
Abstract
Keywords
Introduction
Pregnancy contributes to overweight among women. Postpartum weight retention may lead to the development or aggravation of obesity and significantly affect women’s health postpartum, during subsequent pregnancies, and later in life.1,2 Studies have shown that interpregnancy weight retention increases the risk of several adverse pregnancy outcomes (gestational diabetes mellitus, preeclampsia, cesarean delivery, and macrosomia) even if women maintain a normal BMI.3–5 Furthermore, postpartum women’s maternal health needs are often unmet, leaving these women unprepared for the physical changes related to pregnancy and birth, such as the physical impact on the body caused by the pregnancy and birth, the mental well-being and the sleep and fatigue.6–8 In a recent study associated with the current research, we found postpartum women to need assistance in changing their behavior to promote a healthier lifestyle. 9 Mothers lack high-quality information from healthcare professionals (HCPs) about postpartum bodies and exercise, and they need tools to understand and prioritize their health risks; thus, interventions are needed to assist and motivate postpartum women in attaining a healthy lifestyle. 9
Interventions based on information and communication technology (IT), such as mobile applications (apps), are increasingly used in healthcare delivery and can support individuals’ self-management. 10 Furthermore, Danish women of the childbearing age use smartphones daily and are familiar with app use 11
However, a recent systematic review on IT-based interventions promoting a healthy postpartum lifestyle found no evidence of significant health effects, suggesting that adherence to such interventions is challenging. 12 These findings demonstrated the need for IT design to reflect on postpartum women’s lifestyle-change motivations and adherence. Engaging users and stakeholders in the IT development phase can develop interventions that are not only relevant but also user-friendly while meeting users’ needs. 13 Accordingly, the current study aimed to develop an IT intervention through close collaboration with users and stakeholders, incorporating motivational features.
Methods
Overview of the participatory design phases, research methods and user activities, and behavior change wheel integration.
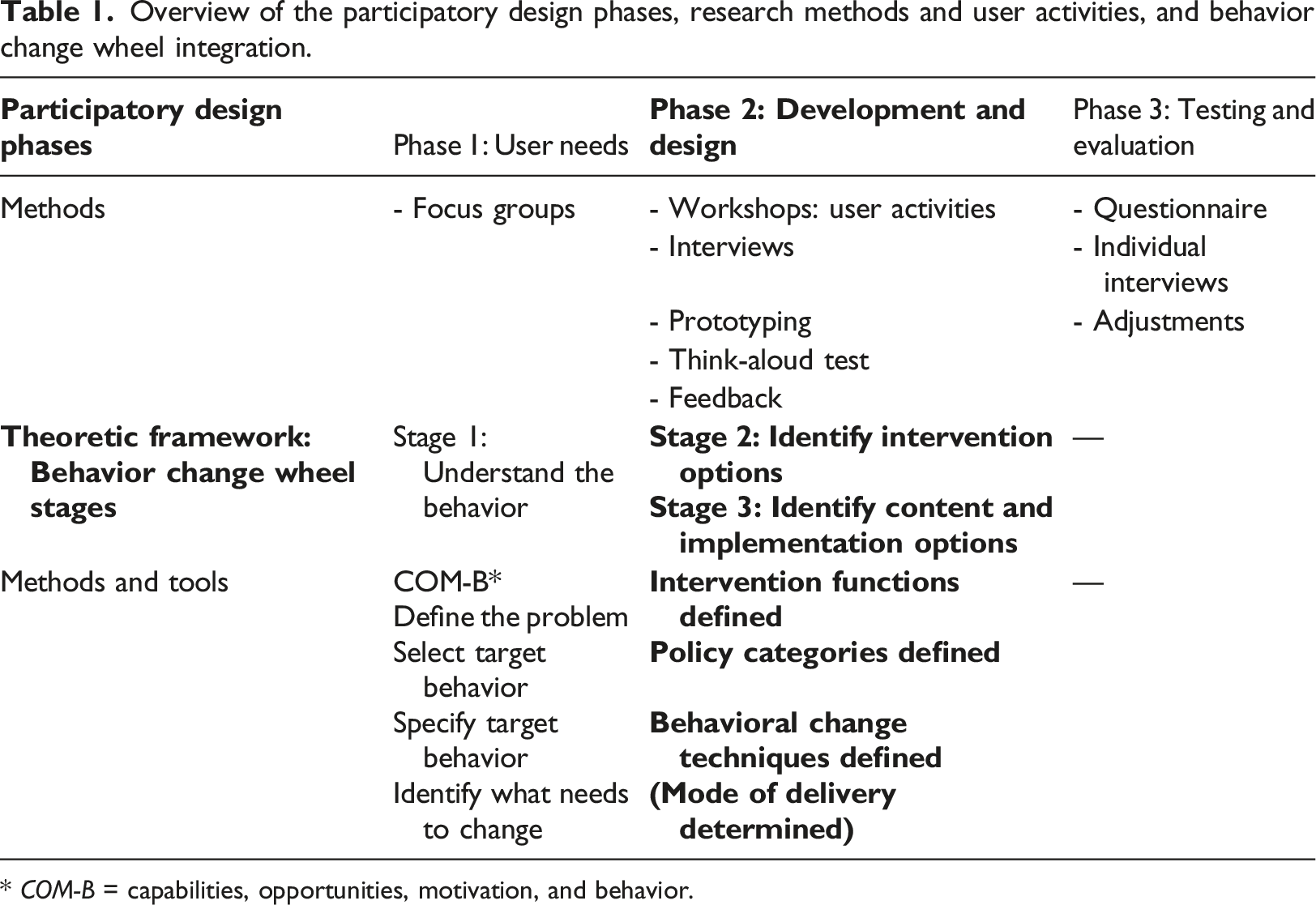
* COM-B = capabilities, opportunities, motivation, and behavior.
