
Abstract
Background
The COVID-19 pandemic accelerated the adoption of telemedicine across healthcare specialties, with digital health technologies becoming essential tools for maintaining patient care while ensuring safety.
Objective
This cross-sectional study compared patient satisfaction and clinical outcomes between two widely used telemedicine modalities in urology: traditional phone calls versus WhatsApp messaging consultations.
Methods
Conducted in Madinah, Saudi Arabia, from March 2021 to December 2022, the study included 77 participants who chose either phone consultations (n = 32, 41.6%) or WhatsApp consultations (n = 45, 58.4%). Patient satisfaction was measured using validated 10-point scales, and urologist confidence in diagnosis was similarly assessed. Statistical analysis employed t-tests and Fisher's exact tests.
Results
Phone call users reported significantly higher initial satisfaction than WhatsApp users (8.7 vs. 8.0; p = 0.030), with no differences in urologist diagnostic confidence (p = 0.935) or follow-up satisfaction (p = 0.570). Phone calls were more frequently used for urgent cases (59.4% vs. 28.9%; p = 0.010), whereas WhatsApp was preferred for elective cases (71.1% vs. 40.6).
Conclusions
Both telemedicine modalities are clinically effective. Phone consultations provide superior immediate satisfaction, ideal for urgent needs, while WhatsApp offers a practical alternative for elective, asynchronous care. Healthcare systems can integrate either platform based on clinical urgency and patient preference.
Keywords
Introduction
The digital transformation of healthcare has fundamentally reshaped medical practice, with telemedicine emerging as a critical component of modern healthcare delivery systems. Originally conceptualized in the 1950s, telemedicine has experienced unprecedented growth over the past two decades, driven by advances in digital communication technologies and, more recently, by the global COVID-19 pandemic.1,2 The World Health Organization defines telemedicine as “the delivery of healthcare services by all healthcare workers using information and communication technologies for the exchange of dependable data for the diagnosis, treatment, and prevention of disease and injuries, research and evaluation, and continuing education of healthcare providers, where distance is an important aspect.” 3
The advantages of digital health technologies in clinical practice are multi-faceted, encompassing reduced financial burden on patients and healthcare systems, improved access to specialized care, enhanced appointment adherence, and the ability to maintain continuity of care during challenging circumstances.3–5 The COVID-19 pandemic served as a catalyst for widespread telemedicine adoption, as healthcare systems worldwide implemented lockdown measures and social distancing protocols. In Saudi Arabia, these circumstances necessitated rapid adaptation of healthcare delivery methods, with telemedicine becoming essential for maintaining urological care while minimizing infection risks. Recent evidence has further demonstrated the practical utility of digital communication platforms in urological care. For instance, a prospective observational study by Sancı et al. showed that mobile app communication significantly reduced emergency room visits following circumcision procedures, highlighting how digital health tools can effectively support post-operative monitoring and patient reassurance in urology. 6 Such applications exemplify the growing integration of telemedicine into routine urological practice, extending beyond consultation to encompass comprehensive perioperative care.
Urology, as a specialty, has demonstrated adaptability to telemedicine implementation. Recent studies have highlighted significant advantages of digital health applications in urological practice, including improved clinical outcomes, enhanced patient satisfaction, and cost-effectiveness compared to traditional in-person consultations.2,7 The benefits extend beyond mere convenience, encompassing improved access to specialized care for patients in rural or remote areas, reduced travel time and associated expenses, and enhanced monitoring capabilities for chronic urological conditions. Furthermore, telemedicine offers a more comfortable and private consultation environment, which can be particularly valuable in urology given the sensitive nature of many urological conditions, potentially leading to higher levels of patient engagement and treatment adherence. 8
Despite the growing body of evidence supporting telemedicine in urology, there remains a significant gap in comparative research examining different digital health modalities. While various platforms and communication methods are available for telemedicine delivery, limited evidence exists comparing the effectiveness and patient satisfaction between specific modalities such as traditional phone consultations and modern messaging applications like WhatsApp. This knowledge gap is particularly relevant in the context of developing healthcare systems, where resource optimization and patient preference accommodation are crucial considerations.
The present study addresses this gap by comparing the efficacy and patient satisfaction of two widely accessible telemedicine modalities: traditional phone calls and WhatsApp messaging consultations in urological practice. By examining these digital health approaches within the context of the Saudi Arabian healthcare system during the COVID-19 pandemic, this research contributes valuable insights into the practical implementation and comparative effectiveness of different telemedicine platforms in urology.
