
Abstract
Given the increasingly widespread use of mobile phones in the developing world, the application of this technology for healthcare (also referred to as m-health) has tremendous potential. However, there is a need for more research on factors that influence the sustainable and scalable adoption of m-health in developing countries. To fill this gap, in this study, drawing on the theory of diffusion of innovation, we conducted in-depth interviews with 29 health professionals in Sri Lanka to understand their views on the benefits and barriers to adopting m-health. Participants had mixed views on the adoption of this technology. Reasons for m-health adoption included efficiency and usefulness in emergency situations. Barriers to adoption included risks for miscommunication/misinterpretation and lack of systems/policies for implementing m-health technology. With regard to the innovation-decision process, most participants appear to be in the stages of “persuasion” and “decision”; with regard to degree of innovativeness, interviewees comprise a mix of “early adopters” and “laggards.” Assuming mobile health apps afford improvements in health outcomes for developing countries, contextual factors in each national setting should inform design and implementation of m-health interventions.
Introduction
Mobile health or mHealth (or m-health) can be defined as the use of “wireless communication devices to support public health and clinical practice.” 1 There are now a greater number of cell phone users than landline phone users across the globe, and more than three-fourths of the world has access to a mobile phone. 2 The advantages of mobile technology include wireless communication, portability, and computing power (see Figure 1). 3 This translates into tremendous potential for this technology in healthcare. Indeed, studies have already demonstrated the wide range of applications of mobile technology in fields such as home health monitoring, medical records management and communication, and public medical education.4–7
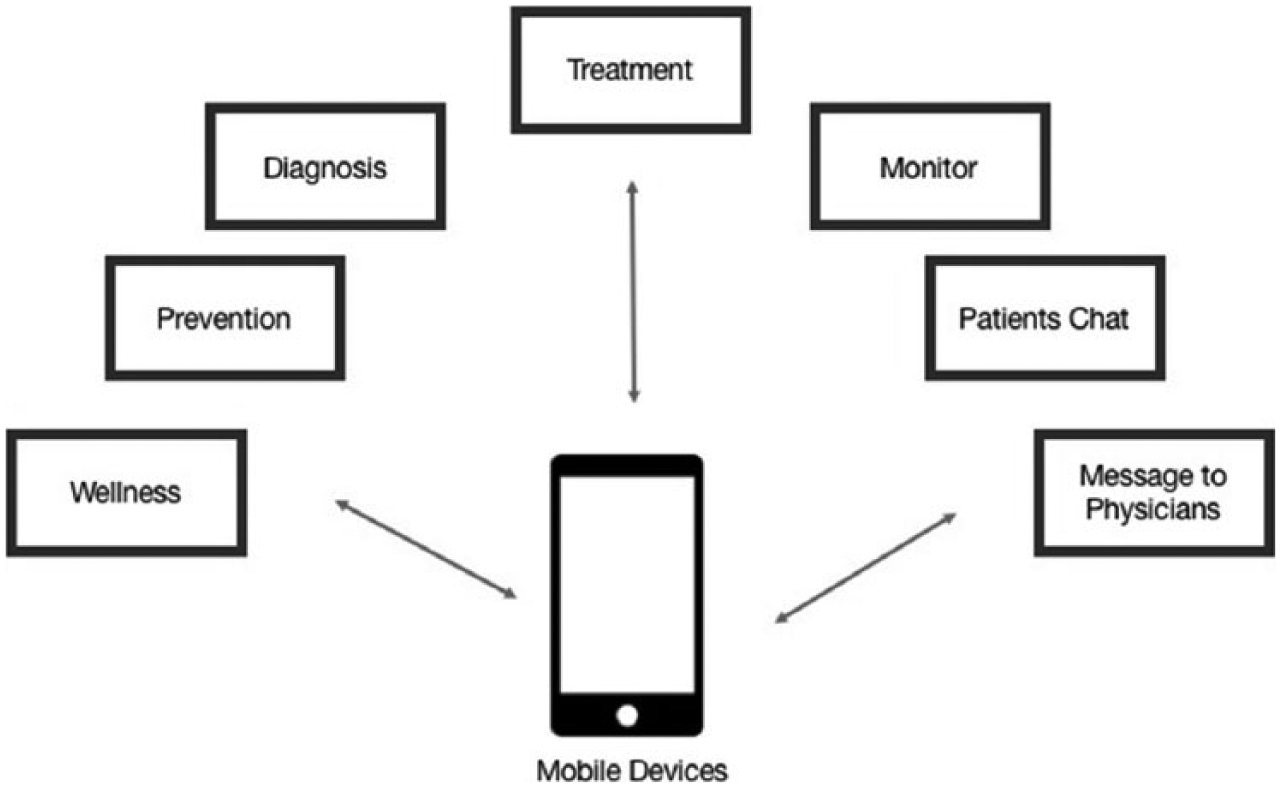
Mobile health applications (m-health).
