
Abstract
This study aims to determine whether the British Heart Foundation PocketCPR training application can improve the depth and rate of chest compression and therefore be confidently recommended for bystander use. A total of 118 candidates were recruited into a randomised crossover manikin trial. Each candidate performed cardiopulmonary resuscitation for 2 min without instruction or performed chest compressions using the PocketCPR application. Candidates then performed a further 2 min of cardiopulmonary resuscitation within the opposite arm. The number of chest compressions performed improved when PocketCPR was used compared to chest compressions when it was not (44.28% vs 40.57%, p < 0.001). The number of chest compressions performed to the required depth was higher in the PocketCPR group (90.86 vs 66.26). The British Heart Foundation PocketCPR application improved the percentage of chest compressions that were performed to the required depth. Despite this, more work is required in order to develop a feedback device that can improve bystander cardiopulmonary resuscitation without creating delay.
Keywords
Introduction
The provision of effective bystander cardiopulmonary resuscitation (CPR) in out-of-hospital cardiac arrest (OOHCA) remains unacceptably low,1–5 despite evidence that suggests that effective bystander CPR is associated with more favourable clinical outcomes and improved survival rates. 6 It is recognised that CPR is frequently inadequate when performed by laypersons, 1,7 with many responders reluctant to perform mouth-to-mouth resuscitation during CPR. 8 To encourage uptake of bystander CPR attempts within the United Kingdom, the British Heart Foundation 8 launched a campaign to promote chest-compression-only CPR, with multiple studies supporting this approach.9–12 As part of their campaign, the British Heart Foundation produced a smartphone PocketCPR training application to provide real-time feedback on the depth of chest compressions performed during CPR and provide metronomic feedback to ensure accurate external chest compression rate. The importance of adequate chest compressions’ depth and accurate rate of compressions were both reaffirmed within current resuscitation guidelines, 13 with suboptimal compression rates associated with poor return of spontaneous circulation. 14 Nevertheless, the performance of both compression depth and compression rate by bystanders is shown to be suboptimal.15,16
To improve the performance of chest compressions, feedback systems have been used successfully in training to improve the overall quality of layperson CPR3,4,6,9,17 and maintain skill acquisition and retention,17,18 although there has been insufficient evidence to validate these applications for use in practice. This study endeavours to determine whether the British Heart Foundation PocketCPR feedback application would improve chest compression performance during bystander resuscitation.
Materials and methods
Objectives
The aim of this randomised crossover manikin study was to investigate whether using the British Heart Foundation PocketCPR training application would improve the performance of chest compressions against current resuscitation guidelines when used by laypersons with no recent CPR training.
We hypothesised that the British Heart Foundation PocketCPR training application would increase the proportion of chest compressions performed at the recommended depth of 50–60 mm and improve the rate of chest compressions per minute, compared to no application.
Participants and randomisation
Participants were recruited from a university campus on an opportunistic basis. All participants were required to be aged 18 years or over, not be a healthcare professional and not having attended a CPR training course in the last 6 months. This last point was pertinent, since it is acknowledged in the literature that skills and knowledge relating to bystander CPR decay rapidly after initial training.19–21
Volunteers were provided with a participant information sheet and an opportunity to ask questions of the researchers before being asked to give written consent.
Methodology
In this randomised crossover study, each participant was asked to attempt a 2-min period of CPR on a Laerdal Resuscitation manikin (Resusci Anne Skills Station, Laerdal Medical Limited, Orpington, UK) with and without the PocketCPR application in accordance with a pre-randomised order. Candidates were not required to have previous experience or ownership of a smartphone device to take part and were provided with information as to how to hold the iPod and activate the PocketCPR software. Randomising the participants reduced the risk that the participant may perform better in the second arm of the study where they had previously used PocketCPR. The randomisation order was generated using the statistical software package PASW (version 17.0.2; SPSS Inc, Chicago, IL, USA) and ensured that 50 per cent of the participants performed first with the PocketCPR application and 50 per cent without. The PocketCPR application was used on an iPod Touch 2009 device.
Participants were required to rest for 2 min between each CPR scenario to ensure that operator fatigue did not adversely affect the second attempt. The instructions given to participants were limited to information on how to hold the iPod and how to activate the British Heart Foundation PocketCPR software.
