
Abstract
Suicide is strongly associated with mental health and substance use disorders, which makes mental health- and substance misuse services important areas for suicide prevention. The aim of The Norwegian Surveillance System for Suicide in Mental Health and Substance Use Services is to describe all suicide deaths in Norway that occur within one year after contact with mental health and substance misuse services. The study uses a hybrid registry case series design. It consists of a yearly linkage between the Norwegian Cause of Death Registry and the Norwegian Patient Registry, which is linked with a questionnaire. The linkage is conducted by using a cryptographic hash function of the deceased’s personal id, thus ensuring that the project can link data across sources without the use of directly identifiable information. This indirect linkage ensures the deceased’s confidentiality. Moreover, the The Norwegian Surveillance System for Suicide shows how administratively collected data can be harnessed and used for surveillance. Both use of hybrid registry designs and linkage through cryptographic hash functions might contribute to the development of health informatics as well as quality improvement in health care.
Keywords
Background
Suicide is an important contributor to premature mortality, contributing to nearly two million years of life lost in Western Europe in 2016. 1 The causes of suicide are multi-factorial and complex, but mental disorders are an important risk factor for suicide.2,3 Because of the strong association between suicide and mental disorders, mental health services are important areas for suicide prevention. Internationally, the prevalence of contact with in- or outpatient mental health services is approximately 25% in the last year before suicide, with large variations between countries. 4 In Norway, with large publicly funded services, over 40% of people who die by suicide had contact with mental health- or substance misuse services within the last year. 5 To more efficiently prevent suicide in connection with care, more knowledge regarding the patients who die and their contact with and treatment in services for mental health and substance use is crucial to develop and implement precise and effective suicide prevention.
In the UK, the National Confidential Inquiry into Suicide and Safety in Mental Health (NCISH)6,7 has collected national data on patients who died by suicide who had contact with mental health services in the last year before suicide for over 20 years. Their overall aim is to improve safety for mental health patients, by examining circumstances leading up to the suicide, identifying related factors, and recommending measures based on the findings. 8 The NCISH database consists of information collected from a clinical survey completed by the consultant psychiatrist who was caring for the patient. NCISH has provided valuable knowledge on this important high-risk group for suicide (for example 9–11), which has been the basis for service recommendations, where some have been found to reduce the suicide rates in the services. 12
The Scandinavian health registries, although initially developed for administrative purposes, have been an important data source for suicide research, and have provided information regarding suicide mortality and risk factors for suicide using prospective designs. 13 The use of a personal identification number unique to every citizen is an important element in many of the Scandinavian health registries. In Norway, the registries that are not based on consent, but contain personally identifiable information, is established after evaluation by the Norwegian government and demand that confidentiality issues are handled strictly. A dedicated key manager handles the personal IDs in the registries. Researchers can get access to data through a formal application process, but this requires that the study is aligned with the aims of the registries and all data needs to be relevant and necessary for the project.
A variety of approaches to registry studies have been developed. One of these approaches is a design that links registry data with other sources of data, which are called hybrid registry designs. 14 While data linkage is an important aspect of registry studies, hybrid designs refers to the linkage of registry data with other data not commonly included in registries, such as questionnaires. This design allows supplementing existing registry data with other relevant variables to enable other research questions, control different confounders and conduct more clinically relevant studies. When using traditional registry study methods, the registries can conduct or facilitate the linkage on behalf of the researcher. In hybrid registry studies, on the other hand, the researchers needs access to personally identifiable information to link data across sources. As mentioned above, this represents a significant data protection issue in registries not based on consent.
This paper aims to describe the design of a national hybrid registry surveillance system on suicide in mental health- and substance misuse services – The Norwegian Surveillance System for Suicide in Mental Health and Substance Use Services (NoSS). Furthermore, we will illustrate how such a national system can be developed to handle challenges regarding information security and confidentiality.
