
Abstract
The new adoption of healthcare information technology is costly, and effects on healthcare performance can be questionable. This nationwide study in China investigated the efficient performance of healthcare information technology and examined its spatial correlation. Panel data were extracted from the Annual Investigation Report on Hospital Information in China and the China Health Statistics Yearbook for 2007 through 2015 (279 observations). Stochastic frontier analysis was employed to estimate the technical efficiency of healthcare information technology performance and related factors at the regional level. Healthcare information technology performance was positively associated with electronic medical records, total input, and cost of inpatient stay, while picture archiving and communication systems and net assets were negatively related. Local Indicators of Spatial Association showed that there existed significant spatial autocorrelation. Governmental policies would best make distinctions among different forms of healthcare information technology, especially between electronic medical records and picture archiving and communication systems. Policies should be formulated to improve healthcare information technology adoption and reduce regional differences.
Keywords
Introduction
The adoption of healthcare information technology (HIT) by governments should enable better coordination of healthcare services, help control medical costs, and improve quality of care.1,2 In 2009 in the United States, the Health Information Technology for Economic and Clinical Health Act was passed and funded with $27 billion. 3 In China, the Twelfth Five-Year Plan for social and economic developments pledged an estimated investment in HIT of ¥6 billion for 2007, increasing to ¥33.4 billion in 2015. 4
The implementation of HIT, including electronic medical records (EMRs), is costly, and its practical value has come into question. Several studies have reported that HIT has had positive effects on bed utilization rate, 5 operating costs per bed,1,3 and hospital revenues. 6 However, many HIT systems have failed to meet clinical needs or have had adverse organizational effects, 7 while adding to the hospitals’ financial burden. 8 Studies of the benefits of implementation of HIT have rarely considered the differences in sophistication of technology across local regions and among provinces. 9 In the United States, regional differences in the adoption of an EMR system have been problematic, 10 where underserved areas are especially affected by less access to technology. 11
Shu et al. 12 investigated EMR adoption in 848 tertiary hospitals in China, and found that most hospitals have only basic systems. To control the rapid growth of medical expenditure and to improve quality of healthcare, China has set a goal to implement HIT uniformly throughout the nation by the end of 2020. 13 Although HIT has been heavily invested, it is not clear that these goals can be achieved, and studies have been insufficient. In addition, some reviews on HIT performance have reported mixed results, leaving unanswered questions.14,15 This study evaluated the efficiency of HIT on healthcare performance in China, and its spatial correlations.
Literature review
Recent years have witnessed the rapid adoption of HIT, and the value of HIT inputs has become a great concern. 16 Specifically, HIT is information technology applied in the field of healthcare to manage and use healthcare information. 17 HIT is designed to improve the efficiency of communication among providers 18 and between hospital and patient. 19
However, only a few studies have investigated an association between HIT investment and hospital performance, and reports have varied. Li and Collier 20 used a structural equation model to evaluate the survey data of 142 community hospitals, and found that HIT improved clinical quality and hospital financial performance. Wang et al. 5 developed a theoretical model to analyze financial data from 2011 to 2016, and also reported a positive association between IT investment and financial performance.
Yet, Ginn et al. 21 adopted cross-sectional data from the 2007 American Hospital Association (AHA) electronic health record implementation survey, and with a general linear mixed model found a negative association between HIT adoption and financial performance. A recent review of HIT adoption on medical outcome performance reported that 19 percent (12/37) of the studies found no statistical difference in outcomes. 22 These contradictions may be due to limitations of the studies, such as considering only a single technology, 23 short-term evaluation, 21 or different outcome measures. 24 In addition, because the informatics industry changes so rapidly, study reports may quickly become outdated and therefore unreliable.