The application of mobile technology for health is particularly important in the developing world for the management of chronic disease, a major cause of morbidity and mortality. 2 Mobile technology has the potential to improve healthcare in developing countries “by removing physical barriers to care and service delivery and by improving weak health system management, unreliable supply systems, and poor communication (p. 255).” 1 For example, in low- and middle-income countries, m-health has demonstrated positive results in patients with chronic disease such as increasing appointment attendance rates through SMS and mobile phone appointment reminders and improving quality of life through regular disease counseling. However, whether m-health can be adopted in a sustainable and scalable manner in the developing world needs more investigation; in particular, it is important to understand factors that can impact m-health use such as healthcare context, social values, and culture, which differ from one country to another. 2
In this study, we applied Rogers’ diffusion of innovation to understand the factors that influence the adoption of m-health in a particular developing country—Sri Lanka. Diffusion of innovation 8 for m-health pertains to innovation at the community or country level as a consequence of both a user demand-pull and a technology-push approach to get advantages from technological developments without failing to win favor from target groups. 9
According to the theory, the process of adoption of a new technology, called the innovation-decision process, involves five stages: knowledge, persuasion, decision, implementation, and confirmation.8,10 In the knowledge stage, individuals become aware of an innovation and begin to learn and seek out information about it. In the persuasion stage, individuals begin to form an attitude (positive or negative) about the innovation. Individuals then decide to either reject or adopt the innovation in the decision stage. At the implementation stage, the innovation is tested or tried out, and finally, in the confirmation stage, individuals seek out messages that back up or confirm their decision to adopt or reject the innovation.
The rate of spread of an innovation is influenced by three clusters of factors: 11 (1) the perceptions/properties of the innovation, that is, whether the innovation is perceived as beneficial (or as having a relative advantage over the currently used technology); compatible with the values, beliefs, past history, and current needs of the users; simple; testable; and observable; (2) the types of adopters such as innovators, early adopters, early majority, late majority, and laggards; and (3) contextual factors, that is, characteristics of the social system in which the diffusion of innovation takes place.
Drawing on the factors outlined above, this study aims to understand how health professionals in Sri Lanka view the benefits and barriers to adopting mobile technology on a large scale in a sustainable manner. We chose Sri Lanka as the focus of this study as it is a lower-middle-income country 12 faced with the challenge of providing accessible, specialized care to patients in rural areas. 13 This is a challenge that has the potential to be tackled through m-health technology as about 25.9 million people in Sri Lanka subscribe to cellular mobile phone services, 14 and there are a significant number of mobile subscribers in rural areas 14 although there might be limited cell phone service. Also, only 0.1 percent of Sri Lanka’s budget is allocated to health, 15 and the country has a severe shortage of qualified health professionals. 16 Given these challenges, it is worthwhile for the country to invest in innovative health systems such as m-health technology, 16 provided the technology and content appeal to individual end users.
The few studies on the application of mobile technology in healthcare in Sri Lanka have focused on the technological aspects of m-health projects. For example, how mobile phones can be used for the early detection of infectious disease outbreaks by digitizing and transmitting patient data to health officials has been studied in Sri Lanka and India.17,18 Arguably, it is also important to understand how those who may be involved in providing m-health interventions perceive this new technology. To address this gap, in this study, we conducted qualitative in-depth interviews with health professionals in the public and private sector hospitals in Sri Lanka. Specific research questions were about how the characteristics of m-health are viewed (e.g. its risks/benefits) and whether contextual factors, such as healthcare infrastructure, support the adoption of this technology.
