
Abstract
Introduction
Telehealth offers a promising route to expand access to care in low-resource settings such as Somalia, but community readiness remains poorly characterized. This study assessed knowledge, perceived benefits and concerns, and predisposition to use telehealth among adults in Mogadishu.
Methods
We conducted a 6-month cross-sectional survey in Mogadishu (December 2024 to May 2025) using convenience sampling in community settings and online. A forward–backward translated questionnaire captured sociodemographic data and four composite scores. Nonparametric tests compared median scores across groups, and Spearman's rank correlations assessed associations among outcomes.
Results
We analyzed 423 eligible responses. Scores indicated moderate knowledge and perceived benefits, consistently high concerns, and modest predisposition to use telehealth. Knowledge was higher among participants with university education, employment, and better self-rated health, and showed a very weak inverse association with predisposition. Previous telehealth users reported higher perceived benefits, which increased with intention to use telehealth. Predisposition was higher among unemployed participants and those with previous telehealth use. Perceived concerns were high across all subgroups. Knowledge showed a very weak positive association with concerns, while perceived benefits were positively associated with both concerns and predisposition, with small effect sizes.
Conclusion
Mogadishu residents had moderate knowledge and interest in telehealth but persistent concerns about reliability, quality, and data privacy. Education, employment, and prior exposure shaped attitudes, yet greater knowledge did not necessarily increase adoption. Targeted digital literacy, user-centred pilot programmes, and clear safety and privacy regulations are needed to realise the promise of telehealth in Somalia.
Introduction
Telehealth, a rapidly evolving field in healthcare delivery, has emerged as a transformative solution for addressing the challenges of accessibility, quality, and efficiency in healthcare systems worldwide. 1 Defined as the provision of healthcare services and information via remote technologies, telehealth encompasses a wide range of applications including telediagnosis, telemonitoring, teletriage, teleintervention, and remote patient monitoring. 2 The advent of advanced information and communication technologies has been instrumental in driving this shift toward telehealth, offering unprecedented opportunities to expand healthcare coverage and improve patient outcomes. 3 By complementing traditional in-person visits, particularly for follow-ups, routine check-ins, and minor issues, telehealth ensures that patients seek in-person care only when necessary, thereby optimizing healthcare resource utilization. 4
The global expansion of telehealth has been particularly pronounced in rural and remote settings, where access to healthcare services has historically been limited.5,6 For instance, in Australia, telehealth services have been effectively employed to bridge the healthcare gap between urban and rural areas, improving access to specialized care for remote populations. 5 Similarly, African countries, such as Kenya, Tanzania, and Uganda, have leveraged telehealth to overcome geographical barriers and resource constraints, highlighting the potential of these technologies in resource-limited settings.7,8 In Somalia, healthcare system faces numerous challenges that significantly impede the delivery of quality care to the population. Characterized as one of the poorest healthcare systems globally,9,10 Somalia struggles with limited availability of essential services, a fragmented infrastructure, and a critical shortage of resources and skilled healthcare professionals. 11 Years of conflict and instability have exacerbated these issues, leading to heavy reliance on external aid and private providers. 12
The country's healthcare facilities often lack proper equipment and staff, struggling to meet the needs of patients, particularly in emergency situations.12,13 Consequently, Somalia faces alarmingly high rates of infant and maternal mortality, malnutrition, and infectious diseases, placing it among the countries with the lowest health outcomes worldwide.14–16 Considering these challenges, digital and telehealth have emerged as promising solutions to address some of the critical issues plaguing Somalia's healthcare system.17,18 Digital health, encompassing a broad range of technologies, including telehealth, mobile health, and electronic health records, offers the potential to significantly improve healthcare access, quality, and efficiency in Somalia.17,19
The growing Internet and telecommunications infrastructure in the country provides a foundation for the implementation of these technologies. 20 This increased access to information and communication channels has the potential to greatly benefit healthcare practitioners and improve overall healthcare conditions within the country. However, the successful implementation and acceptance of telehealth in Somalia centers on understanding community perspectives and the factors influencing its adoption. Factors such as knowledge, perceived benefits, concerns, and predisposition toward telehealth play crucial roles in determining the uptake and effectiveness of these services. 21
Despite its potential benefits, there is a notable lack of studies investigating these factors in the Somali population. This gap in research underscores the need for a thorough evaluation of community readiness and attitudes toward telehealth services. By providing a comprehensive analysis of the knowledge, perceived benefits, concerns, and predisposition toward telehealth among Somalis, this study aims to lay the groundwork for evidence-based strategies to integrate telehealth into Somalia's healthcare system. The findings will not only contribute to the growing body of literature on telehealth in developing countries but also offer practical insights for healthcare providers, policymakers, and technology developers working toward improving healthcare access and quality in Somalia through innovative digital solutions.