Methods
Aim
The primary aims of the NoSS are to (i) Identify all deaths by suicide in Norway that occur under or within 1 year after contact with secondary mental health services, and (ii) Collect systematic information about the patients, their treatment, and the circumstances regarding the suicide. Our secondary aim is to develop, implement and evaluate the effectiveness of suicide prevention interventions at a system level in the services. The project is based on the model developed by the NCISH. We will here describe the adaptations and modifications of the system to a Norwegian context.
Sample and setting
The sample includes all people in Norway who died by suicide or deaths by undetermined intent (ICD-10 codes X60-X84; Y10-Y34; Y87.2) from 01.01.2008 to 31.12.2023 and who had contact with secondary mental health services (adult and child and adolescent mental health services), private specialists practioners, or substance misuse services the year before suicide. The Norwegian health care system is universal and built on the principle of equal access for all inhabitants. Four regional health authorities control the provision of secondary health services across almost 30 health thrusts. Most hospitals are public hospitals, funded and owned by the state. In addition, there are a small number of privately owned hospitals and private specialist practitioners, but all of these are also funded by the public and operate on behalf of a public health authority through contracts. In this project, mental health- and substance misuse services refer to all publicly funded health thrusts in Norway providing specialist treatment for mental disorders and substance use disorders, including the private institutions and specialists in psychiatry or clinical psychology working under a contract with a regional health authority.
Data sources
We use data from three sources: The Norwegian Cause of Death Registry (NCDR), the Norwegian Patient Registry (NPR), and an electronic questionnaire. These sources are later linked using a unique project ID generated by a cryptographic hash function of the personal ID (see Figure 1), from here on called hashed ID. This linkage is further described in the section procedure while the generation of the project ID is described under infrastructure. Illustrates the design of the data collection system, including the flow of project ids and 11-digit personal IDs. Full lines represent direct registration (DR) and dashed lines represent prompted registration (PR). Colored lines and boxes are used to separate the different types of data, where yellow is data from secondary services for mental health and substance use, blue is registry data, and purple is the linkage key. The small grey boxes are time stamps, which correspond to the elements fully described in Table 1.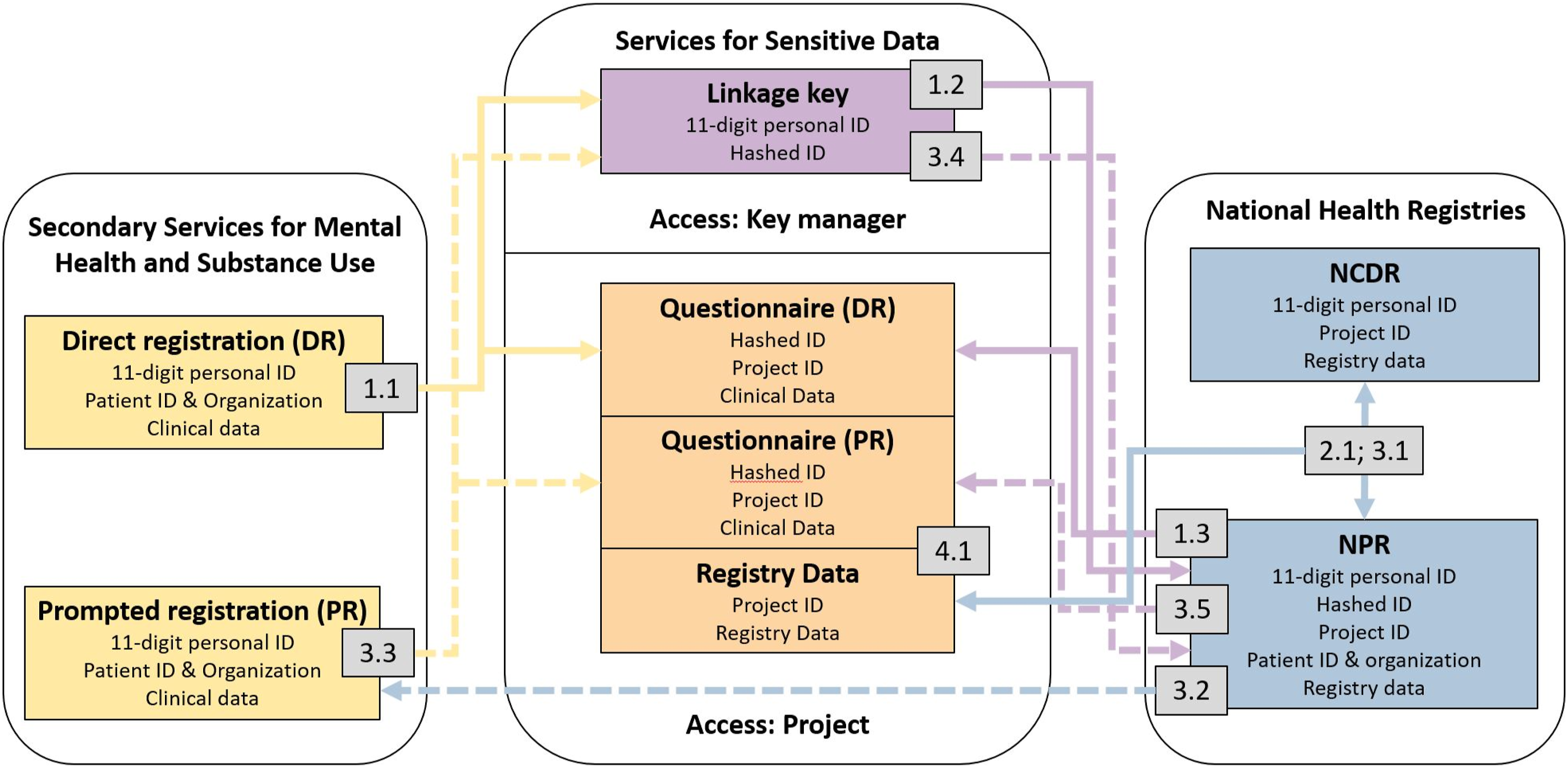
