
Abstract
Background
Sound and reliable health information is needed to promote culture of evidence based decision making. The aim of this study was to assess knowledge and attitudes of healthcare providers to use District health information system among public health facilities in South-West Ethiopia.
Method
Cross sectional quantitative study was conducted. A total of 264 participants were approached. Descriptive and analytical statistics was done.
Result
Overall 130 (49.2%) of respondents had good knowledge to use DHIS (95% CI: [43, 55.3]). 149 (56.4%) of respondents had favourable attitudes (95% CI: [53.2, 59.8]). Sufficient skills [AOR = 2.20, 95% CI: (1.16, 4.19)], older age [AOR = 1.92, 95% CI: (1.03, 3.59)] , resources [AOR = 2.56, 95% CI: (1.35, 4.86)], staffing [AOR = 2.85, 95% CI: (1.49, 5.48)] and high experiences [AOR = 4.66, 95% CI: (1.94, 5.78)] were variables associated with knowledge. Being trained [AOR = 3.59, 95% CI: (2.48, 5.42)], provision of feedback [AOR = 4.08, 95% CI: (1.87, 8.91)], motivation [AOR = 2.87, 95% CI: (1.36, 6.06)] and health need [AOR = 2.32, 95% CI: (1.10, 4.92)] were variables associated with attitudes
Conclusion
Thus, Knowledge and attitudes of healthcare providers to use DHIS working in public health facilities in this setting is relatively low. The results highlight the need to improve knowledge and attitudes to use DHIS among healthcare providers focusing on the identified gaps.
Background
Sound and reliable information is the foundation across all health system building blocks and is essential for health system policy development and implementation, governance and regulation, health research, human resources development, health education and training, service delivery and financing. 1 Health Information system (HIS) as an integral part of health system, is used to facilitate the use of population based data that has been widely generated from health facilities. 2 The District Health Information System (DHIS), is an open source electronic Information system currently used in over 60 countries to manage and visualize routine health data, particularly facility based data. 3 DHIS has to be able to protect patient’s data to increase quality of health service. This is because, DHIS is required so as to provide allowable users’ accessibility to the patient’s data all the time. 4
The Ethiopian health information system includes all data and records about the population’s health. Of this, health management information system (HMIS) has been reformed with a big reduction in data collection tools and limited variables at regional and national levels.5–7 One of the strategic changes made is standardization with one data source, one channel and one reporting system, as opposed to the previous fragmented vertical system for different health programs.5,8
Ethiopia has nationally driven strategy of national eHealth coordination and alignment to build a flexible and efficient eHealth capability. This strategy, the National eHealth strategy of Ethiopia is aimed at guiding and streamlining the Information and Communication Technology (ICT) solutions in the healthcare sector.7,9 To adapt e-health standards (Legal and Regulatory framework), Implementing the national ICT infrastructure for e-health (Infrastructure, standards and system for eHealth) and Establish governance and leadership for eHealth were among strategic Areas of strategic plan of HIS.5,8,10
The DHIS helps to collect, analyse and utilize reliable data that is vital for health workers to provide a cost effective health care to the population in addition to timely and accurate Information which is crucial policy maker to be able to make well in med decisions to improve national health care.11–13 The World health organization has identified health Information system as one of the six key attributes, or building blocks of a health system including health work force, leadership and governance, health service delivery, health care financing, and access to essential medicine.14–16 However the DHIS in most developing countries is inefficient and is greatly affected by unreliability of data resulting from under reporting. 1
The WHO has identified that the problem of under reporting is huge and is linked to the lack of knowledge and attitudes among the health workers characterized by insufficient analysis skill, training and lack of initiative for using information.11,17,18 In Ethiopia, healthcare providers includes Performance Monitoring Team (PMT), a team of multidisciplinary health work force that is primarily responsible to improve data quality, use information regularly, monitor progress and improve performance of health care delivery at all levels of the health system. PMT is healthcare providers serving as one of the major platforms for health information use in Ethiopia.19,20 To promote utilization of DHIS, to meet one of the transformation agenda of the Ministry of Health of Ethiopia, healthcare providers’ attitudes and knowledge to use locally collected data for evidence based decision making is a mandatory path to provide quality of health service.19,20
Understanding the attitudes and knowledge of healthcare providers towards utilization of DHIS is important for the provision of effective and efficient health services. 21 Determining the healthcare providers’ attitudes and knowledge will also aid in understanding the impact of DHIS on workload and quality of clinical health care.22–24 Studies have identified that the knowledge and attitudes of healthcare providers to use DHIS is required where over 90% of available data are generated within only 2 years that requires wise use of this data.25,26 The standard procedure for data use and measurement of the health system in sub Saharan Africa was too low due to poor knowledge and attitudes among healthcare providers. 25
Utilization of DHIS is expected to promote the quality of health service but lack of favourable attitudes and sufficient knowledge are among the prominent factors that hindering the use of DHIS among healthcare providers.21,27–30 As an emerging of DHIS2 software technology in the health sector of Ethiopia, to facilitate the quality of health services, it prominently require information about the knowledge and attitude toward utilization of DHIS among healthcare providers.31,32 However, considering the problem of health data collection in the health facilities and the utilization of reliable health information, the need arise to assess the knowledge and attitude of health care workers towards the use of DHIS. This because positive attitude of healthcare providers may lead to the successful running of DHIS utilization. Therefore, this study aimed to assess the knowledge and attitudes of healthcare providers to DHIS and factors that will affect their extent of knowledge and attitudes of using DHIS for their decision making purpose.