Methods and materials
Study design and setting
We conducted a 6-month cross-sectional survey in Mogadishu, Somalia, December 2024–May 2025, to evaluate adults’ knowledge of telehealth, perceived benefits and concerns, and willingness to use such services. Mogadishu was selected because connectivity, provider availability, and security conditions enable mixed-mode data collection. Rural and remote districts were not sampled during the study. This urban focus circumscribes external validity and likely reflects an upper-bound view of readiness in the connected areas. The overall design followed the framework developed by Kabir et al. for similar low-resource contexts, 21 with minor adaptations to ensure cultural relevance for Somali respondents.
Participant recruitment
Because insecurity and limited infrastructure make probability sampling impractical, we opted for convenience sampling. Adults meeting three criteria—Somali nationality, residence in Mogadishu, and age of at least 18 years—were invited via two modes: (i) in-person intercept recruitment at community venues and (ii) online recruitment through Facebook, WhatsApp, Telegram, and LinkedIn. Responses from individuals outside Mogadishu or those with incomplete questionnaires were excluded from the analysis. Because the denominator of the contacted or eligible individuals was unknown across channels, a conventional response rate could not be calculated.
Questionnaire development and data collection
The survey instrument was a semistructured questionnaire derived from Kabir et al. 21 After forward and backward translation from English to Somali, we pilot-tested the Somali version with 30 adults to verify its clarity and cultural suitability, which prompted minor revisions. Internal consistency of the multi-item scales in the Somali version was acceptable (Cronbach's α = 0.76). Content covered demographics, prior telehealth service utilization, perceived health status, four outcome domains (knowledge, perceived benefits, perceived concerns, and predisposition), and a single intention item. Items used brief factual prompts and 3- or 5-point Likert responses, with scoring detailed in the Variables and measurements section. Surveys were administered on paper for in-person recruitment and via Google Forms online, with anonymous responses and exclusion of records with missing primary outcomes. The full English and Somali questionnaires are provided as Supplemental file (S1).
Sample size calculation
The sample size was determined using Cochran's formula.
22
The formula used to calculate the sample size is as follows:

Initially, a sample size of 384 participants was used. A total of 423 participants were recruited, accounting for 10% of potential nonresponses.
Variables and measurements
The four composite outcomes were calculated. Knowledge comprised of five items scored from 1 to 3 (total: 5–15). Perceived benefits were assessed using three Likert items scored from 1 to 5 (total: 3–15). Perceived concerns relied on one Likert item scored from 1 to 5. Predisposition to use telehealth services was assessed using two Likert items scored from 1 to 5 (total 2–10). Intention to use telehealth services was captured with a single item (“plan to utilize”; No/Maybe/Yes) and analyzed as a separate categorical predictor. Median splits classified each outcome as “higher” or “lower.” The predictor variables included age, sex, marital status, education, employment, district of residence, prior telehealth service utilization, and perceived health status. Perceived health status used the World Health Organization single item with five options (very good, good, fair, bad, and very bad), and analyzed and reported the categories for both descriptive and inferential comparisons.