Methods
Study design and setting
This cross-sectional comparative study was conducted at a private urology clinic in Madinah, Saudi Arabia, from March 2021 to December 2022, and reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. The study period was specifically chosen to capture the peak implementation phase of telemedicine services during the COVID-19 pandemic, when traditional in-person consultations were limited due to public health restrictions. The research protocol received ethical approval from the Research Ethics Committee in the College of Pharmacy, Taibah University, Saudi Arabia (COPTU-REC), under the ethical reference number COPTU-REC-20210103Othman, dated January 3, 2021. The approval process adhered to established guidelines and regulations, including the Saudi National Regulation of the National Bioethics Committee, the Declaration of Helsinki, the International Conference on Harmonization (ICH), and the United States Codes of Federal Regulations.
Participants and eligibility
The study employed a convenience sampling approach, including all patients who contacted the private urology clinic for consultations during the study period and were unable to attend in-person visits due to COVID-19 restrictions or personal preferences. No specific age restrictions or exclusion criteria were applied, ensuring broad representation of the patient population seeking urological care. For participants under 18 years of age, medical history and consent were obtained from parents or legal guardians. All participants provided informed consent before consultation and were assured of confidentiality and anonymity throughout the study process.
Intervention and data collection
Upon initial contact with the clinic, patients were screened by the attending urologist and informed about the study objectives and procedures. Participants who agreed to participate were given the choice between two telemedicine modalities: phone call consultations or WhatsApp messaging consultations. This choice-based allocation was implemented to reflect real-world patient preferences and ensure practical applicability of the findings. Consultations in both modalities were conducted by three urologists from the same clinic, with each urologist handling both phone and WhatsApp consultations. All urologists followed a standardized protocol for patient assessment, diagnosis, and treatment recommendations to ensure consistency across evaluations and minimize provider-dependent bias.
For the phone consultation group, the urologist initiated contact within 24 h of the patient's request, conducting a structured telephone interview to gather medical history, assess symptoms, and provide clinical recommendations. For the WhatsApp consultation group, the urologist sent an initial message within 24 h, requesting patients to provide their medical information, symptoms, and any relevant images or documents through the WhatsApp platform.
During each consultation, the urologist systematically recorded comprehensive data including the mode of communication, consultation type (urgent or elective), demographic characteristics (age, gender, and education level), presenting symptoms (chief, secondary, and tertiary complaints), provisional diagnoses (primary and secondary), and treatment recommendations (first- and second-line). The consultation duration was recorded for phone calls, while message exchange patterns were documented for WhatsApp consultations.
Outcome measures
The primary outcome measure was patient satisfaction at the time of consultation, assessed using a validated 10-point Likert scale ranging from very dissatisfied (1) to very satisfied (10). Secondary outcome measures included urologist confidence and satisfaction with the diagnosis, measured using a similar 10-point scale from very dissatisfied/low confidence (1) to very satisfied/high confidence (10). Additional secondary outcomes encompassed patient satisfaction after follow-up consultation, patient-reported improvement at follow-up (measured on a binary yes/no scale), and consultation type classification (urgent vs. elective) based on the urologist's clinical assessment. However, clinical improvement was assessed based on patient self-report without objective clinical measures, consistent with the pragmatic design of this real-world study.
Follow-up assessments were conducted through phone calls or WhatsApp messages, depending on the initial consultation modality, to evaluate patient satisfaction with the overall care process and assess clinical improvement or symptom resolution. The timing and duration of follow-up varied based on clinical need and patient response, reflecting the pragmatic nature of real-world clinical practice.
Sample size considerations
The sample size for this study was determined by practical considerations and the available patient population during the study period, rather than formal statistical power calculations. This represents a limitation of the study design, as acknowledged in the Limitations section. The convenience sampling approach was necessitated by the urgent need to implement telemedicine services during the pandemic and the exploratory nature of comparing these two specific modalities in the local healthcare context.
Statistical analysis
Data analysis employed both descriptive and inferential statistical methods using IBM SPSS version 27.0.1. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to characterize participant demographics and response patterns. The normality of continuous variables was assessed through visual inspection of Q–Q plots and the Shapiro–Wilk test where appropriate.