The Norwegian cause of death registry
The NCDR is managed by the Norwegian Institute of Public Health and is a national registry based on death certificates. The registry covers over 98% of all deaths in Norway, including people registered as Norwegian residents dying abroad. 15 The aim is to monitor causes of deaths and changes over time and provide data for statistics and research that can be used in the planning and quality assurance of the health care services and administration in Norway. 16 The reliability of the Norwegian suicide statistics is good, with a high percentage of reported suicides being confirmed as suicide. 17 ICD-10 codes with undetermined intent (Y10-Y34, Y872) are not frequently used, varying between 0 and 35 deaths per year, 18 compared to approximately 600 suicides per year in Norway. In this project, information on gender, age, ICD-10 diagnoses for the cause of death, and date of death are retrieved from the NCDR.
The Norwegian patient registry
The NPR is owned and managed by the Norwegian Directorate of Health. It was established in 1997 by a private research institute but transferred to the Norwegian Directorate of Health in 2007. 19 The NPR contains information about all publicly funded treatment in secondary health services in Norway. This includes administrative data, patient demographics, and medical information such as diagnoses and reimbursement information. 20 Specialized health care services, including private institutions and specialists, contracted to the regional health authorities, routinely report these data to the NPR. A personal identification number unique to every Norwegian citizen is a key element in the registry and makes linkage to other registries possible. The NPR holds directly personally identifiable information back to 2008 for mental health services, and from 2009 and forwards for substance misuse services. Since 2010, the registry has coverage above 99% for mental health services and substance misuse services, and over 98% for somatic health services. In child and adolescent mental health services and for private mental health specialists, the coverage is over 99% and 97%, respectively, from 2012. 21
For the current project, the datasets are from mental health- and substance misuse services, child and adolescent mental health services, private specialists (both somatic and mental health), and somatic health services. Information regarding contact with services (including the type of service, service modality, and dates of contact), ICD-10 diagnoses, treatment procedures, and use of coercion are retrieved from the NPR.