Data analysis
Data were analyzed in Stata version 17. Descriptive statistics summarized the data. Normality was assessed using the Shapiro–Wilk test and histogram inspection; because outcome distributions were nonnormal, we used Mann–Whitney U tests for two-group comparisons and Kruskal–Wallis tests for comparisons involving three or more groups. Associations among continuous composite scores were examined using Spearman's rank correlation; coefficients are reported as ρ (rho; equivalent notation rs). Coefficients near zero are described as very weak, and interpretation emphasizes direction, statistical significance, and practical relevance. Kruskal–Wallis tests used the five-category perceived health status variable. Statistical significance was defined as two-tailed p < 0.05.
Results
Participant characteristics
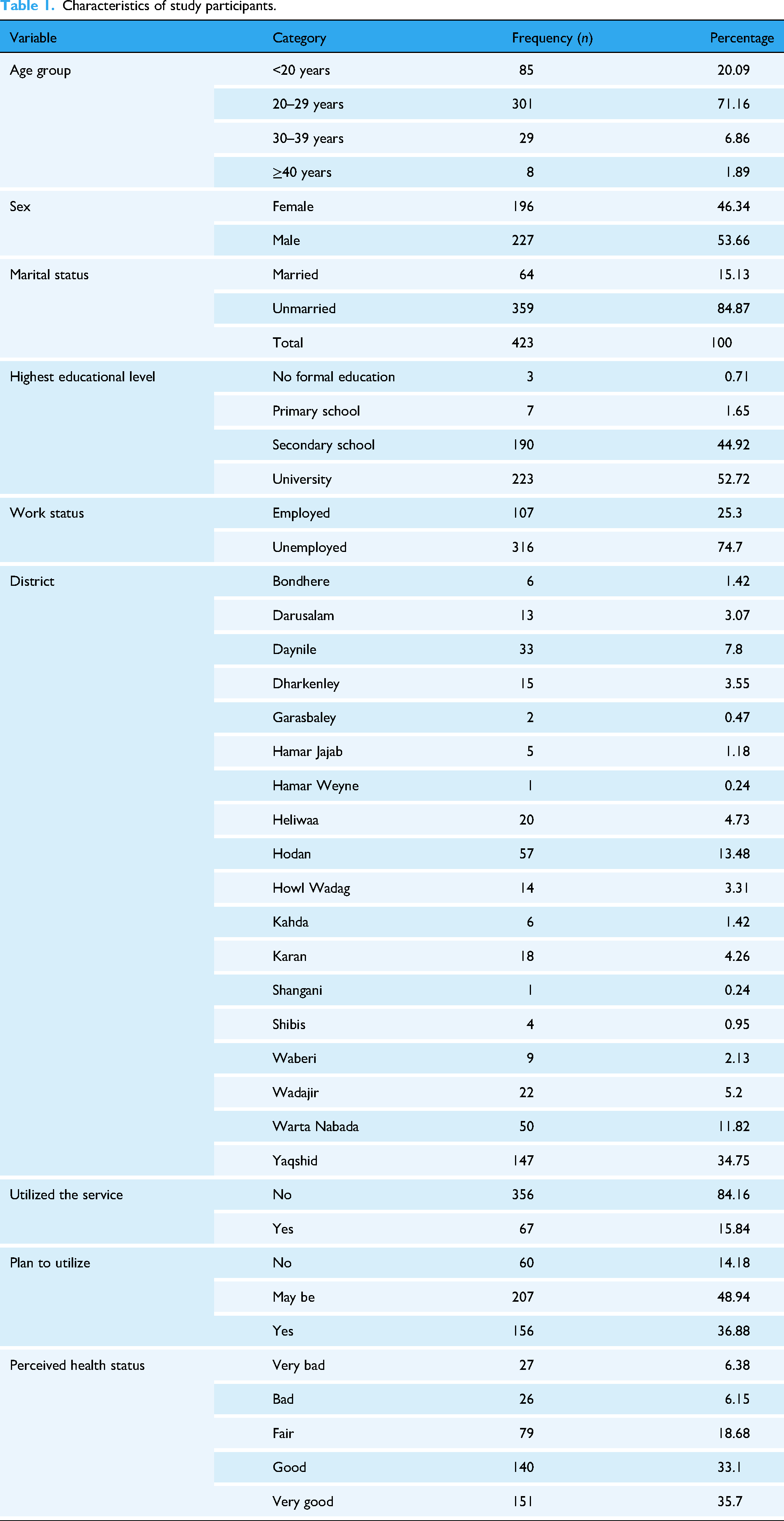
In total, 423 participants completed the survey. Most participants were aged 20–29 years (71.2%), followed by those aged <20 years (20.1%), 30–39 years (6.9%), and ≥40 years (1.9%). More than half of the participants were male (53.7%) and the remainder were female (46.3%). Most were unmarried (84.9%) or unemployed (74.7). Educational attainment was high, with 52.7% having a university-level education and 44.9% having completed secondary school. Regarding telehealth exposure, 15.8% of participants reported previous use of telehealth services. A total of 36.9% expressed intention to use telehealth in the future, 48.9% were unsure, and 14.2% did not plan to use it. Perceived health status was predominantly positive, with 35.7% rating their health as “very good” and 33.1% as “good.” Participants were drawn from multiple districts in Mogadishu, with the largest proportion from Yaqshid (34.8%), followed by Hodan (13.5%) and Warta Nabada (11.8%) (Table 1).