The behavior change wheel (BCW) is a theoretically founded framework for designing behavioral-change interventions systematically. 19 Applying the BCW framework ensures a systematic approach to determining postpartum women’s behaviors that must change so that they can attain a healthier lifestyle, as well as intervention functions, policy categories, and behavioral change techniques (BCTs) that could encourage these changes. Thus, this solution is based on behavioral change theory. The BCW framework was integrated into the study’s PD design to systematically define intervention types. Carvalho et al. have used a similar approach. 20 BCW comprises three stages: (1) understanding a behavior, (2) identifying intervention options, and (3) identifying content and implementation options. 19 In Phase 2 of the current study, the second and third BCW stages were applied, except for the implementation. During the second stage, intervention functions and policy categories were identified. Based on the work of Michie et al., 21 intervention functions include education, persuasion, incentivization, coercion, training, enablement, modeling, environmental restructuring, and restrictions. Policy categories include communication or marketing, legislation, service provision, regulation, fiscal measures, guidelines, and environmental or social planning. During the third stage, BCT were chosen. BCTs were selected from a taxonomy of 93 hierarchically clustered techniques. 22
Setting and participants
Two workshops and four individual semi-structured interviews in addition to feedback sessions with seven participants, and think-aloud tests with six women, were conducted between August 2019 and May 2020. Figure 1 provides an overview of this study’s design and development processes. Overview of the study’s design and development processes.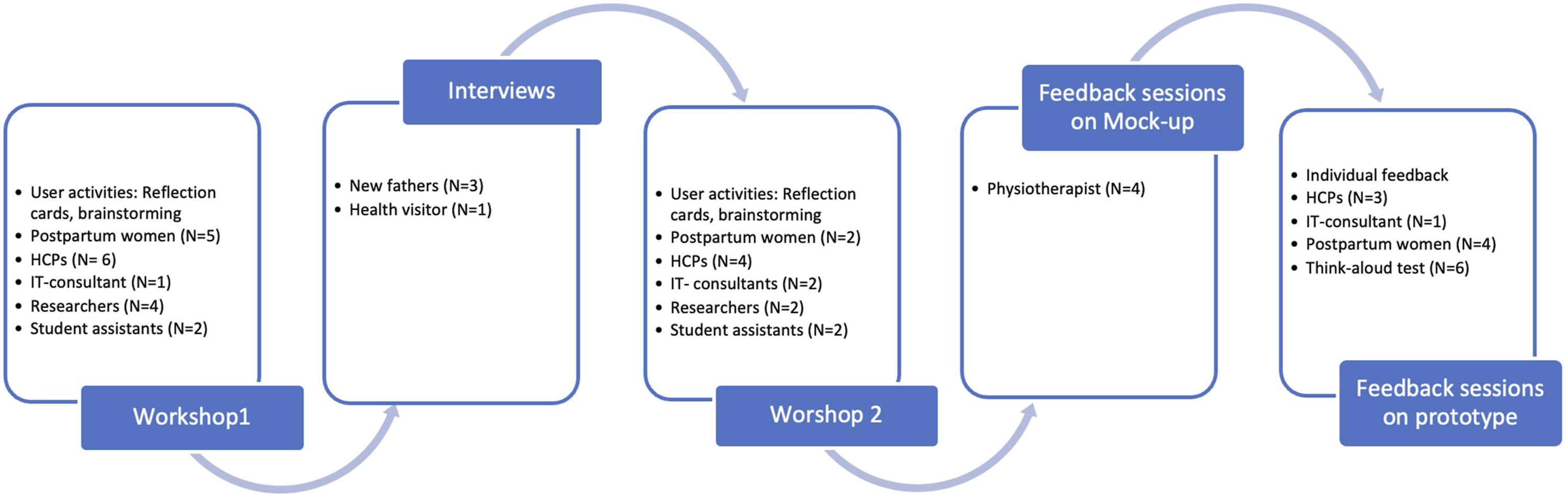
The study’s workshops were held on the premises of University College Lillebælt, Odense to ensure an inspiring yet neutral setting, rather than a hospital setting. Postpartum women and their partners, various health care professionals (HCP) with practical and professional knowledge about postpartum bodies, IT experts, and researchers were invited to the workshops.
Workshop and feedback-session participation.