Web-based questionnaire
The original questionnaire developed and used by the NCISH, collects detailed clinical information from a clinician who was responsible for the patient’s care. Among other things, the questionnaire includes the patients’ demographic information, psychosocial history, physical illness, lifetime history, recent life experiences, substance use, treatment history, and details about the suicide. The NoSS has translated and adapted the survey used by the NCISH to a Norwegian context using the web service nettskjema.no. Nettskjema.no is Norway’s most secure and most used solution for data collection for research. It is owned by the University of Oslo and is also used by hospitals, educational institutions, and private companies. The NCISH has permitted translation and adaptation of the questionnaire, and the questionnaire has been used in a pilot study in Agder county in southern Norway. 22 Items that could be retrieved from the NCDR or the NPR have been removed from the questionnaire, and such data are retrieved from the registries (described above). Adaptations include legislation and names of services. Furthermore, items relevant to substance misuse services were added, such as detoxification and medically assisted rehabilitation. An updated example of the questionnaire is available on the NoSS webpage. 23
Design
The project uses a hybrid registry design where data from the national registries are linked with a questionnaire from clinicians who had the last contact with the patient. Figure 1 illustrates the design of the current project. Cases are identified by the registry linkage between the NCDR and the NPR.
Procedure
Overview over the procedure.
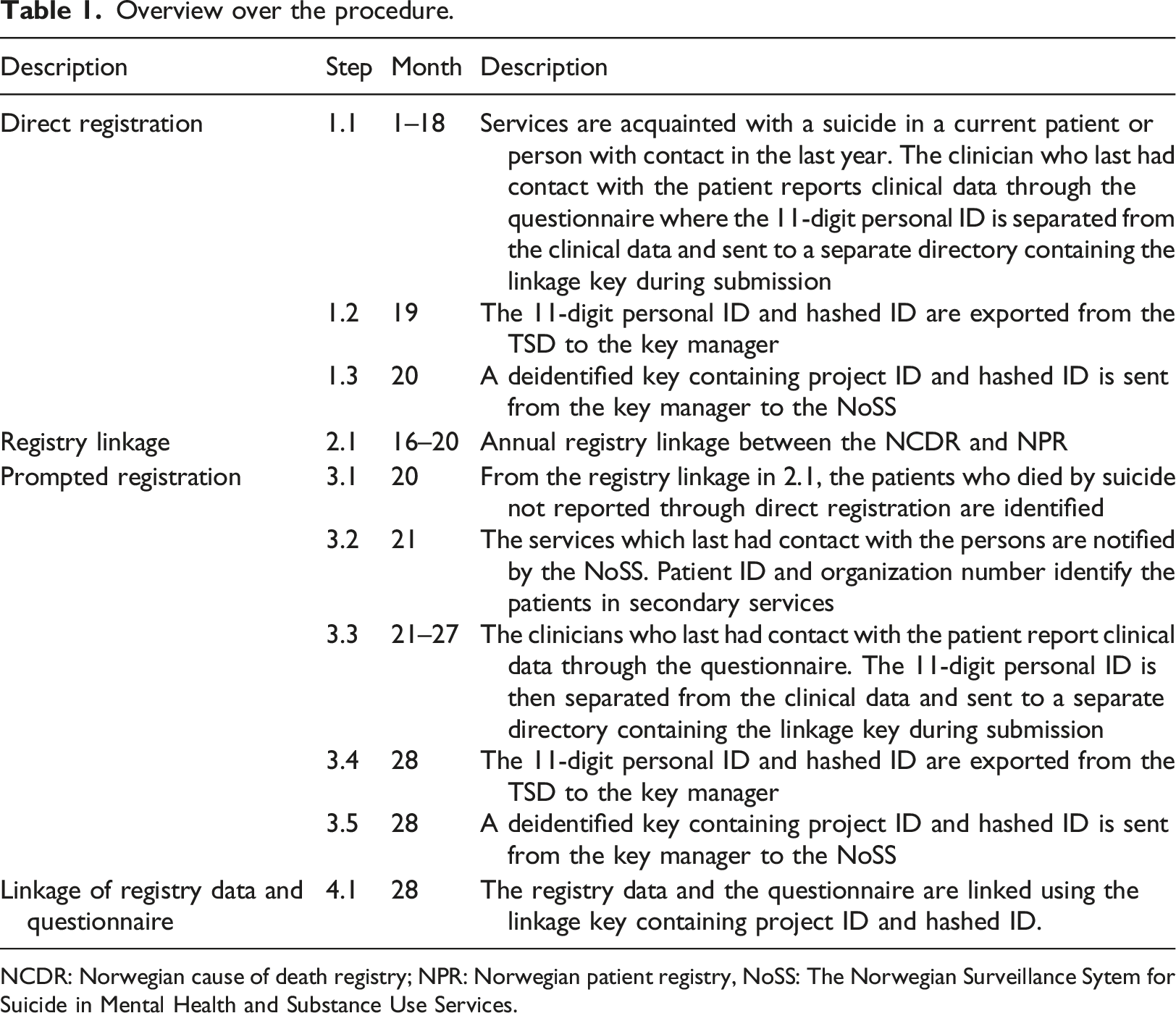
NCDR: Norwegian cause of death registry; NPR: Norwegian patient registry, NoSS: The Norwegian Surveillance Sytem for Suicide in Mental Health and Substance Use Services.
Direct registration
When services are acquainted with a patient’s suicide, the clinicians is obligated to report the suicide directly to the NoSS through the electronical questionnaire (before the registry linkage is conducted), which is described as step 1.1 in Table 1. Direct registration is continuous over the project period and is illustrated by the full lines in Figure 1. During submission, the 11-digit personal ID and the clinical data are sent to separate directories (further described under infrastructure). When the registry linkage (described below) for a calendar year is finished, the direct registration for that year is closed, and the linkage key is exported by the key manager in step 1.2. In step 1.3, the key manager then uses the 11-digit personal ID to link hashed IDs and 11-digit personal IDs to the project ID. Afterward, a linkage key containing hashed ID’s and project ID, which makes it possible to link the questionnaire and registry data, is sent to the NoSS. Direct registration will continue for later calendar years.