Characteristics of study participants.
Distribution of composite scores for the outcome variables
Composite scores were calculated for the four primary outcome variables based on predefined scoring frameworks. The knowledge score, ranging from 5 to 15, had a mean of 9.16 (SD = 2.54) and median of 10 (interquartile range [IQR]: 7–12). The perceived benefit score, ranging from 3 to 15, had a mean of 7.83 (SD = 2.79) and a median of 8 (IQR: 6–9). Perceived concern, measured on a 1–5 scale, had a mean of 3.43 (SD = 1.36) and a median of 3 (IQR: 3–5). The predisposition score, with a possible range of 2–10, had a mean of 5.00 (SD = 2.17) and a median of 5 (IQR: 3–6) (Table 2).
Distribution of the scores of knowledge, perceived benefits, perceived concerns, and predisposition to use telehealth services.

Knowledge of telehealth by study variables
Knowledge scores varied significantly according to the demographic and behavioral factors. Higher scores were observed among participants aged 30–39 years compared to other age groups (p = 0.03) and among those with higher educational levels (p = 0.02). Employed participants had significantly higher knowledge scores than did unemployed participants (mean = 9.63 vs. 9.00; p = 0.02). The differences in the knowledge scores across districts were statistically significant (p = 0.05). Participants who reported an intention to use telehealth had higher knowledge scores than those who did not (p = 0.03). Significant differences were also observed according to the perceived health status, with lower knowledge scores among those reporting “very bad” health (p < 0.001) (Table 3).
Distribution of study variables by knowledge of telehealth.

Note. For two-category variables, p-values are from the Mann–Whitney U test (reported as z). For three or more categories, p-values were obtained using the Kruskal–Wallis test (reported as χ2).
Significance: *p < 0.05.
Perceived benefits of telehealth by study variables
The perceived benefit scores did not vary significantly according to age, sex, education level, marital status, or employment status. A statistically significant difference was observed based on previous telehealth use, with users reporting higher perceived benefit scores than nonusers (mean = 8.55 vs. 7.69; p = 0.032). Perceived benefits also increased across intention to use telehealth. No significant differences in perceived benefits were found across perceived health status (Table 4).
Distribution of study variables by perceived benefit of telehealth.

Note. For two-category variables, p-values are from the Mann–Whitney U test (reported as z). For three or more categories, p-values were obtained using the Kruskal–Wallis test (reported as χ2).
Significance: *p < 0.05.
Perceived concerns of telehealth by study variables
Perceived concern scores did not differ significantly by age, sex, education level, marital status, employment status, previous telehealth use, or intention to use it. Differences across districts and perceived health status categories were not statistically significant (Table 5).
Distribution of study variables by perceived concerns of telehealth.