For inferential analysis, Fisher's exact test was utilized to examine associations between categorical variables, including preference patterns and consultation types. Independent samples t-tests were employed to compare continuous variables, such as satisfaction scores, between the two consultation groups. The significance level was set at p < 0.05, corresponding to a 95% confidence interval. All statistical tests were two-tailed, and effect sizes were calculated where appropriate to assess the clinical significance of observed differences. However, no adjustments for multiple comparisons were applied, which should be considered when interpreting statistical significance.
Results
Participant characteristics
The study included 77 participants, with 32 (41.6%) choosing phone call consultations and 45 (58.4%) opting for WhatsApp consultations. The demographic characteristics were well-balanced between groups, indicating no significant selection bias based on basic demographic factors. As detailed in Table 1, the majority of participants in both groups were new patients (90.6% in the phone group vs. 82.2% in the WhatsApp group; p = 0.711), male (74.2% vs. 68.2%; p = 0.616), and local residents of Madinah (81.3% vs. 71.1%; p = 0.423). Educational attainment was similar between groups, with the majority holding bachelor's degrees (60.7% vs. 59.0%; p = 1.000).
Sociodemographic characteristics of the participants by consultation group.

Values are presented as mean ± SD; all other values are presented as No. (proportion %).
The mean age was 37.9 ± 17.0 years for the phone consultation group and 32.5 ± 16.2 years for the WhatsApp group, with no statistically significant difference (p = 0.163). This age distribution suggests that both younger and older patients were comfortable using either telemedicine modality, indicating broad acceptability across age groups.
Clinical presentations and management
Analysis of clinical presentations revealed similar patterns of urological complaints between the two groups, as comprehensively presented in Table 2. The most common chief complaints in both groups included voiding lower urinary tract symptoms (LUTS), dysuria, storage LUTS, and flank pain, with no statistically significant differences in the distribution of presenting symptoms (p = 0.678). Dysuria emerged as the most frequent secondary complaint in both groups (54.5% in the phone group vs. 50.0% in the WhatsApp group; p = 0.307).
Differences in symptoms, diagnosis, and treatments between the two groups.
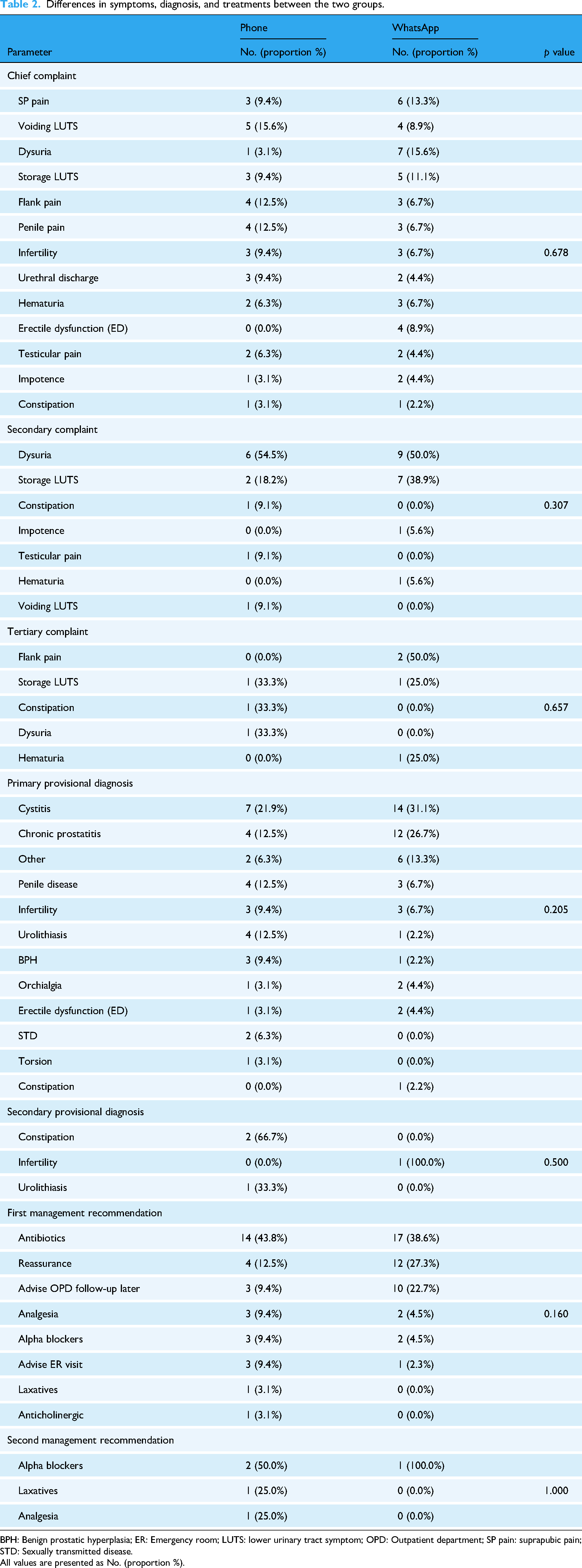
BPH: Benign prostatic hyperplasia; ER: Emergency room; LUTS: lower urinary tract symptom; OPD: Outpatient department; SP pain: suprapubic pain; STD: Sexually transmitted disease.