Methods
Study design and setting
A quantitative cross sectional study design was conducted from 01 March 2020 to 29 April 2020. The study was conducted among public health facilities in South west of Ethiopia. It’s included different health facilities that covers Health center, Hospitals and Referral Hospitals. All public health facilities within the selected areas of this study was attempted to be accessed. Hence that, overall forty one (41) health centers, two (2) hospitals (one Referral hospital and one primary hospital) of the selected study areas were approached for this study.
Study participants and sample size determination
The study has focused mainly on healthcare providers those who deeply interact with generation and utilization of data. The healthcare providers participated in handling data, generating data, using generated data and they serve as a focal person/head within their department/wards collectively known as PMT members according to Ethiopian health system context and they trained in DHIS2 use. Sample size was also determined based on study participants of every health facility. So that the total number of study participants within the zone were 264, by reaching all DHIS data users. Hence that, all DHIS users were approached.
Operational definition
Attitudes of health professionals
Healthcare providers those who scored the median value and above the median values were categorized as favourable attitudes to use DHIS whereas those who scored of less than median values categorized as unfavourable attitudes to use DHIS.
Knowledge of health professionals
The healthcare providers scored of median values and above the median values were categorized as good knowledge to use DHIS whereas less than median values categorized as poor knowledge.
Data collection tools and procedures
A self-administered English version questionnaire was used to collect data from study participants. The questionnaire for this study was adopted from the Performance of Routine Information System Management (PRISM) tool with other related literature and pretested for its content validity.26,33,34 Additionally the tool was piloted in other zone (East Wollega) that had comparable settings to the study sites. Reliability analysis was carried out before starting the actual data collection to see whether the tool can measure the true value of the outcome variable.
Data quality control
Data was collected by trained data collectors using an English version questionnaires. Before the actual data collection, a pre-test was conducted among 5% of samples at Buno Bedelle general hospital and health center at Bedelle town. The validity of the questionnaire was determined based on the view of experts and the reliability was obtained by calculating the value of Cronbach’s alpha (α = 0.78).
Data processing and analyzing
The data entry and analysis was done by SPSS version 22. To explain the study population in relation to relevant variables, descriptive statistics was used. Associations between dependent and independent variables were checked and their strength was presented using odds ratios and 95% confidence intervals. Both bi variable and multivariable logistic regression was used to assess the association between outcome and explanatory variables. A P value < 0.05 was considered statistically significant in the multivariable logistic regression.