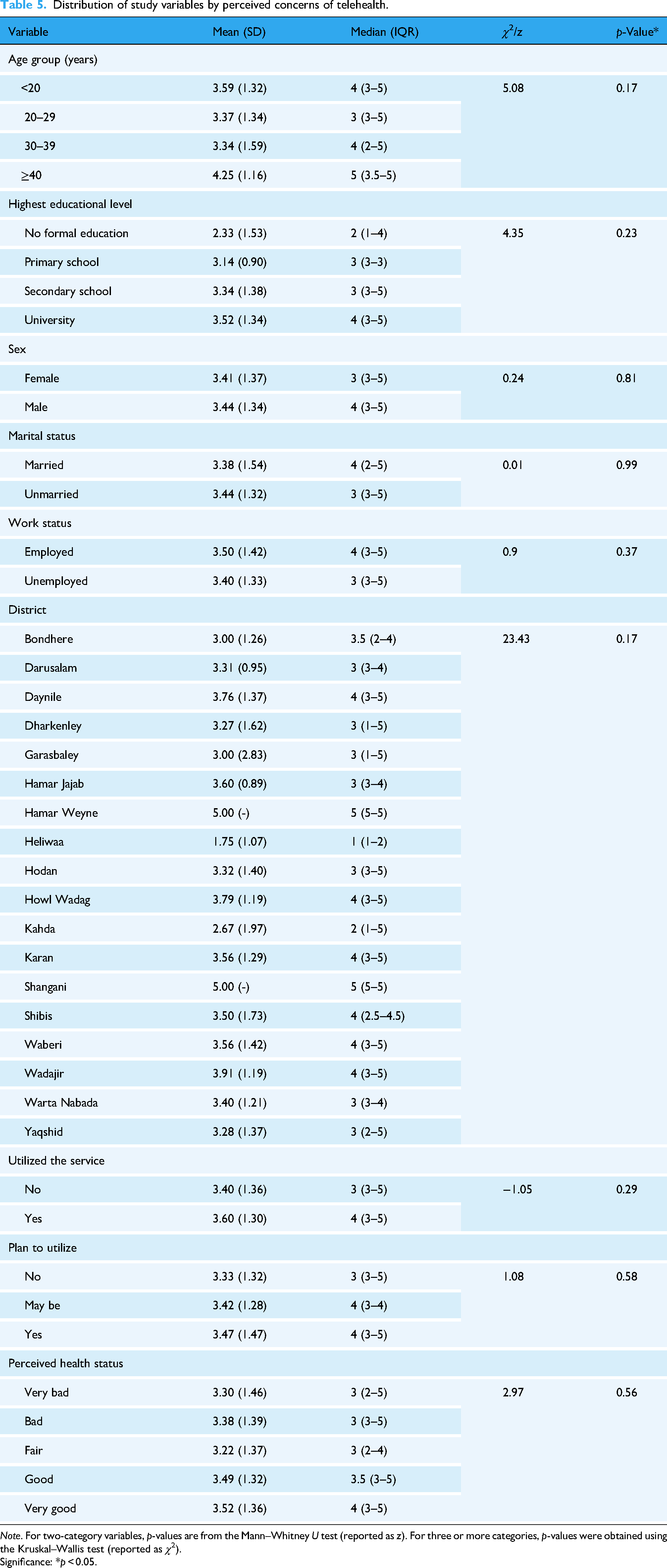
Note. For two-category variables, p-values are from the Mann–Whitney U test (reported as z). For three or more categories, p-values were obtained using the Kruskal–Wallis test (reported as χ2).
Significance: *p < 0.05.
Predisposition to use telehealth by study variables
Predisposition scores were significantly higher among the unemployed participants than among the employed participants (mean = 5.13 vs. 4.59; p = 0.03). Participants who had previously used telehealth services reported higher predisposition scores than those who had not (mean = 5.61 vs. 4.88; p = 0.02). No significant differences in predisposition were observed according to age, sex, marital status, education level, intention to use telehealth services, or perceived health status (Table 6).
Distribution of study variables by predisposition of telehealth.

Note. For two-category variables, p-values are from the Mann–Whitney U test (reported as z). For three or more categories, p-values were obtained using the Kruskal–Wallis test (reported as χ2).
Significance: *p < 0.05.
