
Abstract
Background
With the global spread of the coronavirus disease pandemic, governments have become more interested in applying telehealth technology in 2020.
Objective
This study integrates the technology acceptance model and information system success model to explore the influence of satisfaction, attitudes, and continued use of telehealth systems among middle-aged and older people in remote areas.
Methods
The study participants were patients over 40 years (inclusive) who lived in remote townships in eastern Taiwan, were diagnosed with diabetes or hypertension, and used the telehealth care system. In total, 545 questionnaires were returned, resulting in a recovery rate of 99%.
Results
Accepting the hypothesized structural equation model, this study found that information, system, and service quality were influenced by the mediating effect of perceived ease of use and the perceived usefulness of the technology acceptance model. The use of telehealth care systems among chronic patients increased significantly.
Introduction
With the global spread of the coronavirus disease 2019 (COVID-19) pandemic in 2020, governments have become more interested in applying telehealth technology. Telehealth can improve access to care, reduce utilization of medical center resources, and reduce infection transmission risk. 1 An important advantage of telemedicine, in addition to its being beneficial for keeping both patients and health workers safe, is that it improves access to healthcare givers, especially in cases of chronic conditions. 2 Telehealth can also bridge the gap between urban and rural medical resources and can become an essential tool for epidemic prevention during infectious disease outbreaks.
Several countries have applied information and communication technology to long-distance care by combining medical care and technological development. The resulting functions, which are expected to reduce medical and labor costs, include notifications of abnormalities, medication reminders, physiological recording and monitoring, remote video, and medical consultation.3,4
Telehealth can improve continuity of care, access to care, and health outcomes. The application of telehealth care systems can also support person-centered health care in COVID-19 treatment. 5 Remote health monitoring can help reduce unanticipated occurrences through timely treatment, prevent the wasting of medical resources, and monitor the compliance of patients with medical prescriptions. Previous studies found that telehealth is an effective tool for treating patients with diabetes and hypertension. It can reduce harm from disease progression and increase chronic patients’ willingness to accept self-care at home. 6 Telehealth services have the potential to improve access to care, especially in rural or urban areas with scarce health care resources. 7 Not only can it effectively control and reduce the incidence of hospitalization, but it can also significantly delay readmission.8–10
Previous research has established the benefits of telehealth care. A recent study using the Internet and a telehealth care system to strengthen interactions between the community, hospital staff, and family members through virtual video, telephone, and visitor management can effectively improve family members’ satisfaction and reduce patient transfer costs and length of hospitalization. 11 Several medical institutions in Taiwan have implemented telehealth care systems, allowing older and chronic patients to monitor physiological information at home and within the community to understand their health status and prevent disease. In addition, such systems can aid caregivers or family members in improving the quality of care for older adults. Therefore, telehealth care systems are currently among the most critical medical services. Monitoring the health status and home security of older adults using telehealth devices can help maintain a good quality of life and reduce the burden on their families, as well as the cost of care.
Currently, a considerable amount of research exists on adopting healthcare technology from the perspectives of healthcare professionals as users. 12 However, there is still a lack of an in-depth understanding of the motivations and needs associated with using telecare technology for older adults or those with chronic diseases. 13 Therefore, when the chronically ill or the older adults use remote care technology, health care workers must explore how to utilize healthcare-related information and communication technology to promote these individuals’ acceptance of remote care technology. To ensure that the telehealth care system achieves the aforementioned effects to aid such patients in the future, this study explored the experiences of and related factors in the acceptance of information technology among middle-aged and older patients who are chronically ill using a telehealth care system. To successfully extend life, it is necessary to improve the quality of life for individuals in their later years.
An information system’s success is determined by its user, whose behavioral attitudes and intentions may be affected by it. 14 According to the technology acceptance model (TAM), the user’s cognitive evaluation of whether the system is conducive to promoting work effectiveness and ease of use will affect his subsequent attitudes and intentions. 15 However, the information system success model (ISSM) focuses on the relationship between system output quality, user satisfaction, and benefits. No additional context for the impact on user attitudes, behaviors, or intentions is available. 16 Therefore, to fill this research gap, this study focuses on middle-aged and older patients and attempts to integrate the concepts of TAM and ISSM with the application of a telehealth care system for chronic disease management in remote areas during the COVID-19 pandemic.