All values are presented as No. (proportion %).
Provisional diagnoses were comparable between groups, with cystitis being the most prevalent diagnosis (21.9% in the phone group vs. 31.1% in the WhatsApp group; p = 0.205). Other common diagnoses included chronic prostatitis, urolithiasis, and various penile conditions. The similarity in diagnostic patterns suggests that both telemedicine modalities were equally effective in facilitating accurate clinical assessment.
Treatment recommendations also showed no significant differences between groups, as documented in Table 2. Antibiotics were the most frequently prescribed first-line treatment in both groups (43.8% vs. 38.6%; p = 0.160), followed by reassurance and advice for outpatient follow-up. Alpha-blockers were commonly recommended as second-line therapy when applicable.
Consultation characteristics and satisfaction outcomes
The mean consultation duration for phone calls was 9.3 ± 3.8 min, providing a baseline for comparison of consultation efficiency. WhatsApp consultations, being asynchronous, did not have a directly comparable time metric but allowed for more flexible communication patterns.
Patient satisfaction at the time of consultation showed a statistically significant difference between groups, as illustrated in Figure 1, with phone call users reporting higher satisfaction scores compared to WhatsApp users (8.7 ± 0.9 vs. 8.0 ± 2.1; p = 0.030). This represents a clinically meaningful difference of 0.7 points on the 10-point scale, suggesting that the immediate, synchronous nature of phone consultations provided superior patient experience during the initial consultation phase.
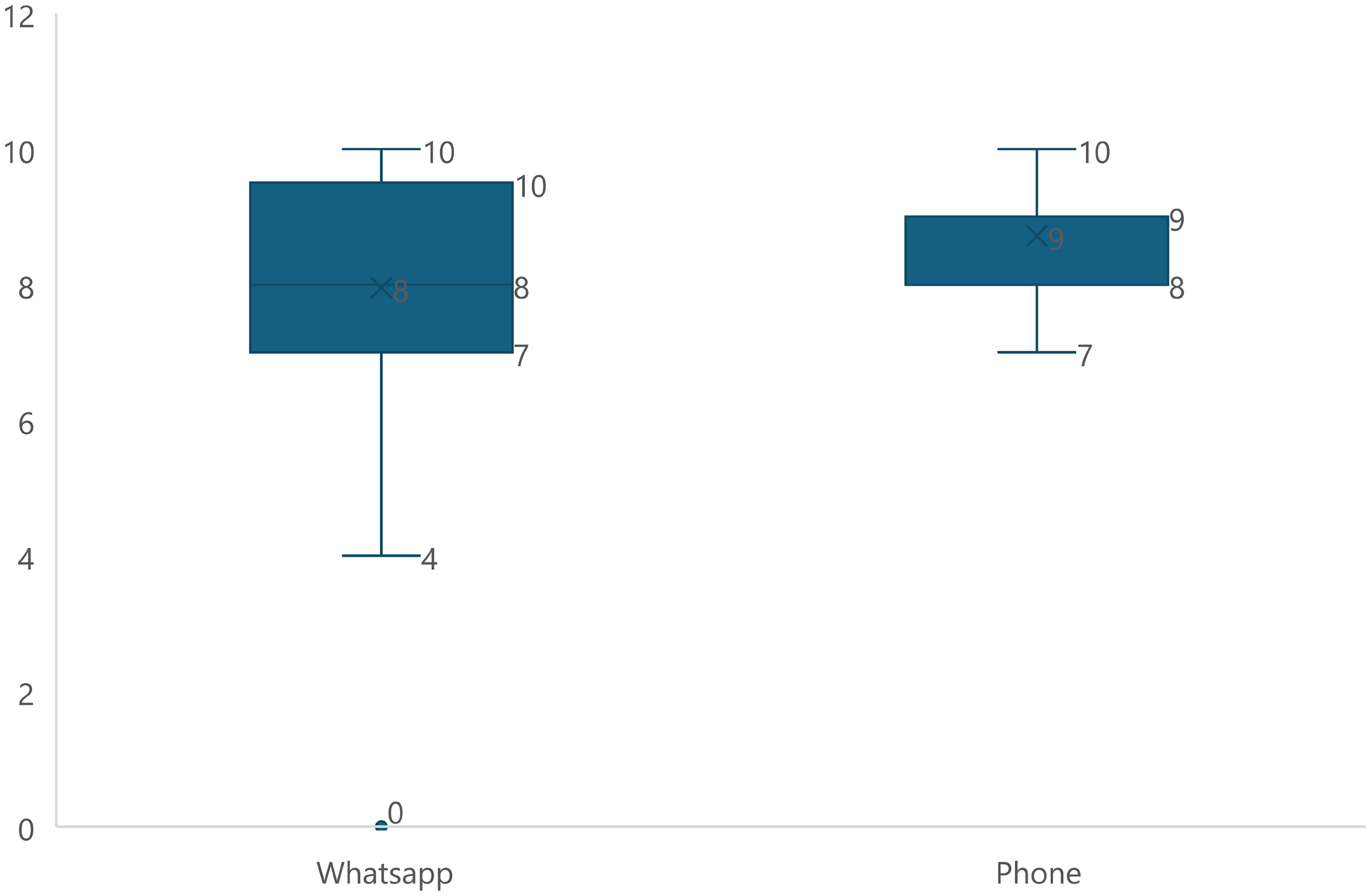
Comparison of patient satisfaction at consult time between patients using the two methods of consultation.
However, urologist confidence and satisfaction with diagnosis showed no significant difference between groups (7.7 ± 1.8 vs. 7.8 ± 2.1; p = 0.935), indicating that both modalities enabled clinicians to achieve similar levels of diagnostic confidence. This finding suggests that the clinical effectiveness of both approaches was comparable from the healthcare provider's perspective.