Correlation matrix between key study variables
Spearman's rank correlation analysis was conducted to assess associations among the four outcome variables (Table 7). Knowledge showed a very weak positive correlation with perceived concerns (ρ = 0.099, p < 0.05) and a very weak inverse correlation with predisposition (ρ = −0.111, p < 0.05). Perceived benefits were positively correlated with perceived concerns (ρ = 0.128, p < 0.05) and predispositions (ρ = 0.317, p < 0.05). No significant correlation was observed between knowledge and perceived benefits (ρ = 0.005, p > 0.05). These effect sizes are small; therefore, the findings should be interpreted as limited in magnitude, despite their statistical significance.
Spearman's rank correlation coefficient matrix.

*Values are Spearman ρ. *p < 0.05.
Discussion
This study is one of the first to map how adults in Mogadishu understand value, fear, and intention to use telehealth services. Four findings were obtained in the present study. First, overall knowledge and interest in telehealth were moderate, but both varied according to socioeconomic status. Second, prior experience was a powerful driver of positive attitudes; however, concerns about reliability and data security remained high across all the groups. Third, knowledge was inversely related to the willingness to adopt, suggesting that better-informed individuals may be more alert to system weaknesses. Finally, readiness to use telehealth was highest among the unemployed, a pattern that underscores technology's perceived affordability. Participants with university education, formal employment, and good perceived health status scored the highest in terms of telehealth knowledge. Similar education- and income-linked gradients have been reported across several low- and middle-income countries (LMIC) settings, confirming that digital health literacy is closely associated with social advantage.23,24
Conversely, respondents in very poor health showed the lowest knowledge levels, echoing studies on the “digital divide,” where poor health frequently coexists with reduced access to reliable information and technology.25,26 These gaps highlight the need for inclusive digital literacy strategies that reach individuals who would benefit the most from remote care but know the least about it. Contrary to the common assumption that knowledge automatically drives uptake, we observed a weak but significant negative correlation between knowledge and predisposition to telehealth service use. In other words, the better-informed participants were slightly less willing to use remote care. Prior work suggests that people who understand telehealth also recognize its shortcomings, including unstable connectivity, uncertain clinical quality, and weak data protection.27–29
Therefore, public education campaigns need to focus on increasing awareness while transparently addressing legitimate concerns. Prior users consistently rated the benefits of telehealth higher than nonusers, supporting the technology acceptance model, which posits that perceived usefulness shapes behavioral intention.30–33 However, perceived concerns were also high and did not vary according to the demographic characteristics. Concerns about impersonality, diagnostic accuracy, and data privacy mirror reports from Kenya, Ghana, and Ethiopia, where telehealth regulation and quality assurance remain limited. 21 34–37 The positive correlation between perceived benefits and concerns suggests the coexistence of appreciation and apprehension. Therefore, effective programs must balance promotional messages with demonstrable safeguards.
Unemployed respondents showed greater willingness to adopt telehealth than those in paid work, probably because remote consultations reduce indirect costs, such as transport and time away from informal jobs. Prior experience was another decisive factor: participants who had already used telehealth were far more likely to use it again, implying that low-risk demonstration projects or free pilot sessions could spur wider uptake.38–41 These patterns suggest that scaling telehealth in Somalia will require more than just technical deployment. First, inclusive digital literacy initiatives must reach groups with limited education or poor health through community media and trusted messengers who can explain their advantages and safeguards. In Ethiopia, maternal health information delivered by respected local agents achieved the strongest results when communication channels were tailored to the context. 42 Second, embedding telehealth pilots inside primary care centers will allow patients to experience the service first-hand and provide providers space to refine their workflows; a district hospital program in Mali dramatically expanded access to remote communities. 43 Third, a comprehensive regulatory framework that clarifies service quality, provider accountability, and data protection standards is essential to build public trust and sustain momentum.
Limitations
This study had several limitations that affected its interpretation and generalizability. First, we used convenience sampling through in-person and online recruitment, and the denominator of contacted or eligible individuals was unknown; therefore, a conventional response rate could not be calculated. Second, the data were collected only in Mogadishu, an urban setting with relatively better connectivity, which means that rural and remote communities were not represented. This reflects an urban perspective and may not extend to settings that often focus on successful telehealth initiatives. Third, the sample was predominantly young and relatively well-educated, which likely overrepresented digitally connected groups and underrepresented older adults and those with lower digital access.