Result
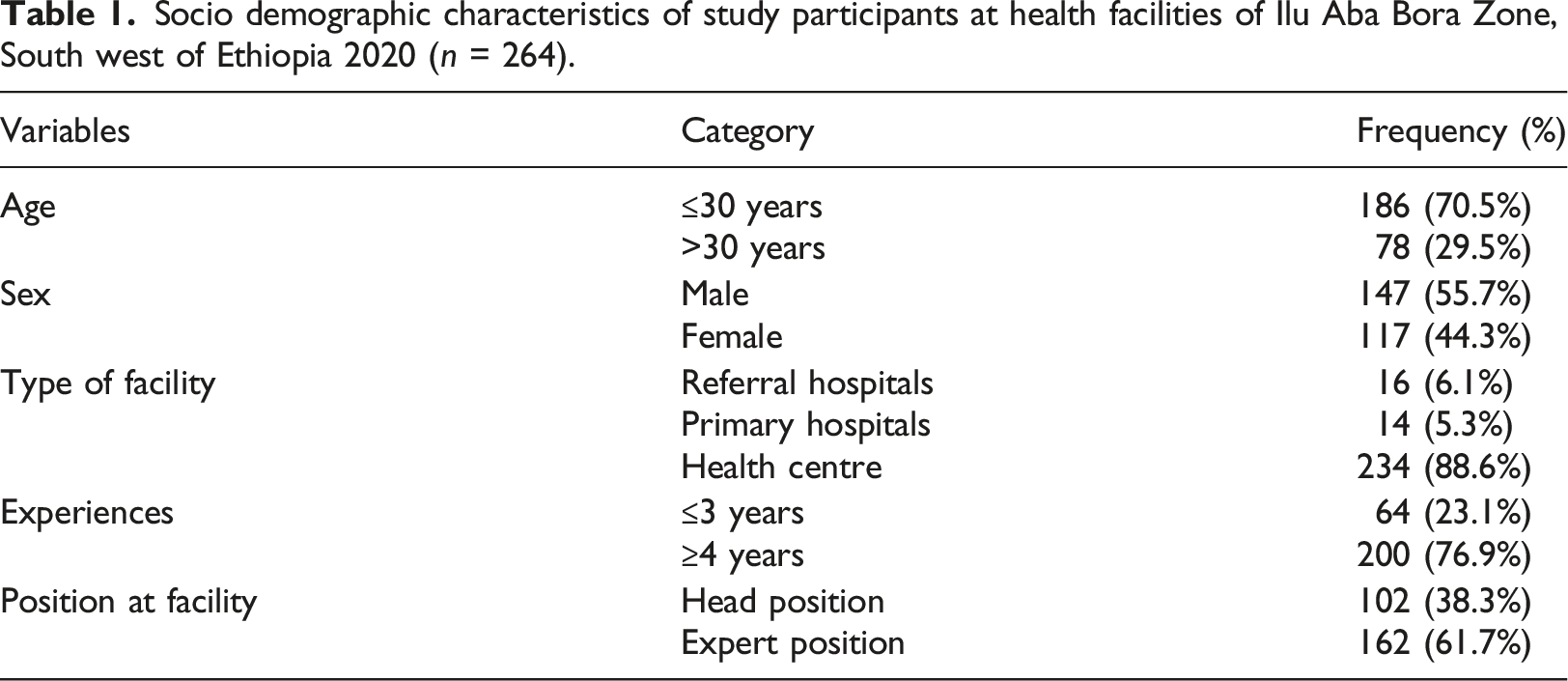
Socio demographic characteristics
Socio demographic characteristics of study participants at health facilities of Ilu Aba Bora Zone, South west of Ethiopia 2020 (n = 264).
Knowledge and attitudes towards the use of district health information system
Of the study participants approached, near to half of respondents 130 (49.2%) have good knowledge about utilization of DHIS (95% CI: [43, 55.3]).
The attitudes of healthcare providers was also assessed. Among 264 of respondents approached, 149 (56.4%) of the respondents had favourable attitudes towards the use of DHIS (95% CI: [53.2, 59.8]).
Factors associated with knowledge and attitudes to use district health information system
Variables that were significant at P value of 0.2 and less than 0.2 in the bi variable analysis were considered and nine (9) variables were entered in to multivariable analysis. Of the nine (9) variables, five (5) variables were significantly associated with attitudes to use DHIS at P value of less than 0.05. When considering knowledge of healthcare providers, four (4) variables were significantly associated with knowledge to use DHIS.
Univariable and multivariable logistic regression factors associated with knowledge to use DHIS among PMT members at health facility in Ilu Aba Bora zone, Oromia region, south west of Ethiopia 2020.