Methods
Study sample
This study’s sample included middle-aged and older chronically ill patients with diabetes and hypertension who lived in six townships in eastern Taiwan (three in Hualien County and three in Taitung County) and used the telehealth care system. The sampling conditions included chronic patients who were: (1) medically diagnosed with diabetes or hypertension; (2) aged 40 years or older and using a telehealth care system; (3) able to speak Chinese, Taiwanese, or Hakka; and (4) willing to participate in this study.
Conceptual framework and hypothesis
Although this study is primarily based on the TAM, influential external variables may include factors such as system characteristics, user characteristics, and organizations. Therefore, some scholars have also proposed the use of “information quality (INQ),” “system quality (SYQ),” and “service quality (SEQ)” as well as the external variables of “perceived usefulness (UF)” and “perceived ease of use (EOU)” for study and discussion. 17
Therefore, this study adopts the ISSM and believes that “information quality,” “system quality,” and “service quality” will directly affect the users’ satisfaction and, ultimately, their “intent to use (INT).”
Before adopting new technology, users self-assess to determine whether their lives will benefit substantially from it.
14
As previous research has demonstrated, the higher the perceived usefulness of a telehealth care system, the higher the intention to use it. Similarly, the higher the perceived ease of use of the telecare system, the higher the intention to use it.
15
Figure 1 illustrates this study’s conceptual framework. Conceptual framework.
This study proposes the following research hypotheses:
“Information quality” has a positive relationship with “Perceived usefulness”; that is, the better the “Information quality” of the telehealth care system, the higher its “Perceived usefulness.”
“Information quality” has a positive impact on “Perceived ease of use”; that is, the better the “Information quality” of the telehealth care system, the higher its “Perceived ease of use.”
“System quality” has a positive relationship with “Perceived usefulness”; that is, the better the “System quality” of the telehealth care system, the higher its “Perceived usefulness.”
“System quality” has a positive impact on “Perceived ease of use”; that is, the better the “System quality” of the telehealth care system, the higher its “Perceived ease of use.”
“Service quality” has a positive impact on “Perceived usefulness”; that is, the better the “Service quality” of the telehealth care system, the higher its “Perceived usefulness.”
“Service quality” has a positive impact on “Perceived ease of use”; that is, the better the “Service quality” of the telehealth care system, the higher its “Perceived ease of use.”
“Perceived ease of use” has a positive impact on “Perceived usefulness.”
“Perceived usefulness” has a positive relationship with “Intent to use.”
“Perceived ease of use” has a positive effect on “Intent to use.”
Study tools
In this study, a structured questionnaire was used for data collection. Its content was revised with reference to domestic and foreign literature. The content of the questionnaire included: (1) basic demographic information such as sex, age, marriage, education level, and primary caregiver identification; (2) the ISSM.14,18–19; and (3) the TAM. 15
The ISSM contains five items in the information quality dimension (for example, the ability to provide what the patients need and timely, correct, or complete information); four items in the system quality dimension (for example, all functions work normally, fast connection speed, system stability, and fast query and archive speed); and four items in the service quality dimension (for example, can help chronic patients solve problems with the system or equipment). A five-point Likert scale was used (1 = strongly disagree, 5 = strongly agree), with higher scores representing higher levels of agreement. The TAM consists of four items of perceived usefulness, four items of perceived ease of use, and three items of intent to use. This measure was also scored using a five-point Likert scale (1 = strongly disagree, 5 = strongly agree), with higher scores representing higher levels of agreement.
Five experts and scholars were invited to conduct a validity appraisal of the questionnaire. Each questionnaire item was scored on the three dimensions of “importance,” “text clarity,” and “appropriateness,” and the title words were modified. After pre-testing the revised questionnaires, formal questionnaires were used to collect the data.
Data collection
This study was reviewed and approved by the Research Ethics Committee. The study trained interviewers who visited the homes of chronic patients using the telehealth care system. Patients were informed regarding the purpose of the research, and the data collection has obtained the respondents' verbal consent and filled in the consent form. Face-to-face interviews were used to collect the questionnaire data.