The software gives visual feedback in the form of a bar on the display indicating current compression depth with a green colour marking the ideal interval and verbal feedback prompts (including ‘press harder’, ‘press faster’, ‘press slower’ and ‘good depth’) (Figure 1). Additionally, the device has an integrated metronome which ticks at a rate of 100/min, signalling the correct compression rate. There was no feedback on ventilations since this application is designed to support chest-compression-only CPR. When performing CPR without the device, the participant received no verbal or visual feedback and no metronome guidance.
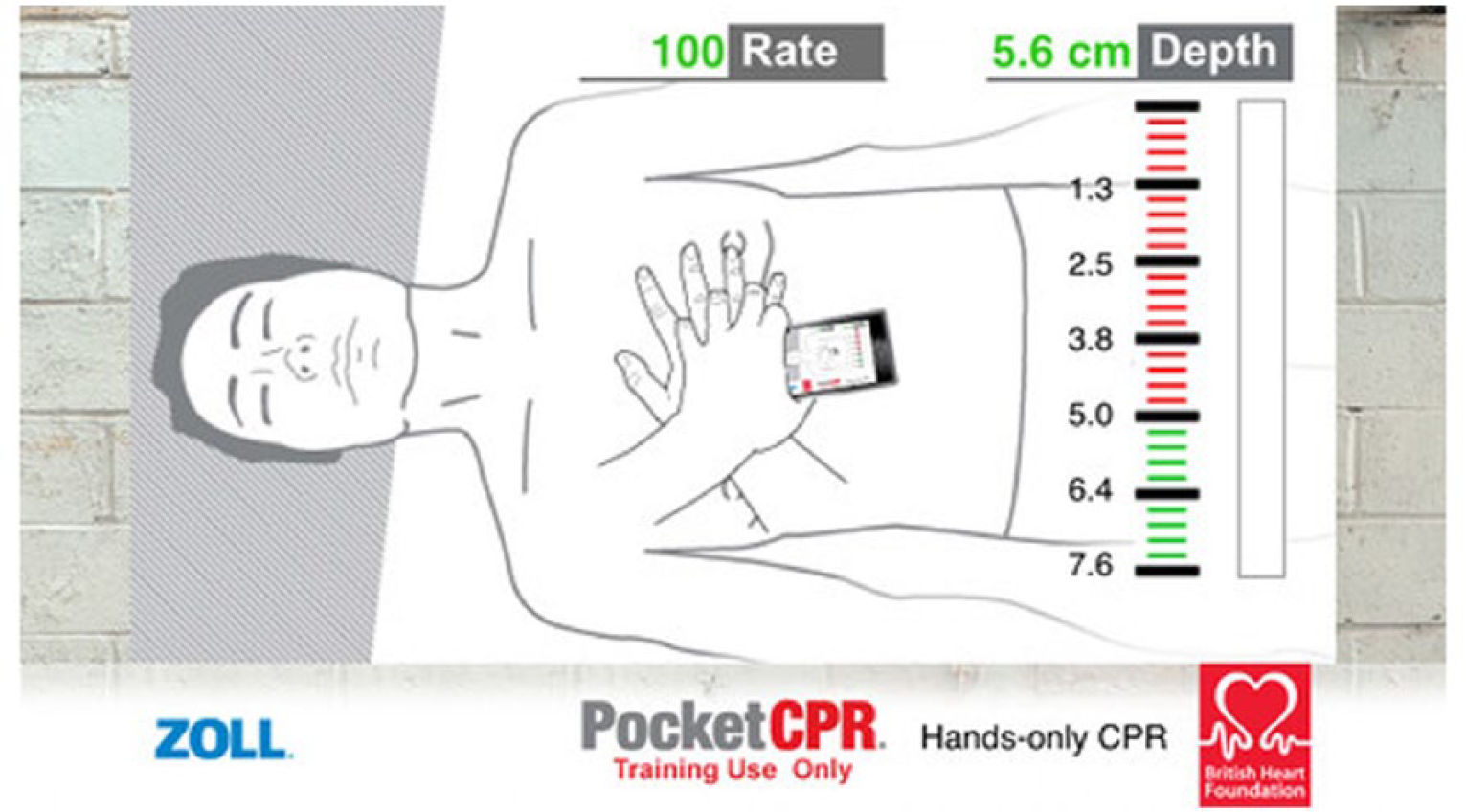
Screen print of PocketCPR feedback screen.
Data collection
Performance measurements derived from the manikin software were recorded onto a connected laptop. These were compression rate, compression depth, hand position for performing chest compressions, tidal volume of ventilation attempt and time off the chest once CPR had been started. Additional observations (including time to start CPR) were recorded manually by the researchers. Manual observations included any ventilation attempt and rate which did not register in the manikin due to an occluded airway.