Materials and methods
The first author conducted in-depth interviews with healthcare providers working in public or private hospitals. Recruitment and interview procedures were approved by the University Institutional Review Board Committee on Human Subjects. Participants were recruited by convenience and snowball sampling.
Participants
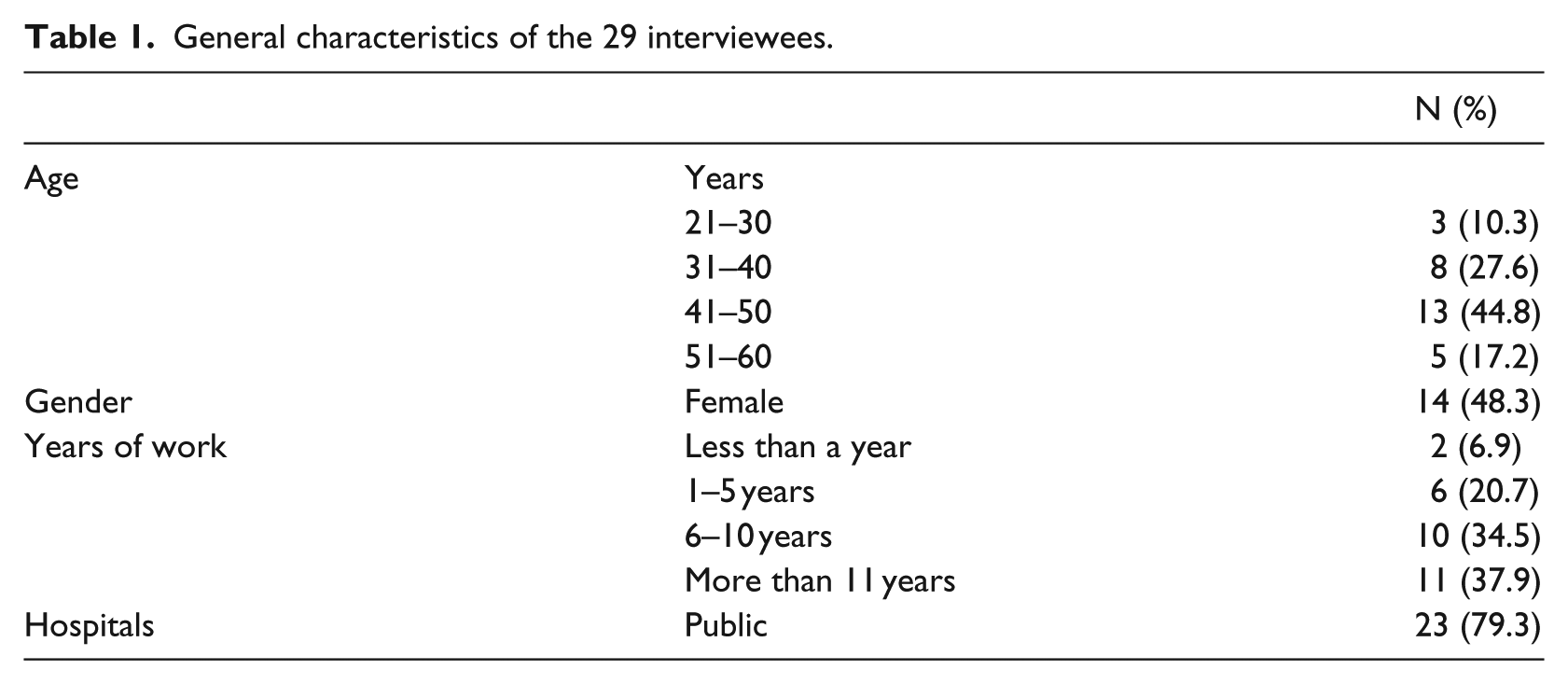
The 14 women and 15 men who participated in the interviews were all healthcare providers born in Sri Lanka. Participants ranged in age from 27 to 56 years (mean age = 41 years). Female interviewees were 14 (48.3%). Participants had worked in their field as a physician or a health administrator for an average of 9 years (range, 1–29), and of the 29 participants, 6 were working in private hospitals. Among them, 23 interviewees were from public hospitals and 11 interviewees were working at public hospitals in the capital city, Colombo (Ayurvedic Teaching hospital, Durdan hospital, Golden Key Eye & Ent Hospital, etc.; see Table 1).