Results
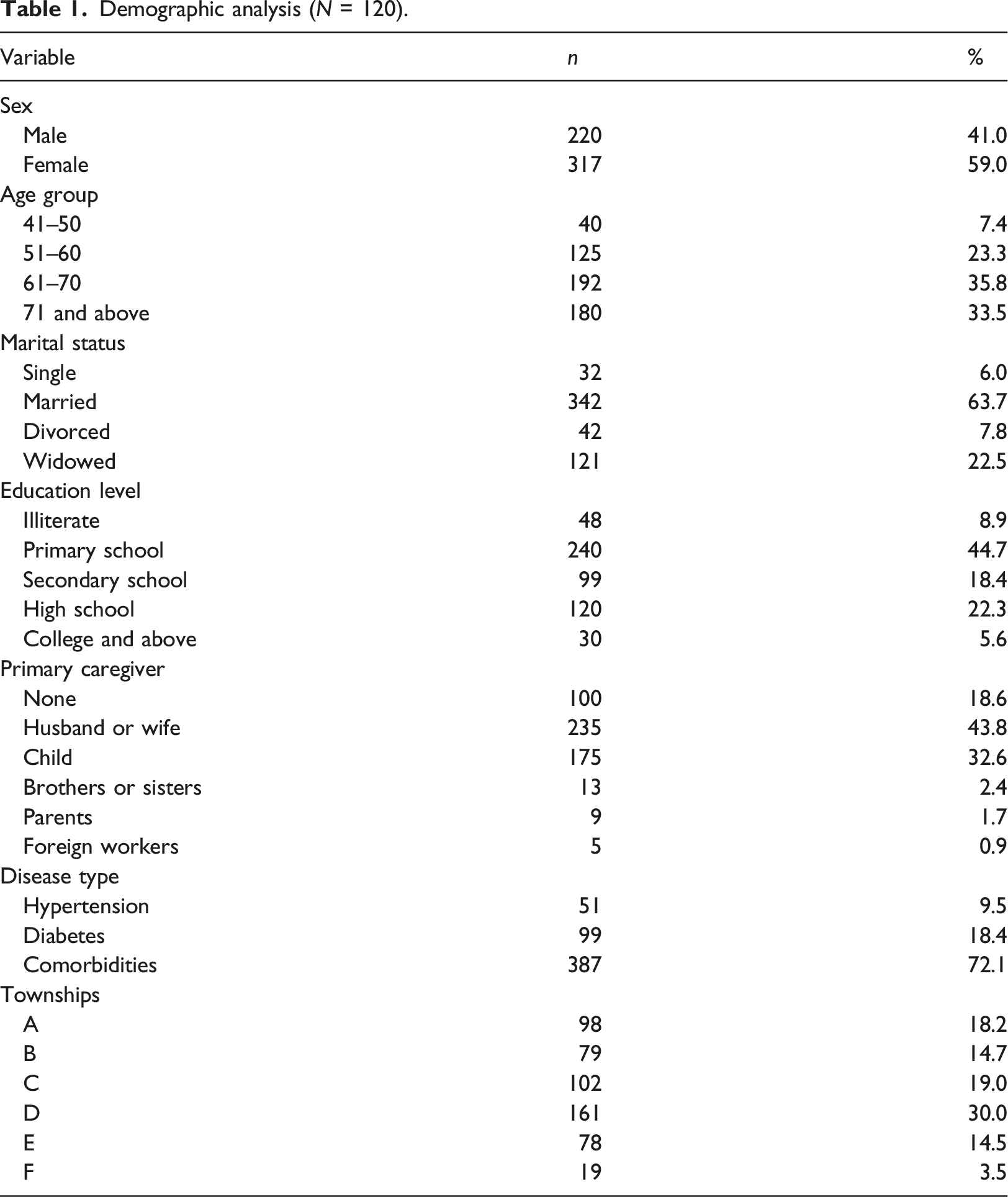
A total of 545 chronically ill patients used the telehealth care system, and 541 responded to the survey. Four questionnaires contained incomplete or inconsistent answers, so they were excluded from the analysis. In total, 537 valid questionnaires were recovered with a recovery rate of 99%.
Demographic analysis (N = 120).
Demographic variable differences in each dimension
Independent samples T test results for sex.

Differences of demographic variables in each dimension.