Registry linkage
In the second phase of the procedure, an annual linkage between the NCDR and NPR is conducted in step 2.1. First, all persons registered with suicide and deaths by undetermined intent (X60-X84; Y10-Y14; Y87.2) as the underlying cause of death are extracted from the NCDR. Then, the project ID is generated by the NCDR, and a list of the 11-digit personal ID and the project ID is sent to the NPR. Next, the NPR links the personal IDs with data. People who died by suicide and are registered with contact in adult mental health services, child and adolescent mental health services, substance misuse services, private mental health specialists, or registered on a waiting list in the mentioned services within one year before the date of death are included. When the linkage is finished, NCDR and NPR deliver data to the project. The project ID from the NCDR allows linkage between the two sources within the project.
Prompted registration
When the registry linkage is complete and the direct registration for the calendar year is closed, the third phase of prompted registration phase starts. Prompted registration is illustrated through the dashed lines in Figure 1. In step 3.1, the key manager sends the NoSS a list of patients included in the registry linkage that has not been directly registered for the calendar year, which includes the organization number and patient ID, which is an arbitrary number that identifies a patient within a health organization from the NPR, from the key manager. Clinicians in the services are in step 3.2 inquired to register all persons who died by suicide after contact with the services in the last year in the NoSS. The inquiry is made by the NoSS based on the patient ID. Organizations in the services are directly contacted by NoSS with lists of patient to report with organization number and patient ID. Prompted registration then starts, and is conducted using the same procedure as described under direct registration (step 3.3). Further prompts are made at approximately two months intervals.
Prompted registration for a calendar year is ended after approximately six months, after prompting and assisting registration. The key manager then extracts the linkage key (step 3.4) containing an 11-digit personal ID and the hashed ID for the prompted registration, which subsequently is linked with the project ID. As in direct registration, the linkage key containing hashed ID and project ID is delivered to the project. Again, the hashed ID and the project ID from the NCDR are linked using the personal ID, and a list containing the hashed ID and project ID is returned to the project from the NPR (step 3.5).
