activities that can be replicated in the real world rather than in abstract games. «The major concern for us after the acute phase is to regain autonomy. SG should help us in that, simulating daily life activities, like cooking». «One thing that I miss a lot is participating in a group class in the gym, at my own pace», said a young woman. «I would love to play football again», said a young man. «Swimming is a nice scenario, which is something I cannot do now, and it is something that I enjoy a lot». «Simulating a mountain walk would be useful for me; I could learn how to overcome difficulties like stairs».
About the level of difficulty, «The game should evaluate our capacities and automatically adapt to us».
Another important suggestion given by the stroke survivors was that feedback should always be positive to avoid frustration. «Games (SG) should always be rewarding, even when the player can´t do the task. Stroke survivors are usually more depressed and if they don´t see any evolution in the game they wouldn´t want to continue the game». «What is important is not to win but to recover while having fun. Usually, we don´t have the means to have fun».
Design Strategy
In SG development a multidisciplinary team is welcome, where the users must be involved from the beginning. Stroke survivors appreciate rehabilitation experts' involvement but, as one stroke survivor said:
«Rehabilitation experts know the “house outside” but the only person who knows the “house inside” is the stroke survivor, so both must be involved».
Another concern stroke survivors had was the language used in the games - they appreciate the possibility of choosing the language as most of the games presented in examples were in English.
By the end of the meeting, and after clarifying their doubts, needs and expectations, all the stroke survivors showed interest in trying SG custom-made for them.
Discussion and future work
SGs differ from commercial videogames, which are intended for able-bodied users and so do not take into account the physiological, physical, and cognitive handicaps of stroke survivors and may lack the level scaling adaptability of purpose-made virtual environment systems created with the assistance of rehabilitation specialists. 48 The final user usually is involved only when a playable version of a game exists, instead of being consulted in early stages of the game design. 49 Perhaps for this reason, stroke survivors do not appreciate commercial videogames; they prefer scenarios representing «real life» activities, and avatars they identify with. This is coherent with «similarity», one of the most potent persuasive concepts - regardless of a person’s personality, a comparable other is more likely to convince them than a distinctive other.50,51
Positive feedback is a gamification principle 34 well identified in this study and it is crucial to improve motivation.
Persuasive methods are more effective when they are tailored to people rather than using a one-size-fits-all approach 52 and reflect the fact that the participants appreciate their involvement in the SG conceptualization, as well as the involvement of rehabilitation experts who know their needs.
Chronic stroke survivors' expectations differ from the acute phase, where simpler tasks, more oriented to motor recovery are better accepted. In chronic phase after stroke, survivors point out other interests for games besides physical ones, such as socialization and recreation, and prefer activities more focused on what becomes difficult or impossible to do after stroke and/or activities that help their autonomy. Even if SG couldn´t eliminate their impairments, the fact that they could create the illusion of a body and mind similar to the one before the stroke seems to be an area to be explored by SG designers.
Having the illusion of moving the paretic limb again appears as a point of high interest to those who cannot do it anymore, which means an expectable good acceptance of SG applying the mirror therapy principles. The individuals without any movement in one hand must play using only the other hand, even if they see the mirror of the paretic hand.
The stroke survivors with hemineglect could have difficulties in performing tasks that involve the side of the scenario that they neglect, hemianopsia could make it difficult to visualize the entire scenarios. These handicaps should be taken into account in SG design for stroke survivors and individual customization should be possible to make to as to minimize the negative impact caused by those handicaps.
Language selection and level of difficulty adaptation were also customization issues pointed out by the participants and fill the gamification elements presented in the literature. 34
Concerns were presented about games triggering epileptic seizures or about the fact that the senses in VR are focused on the virtual environment and how this could cause insecurity in users - these concerns must be considered by SG designers and the rehabilitation experts' involvement in the team should help clarify and reassure the end-users. Image frequency and refresh rate, screen quality, colour and intensity choices must be well thought out to avoid epileptic seizures and extra caution must be taken in immersive scenarios to be safe.