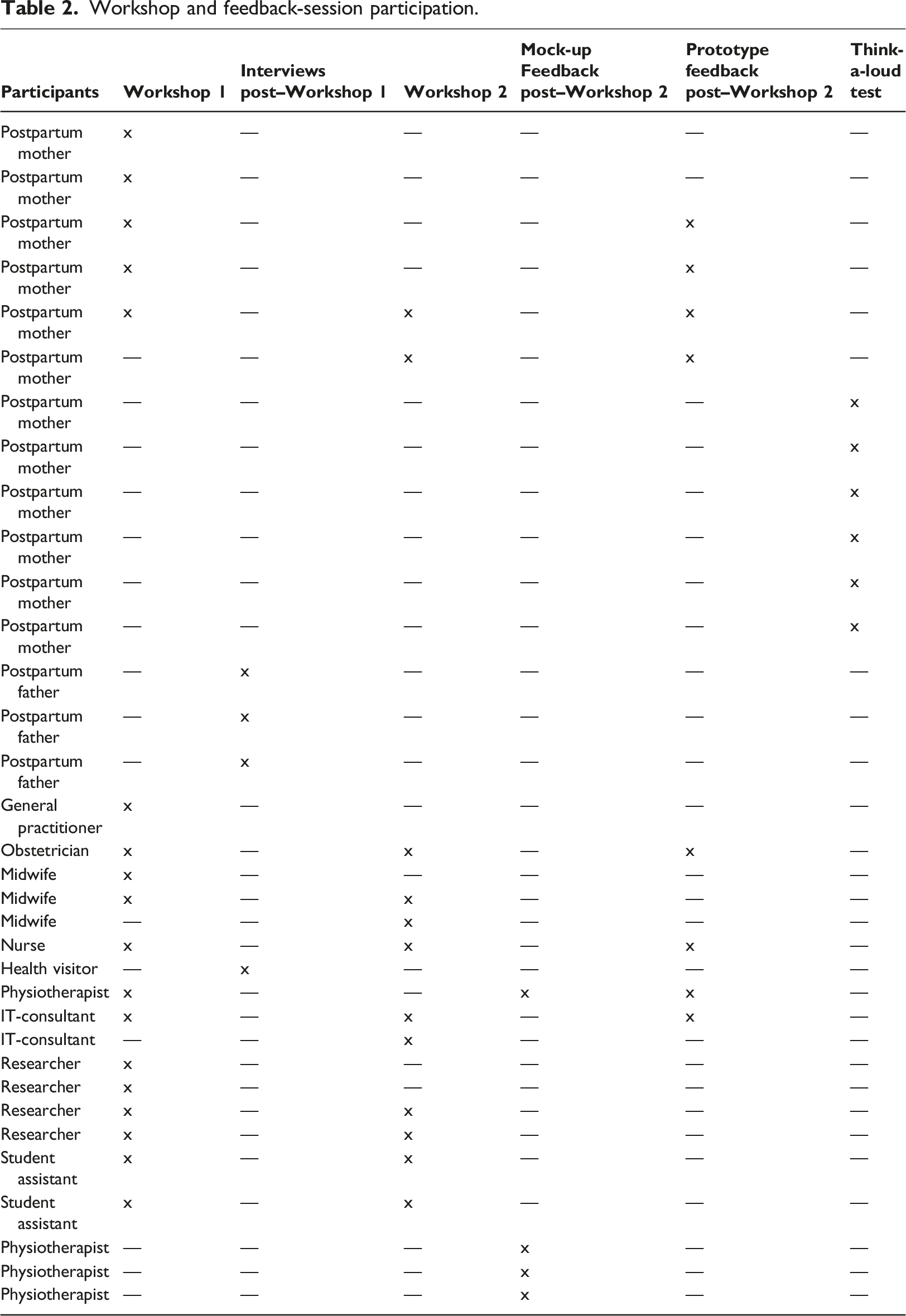
To accommodate our finding that close networks significantly affect postpartum women’s opportunities to live a healthy lifestyle, 9 we invited both mothers and fathers to this study’s workshop. Unfortunately, only mothers signed up to participate. Similarly, we were unable to recruit health visitors (municipal nurses who follow families with a newborn baby). Therefore, we conducted individual semi-structured interviews with representatives from these two groups to ensure their input in our solution’s development. Additionally, the physiotherapist who participated in the first workshop could not participate in the second workshop, so we presented her and three of her colleagues with the results and mock-up of Workshop two to obtain their feedback.
Workshop 1
Workshop 1 took place in August 2019. It aimed to co-create mock-up content. Participants were divided into two groups—one with postpartum women and the other with HCPs and the IT expert—to ensure the former group did not feel overruled by HCPs’ presence. A research team member was present with each group. Participants were presented with our findings from the first PD phase to obtain a collective understanding of the research problem. Next, the usual healthcare steps that the postpartum women would undergo (their user journey) were presented. All participants were asked to brainstorm about the user journey and whether they felt any points were missing or needed to be changed. Successively, they discussed their individual thoughts with their group. Participants were then divided into mixed groups of HCPs and new mothers to enhance mutual learning. Using reflection cards, they then proposed different ways to support a healthy postpartum lifestyle using IT.
Individual interviews
Three fathers and one health visitor participated in the study’s supplementary interviews. These interviews aligned with Workshop 1’s content. Thus, these participants were presented with the Phase 1 PD findings and the Workshop 1 results, which they were invited to comment on.