Statistical analysis
Sample size was calculated based on the primary outcome measure of the adequate depth of compression. Previous research has reported that 42 per cent of trained prehospital providers delivered chest compressions with a mean depth of 50–60 mm during 1-min simulated cardiac arrest scenario, compared with 39 per cent listening to a musical prompt (correlation coefficient (phi) = 0.44051). 22 In order to detect 15 per cent (from 42% to 57%) increase in the proportion of laypersons delivering compressions at the recommended depth with a power of 0.85 and an alpha of 0.05, it was estimated that 108 subjects were required (sample size for paired cohort study calculated using StatsDirect, version 2.7.8; StatsDirectLtd, Altrincham, UK).
Analysis compared the difference in performance of chest compressions with and without the British Heart Association PocketCPR application. The primary outcome measure of mean compression depth was analysed alongside secondary outcome measures of mean total compressions in 2 min of simulated CPR, mean compression rate, mean total correct compressions and correct hand position.
The quality of chest compressions was measured with Resusci Anne Skills Station (Laerdal Medical Limited, Orpington, UK). IBM SPSS Statistics version 22 software package was used to calculate descriptive statistics, p values, 95 per cent confidence intervals (CIs) and Wilcoxon’s rank-sum tests for two related samples. A significance level of p < 0.05 was considered to be statistically significant.
Ethical considerations
This randomised control trial received ethical approval from the Coventry University Ethics Committee (P4090).
Results
Flow and baseline characteristics
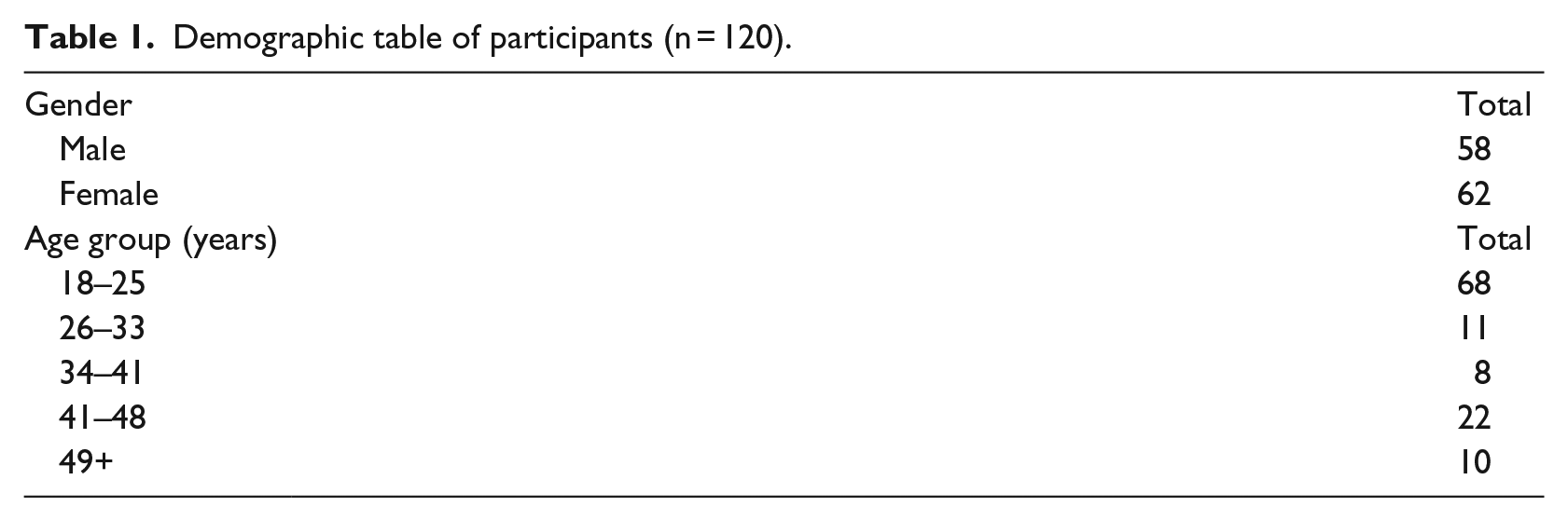
A total of 118 subjects were recruited to the study and were included in the analysis. The sample size of 108 subjects determined by the power sample size calculation was satisfied. Baseline characteristics are shown in Table 1.