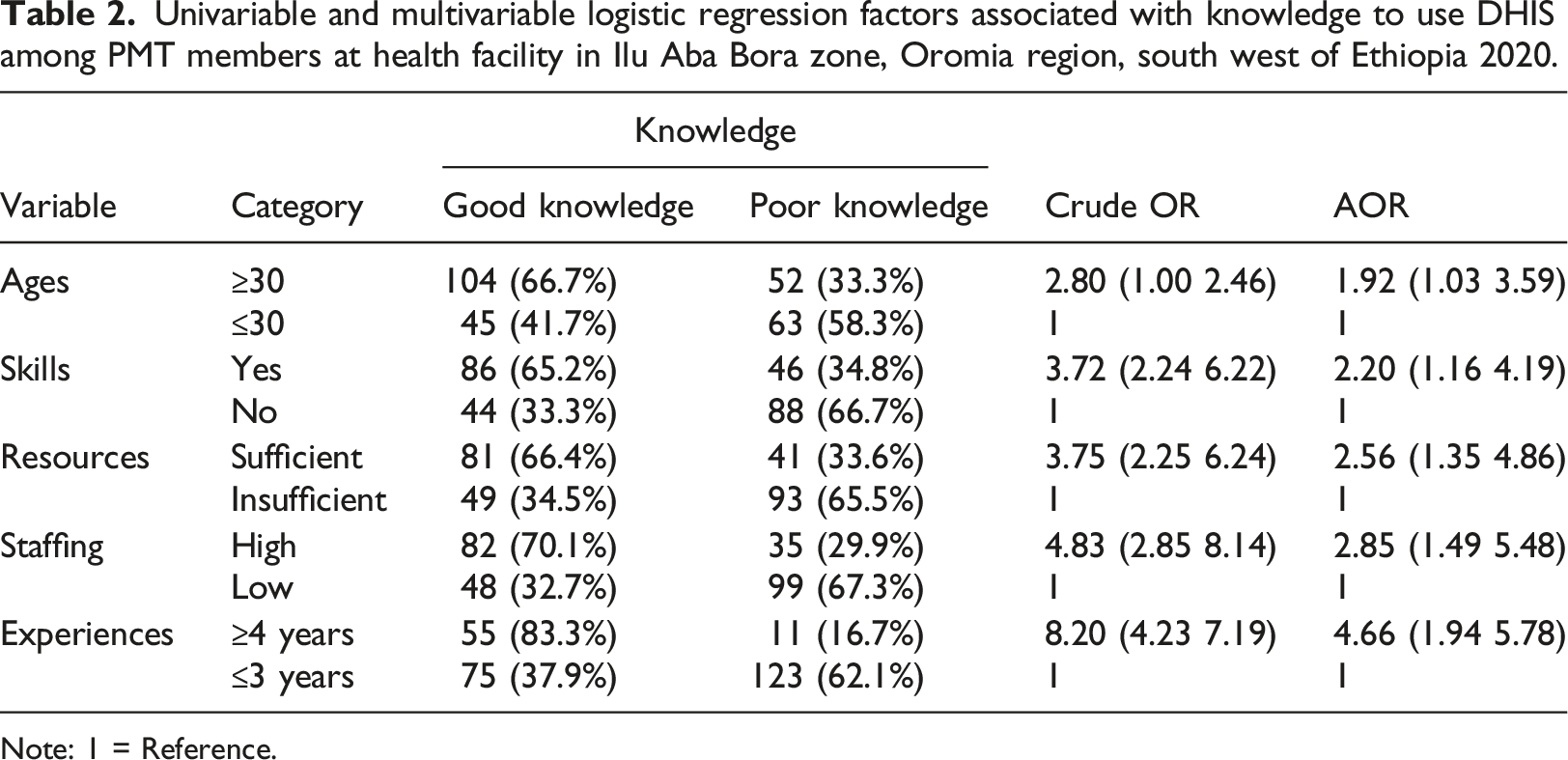
Note: 1 = Reference.
Univariable and multivariable logistic regression factors associated with attitudes to use DHIS among healthcare providers at health facilities in Ilu Aba Bora zone, Oromia region, South West of Ethiopia 2020.