Workshop two
Workshop two took place in September 2019. It aimed to collect feedback on the Phase 2 mock-up and provide background knowledge for a prototype solution’s development. Since some participants had been unable to participate in Workshop 1 due to their schedules (see Table 2), the knowledge gathered from Workshop 1 was presented to establish a common understanding. Participants had an opportunity to provide feedback on this presentation’s content. Next, a user journey was presented for the proposed app and mock-ups. Participants were asked to reflect on and discuss these materials and then provide feedback. Because fewer participants were present compared to Workshop 1, only one group was formed. Participants’ individual feedback was successively obtained before the discussion opened to the whole group.
Feedback sessions
Once feedback was provided by the physiotherapists post workshop 2, the prototype’s content was developed. Feedback on this content was obtained individually from some workshop participants (see Table 2).
Ethical concerns
This study complies with the Declaration of Helsinki. 23 Prior to each workshop or interview, all participants received oral and written information about the project before signing an informed consent form. They could, at any time, withdraw their participation. All participants consented to the potential use of data from the workshops and interviews, including pictures, for this project. The study was approved by the Danish Data Protection Agency (case no. 17/43,487). It was also submitted for assessment to the Scientific Ethics Committee, who determined that their approval was unnecessary, according to the Danish legislation.
Analysis
Both workshops were filmed, and two student assistants studying multimedia design helped take notes and pictures. At the end of each workshop, all notes were gathered. The interviews were recorded and transcribed using NVIVO by the first and fifth authors. The transcribed text was systematically condensed for analysis. 24 Each statement from the study’s interviews and workshops used in this article were translated from Danish to English.
Results
Workshop 1 and the post-Workshop 1 interviews provided the following suggestions for an intervention supporting a healthy postpartum lifestyle.
A lack of focus on postpartum bodies
HCP participants were unaware of who—if anyone—should be responsible for discussing postpartum lifestyle with new mothers, and they regarded this topic as being unprioritized. Participating mothers felt that they lacked information and were unsure how to exercise postpartum. Because of their insecurity, they preferred passivity to prevent harm to their bodies. One participant explained, I really felt insecure about which exercises to do and which to avoid. . . . I could just feel my body was different. . . . I had to find a private physiotherapist to get the right exercises and information. . . . I needed trustworthy guidance. (Postpartum woman)
Participating postpartum women searched the internet and social media for inspiration and information about postpartum bodies and exercise, though such sources’ credibility was often a concern. Thus, these women preferred information from HCPs with professional knowledge about postpartum bodies. These mothers’ diets had not received much attention, though most of these women knew they consumed too many sweets. Around the time of their births, these women had received leaflets from HCPs concerning postpartum bodies; however, it was commonly described by the participants that they had never read these materials.
Podcasts and exercise videos
Participants suggested podcasts and exercise videos to inform new mothers about a healthy lifestyle postpartum. The mothers proposed podcasts since most had already listened to podcasts when walking with their strollers. This content, they suggested, should focus on how to exercise and attain a healthy lifestyle postpartum, such as obtaining or maintaining healthy family diets. Participants also suggested that these podcasts should be delivered by postpartum health experts. The mothers proposed videos because this format allowed them to exercise at home while caring for their babies. However, they noted that such videos should not be excessively long since these women often lacked time to watch them.
Push notifications
Participants expressed positive preferences for push notifications. They considered push notifications a tool to increase app use, avoid information overload, and present information when needed. One participant explained, I think I will need some messages from the app so I don’t forget about it. . . . As a new mother, you tend to forget everything that is not baby-related. . . but I think I would use it [the app] if I got reminders. (Postpartum woman)
Tracking users’ own data
The participating mothers also requested a way to track their own data, such as weight, after the first postpartum months. Additionally, they wanted push-notification reminders about weighing themselves regularly.
The mobile application My Hospital
The mothers also suggested an app intervention, citing flexibility and easy updates about new podcasts, videos, and messages. They suggested that the My Hospital app (used by hospital patients in the Region of Southern Denmark) should be part of the intervention since they were already familiar with it from their pregnancies. Each department of the Region’s Hospitals can have one or more modules in the application. 25 Since the platform already existed, and it was possible to add the proposed content in a module in the application, there was no need for technical development between the two workshops. In addition, the platform is free of charge and lives up to European GDPR standards. Once the women are locked on the platform, they can give their consent to receive push-notification.
Mock-up
Workshop 1 resulted in a list of mock-up proposals. Prior to Workshop 2, a mock-up was created in collaboration with the IT specialist who had participated in Workshop 1. Thus, this process was iterative. The mock-up was presented on paper using a WoodPad (instead of an iPad), and one of its menus listed question marks, indicating to participants that they could change or adjust the mock-up. (Figure 2)
Workshop two focused on the intervention’s content. Podcast themes and which kinds of professionals should present the content were discussed. Exercise videos and push notifications were debated, as well as weight tracking and effective push-notification frequency that would not disturb users. One participant remarked, If I receive too many messages, I can also get annoyed, but nor should I forget about the app. Once or twice a week might be fine. (Postpartum mother)
Thus, the app’s push-notification format was determined. It had to refer to app content or offer good advice, given users’ individual postpartum weeks.