Reliability and validity of confirmatory factor analysis (CFA)
Standardized factor loading should ideally be higher than the threshold of 0.7, but values above 0.6 are acceptable. 20 The standardized factor loading in this study was between 0.65 and 0.93, indicating that the reliability of each item is acceptable. A square multiple correlation (SMC) greater than 0.5 is ideal, whereas 0.36 is acceptable. 21 In this study, the SMC ranged from 0.43 to 0.90. The composite reliability (CR) of the study components was between 0.90 and 0.96, all exceeding 0.7, which met the standard recommended by research. 22 The scale demonstrated good internal consistency for each facet.
Finally, the average variance extracted (AVE) calculates the variance explanatory power of each measured variable in relation to the latent variables. The higher the coefficient value, the better the discriminative and convergent validity of the results. This study’s AVE was between 0.70 and 0.82, which was greater than 0.5 and in line with empirical standards. 22 Each facet of the questionnaire was shown to have good convergent validity.
Measurement mode result analysis.
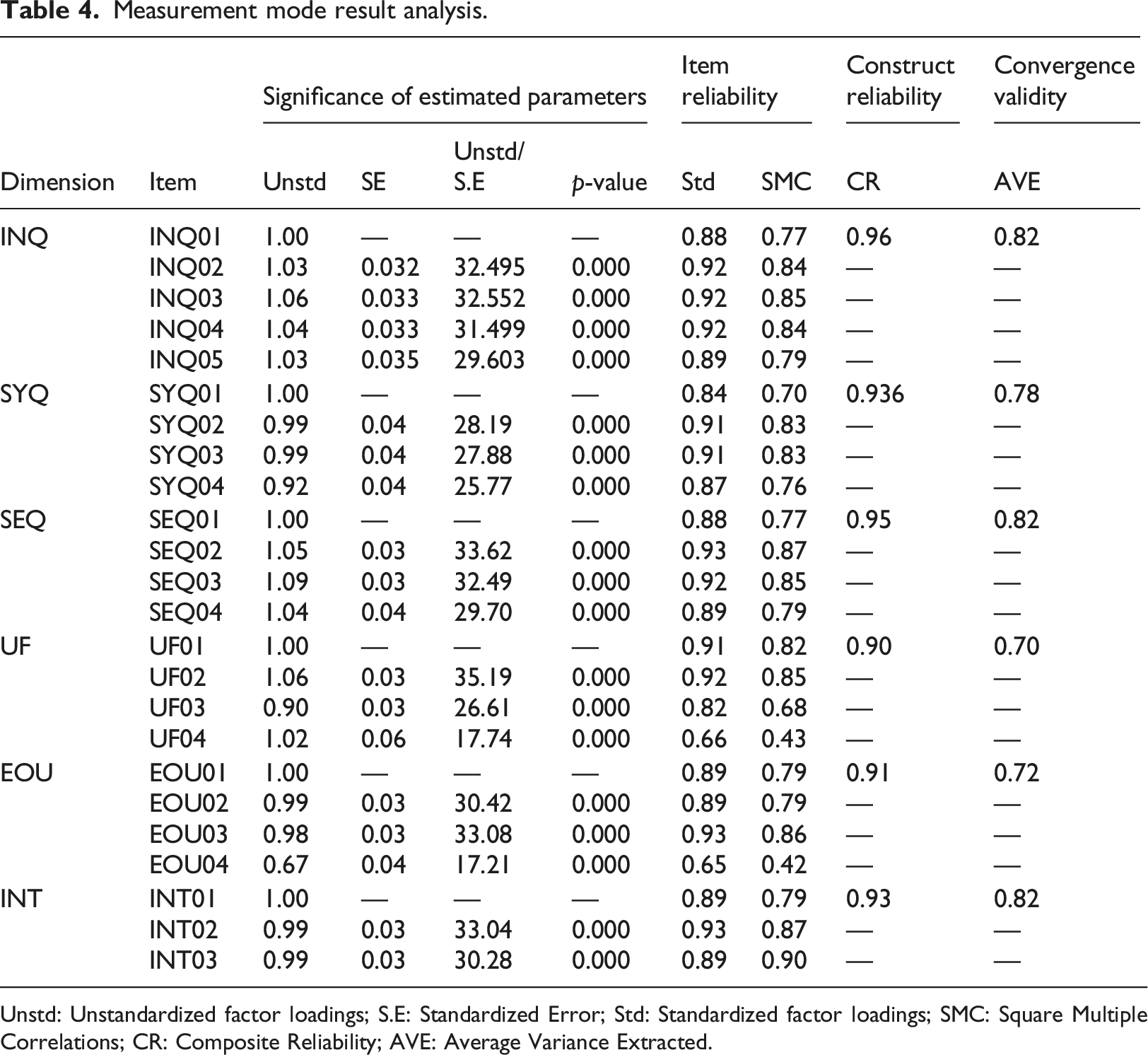
Unstd: Unstandardized factor loadings; S.E: Standardized Error; Std: Standardized factor loadings; SMC: Square Multiple Correlations; CR: Composite Reliability; AVE: Average Variance Extracted.