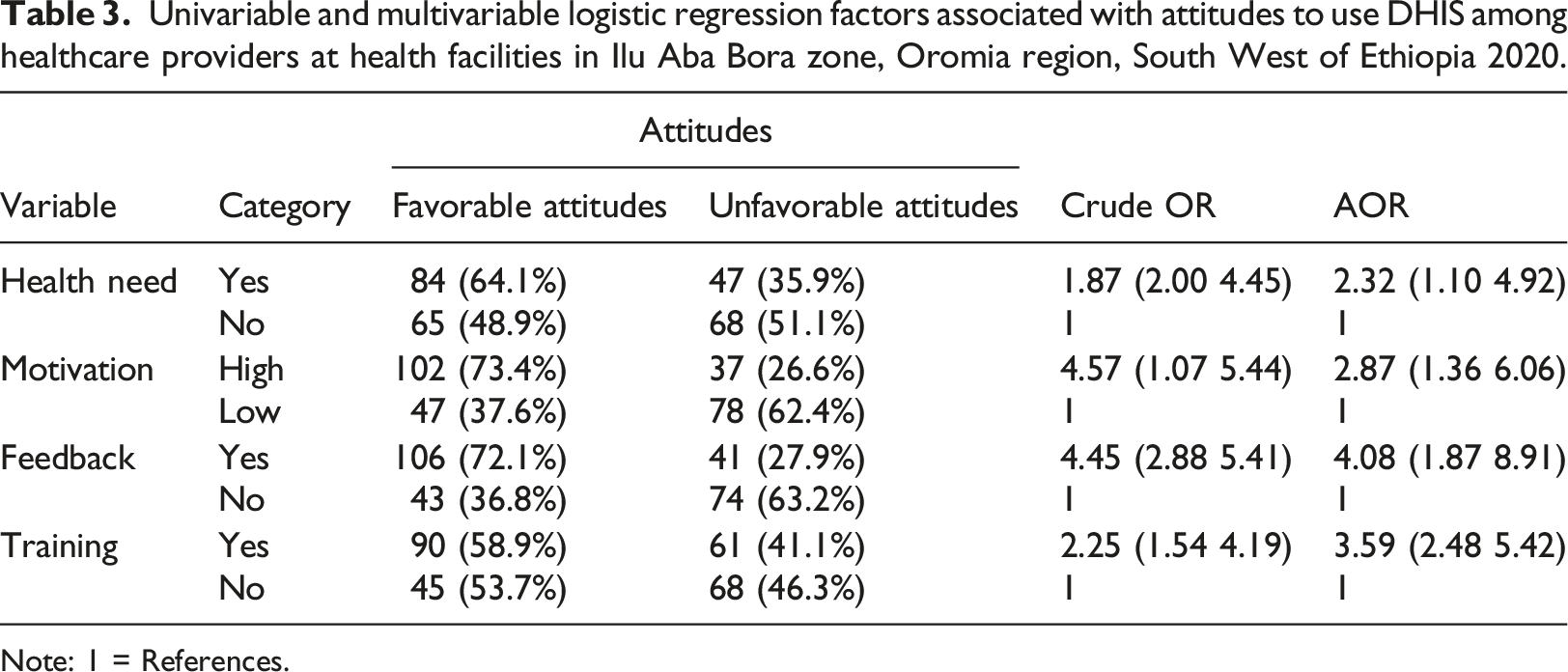
Note: 1 = References.
Discussion
The discussion of this study precede with a summary of some assessment studies that have been conducted on the knowledge and attitudes to use DHIS in south west of Ethiopia. To cope with purpose of the study, a cross sectional study was conducted among healthcare providers. Data was collected from different health institutions and facilities including referral hospital, health centers and primary hospital in Ethiopia to assess the knowledge and attitudes towards utilization of DHIS. To promote the utilization of DHIS in health facilities, it is essential to determine and focus the healthcare providers’ knowledge and attitude in using of DHIS.4,24,35,36 Thus skills, resources, staffing, ages, and experiences were factors statistically associated with knowledge to use DHIS. Also the variables health needs, motivation, feedback and training were associated factors that determines the attitudes of health professionals towards the use of DHIS.
Taking into account the studies on healthcare providers’ knowledge and attitude towards the use of DHIS is the most important to identify gaps and provision of evidence to provide quality health service. 37 In this study, about 128 (49.2%) of respondents have good knowledge about utilization of DHIS(95% CI: [43, 55.3]) which was lower than the study conducted in Kenya. 38 The result of this study was also inconsistent with the study conducted in Kuwait 39 though consistent with the study conducted in South Africa. 36 But the result of this study was greater than the study conducted in Liberia. 40 The attitudes of healthcare providers in this study was also assessed where 56.4% (95% CI: [53.2, 59.8]) of respondents have favourable attitudes towards use of DHIS, which is less than study conducted in Kuwait. 39 The study conducted in Isfahan hospitals was also greater than the result of this study. 4 This might be due to the fact that the infrastructure in Isfahan is more advanced than that of in Ethiopia. But this result was greater than the study conducted in India where the attitudes of health professionals to use EHealth was 39%. 41 The cross sectional study conducted in Uganda also identified that majority of healthcare professionals had positive attitudes towards health Information systems attributes where the level of skills and ICT use among healthcare providers are the factors that could determine their attitudes to use health Information systems. 42
The current study revealed that the knowledge of healthcare providers could be affected by skills related to utilization of DHIS. The result is similar to the study conducted in Kuwaiti hospitals. 43 But the result was inconsistent with the study conducted in Uganda. 44 This might be due to the fact that skills of healthcare providers could be over a period of time. The study also identified that respondents with longer experiences were 4.66 times [AOR = 4.66, 95% CI: (1.94, 5.78)] more likely to have good knowledge of DHIS utilization. This study supports the study which was conducted in Kuwaiti hospitals [43]. This study has shown that respondents with available resources were 2.56 times [AOR = 2.56, 95% CI: (1.35, 4.86)] more likely to have a good knowledge towards the use of DHIS their clinical purposes. This result was in lined with the study conducted in Ghana. 45
The study revealed that having adequate staffing will helps respondents to have good knowledge of DHIS utilization [AOR = 2.85, 95% CI: (1.49, 5.48)]. The study conducted in Ghana supports this result which stated that utilization of DHIS was affected by adequacy of staffing. 45 The result was in line with the study conducted in Kenya, performance of routine health information was affected by adequacy of staff. 46 The finding of this study has shown that respondents with adequate training has more favourable attitudes 3.59 times [AOR = 3.59, 95% CI: (2.48, 5.42)] towards the utilization of DHIS when compared to respondents who has inadequate training about DHIS use. This study was similar to the study conducted in Walden University. 47 But as the study conducted in Ghana, training do not determine the attitudes of health professionals towards the utilization of health information. 48 The possible explanation will be goes to explanation that the extent of study participants will be the determinant reason for this variations. The result of this study is in line with study conducted in Kuwaiti hospitals provided that previous experience in computer use, computer skills and training were the most determinant factors that will be associated with attitudes of healthcare providers to use DHIS. 49