The podcasts were determined to require relevant information—for instance, about exercise and bodily expectations after pregnancy and birth.
Based on the presented user journey, when women should be informed about the app was discussed. The preferred time was at the end of pregnancy, when women remained motivated to take in new information. Finally, a name for the module was chosen by the participants: Healthy Together.
The participating physiotherapists were presented with the mock-up and content from Workshop 2. They agreed on the content but stressed the importance of not focusing on weight until a couple of months postpartum, after mothers’ bodies had adjusted from pregnancy.
The behavior change wheel
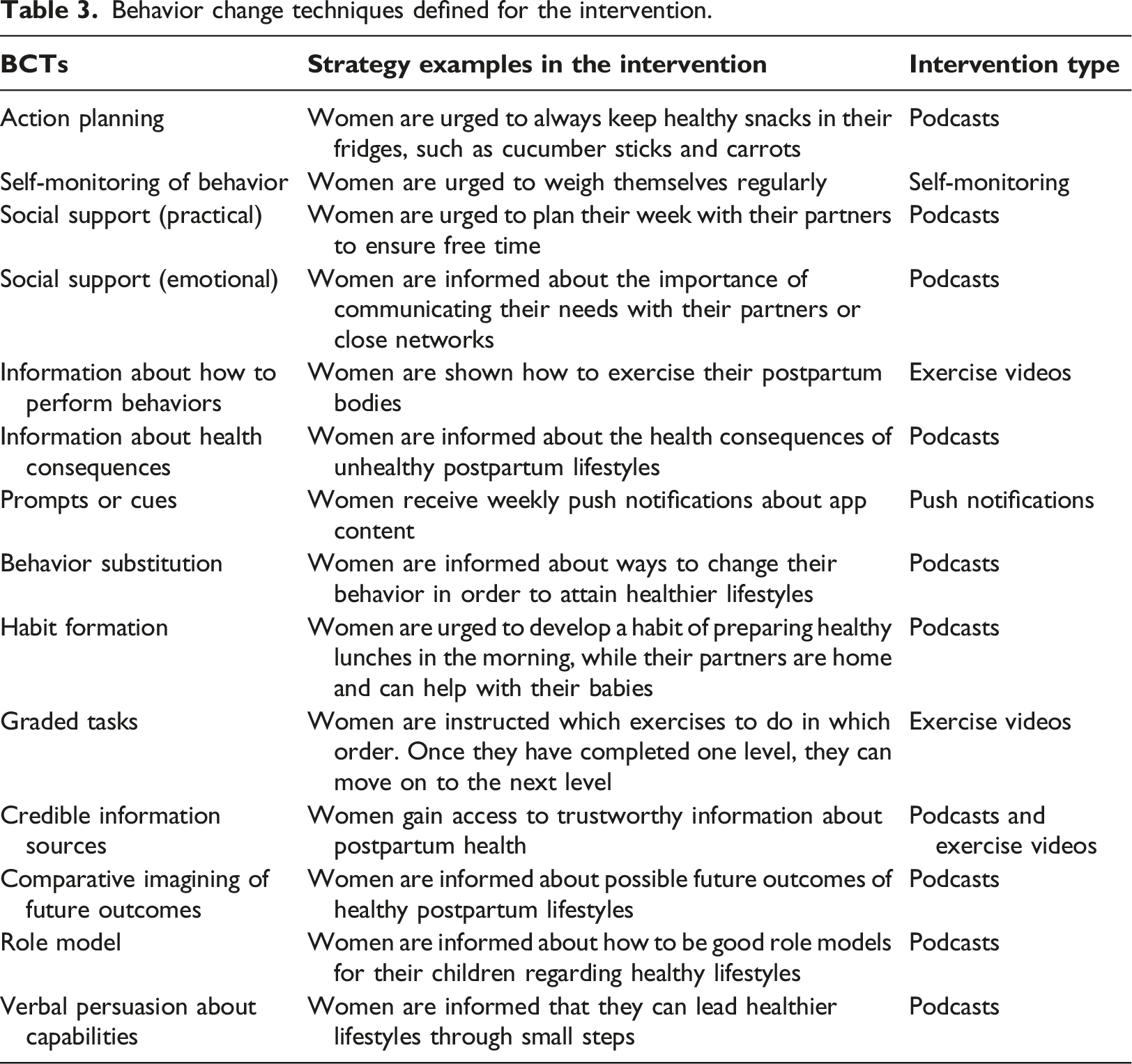
Based on the BCW framework, the intervention’s functions most relevant to the intervention were defined as: education, persuasion, training, and enablement. Podcasts applied education, teaching various relevant topics related to a healthy postpartum lifestyle. Exercise videos applied education, with a physiotherapist showing how to properly exercise after pregnancy and birth. The podcasts and push notifications applied persuasion, inducing positive feelings about a healthy lifestyle or negative feelings about unhealthy lifestyle risks. The intervention also applied training, giving users access to exercise videos they could use at home. Finally, it applied enablement, urging women to engage their partners or close networks with baby tasks.