Fourth, outcomes and predictors, such as utilized the service, plan to utilize, and perceived health status, were self-reported, which introduces potential recall and social desirability bias. Fifth, although the questionnaire underwent forward and backward translation and piloting and showed acceptable internal consistency in the Somali version, we did not assess test–retest reliability or external validity, and the single item used for perceived health status may be prone to residual misclassification despite standardized category labels. Sixth, its cross-sectional design precludes causal inferences. Finally, several subgroup cells were small, and some between-group differences and correlations, although statistically significant, were of small magnitude; therefore, practical significance should be interpreted with caution.
Conclusion
This survey provides one of the first systematic portraits of how urban Somalis perceive and intend to use telehealth services. Overall, knowledge and perceived benefits were modest, while apprehension about privacy, diagnostic accuracy, and service reliability remained high. Socioeconomic factors mattered: university education, employment, and good perceived health status predicted higher knowledge, whereas unemployment and previous experience predicted greater willingness to adopt telehealth. Crucially, the very weak negative association between knowledge and predisposition suggests that awareness campaigns must tackle legitimate concerns and not merely promote advantages. Policymakers and program leaders have the following three priorities: first, inclusive digital literacy strategies should reach groups with limited education or poor health using community media in Somali to explain both benefits and safeguards. Second, embedding low-cost pilot services within primary care facilities will provide patients and providers with hands-on familiarity, demonstrating value while refining workflows. Third, a clear regulatory framework that sets service quality benchmarks, secures patient data, and clarifies provider accountability is vital for sustaining public trust. The findings should be interpreted considering several limitations, including convenience sampling, reliance on self-reported measures, and the cross-sectional design, which precludes causal inferences from being made. Future nationally representative longitudinal studies augmented by qualitative work exploring contextual barriers, such as bandwidth and language, are warranted to track how attitudes evolve as Somalia's digital infrastructure matures. When combined with regulatory reform and targeted capacity building, telehealth could become a practical tool for mitigating persistent gaps in access to quality healthcare in Somalia.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251406298 - Supplemental material for Knowledge, perceived benefits, perceived concerns, and predisposition to use telehealth services in Mogadishu, Somalia: A cross-sectional survey
Supplemental material, sj-docx-1-dhj-10.1177_20552076251406298 for Knowledge, perceived benefits, perceived concerns, and predisposition to use telehealth services in Mogadishu, Somalia: A cross-sectional survey by Mohamed Mustaf Ahmed, Zhinya Kawa Othman, Jamilu Sani, Ahmed Adam Mohamed, Amal Naleye Ali, Abdinasir Mohamed Aray, Mohamed Yusuf Mohamed, Mulki Mukhtar Hassan, Olalekan John Okesanya, Don Eliseo Lucero-Prisno and Najib Isse Dirie in DIGITAL HEALTH
Footnotes
Ethical approval and consent to participate
Ethical approval for this study was granted by the Ethical Review Board of the National Institute of Health (NIH)—Somalia (reference NIH/IRB/44/NOV/2024; letter dated November 5, 2024). All procedures adhered to the ethical standards of the committee and to the principles of the 1964 Declaration of Helsinki and its later amendments. Written informed consent was obtained from all participants prior to any data collection. For in-person respondents, consent was documented on a paper form; for online respondents, consent was documented electronically within the form. Participation was voluntary and anonymous, and no personal identifiers were collected. The Ethics Board reviewed and approved these consent procedures.
Author contributions
MMA conceptualized this idea. The study design was developed collaboratively by MMA, AAM, and ANA. Material preparation and data collection were performed by AMA, MMH, and MYM. MMA and JS analyzed and interpreted the data. The initial draft was composed of MMA and JS. OJO, ZKO, and NID critically revised the manuscript for important intellectual content. DEL-P III supervised the study. All authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.