General characteristics of the 29 interviewees.
Interviews and analysis
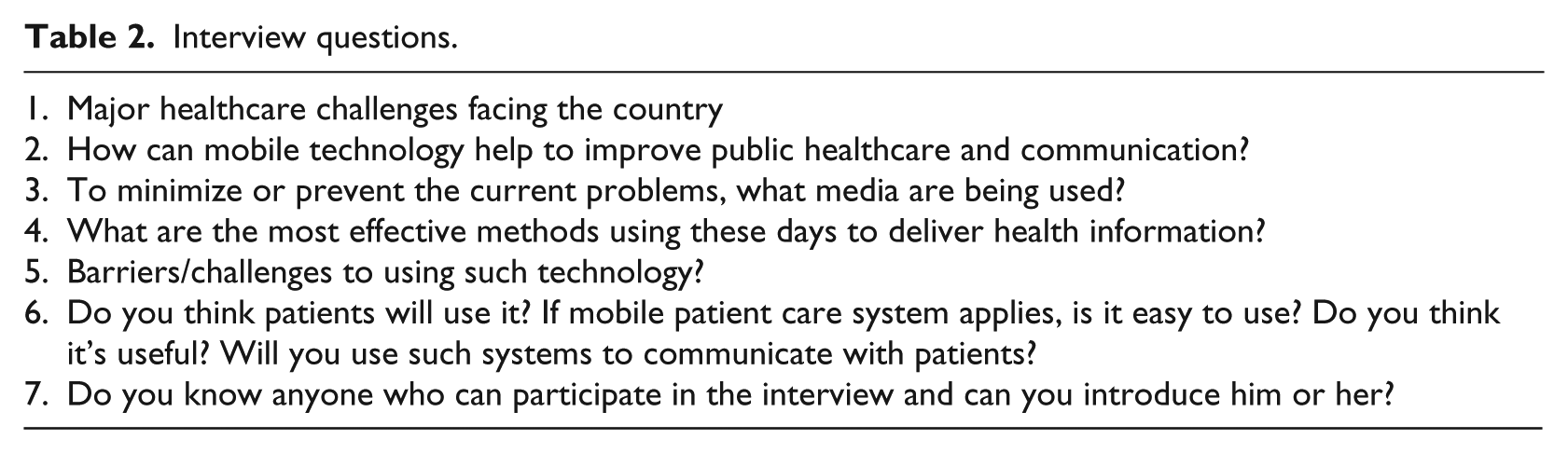
Semi-structured interviews were conducted at participants’ workplace and lasted about 40 min. Interviews were conducted one-on-one or in groups of one to three people. Topics included the healthcare challenges facing the country and the risks/benefits of m-health technology (see interview questions in Table 2). All interviews were recorded and transcribed. To control quality of this research for the credibility of naturalistic work, 19 two trained researchers, individually, analyzed the data and compared and contrasted the analysis results together. Data collection was continued till new interviews yielded very little or no new information. Researchers coded the transcripts independently using a constant comparative approach. 20
Interview questions.
Results
The interviews revealed a mix of advantages and disadvantages of m-health. Some respondents could be characterized as “early adopters”—they were enthusiastic about m-health and believed in its potential. Others acknowledged the benefits of m-health but did not believe in the large-scale adoption of this technology for various reasons. The following themes were identified in the interviews.
Reasons for adopting m-health technology
Respondents discussed the advantages of m-health. The main motivations for adopting m-health were its potential to improve doctor–patient communication and efficiency, particularly in emergency situations.