Demographic table of participants (n = 120).
Primary outcome
When using the PocketCPR application, 44.28 per cent of the total number of compressions were measured to be the correct depth compared with 40.57 per cent of mean total compressions when the PocketCPR application was not used (p < 0.001). The actual number of correct depth compressions was also higher in the PocketCPR group than would be anticipated by the percentages (90.86 vs 66.24), as this group performed more compressions in the 2-min period.
Secondary outcomes
Further analysis was performed on the secondary outcome measures, and the results are reported in Table 2.
Results.
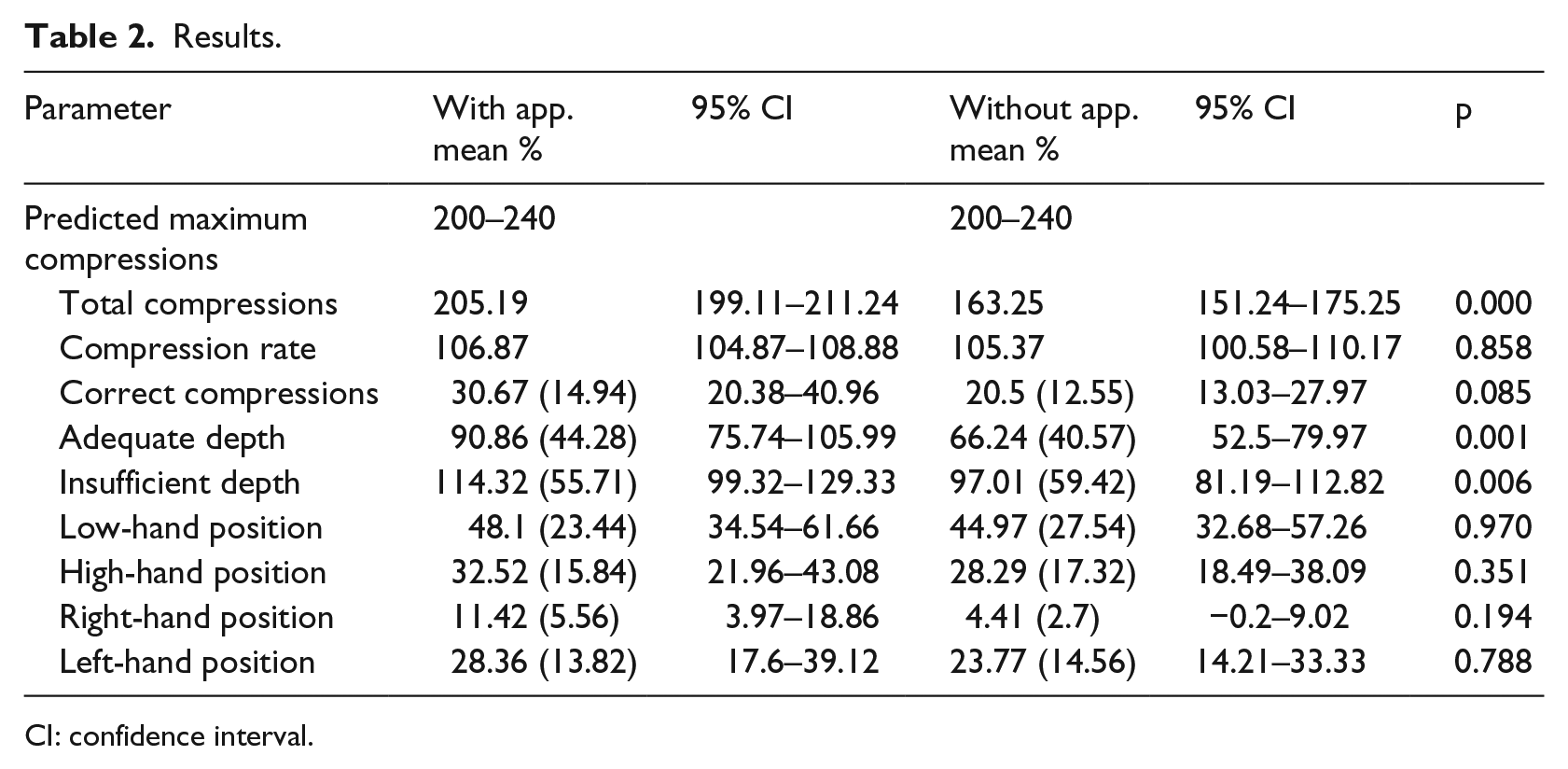
CI: confidence interval.