Linkage of registry data and questionnaire
After the direct and prompted registration phases are finished, the registry data and the questionnaire are linked using the hashed ID and the project ID in the final step (4.1) of the procedure. Persons reported in the direct registration that are not identified in the registry linkage is then deleted from the database. For the first calendar year in 2018, 18 registrations were deleted. From 2019 and forwards we have discouraged direct registration when the clinicians are in doubt regarding the cause of death. As such, the mentioned number of deletions probably represents a maximum number. Registration of a calendar year is then completed.
Infrastructure
The project uses a secure research data infrastructure, the TSD (in Norwegian, Services for Sensitive Data) to collect, store and analyze data. TSD is designed for storing and post-processing sensitive data in compliance with the Norwegian Personal Data Act, which incorporates GDPR -the European Data Protection Regulation, and Health Research Act. TSD is developed and maintained by the central IT department (USIT) at the University of Oslo and supports research activities at Norwegian public institutions.
TSD provides virtual servers with desktop backup systems, storage systems, high-performance computing facilities, and databases all confined within a highly secured environment. Access to the infrastructure of the project in TSD is controlled by project admins, and a two-factor login is required to access the TSD. Data collected with questionnaires created with Nettskjema.no is in memory encrypted and made available inside the project in TSD. TSD is a part of the European Open Science Cloud, 24 thus making data as available as possible and as closed as needed. All data in the project is handled and analyzed in TSD.
The questionnaire is available online with no login required. It is hosted at the University of Oslo and all data is stored in the infrastructure of the University of Oslo. The questionnaires use interlinked forms. First, an inclusion form containing a unique personal identifier is followed by the questionnaire. For both forms, the unique personal identifier is used as an input to a cryptographic hash function. Then for the questionnaire, the 11-digit personal identifier is replaced with an encrypted hash of the identifier during submission and is delivered to the project database where the project members have access. The hashed ID will serve as a unique project ID that enables the project to link the questionnaire and registry data. The inclusion form with the linkage key (containing the unique personal identifier and the hashed ID) is delivered to a separate folder where only the key manager has access.
The project is set up with granular access within TSD with one dedicated area to the project and the key manager respectively. Group moderators govern access to groups with privileges allocated to the project administrators and the key manager respectively. Access is granted through requests to the TSD. It is thus impossible for members of the project to access the area of the key manager and vice versa. No one in the project has access to both the dataset and the linkage key, and the data are only available with de-identified IDs.
All data in the project is delivered to an access-controlled PostgreSQL database. Database storage offers reliable and unitary storage of data across sources. Moreover, linking data between the three sources is feasible. Data from the questionnaires with encrypted IDs are automatically imported into the database upon submission. Registry data is manually imported yearly. Database schemas are used to store questionnaires and registry data separately while simultaneously allowing linking the data between schemas.
Discussion
In this protocol we have described a national suicide surveillance system, which uses available registry data and collects information from clinicians without the researchers having access to directly identifiable information, thus ensuring the deceased patient’s confidentiality. To our best knowledge, this is the first national project examining deaths by suicide and deaths by undetermined intent using a hybrid registry study design that combines registry data with a questionnaire. Consequently, the advantages of the Scandinavian health registries can be combined with cross-sectional surveys, to overcome some limitations of registry-based research; the lack of relevant variables recorded in most such administrative registries.
The consequence of using a hybrid registry design will be that you gain relevant information regarding the cases, while you miss the opportunity to use non-exposed controls. As described in this protocol we can add clinical variables to the data, thus describing the patients using variables that are specifically relevant for suicide and suicide prevention. While the current project utilizes national registry data, it does not use standard large-scale registry data designs such as nested case-control or cohort designs. While lacking the strength of a prospective design, the combination of registry data and a clinical questionnaire gives more flexibility, since changes can be easily made in the questionnaire without tedious and resource-demanding changes in reporting routines to the large national registries. New variables can be added to monitor specific trends or new interventions. It also makes user involvement easier, since feedback and experiences can actively be used to improve the questionnaire.