Structural equation model analysis
Structural model fit.

Validation of structural equation models
Regression coefficients.
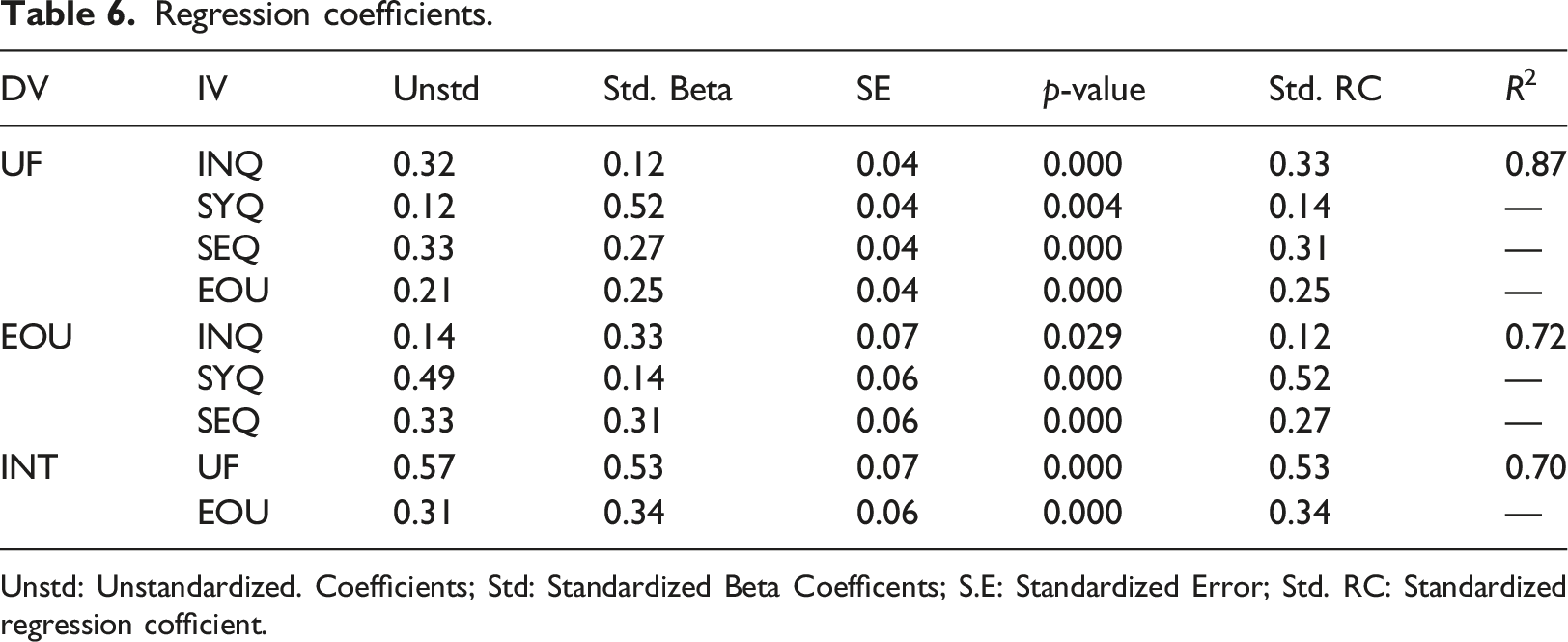
Unstd: Unstandardized. Coefficients; Std: Standardized Beta Coefficents; S.E: Standardized Error; Std. RC: Standardized regression cofficient.