In relation to the methods used by the authors, in research, each investigation method gives different information, and several methods should be used in a complementary way. The methodology must be selected according to the nature or phase of the study. For instance, randomized clinical trials are the gold standard of clinical studies with the intend to validate the effectiveness of an intervention and use mostly quantitative methods. 53
The participatory approach in the development of SG intends to follow a UCD approach, in which quantitative methods such as questionnaires are turned into qualitative methods such as semi-structured and structured interviews and focus groups with users. 54 Understanding the perspectives of the health professionals, stroke survivors and SG designers can contribute to improving the efficacy and effectiveness of clinical interventions and turn them more equitable and humanized. 45
This methodology makes sense as a generalization is not a guiding principle in customization of computer technologies for people with disabilities. The qualitative research uses smaller samples than quantitative research, but the choice of participants is crucial - they should represent the stakeholders and motivate participants to communicate with the investigator. 46
Based on the results of this work, the authors started the design of a VR-based SG for upper limb rehabilitation, taking inspiration from the traditional whac-a-mole pastime (Figure 6). The game narrative supports two modes: one version to be played with any arm to pick a virtual hammer and hit targeted objects, and another version, a mirror version, which converts a traditional rehabilitation approach to a VR setting, providing the illusion that the arm affected by the stroke is moving. The prototype of the whac-a-mole SG 390x292mm (59 x 59 DPI).
Three levels of difficulty were designed, changing the number of moles and the frequency of appearance, allowing survivors to customize their experience, without penalties; even when the player fails to hit a mole in the allocated time: no points are lost; the user still has opportunities to repeat and succeed. To be immersive, the authors’ choice was to use the Oculus Quest 2®, since it offers inside-out marker less tracking without any additional hardware, requires little environment setup and doesn’t need a computer to run. This SG is meant to offer an opportunity for patients to have fun, doing an activity difficult or even impossible for most of the participants in real life, and to activate the affected brain area through the affected upper limb movement or VR mirror therapy. Next step will be testing the SG with the same participants in order to obtain their opinions related to the levels of difficulty, details of the scenario, and other elements, and collect their suggestions to improve engagement; afterward the aim is to involve a larger number of stroke patients from the same association.
Conclusions
The design of SG should consider the post-stroke phase and adapt it to the individual´s needs, preferences, and capabilities. SGs are possible tools to persuation stroke survivors to use the upper limb or to game in a way which promotes the paretic upper limb cortical area activation; combating depression and isolation is also a goal. However, SG design for chronic stroke survivors is still not explored to a high extent. To reach more solid conclusions, the scientific community must explain and discuss the game design aspects of clinical trials in depth, share experiences and learn with the several approaches.
SGs with their attractive character could contribute to increasing motivation and repetitive training. Users are introduced to an environment that can provide them with both realistic and unrealistic actions, so they can interact as if they were in a real environment with virtual objects, in the virtual world. Each study, guided by its own needs, created and used its own innovative VR games, which often present different software. Despite the diversity of activities in which patients in each study are invited to participate, there are some common goals behind them. Performing elbow and sholder flexion and shoulder abduction movements are always key goals that almost all researchers try to incorporate into their virtual reality software. The important thing for this research is the involvement of patients in the design of games. Their experiences help researchers to develop appropriate scenarios of a faithful simulation of their daily lives for use themselves that will help them cultivate special skills for dealing with a situation in real life.
During the SG development process, qualitative and quantitative studies must be used according to the nature and phase of the study. In UCD, qualitative studies are useful to understand the users’ opinion; quantitative methods are crucial for clinical studies which intend to test the effectiveness of a solution in several measurable outcomes. A UCD is present in the more recent conceptual frameworks in rehabilitation in general and in persuasive SG for upper limb after stroke in particular. More clinical studies applying those frameworks will be important to create guidelines to design SG effective in their goal of being persuasive and benefiting the user, considering a bio-psycho-social approach: promoting not only function but also well-being and social participation.
Footnotes
Acknowledgements
The authors thank Portugal AVC for their support and participation in the study.
Author contributions
Paula Amorim has given substantial contributions to the conception or the design of the manuscript, Paula Amorim, Helder Serra, Beatriz Santos Sousa and Paulo Dias to acquisition, analysis and interpretation of the data. All authors have participated in drafting the manuscript, Miguel Castelo-Branco and Henrique Martins revised it thoroughly All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially funded by FCT - Fundação para a Ciência e a Tecnologia (FCT) I.P., through national funds, within the scope of the UIDB/00127/2020 project (IEETA/UA, ![]() ).
).
Ethical approval
The study was approved by the University of Beira Interior Ethics Committee.