Better service
Respondents discussed how m-health makes it possible for patients to access their healthcare providers even outside the hospital. In doing so, it improves the doctor–patient relationship, which in turn can improve the service patients receive:
Doctors and patients can communicate easily through mobile technology. It may be better than face-to-face communication. Sometimes patients feel uncomfortable to tell what they really think in front of doctors. (Participant 28)
Efficiency
Respondents discussed how m-health can save time. Patients in remote areas do not have to commute to hospitals and can instead communicate with health professionals through mobile technology. Also, the technology enables health professionals to constantly monitor patients’ health status and to manage patient appointments. Given their ubiquity and ease of use, respondents expressed frustration that mobile phones for m-health were not being fully exploited. The quote below illustrates this point:
In Sri Lanka, now, telephone usage is more than 95%. It’s sad that we’re not using that to provide more health care. We don’t have enough qualified persons and staff to provide these services. I know that most mental [health] officers only have time after hours because they are working until then. Then they have time to call after working hours. (Participant 14)
Barriers to accepting m-health technology
Although interviewees acknowledged the advantages of m-health, they also pointed out several drawbacks of this technology. Barriers to adopting m-health were as follows: indirectness of communication, poverty (and associated illiteracy and infrastructure problems), and inequality/gap between private and public sectors.
Indirectness of communication
The theme of the importance of direct communication came up several times (e.g. in interviews with Participants 1 and 2). Although respondents believed that mobile phones were convenient and efficient and could be useful in emergency situations and for communicating basic health information, they did not believe it could be useful for long-term care and that it was risky and unethical to communicate health information over the phone as there could be misunderstandings and potential for legal action. They believed that for effectively treating patients, face-to-face doctor–patient communication was critical. The quotes below illustrate these points:
Face-to-face is the best way. When we talk to the patients, we can see whether the patient understood or not. We can ask them if they understood and also see their facial expressions. But over the phone, we tell them something and we think the patient got the information correctly but they have the wrong information. So if the patient doesn’t get the information properly, in person, we can write and draw and give the instructions to them. … Sometimes we think it’s [mobile technology] convenient, but shortcuts in medicine [are] not good. We have to have face-to-face, doctor-to-patient communication. That is more important than more modern ways of communicating. (Participant 12) We can’t depend on mobile phones. We can incorporate mobile phones to our practice to communicate with patients certainly, but not 100%. I cannot say mobile phones are not effective at all. Mobile phones are important in managing the patient for emergencies so we can tell the patient what to do. We can tell them a certain amount of instructions only but not for long-term management. … We clinically need to see the patient to assess them and assign drugs. Mobile phones are not good for treatment. (Participant 12)
Some respondents (Participants 5 and 6) also believed that mobile phones were for personal use, especially among older adults, and were not an appropriate medium for delivering health information. Instead, media like “posters,” “leaflets,” and “documentaries” should be used to educate people about health.
Poverty
Several respondents talked about how m-health was not feasible in a developing country like Sri Lanka because of infrastructure problems in rural areas and because of literacy problems—most people would not know how to use the technology. In fact, one respondent (Participant 3) talked about how the poor may not even have access to television let alone a mobile phone and so health education had to be delivered through community medical officers. Another respondent (Participant 4) pointed out that even if the poor had access to mobile phones, the phones were not Internet-enabled. Finally, respondents believed in traditional means of health education such as oral communication, health campaigns, and health booklets or through traditional media such as newspapers, television, and radio (Participants 1, 2, 5, and 6).