Thus, the structural pattern hypothesis of this study was established (Figure 2). INQ, SYQ, and SEQ of the telehealth care system had a significant positive mediating effect on the EOU and UF of the TAM and a significant positive impact on chronically ill patients’ INT. EOU also directly affects UF. In short, if chronically ill patients perceive telehealth care systems as simple and easy to use, they will find them even more helpful. The INQ, SYQ, SEQ, and EOU were 87% predictive of UF. The INQ, SYQ, and SEQ were 72% predictive of EOU. UF and EOU were 70% predictive of explained INT. Overall structure model. Note: INQ, information quality; SYQ, system quality; SEQ, service quality; EOU, perceived ease of use; UF, perceived usefulness; INT, intention to use.
Discussion
This study found that information, system, and service quality have a significant impact on perceived ease of use and usefulness. In other words, when chronically ill patients believe that a telehealth care system’s information, system, and service quality are good, they will feel that the telehealth care system is easy to operate and can be learned and used without much effort. This may not only help these patients better control their chronic conditions, but it may also improve their quality of life.
Therefore, this study supports the discourse on the ISSM and TAM. If users are willing to use an information technology system, they must feel that these systems have good functions, are easy to use, offer correct information, and have good service quality. Most importantly, users find these systems helpful. In addition, this study supports the statement that ease of use affects the TAM’s proposed usefulness. It is necessary to help users perceive information technology as easy to learn and easy to use because the friendly design is the key point through which information technology systems become increasingly popular. Therefore, the functional interface of the telehealth care system, including the login, search, record, and service features, must use a straightforward design.
Finally, this study accepts the hypothesized structural equation model and finds that information, system, and service quality are influenced by the mediating effects of the TAM’s perceived ease of use and usefulness, thereby significantly increasing chronically ill patients’ use of telehealth care systems. In this study, patients were allowed to transmit physiological data such as blood pressure and blood sugar from their own homes to a remote health care system server. In addition, similar to other studies, telephone consultations and video services were provided.24,25 These results show that a useful and easy-to-use telehealth care system will increase users' willingness to continue to use it. Evaluations of good quality in all aspects are crucial, particularly following chronically ill patients’ use of the telehealth care system, because these comprehensive evaluations also affect patients’ willingness to continue using the system.
Therefore, the telehealth care system provider, whether a medical institution, health institution, or equipment manufacturer, must pay close attention to the users’ responses and feedback. Moreover, actively dealing with any issues reported by the users' response will promote their continued use of the system.
Conclusion
From the end of 2019 to the end of 2021, this plan trained volunteers in remote areas to become health gatekeepers; that is, semi-professional health care workers who assisted and taught chronically ill patients in remote areas to use the telehealth care information system. Patients were able to measure blood pressure, blood sugar, blood oxygen, heart rate, and other information at home. Then, they used mobile phones, tablets, or gateways to automatically upload information to the hospital cloud platform, which was capable of generating continuous physiological measurement records, analyzing cases, and proactively monitoring for abnormal measurements. If an abnormal situation was present, the platform proactively notified the patient, family members, and care team by message, phone line, email, or customer service contact so the medical staff could keep abreast of patients’ status when they were at home.
Devices used by chronically ill patients at this stage were funded by the Taiwanese government’s demonstration program. In the future, if the coverage of chronic diseases could be expanded and the telehealth system could be offered to more patients with other chronic diseases by taking a comprehensive inventory of the availability of various resources and considering the openness, connectivity, and continuity of back-end data, it will be possible to maximize health management benefits.
The COVID-19 pandemic has accelerated the progress of telehealth care and prompted changes in the healthcare system, making telehealth care play an essential, burden-sharing role. Medical institutions provide continuous care for chronically ill patients in remote areas through a telehealth system, which can solve the long-standing problem of uneven distribution of medical resources. 26 It is recommended that medical institutions, long-term care institutions, and community centers use remote health care in the future for public or patient health management. In addition, expanding the use of innovative technologies such as 5G mobile communication, Internet of Things, artificial intelligence, or big data analysis would allow the public to use professional medical diagnostic services through telehealth-related equipment without entering a hospital or clinic. In this way, the risk of cluster infection will be reduced, limited physical medical resources would be reserved for severely and acutely ill patients, and smart technology could be used to provide more comprehensive and dedicated medical care. 27
Footnotes
Acknowledgements
We express our gratitude for Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taiwan (R.O.C.) for providing research funds and all participating without whom this study could not have been successfully completed.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taiwan (R.O.C.).
Ethical approval
This study was reviewed and approved by the Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation Research Ethics Committee (IRB 108–209-B).