Follow-up satisfaction scores also demonstrated no significant difference between groups (9.0 ± 2.1 vs. 8.7 ± 2.5; p = 0.570), indicating that any initial satisfaction differences were resolved during the follow-up phase. Patient-reported improvement at follow-up showed a trend favoring phone consultations (70.8% vs. 51.4%) but did not reach statistical significance (p = 0.181).
Consultation type patterns
A significant difference emerged in consultation type preferences between the two modalities (p = 0.010), as demonstrated in Figure 2. Phone consultations were more frequently utilized for urgent cases (59.4% vs. 28.9%), while WhatsApp consultations were predominantly chosen for elective cases (71.1% vs. 40.6%). This pattern suggests that patients and healthcare providers intuitively recognized the advantages of synchronous communication for urgent situations requiring immediate clinical decision-making, while asynchronous WhatsApp communication was preferred for routine, non-urgent consultations.

Comparison of type of consultation between the participants using the two groups of consultation.
This finding has important implications for healthcare system planning and resource allocation, suggesting that different telemedicine modalities may be optimally suited for different types of clinical scenarios. The preference for phone consultations in urgent situations likely reflects the need for immediate clarification, real-time clinical assessment, and prompt therapeutic decision-making that characterizes urgent urological presentations.
The comprehensive results of satisfaction measures, consultation outcomes, and comparative effectiveness metrics are systematically presented in Table 3, which demonstrates the nuanced differences and similarities between both telemedicine modalities across multiple outcome measures. These findings collectively support the implementation of multi-modal telemedicine approaches that leverage the specific advantages of each communication platform based on clinical context and patient needs.
Satisfaction and results of the participants using the two groups of consultation.