A review of the literature offers several insights into the study of HIT and its potential improvement and usefulness. First noted is that the data used in many HIT studies have been cross-sectional, and on a small scale,6,25,26 which may lead to deviations in estimates. A recent systematic review of HIT adoption studies reported that only 27 (11%) of 236 used a time-series design. 14
Second, the importance of differences in demographic and socioeconomic factors, even among small adjacent geographic areas as revealed by spatial unit analysis, has been underestimated in health studies. 27 Kawaguchi et al. 28 found that EMR adoption in Japan generally increased from 2008 to 2014, but only in clinics, and among many factors considered was positively associated consistently only by average income; other geographic differences did not improve. The authors concluded that adoption of EMRs required financial and technical support, specific to the spatial unit and facility.
A third insight was offered by Angst et al. 29 who classified HIT systems as either clinical or administrative, because patient and administrative data are different data streams. According to our review of the literature, evaluations of HIT performance have rarely differentiated between clinical and administrative HIT, whether conducted at the in-hospital, regional, or national levels. Clinical HIT systems are designed to improve patient care, and primarily deal with the collection, testing, and processing of patient data for medical purposes or treating patients, 3 which is more closely related to healthcare delivery than administrative HIT.
Finally, among the relevant studies, performance measurements have varied. Dependent variables of hospital performance have included net patient revenue, 30 mortality rate, 31 readmissions, and 32 hospital margins. 33 Each of these variables is limited as a reflection of comprehensive hospital performance.
Baker et al. 34 collected data from 1236 health organizations, proposed dynamic models, and suggested that future work should consider organizational performance measures. However, physicians, nurses, and patients are in general agreement that health outcomes and saving lives, not profit, should be the primary aim of hospitals, and financial return should not be the measure of HIT performance.
What is needed is more study designs that include longitudinal evaluations, which are able to detect time-sensitive and other diverse effects of HIT adoption.35,36 The above shortcomings are considered by our hypothesis in this study, that there are regional differences in the efficiency with which HIT has been adopted in China, and these differences are related to fiscal factors.
Methods
Data and variables
Consistent with Sharma et al., 3 our definition of HIT concerns the collection and delivery of clinical patient data that is relevant to diagnosis and treatment, specifically, EMRs and picture archiving and communication system (PACS). PACS is an information system used to acquire, store, and retrieve medical images. 37 In accordance with the CHIMA (China Hospital Information Management Association) survey, we define EMR specifically as basic EMR comprising electronic clinical documentation, testing and imaging results, computerized provider order entry, and decision support (i.e. clinical guidelines and reminders, drug–allergy alerts, and drug–drug interaction alerts). These functions must be applied in all major clinical departments of a hospital.
The data pertaining to HIT were extracted from the Annual Investigation Report on Hospital Information in China, supported by CHIMA. The annual survey was compiled from responses to a hospital questionnaire on the adoption of HIT. While the survey was not mandatory, the response rate was rather high (average validated hospital questionnaire: 806/year) as published by the Health Bureau. From the survey, EMR and PACS adoption were determined from the response to the survey item, “Status of adoption of EMR system/picture archiving and communication system: (1) implement, (2) plan to build, and (3) is not being considered.” The detailed survey is available on the CHIMA website (www.chima.org.cn).
Included are the data from 31 Chinese regions (provinces and municipalities) for 9 years from 2007 to 2015 (279 observations), dependent upon availability. The percentage of hospitals in the region using EMR and/or PACS was calculated as input factors.
The following health economic factors, one output and six inputs, were based on previous studies,38–42 and were obtained from the China Health Statistics Yearbook. OEit is the number of outpatient and emergency room visits per 1000 personnel (output). BEDit is beds per 1000 personnel, which refers to total active beds in medical facilities. HSit denotes healthcare staff per 1000 personnel, including physicians, nurses, other clinical staff, administrative staff and other nonclinical staff, according to the statistical source of the yearbook. TIit is the total input per 1000 personnel, which includes medical income, government subsidy and other income, which ultimately results in an increase in medical services. NAit denotes the net assets, defined as the the assets of the hospital minus all liabilities, and represents the capital size and economic strength. HWit is the wages of the healthcare staff per capita. CSit is the cost of inpatient stay per capita.