A difference between the NoSS and NCISH is the use of national registry data and the inclusion of substance misuse services and private mental health specialists. Since Norway has nationwide health registries, several relevant variables can be retrieved from the registries. These include ICD-10 diagnoses and treatment history to mention some. An advantage of using the registries is that we have access to the entire use of services across health thrusts from 2008 and forwards. This gives us access to the ICD-10 codes for all contacts in services for mental health and substance use and information regarding these contacts, such as dates, sectors of contact, and level of care. The limitation is that clinical nuances regarding service use, reported in the original questionnaire are lacking. An example is the potential under-recording of comorbidity in the national registries. In sum does the adaption increase breadth at the cost of losing some depth of analysis regarding the last contacts.
The use of registry data makes the questionnaire briefer and less time-consuming for the clinicians, which could increase the response rate. Since both substance misuse services and publicly-funded private mental health specialists report data to the NPR, the inclusion of these services will contribute to a more comprehensive overview of suicide in all secondary mental health services. There are few studies to date focusing on suicide after contact with these services compared to mental health services, and the inclusion of substance misuse services and private mental health specialist will also enable the opportunity to study the overlap with these services and mental health services.
Another advantage of using as much registry data as possible is that important information such as ICD-10 diagnoses are reported before the patient died by suicide. This means the clinicians were not biased by the suicide when registering the diagnoses, except for the small minority of patients dying while under inpatient care. On the other side, diagnoses, and other clinical data reported to the national registers are routine clinical and administrative data, not originally intended for research purposes. This implies that both the reliability and validity of some variables might be unknown or questionable. Studies have found satisfactory correspondence between diagnoses in the NPR and structured interview-based diagnoses for severe mental disorders, 25 but with a lower correspondence between diagnostic interviews and the registry for major depressive disorder, anxiety disorders, and alcohol use disorders.
Another advantage of the design described in this protocol is the development of a national hybrid registry system that can reliably link registry data and a questionnaire without the researchers having access to directly personally identifiable information about the deceased such as name, address, and the 11-digit personal ID. Personal IDs are necessary to reliably link data from different sources, but in this study, they are replaced by an algorithm that creates a project ID of the personal ID. This is an important asset of the design and infrastructure when investigating death by suicide, as there is no way to obtain informed consent, and therefore more strain is put on the protection of individual data.
This data collection system shows that routinely collected registry data can be harnessed and linked with specific questionnaires without the use of directly identifiable personal information. Routinely collected data, such as national registry data or electronic health records, are important sources of data. However, they often lack detailed information needed for quality improvement regarding a specific subject, in this case, suicide after contact with secondary services. Quality improvement systems that monitor developments and can give recommendations based on national data, as described here, is thus important. To develop, implement and evaluate suicide prevention in the services, detailed and nationally representative data regarding the characteristics of the people who die by suicide is needed. The NoSS is designed to serve this purpose and might prove an important addition to other approaches aimed at preventing suicides in these important high-risk groups. Both use of hybrid registry designs and linkage through cryptographic hash functions might contribute to the development of health informatics as well as quality improvement in health care. These advancements are relevant for several other studies that seek to combine routinely collected data with other sources of data.
Footnotes
Acknowledgements
We thank the National Confidential Inquiry into Suicide and Safety at the University of Manchester for the inspiration to develop the Norwegian Surveillance System for Suicide, and for their welcoming cooperation and support over the years and for the approval to adapt and use their original clinical survey. We also thank the Norwegian Directorate of Health, the Norwegian Patient Registry, The Norwegian Cause of Death Registry and the University Centre for Information Technology for their cooperation and their contribution to the development of this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This project has an exemption from the patient confidentiality given by the Norwegian Directorate of Health. It is also approved by The Regional Committee for Medical Research South-East (ref: 32494).