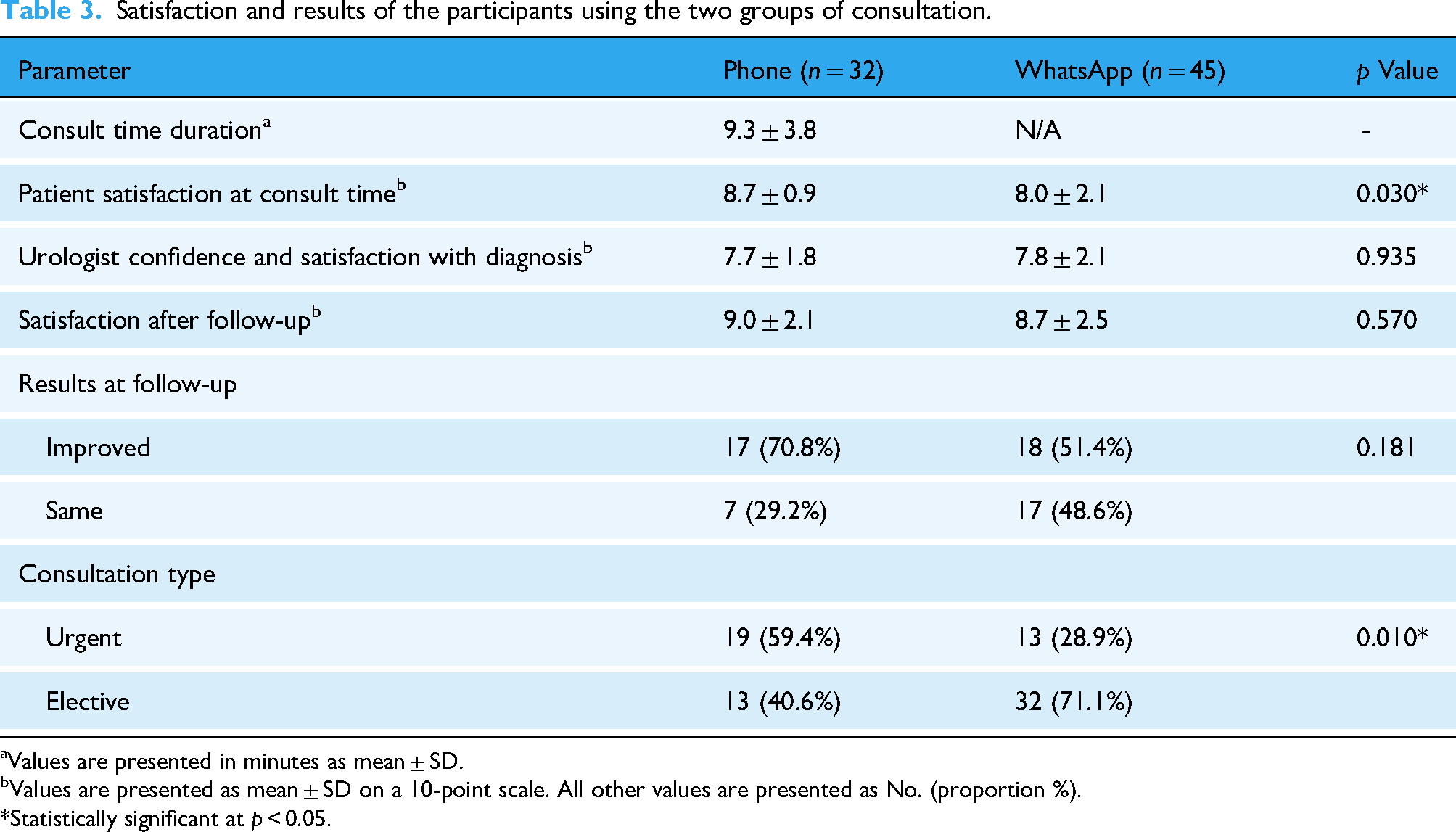
Values are presented in minutes as mean ± SD.
Values are presented as mean ± SD on a 10-point scale. All other values are presented as No. (proportion %).
*Statistically significant at p < 0.05.
Discussion
Principal findings and clinical implications
This study compared two widely accessible digital health modalities in urological telemedicine. Phone consultations yielded significantly higher patient satisfaction during initial consultations while maintaining equivalent clinical outcomes and follow-up satisfaction. The satisfaction difference of 0.7 points on a 10-point scale, though statistically significant, represents a modest effect that should be interpreted with caution given the overall high satisfaction levels in both groups.
Urologists reported equivalent diagnostic confidence across both modalities (7.7 vs. 7.8; p = 0.935), suggesting that digital health technologies effectively support clinical decision-making regardless of communication platform. This finding indicates that provider confidence and clinical effectiveness are not significantly compromised by choosing between synchronous and asynchronous communication modalities.