Behavior change techniques defined for the intervention.
Mobile application content development
Based on this study’s workshops, interviews, feedback sessions, and BCW application, we decided the intervention should contain exercise videos, podcasts, weekly push notifications, and weight tracking.
The videos were produced by a physiotherapist specialized in gynecology and obstetrics. They instructed users how to exercise their postpartum bodies in order to regain the strength needed for normal activities. They also provided examples of how to avoid back and neck pain when lifting, sitting, and standing. These videos allowed postpartum app users to gradually progress from simple to more advanced exercises. One video also explained how to include babies in exercises.
Relevant HCPs for the podcasts were recruited through the hospital. A dietitian with extensive experience in lifestyle advice for pregnant women and diabetes patients was recruited, as well as a gynecologist specialized in contraception. A midwife was recruited online through a midwifery network. This midwife was also a sexologist and a new mother. Her husband participated in one of the podcasts, too. The physiotherapist who had participated in Workshop 1 was also recruited for the app’s podcasts.
We decided the app should reflect themes of postpartum bodies, the pelvic floor, attaining a healthy postpartum lifestyle (focusing on diet, exercise, and sleep), and eight-week postpartum follow-ups with general practitioners. In Denmark, all postpartum women are offered an eight-week check up at the General Practitioner. 26 At 10 weeks postpartum, app users would receive a push notification about tracking their weight. Weekly push notifications were determined to contain advice on a healthy lifestyle and reminders about the app’s content.
Because participating postpartum women wanted a simple app, the app was created with the main features shown below in Figure 3: About Healthy Together, Exercise Videos, Podcasts, My Data, Messages, Questionnaire, and Contact. Picture from Workshop 2.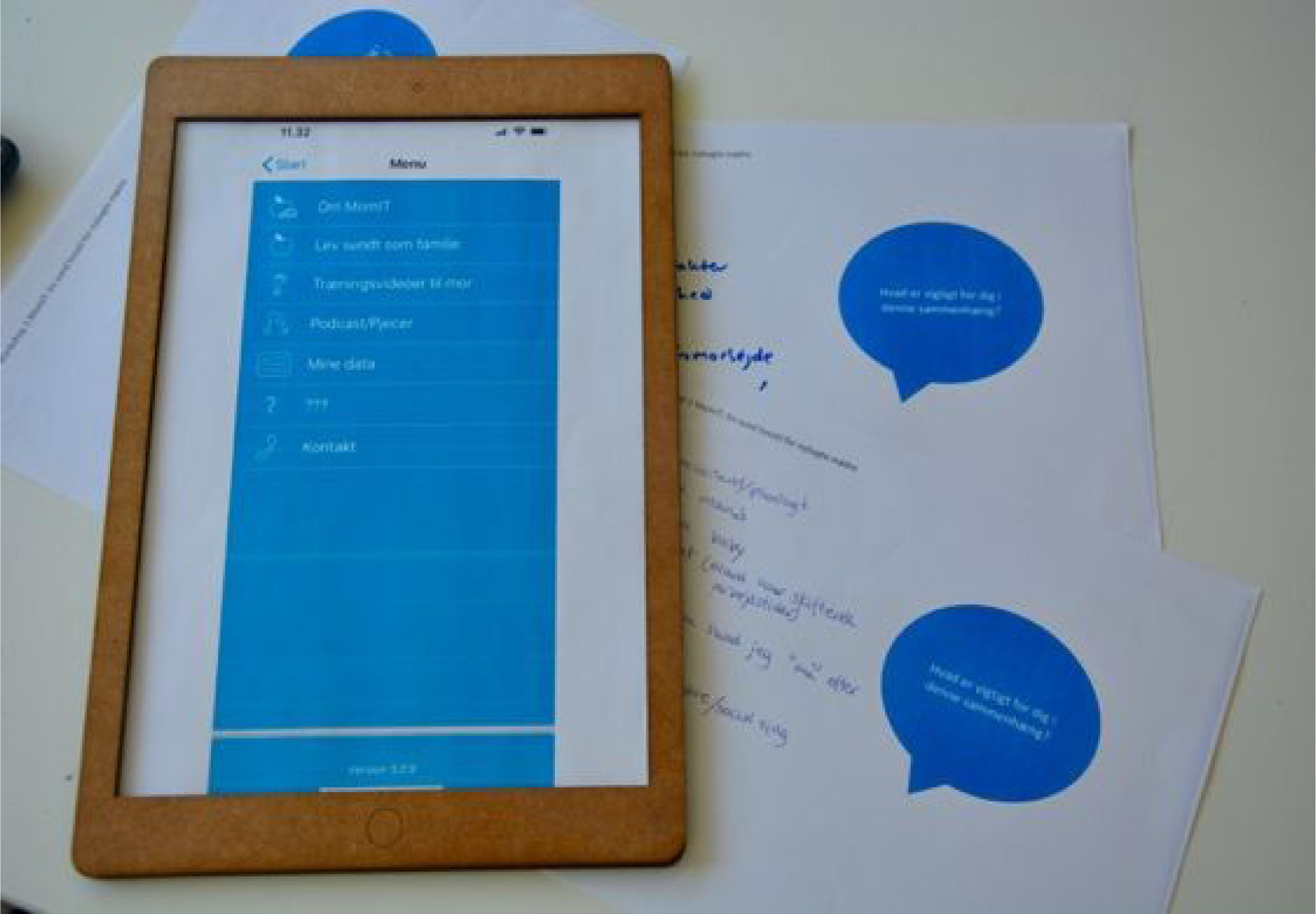
Feedback on the prototype content provided by workshop participants indicated that some users found a podcast too long, and some push notifications were deemed to require reformulation. Accordingly, adjustments were made. Finally, the app’s front end was tested on iOS and Android, and a think-aloud test was conducted with six women of childbearing age to test the app’s navigation. The think-a-loud test was carried out by providing the test persons with a phone on which they could log on to Healthy Together. They were given different tasks on how to navigate in the module, such as please log on the module and find the podcast about the postpartum body. They all passed this test without difficulty; thus, no further adjustments were made.