The 2010 Resuscitation Council (UK) Guidelines 13 advocate a compression rate of 100–120 compressions per minute; therefore, continuous chest compressions over a 2-min period should result in 200–240 compressions being delivered over the 2-min period. While the mean compression rate when using the PocketCPR was broadly similar to the mean compression rate when not using the application, there was a significant difference in the total number of compressions performed. When using the PocketCPR application, the number of compressions delivered fell within the expected range, while the number in the non-PocketCPR group was lower (p < 0.000).
There was no significant difference between mean compression rates, but there was a significant difference between the number of compressions performed during the 2-min time period.
The difference in the mean number of correct compressions when using PocketCPR and without the application was not significant, and the mean number of correct compressions was low in both groups. A total of 14.94 per cent of the mean total compressions (95% CI 20.38–40.96) were correct in terms of rate, depth and hand position when using the application, 12.55 per cent of the mean total compressions (95% CI 13.03–27.97) without the application.
Where compressions were incorrect due to incorrect hand placement, hands were more likely to be too low rather than too high. Where hands were placed away from the midline, subjects were most likely to place their hands further from their body to the left of the midline of the manikin, rather than closer to them to the right of the midline of the manikin.
Discussion
Comment
The PocketCPR training application allowed for a greater depth of compressions during the 2-min resuscitation attempt, which supports the recommendations for CPR in current guidelines. 13 Participants were more likely to reach the recommended resuscitation guidance depth of 50–60 mm for chest compressions when using the PocketCPR application (95% CI 81.19–112.82, p < 0.006). With evidence connecting an increased likelihood of return of spontaneous circulation with chest compressions performed to a depth of 50 mm or more,23,24 the results here suggest that the feedback provided by the PocketCPR application could have real-life applications. Previous manikin-based studies have found that compressions tend towards inadequate depth following only 1 min of CPR due to rescuer fatigue, 25 whereas our results demonstrate that feedback to the layperson allowed chest compressions to be performed to an adequate depth more frequently during a 2-min cycle. This suggests that the PocketCPR application may either ameliorate the effect of rescuer fatigue or help to motivate the rescuer to continue to compress the chest to an adequate depth even when fatigue or a loss of concentration is taking effect.
While the depth of chest compressions improved with the PocketCPR application, it was observed that hand position was frequently reported off-centre (Table 2). This study found that incorrect hand position was often too high on the chest, rather than too low or too far left or right. As a percentage, there was no difference in hand positioning between participants using the PocketCPR device or those without. The use of PocketCPR likely required more dexterity to hold the device between the hands during chest compressions as well as the requirement to visualise the screen to view depth attainment, although our results failed to reach significance. There is insufficient evidence in research to determine if there is any relationship between incorrect hand position and changes in efficiency of CPR. 25 It may also be considered that CPR performed too right or too left is more likely to be effective than chest compressions performed too high and too low due to changes in thoracic pressure as part of the thoracic pump theory. 26
Despite the high number of incorrect hand positions in both groups, use of PocketCPR did result in a greater number of chest compressions that were performed during the 2-min resuscitation attempt. When using the PocketCPR application, participants achieved the predicted range of 200–240 chest compressions, over the 2-min test period, in accordance with resuscitation guidance of 100–120 chest compressions per minute. Although the number of chest compressions performed using PocketCPR was higher than without, there was a noticeable delay in starting chest compressions while participants navigated the British Heart Foundation PocketCPR training application. While any lack of familiarity with the device was ameliorated by the instructions that were given to the participants, on average, chest compressions were delayed by 37.31 s while candidate’s summoned help, confirmed that the patient was not breathing and began chest compressions with device feedback. The delay to begin chest compression is consistent with comparable studies and similar portable feedback devices. 25 Delay to CPR without the device was on average 14.42 s. The PocketCPR device appears to improve the consistency of chest compressions, as participants still performed a greater number of chest compressions in the required time, albeit with an initial delay. It is unclear whether the delay to start initial chest compressions is countered by the increased number of compressions achieved over 2 min, but the delay in starting could be further exacerbated where the application is not readily available on the home screen of an individual about to perform bystander CPR. A recommendation would be to ensure that the application is pinned to a person’s home page on their mobile device in order to minimise any delays in starting chest compressions. To overcome this delay in beginning chest compressions, it is recommended that instruction is more concise, bypassing the approach and navigating straight to resuscitation feedback. Without the application, CPR was often commenced earlier but had lower consistency and longer periods of inactivity due to some participants attempting mouth-to-mouth ventilation. Since bystander resuscitation with periods of inactivity is associated with poorer outcome, 27 it is important to minimise this inactivity. In our study, those performing chest-compression-only CPR using the PocketCPR application had fewer periods of inactivity and more consistency in their compressions. The periods of inactivity serve to explain why the number of compressions in the PocketCPR arm of the study performed significantly more compressions during the 2 min of the study; yet, there was no significant difference in the actual rate of compressions between the two limbs.