Contextual significance in digital health implementation
The COVID-19 pandemic accelerated telemedicine adoption globally from gradual evolution to urgent necessity.9,10 In the Saudi Arabian context, where telemedicine utilization in urology reached 36.15% during the pandemic—significantly higher than in other regional healthcare systems—the findings of this study provide crucial evidence for sustainable digital health implementation strategies.11,12
The preference patterns observed in this study, with phone consultations being favored for urgent cases and WhatsApp for elective consultations, align with broader digital health utilization trends. This differentiation suggests that patients and healthcare providers intuitively recognize the optimal applications of different telemedicine modalities, supporting a hybrid approach to digital health implementation rather than a one-size-fits-all strategy.
Comparison with existing literature
The findings of this study are consistent with previous research demonstrating the effectiveness of telemedicine in urology. Viers et al. 13 reported that two-thirds of urology patients were willing to participate in telemedicine consultations, with comparable clinical outcomes to traditional in-person visits. Similarly, a randomized controlled trial by the same research group found that video consultations provided similar face time with providers (14.5 vs. 14.3 min; p = 0.96) while offering superior convenience and reduced time away from work. 14 It is important to note that this study focused on phone and WhatsApp consultations rather than video-based telemedicine, which has become standard in many healthcare systems. This focus reflects the pragmatic reality of our clinical setting during the COVID-19 pandemic, where phone and WhatsApp were the only readily available modalities. Video consultation infrastructure was not accessible during the study period, necessitating rapid implementation of immediately available platforms. While systematic reviews have demonstrated comparable outcomes across various telehealth modalities,15,16 our findings provide valuable insights for healthcare systems implementing telemedicine under resource constraints or during crisis situations where sophisticated infrastructure may not be feasible.
The higher satisfaction with phone consultations may reflect the immediate, interactive nature of voice communication, allowing real-time clarification and emotional support through vocal cues. This aligns with research by Patel and Douglas-Moore, 17 who reported 93% patient satisfaction with phone consultations in urology, with 83% of patients expressing preference for future phone consultations over in-person visits.
WhatsApp's effectiveness in clinical practice, particularly for conditions requiring visual assessment such as hematuria, has been previously documented by Sener et al. 18 However, our study found no significant preference for WhatsApp among patients with hematuria, suggesting that the visual capabilities of messaging platforms may not always translate to patient preference, possibly due to privacy concerns or comfort with traditional communication methods.
Digital health technology adoption and patient preferences
The demographic analysis revealed no significant differences in age, gender, or education level between groups, suggesting broad acceptability of both digital health approaches across diverse patient populations. This contradicts common assumptions about technology adoption being primarily driven by age or educational factors, indicating that healthcare technology acceptance may be more influenced by clinical needs and personal preferences than by demographic characteristics.
The observed pattern of consultation type preferences—with urgent cases gravitating toward phone consultations and elective cases toward WhatsApp—provides valuable insights for healthcare system design. This natural selection pattern suggests that patients and providers can effectively self-select appropriate digital health modalities based on clinical urgency and communication needs, supporting the implementation of multi-modal telemedicine platforms.
Healthcare system implications
The comparable clinical effectiveness of both modalities, combined with different optimal use cases, supports implementing diversified telemedicine platforms. Phone consultations may be prioritized for urgent care pathways and initial consultations requiring immediate patient reassurance. WhatsApp consultations may be optimal for routine follow-ups, medication adjustments, and non-urgent communications.
WhatsApp consultations may require less immediate physician time and can be managed more flexibly within clinical workflows, offering cost-effectiveness advantages. However, superior immediate satisfaction with phone consultations suggests that patient experience metrics should be considered alongside efficiency measures when designing telemedicine programs.
Future directions and digital health evolution
The findings of this study contribute to the growing evidence base supporting personalized approaches to digital health implementation. Future research should explore the integration of artificial intelligence and clinical decision support systems with both synchronous and asynchronous telemedicine modalities to further enhance clinical effectiveness and patient satisfaction.
Hybrid consultation models combining the immediate satisfaction benefits of phone consultations with the convenience and documentation advantages of messaging platforms represent an important area for future investigation. Research into patient-specific factors predicting optimal telemedicine modality selection could enable more personalized and effective digital health delivery.
Limitations
This study has several important limitations that should be considered when interpreting the findings. First, the sample size was determined by practical considerations and available patient population during the study period rather than formal statistical power calculations. This convenience sampling approach may affect the generalizability of the findings to broader patient populations.