Statistical methods
The stochastic frontier analysis provides a simple description of the associations among the production or service processes involved in the transformation of inputs into outputs. Since the seminal works by Meeusen and van Den Broeck 43 and Aigner et al., 44 it has become a popular tool to estimate efficiency. Stochastic errors are allowed in stochastic frontier models and decomposed in two parts for the inclusion of statistical noise and inefficiency. We adapted the time-varying estimation model of Kumbhakar 45 to assume the distribution of technical inefficiency, from which the efficiency score was calculated.
The provincial HIT adoption technical frontier function is given by

In this equation, OEit is the number of outpatient and emergency room visits per 1000 personnel for province i at time t. Xit is a vector of control variables that affect the efficiency of HIT adoption, including BEDit, HSit, TIit, NAit, HWit, CSit. EMRit and PACSit reflect HIT adoption rate for province i at time t; vit is the normally distributed error term; and µit indicates the level of HIT inefficiency for province i at time t, with half-normal distribution.
The level of HIT technical efficiency can be expressed as follows

EFit is the efficiency score of HIT adoption for province i at time t, ranging between 1 (100% efficient) and 0 (100% inefficient).
Moran’s I and Local Indicators of Spatial Association (LISA) were examined for the efficiency score. Moran’s I is widely used in the analysis of geographic differences in health variables, 46 with values ranging between −1 and +1 (negative and positive autocorrelations, respectively). If there is no global autocorrelation or no clustering, LISA was used to explore the local level spatial cluster or outlier, 47 which could map the structure of spatial autocorrelation to the units of observation inferentially. 48 Four kinds of hotspots can be explored: high–high cluster, which represents a high-value neighborhood; low–low cluster, a low-value neighborhood; high–low spatial outlier, or a high-value area surrounded by low-value neighbors; and low–high spatial outlier, which makes a low-value area salient in a high-value neighborhood. 49 For more details, please refer to Anselin’s 47 work.