Discussion
Previous studies show that postpartum women often lack information about their bodies after birth, as well as guidance about new family life.8–10,27–29 To meet these needs, we co-created an app with users, HCPs, and IT experts to ensure that our solution reflected all participants’ relevant knowledge. 17 The resulting app contains podcasts, exercise videos, weekly push notifications, and weight tracking.
The development of the app using iterations and participants’ involvement were significant to this study since it enabled us to revise our solution until we had developed a suitable intervention. Mutual learning is crucial to the design and development process. 18 Early in our development process, HCPs recognized postpartum women’s insecurity regarding their bodies and lifestyle. HCPs distribute many related flyers at hospitals, but many postpartum women do not read them. 9 Our research revealed that no HCP had taken responsibility for focusing on maternal bodies and lifestyle after delivery. Participating postpartum women realized that the healthcare system regarded postpartum exercise and diet as mothers’ responsibility—and that mothers, therefore, needed to contact relevant HCPs for further examinations or advice.
The app’s push-notification content aimed to avoid information overload by presenting information regularly, in an effective order, and to encourage app use. Evidence has demonstrated that push notifications can positively affect app use. 30 The information provided by our intervention was tailored to themes determined through our mutual learning with workshop participants.
The mothers expressed a wish to register their weight development. Though, some women may already weight themselves, but do not achieve weight loss. It may not be because women are not aware of their weight, but by tracking their weight over a period, they can get an idea about the pace of weight loss. However, in a study on women diagnosed with gestational diabetes mellitus (GDM), only 7 out of 18 used weight tracking more than once. 31 Hence, it may not be all mothers who are in favor of weight tracking. It should be noticed, though that mothers with GDM belong to another target group.
The need for easy access to high quality information can be seen as a lack of information, but also a consequence of images of early retrained bodies portraited on social media. The images can have an impact on the mothers’ understanding of how and when to exercise and eat that contradicts the advice they would receive from an HCP. Thus, it is important that the women are provided with high quality information about postpartum exercise and diet.
To make the app user-friendly, content in the app was communicated through videos, podcasts, and push-notifications, rather than extensive text, making the application easy to use. To our best knowledge, the combination of podcasts, push-notifications, exercise videos and weight tracking has not yet been used in healthcare interventions targeting postpartum women. However, an intervention study that promotes weight loss in overweight and obese women with focus on the pregnancy period does include behavioral podcasts. 32
Trust in online information is not only an issue the women in this study encounter, but is an issue expressed by different patient groups.33,34 Thus, there is a lack of online, high-quality information available for different patient groups. Research shows that sources from hospital doctors have a high trust rate, and therefore there is potential to make information from trustworthy sources, such as HCPs, available online for the public. 35
Strengths and limitations
Participating postpartum women were often unable to confirm their participation in advance since their availability depended on how they and their babies felt on a given day. Participating HCPs’ agendas were also restrictive, and some HCPs had to cancel their participation due to unexpected work. New fathers did not participate in our workshops, nor did health visitors. However, this limitation was mitigated by including their voices after the study’s workshops through semi-structured interviews. Thus, our intervention supports both postpartum women and HCPs’ work.
No health data on postpartum women who participated in the workshops was gathered, which is a limitation. In the second workshop, only one group was formed, which can also be seen as a limitation. However, PD is iterative, and more feedback from workshop participants was given post workshop two in the feedback sessions. In addition, the solution is tested on a new group of postpartum women to get feedback on their experiences and attitudes of using Healthy Together.
Parents who participated in our study may not fully represent all new parents and their opinions. Despite this possible issue in this study’s representation of parents, we consider our app to benefit all postpartum women.
During the study’s workshops, two postpartum women had children who were over six months old; therefore, these women can be viewed as lead users at this stage.36,37 Postpartum lead users are valuable to the innovation process because they have, through their lived experience, familiarity with a postpartum lifestyle beyond most other postpartum women users. Thus, our study’s combination of lead users and new users was valuable for our mutual learning and development process, which can be seen as a strength.