During both limbs of the study subjects managed to achieve an average rate of compression that accords with current resuscitation guidelines, which suggest that chest compressions of at least 100 compressions per minute are more effective than slower rates. 28
Participant recruitment was representative of a normal urban population. Since OOHCA can occur in any environment, the participant demographics are representative of those who may render aid in this situation. During the study, it was noted that most participants were familiar with the device and navigation through the application but were more often unable to effectively follow the instructions as directed. Although we collected information on age, there are many factors that affect the rescuers’ ability or willingness to perform bystander CPR. These include (but are not limited to) socioeconomic profile, education, 29 gender and fitness. 30
Participants in this study were seen to encounter navigation problems while the application was playing due to the touchscreen nature of the device. This resulted in accidental disruption of CPR instruction and restarting the application, which adversely impacted upon the time to perform chest compressions. It would be helpful if the device became locked once the application had been selected and the accelerometers activated by chest compressions. Despite this, the benefit of using the PocketCPR application is that participants only required a smartphone device with the application, rather than additional equipment to secure the device. While other studies have shown improved CPR with the use of smartphones secured in armbands, other studies demonstrate that participants were unable to perform CPR with feedback without the securing mount. 31 While the PocketCPR uses smartphone technology to feedback depth measurement, gripping the device while performing chest compressions is difficult, and the usability is compromised due to the accidental disruption of CPR instruction.
There is a growing body of evidence to suggest that using a smartphone application can improve chest compression depth and rate, 32 which positively affects chance of survival in OOHCA. However, these devices are limited in their usability and complex interfaces, which must be overcome to confidently recommend their use beyond a training application into a real-time feedback device. Smartphone applications may also be useful as prerequiste learning for CPR training. 33
Although this study considers PocketCPR application to improve chest compression performance, the evolution of portable smart technology is becoming ever more prevalent in prehospital resuscitation, evident by the recent endorsement of the Good Smartphone Activated Medics (GoodSAM) application from the Resuscitation Council UK, 34 which alerts nearby rescuers to cases of OOHCA. Therefore, there is opportunity to develop applications like PocketCPR to combine rescuer activation with effective CPR feedback until professional help arrives.
Limitations
There were several limitations within this study. First, over-compression of chest compressions was not measurable on the resuscitation manikin, as the physical design of the manikin prevented the participant from over-compressing. Data were collected to consider whether compression depth was insufficient, but it is not known how many compressions may have been too deep. Despite this, there is insufficient evidence to specify an upper limit for chest compression depth, and chest compressions that are too deep may still be effective. 35
Second, the number of people who have PocketCPR application downloaded onto their portable device or smartphone and accessible during OOHCA incidents may limit the usability of feedback. It is not known how many times the application has been downloaded, but it works on both an Apple and Android platforms, so there is considerable potential for this application be widely available. In the first quarter of 2015 alone, over 74 million iPhones were sold as a stand-alone mobile product. 36 It is not unreasonable to argue that the application should be included as a default application on all devices capable of supporting it.
Finally, as with all simulation and manikin studies, the results of this study cannot measure clinical outcome or survivability but remains a useful proxy measure into the usability of feedback devices for bystanders.
Conclusion
Overall, the standard of bystander resuscitation within this study was poor and chest compressions were still frequently performed at insufficient depth, with incorrect hand positioning and with prolonged periods of inactivity. The PocketCPR application improved the percentage of chest compressions that were performed to the correct depth during bystander compression-only CPR. A greater number of chest compressions were also performed with the application during the 2-min time period when compared to standard basic life support attempts, where compressions were often too shallow and with too few external chest compressions performed. Although use of the application improved CPR performance when compared to no application, CPR performance remained suboptimal. More work is needed to develop an application that can instruct bystanders to perform effective chest-compression-only CPR without delay.
Footnotes
Acknowledgements
The authors would like to thank Malcolm Woollard for his support in the early stages of this study as well as Coventry University for their facilitation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.