Gap between public and private sectors
In several interviews, the divide between the private and public health sectors came up. Respondents felt that although mobile technology could be efficiently and cost-effectively used in the private sector, it was unlikely that mobile technology would be adopted in the public/government sector because of large patient loads and the lack of infrastructure (e.g. no system to support phone-in appointments). Also, a respondent suggested that mobile technology was not compatible with the public healthcare system’s goal of free healthcare as those who could not afford mobile phones would not be able to access the system. The quotes below illustrate these points:
In the government sector, unlike the private sector, the number of patients is huge because our government system is a free healthcare system. Our systems are free. And because of that, the number of patients that needs to be handled is huge. So you cannot call and come. Also, in the government sector, the access should be open to anyone. Anyone should be able to come in and get the treatment as necessary. Any person should have access, but in the private sector, everyone does not have access. Making calls—you have to pay for those things. In Sri Lanka, I don’t think it [m-health] will be implemented in the near future. (Participant 11) I think around 70% of people go to the government sector. The government sectors are free. There are free consultations and free medicines. … For these things in the private sector, the price is very high … Middle class or high class can pay this but poor people cannot. Their income is not enough for the insurance policy. (Participant 18)
Discussion
Drawing on the theory of diffusion of innovation, we aimed to understand the factors influencing the adoption of m-health by healthcare professionals in Sri Lanka. Interviewees acknowledged the advantages of m-health such as efficiency and better healthcare service. These findings are similar to those of previous studies on adoption of m-health technology. 21 Also, as found in previous research, participants discussed drawbacks of m-health such as potential for miscommunication with patients; lack of direct human interaction with patients; lack of infrastructure, such as Internet-enabled mobile phones22,23 to support m-health services; and poor integration of the private and public healthcare sectors. 24
With regard to the innovation-decision process (knowledge, persuasion, decision, implementation, and confirmation), 8 most participants appear to be in between the persuasion and decision stages as they recognize the advantages of m-health but are not ready to adopt it yet. In terms of adopter segmentation, 11 respondents appear to be made up of a mix of “early adopters,” that is, individuals who are quick to embrace a new technology as they are open to experimenting with new ideas, and “laggards,” that is, individuals who are conservative and prefer to stick to tried and tested methods.
According to the diffusion of innovation model, if the early majority (i.e. individuals who adopt an innovation only if they perceive it to be immediately relevant to their needs) is able to interact with innovators and adopters, they too will embrace the innovation, and they will be followed by the late majority. Whether the health professionals in our sample who are cautious about using m-health might change their views if they are exposed to innovators and early adopters is a question worthy of future investigation. Furthermore, giving health professionals the resources to use m-health on a trial basis could help reduce uncertainty about this technology. 25
Although our findings are not based on a random sample of participants, and therefore, may not represent the views of health professionals in Sri Lanka in general, the study has noteworthy contributions. Most studies on m-health focus on the developed world. 3 Through in-depth interviews with health professionals in Sri Lanka, this study contributes to the limited literature on m-health in developing countries. The findings from this research shed a light about the potential of m-health to revolutionize healthcare in developing countries; however, this study shows that resistance to new technology, for example, lack of perceived compatibility with individuals’ values or lack of perceived benefits, and infrastructure problems may pose significant barriers to the adoption of m-health. 26 Therefore, instead of assuming that m-health is useful and needs to be immediately introduced, it is crucial to first evaluate at what stage of the innovation-decision process the target audience is at and design interventions accordingly.
This study evaluates the impact of telemedicine using mobile technology, as listening to both supporters and opponents’ opinion based on health professionals’ experiences. Because there are no specific items for telemedicine evaluation, discussion for this issue is not easy. 27 However, as this study conducted in-depth interviews, we could collect possible reasons for adoption or rejection of m-health.
Second, this study considered both patients and doctors’ status quo on m-health. In other words, interviewees mentioned both m-health givers and receivers’ condition 8 to understand the determinants of diffusion of innovation. Finally, this study explored the bridge between old and new healthcare systems. In general, the researchers studying m-health may more focus on how they make it possible to use a new technology or system efficiently for health providers in their healthcare practice contexts. They already assume that new technology is always useful and need to be disseminated soon. However, many providers need to consider the case for m-health as a linkage between old system and new system healthcare step by step before they adopt.
In future studies, it would be worthwhile to investigate patients’ views about m-health to understand how this technology can be tailored to their needs. Additionally, the cost for the m-health service can be seriously taken for discussion to health providers and recipients. Also, a representative survey of physicians in private and public sector hospitals in Sri Lanka would provide a better sense of how the country’s healthcare sector perceives m-health. Meanwhile, this topic could be extended into a consideration for the way to integrate m-health with Sri Lanka’s current healthcare system. With such ideas, this study can take another side of m-health application in order to supplement healthcare professionals’ opinions as considering how healthcare users or lay persons would evaluate and expect to use m-health technology. At the same time, it would be a continuing agenda for health providers how to minimize the gap between rural and urban areas in terms of the quality of health service and accessibility.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was partially supported by grant number R24HS022140 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.