Moreover, we consider the use of Hospital a strength. My Hospital is already widely used at hospitals in the Region of Southern Denmark and, consequently, most participating women were familiar with the app, having been introduced to it during pregnancy. 25 It is expected the intervention will be delivered by one of the HCPs at the end of the pregnancy. The HCPs can encourage and give instructions on how to use the intervention. To ensure that users could navigate the app, we also conducted a think-aloud test. However, to ensure that users could navigate the app, we also conducted a think-aloud test.
The content in the module may easily be transferred to other settings with a similar population, which can be seen as a strength. Screenshot of the module Healthy Together.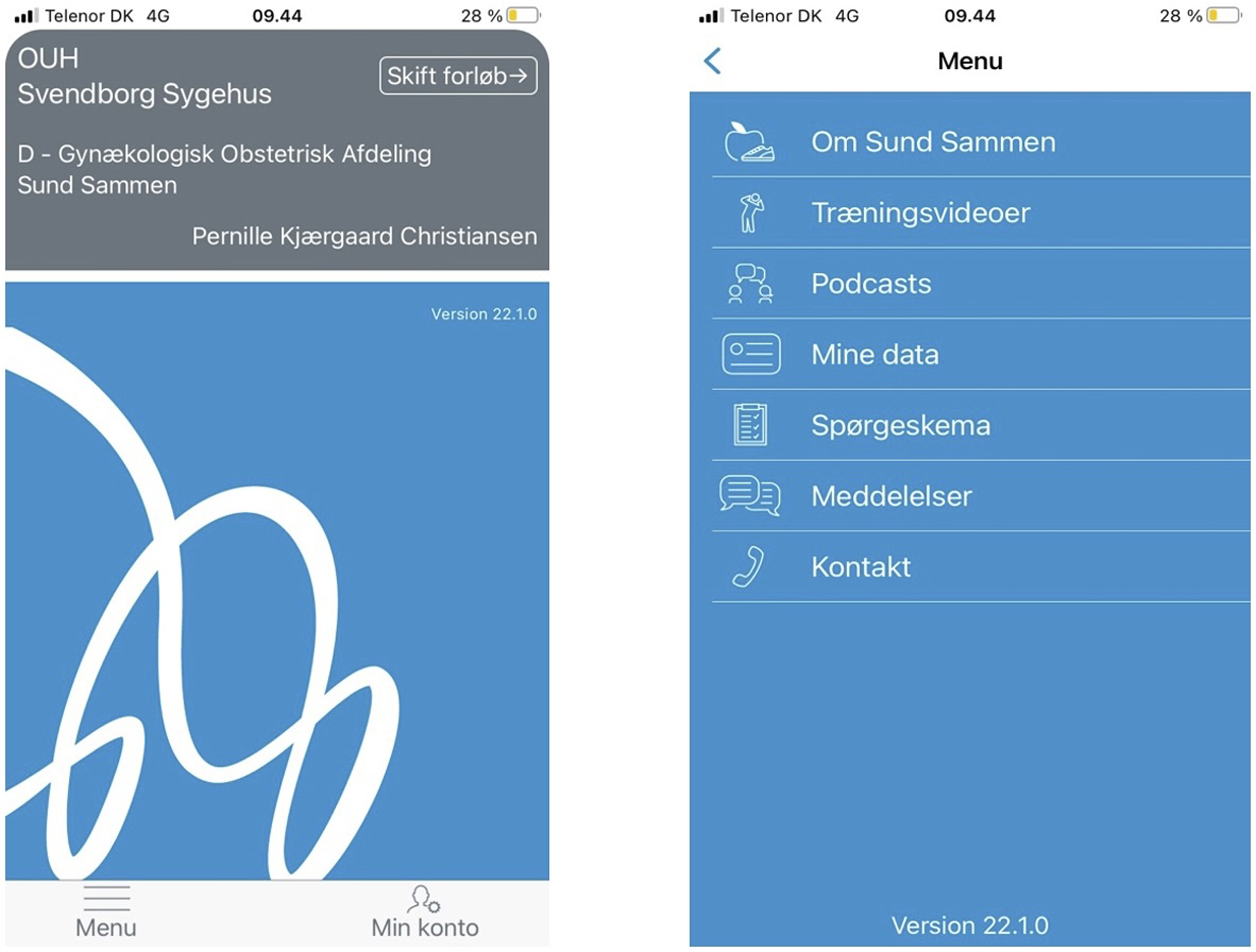
Conclusion
Using participatory design and the behavior change wheel, we successfully designed and developed an intervention that seeks to meet users’ needs and suggests behavioral change techniques. Our intervention was designed for Danish postpartum women, most of whom use smartphones daily and are familiar with app use.
By applying a participatory design and the behavior change wheel, we designed and developed the module through not only mutual learning and a democratic voice among postpartum parents, HCPs, IT consultants, and researchers but also behavioral change. The module contains podcasts, exercise videos, and weekly push notifications to encourage app use, as well as weight self-tracking. To our knowledge, this module constitutes a new approach that combines these various elements as an intervention supporting healthy-lifestyle behavioral changes among postpartum women. Further research is needed to assess whether this intervention works as we intend.
Although previous studies targeting postpartum women used apps with a combination of different tools, the app developed in this study differs from these by its combination of exercise videos, push notifications and podcasts.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.