Second, the study did not systematically assess the underlying reasons for patient preferences between WhatsApp and phone consultations, nor did it measure specific factors that could influence satisfaction levels with each modality. Understanding these preference drivers could provide valuable insights for optimizing telemedicine implementation strategies.
Third, consultations were conducted by three different urologists, which may introduce inter-rater variability despite each urologist handling both modalities and following a standardized protocol. However, all urologists practiced at the same clinic and adhered to consistent clinical guidelines, minimizing potential bias.
Fourth, the single-center design and specific cultural context of Saudi Arabia may limit the generalizability of findings to other healthcare systems and cultural settings. Different populations may have varying comfort levels with digital technologies and different communication preferences that could influence the comparative effectiveness of these modalities.
Fifth, the study period coincided with the COVID-19 pandemic, which may have influenced patient and provider attitudes toward telemedicine in ways that might not persist in post-pandemic healthcare delivery. The urgent need for remote healthcare during this period may have affected satisfaction and acceptance patterns. Additionally, no correction for multiple comparisons was applied in the statistical analysis, potentially increasing type I error risk. This limitation should be considered when interpreting the statistical significance of observed differences between modalities.
Finally, the study lacked standardized follow-up protocols and relied on subjective outcome assessment. Follow-up timing and duration varied based on clinical need rather than predetermined intervals. Clinical improvement was measured through patient self-reported binary responses rather than objective metrics such as validated symptom scores, complication rates, recurrence rates, or re-consultation rates. These methodological limitations restrict comprehensive evaluation of sustained clinical effectiveness across both modalities.
Conclusions
This study demonstrates that phone consultations and WhatsApp messaging serve complementary rather than interchangeable roles in urological telemedicine. Both modalities achieved comparable diagnostic confidence and clinical outcomes. While phone consultations yielded statistically higher initial satisfaction scores, this difference was modest in clinical magnitude. Phone consultations were preferred for urgent cases, while WhatsApp was favored for elective care.
These findings support multi-modal telemedicine platforms that leverage the complementary strengths of both approaches. Phone consultations may be preferable for urgent scenarios requiring immediate communication, while WhatsApp provides an effective solution for routine follow-ups. Healthcare systems should integrate complementary modalities tailored to specific clinical contexts rather than single-platform approaches.
Future research should develop evidence-based guidelines for context-appropriate modality selection and explore hybrid models integrating the complementary benefits of both communication types.
Footnotes
Acknowledgments
The authors would like to thank all participants who contributed to this study and the healthcare professionals who facilitated the data collection process during the challenging circumstances of the COVID-19 pandemic.
Preprint disclosure
An earlier version of this manuscript was posted as a preprint on Research Square under the title “Efficacy and Patient Satisfaction of Urological Phone Call versus WhatsApp Consultation During COVID-19 Lockdown” on August 9, 2024 (![]() ). The current manuscript represents a substantially revised and improved version with enhanced methodology, expanded analysis, and comprehensive discussion aligned with digital health perspectives.
). The current manuscript represents a substantially revised and improved version with enhanced methodology, expanded analysis, and comprehensive discussion aligned with digital health perspectives.
Ethics approval and consent to participate
The Research Ethics Committee in the College of Pharmacy, Taibah University, Saudi Arabia (COPTU-REC) granted approval for this research under the ethical reference number COPTU-REC-20210103Othman on January 3, 2021. The approval followed guidelines and regulations, including the Saudi National Regulation of the National Bioethics Committee, the Declaration of Helsinki, the International Conference on Harmonization (ICH), and the United States Codes of Federal Regulations. Each participant provided informed consent to participate.
Consent for publication
Not applicable. This study does not contain any individual person's data in any form.
Author contributions
Conceptualization: MA (Mansour Alnazari), MA. Methodology: MA (Mansour Alnazari), AB, and MA. Formal analysis: MMA (Musab M. Alghamdi). Data curation: MA (Mansour Alnazari), AB, ESR, and AM. Writing—original draft preparation: MA (Mansour Alnazari), MMA (Musab M. Alghamdi), SA, SOA, and NO. Writing—review and editing: MA (Mansour Alnazari), AB, ESR, and AM. Supervision: MA. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Data are available upon request from the corresponding author.
Guarantor
Mansour Alnazari accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.