As this study shows, having culture of receiving and giving feedback on their utilization of DHIS were 4.08 times [AOR = 4.08, 95% CI: (1.87, 8.91)] more likely to have favourable attitudes to use DHIS, which was similar to the study conducted in Walden University. 47 As the study, 46 utilization of health Information could be determined by feedback services that will be obtained from/within the facility. But the result of this study was inconsistent with study conducted in Ghana identified that provision of feedback do not have any significant association with attitudes to use health information. 48
In this study, age was found to be the factors associated with knowledge of healthcare providers towards the use of DHIS. The study participants of an age thirty (30) and above were 1.92 times more likely to have a good knowledge to use DHIS when compared to respondents of an ages of less than thirty [AOR = 1.92, 95% CI: (1.03, 3.59)]. But the study conducted in Ghana was not in lined with the result of this study which revealed that age has no any significant association with knowledge towards the utilization of DHIS. 48 This result was consistent with the study conducted in Australia. 50 The Motivation to use DHIS can also influence attitudes of healthcare providers. Respondents with high motivations were 2.87 times more likely to have favourable attitudes towards the use of DHIS when compared to respondents with low motivations [AOR = 2.87, 95% CI: (1.36, 6.06)]. The study conducted in Australia was line with this result. 50 The study 46 revealed that motivation to use routine health data determines the utilization of health information among healthcare providers. The results also revealed that health needs favours the attitudes of study participants. The study participants those who need DHIS for health purpose were 2.32 times more likely to have favourable attitudes towards the utilization of DHIS [AOR = 2.32, 95% CI: (1.10, 4.92)]. This result was supported by these studies.4,35,36
Conclusion
In general, about 49.2% of health professionals have good knowledge on utilization of DHIS. Factors associated with knowledge to use DHIS were sufficient skills, availability of resources, ages, sufficient staffing, and longer experiences. Whereas about 56.4% of the respondents had favourable attitudes towards the use of DHIS. The variables health needs, high motivation, provision of feedback and sufficient training were the determinant factors that were associated with the attitudes of health professionals towards the use of DHIS. This study has found significant factors that determine the knowledge and attitudes of health professionals to the use of DHIS. An attempt to providing sufficient training, adequate resources, skills related to DHIS use, promotion of motivation and feedback will help to improve and achieve the expected knowledge and favourable attitudes towards the use of DHIS for betterment of quality health services.
Limitation of the study
The limitation of this study was explained as follows. • The study did not include data on practice • This study didn’t include every healthcare providers but was restricted to only selected healthcare providers. • The sample size was so small due to the nature of study participants
Footnotes
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically important intellectual content; gave final approval of the version to be published; and agreed to be accountable all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study protocol was reviewed and approved by the ethical review board of University of Gondar with Ref .No /IPH/837/6/12 and Informed consent was obtained from each study participant. Permission letter also obtained from each Health facilities. Names of participants and other personal identifiers were not included in the data collection tool.
Data availability
The datasets generated and/or analysed during the current study will be available upon reasonable request from the corresponding author.