The stochastic frontier analyses were conducted using Stata SE 14.0 software, and the spatial patterns were analyzed using GeoDa version 1.12 (University of Chicago). Geographical information was obtained from the National Geomatics Center of China (http://ngcc.sbsm.gov.cn).
Results
Descriptive statistics
The adjusted variables were for 31 Chinese regions (provinces and municipalities) over a period of 9 years from 2007 to 2015 (Table 1). Currency units are expressed in ¥1000 RMB and are converted by the gross domestic product implicit price deflator to 2007 prices.
Descriptive statistics of the measurements.
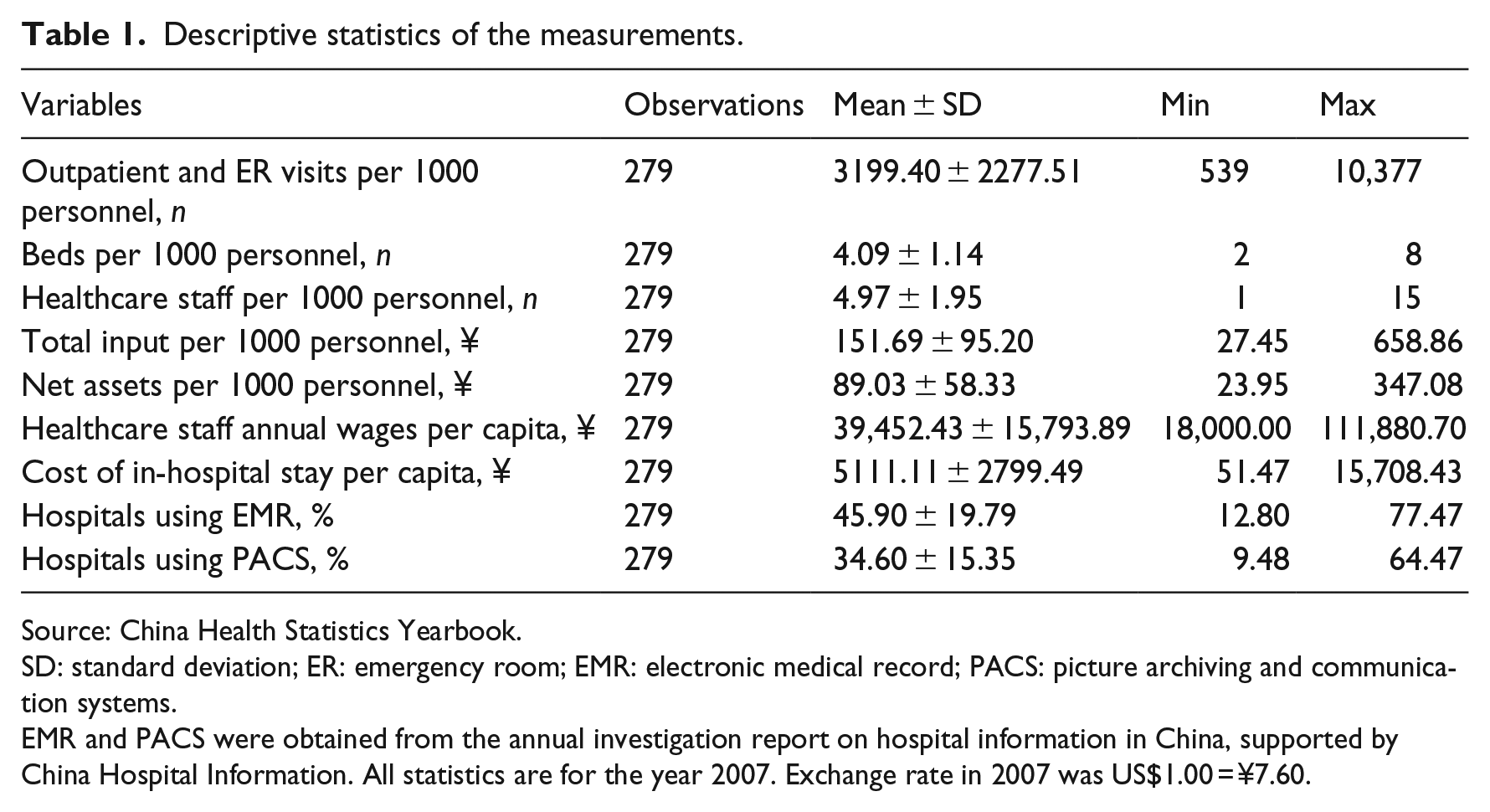
Source: China Health Statistics Yearbook.
SD: standard deviation; ER: emergency room; EMR: electronic medical record; PACS: picture archiving and communication systems.
EMR and PACS were obtained from the annual investigation report on hospital information in China, supported by China Hospital Information. All statistics are for the year 2007. Exchange rate in 2007 was US$1.00 = ¥7.60.
During the 9 years, China’s total health input increased by 46.9 percent, from 7.94 to 11.66 billion RMB. Healthcare staff per 1000 personnel increased by 68.6 percent, from an average of 3.5 to 5.9. The percentage of hospitals using EMR and PACS increased from 19.6 to 68.2 percent, and 17.1 to 44.0 percent, respectively.
Efficiency estimates
Figure 1 illustrates the Chinese healthcare efficiency of all the 31 regions (provinces and municipalities) and mean efficiency scores over 9 years. Efficiency has declined by varying degrees during the 9 years. The efficiency scores decreased rapidly from 2007 to 2010, but this decline then ceased after 2010. The mean estimated healthcare efficiency score was 0.53 ± 0.17 across the 31 regions from 2007 through 2015 in China.
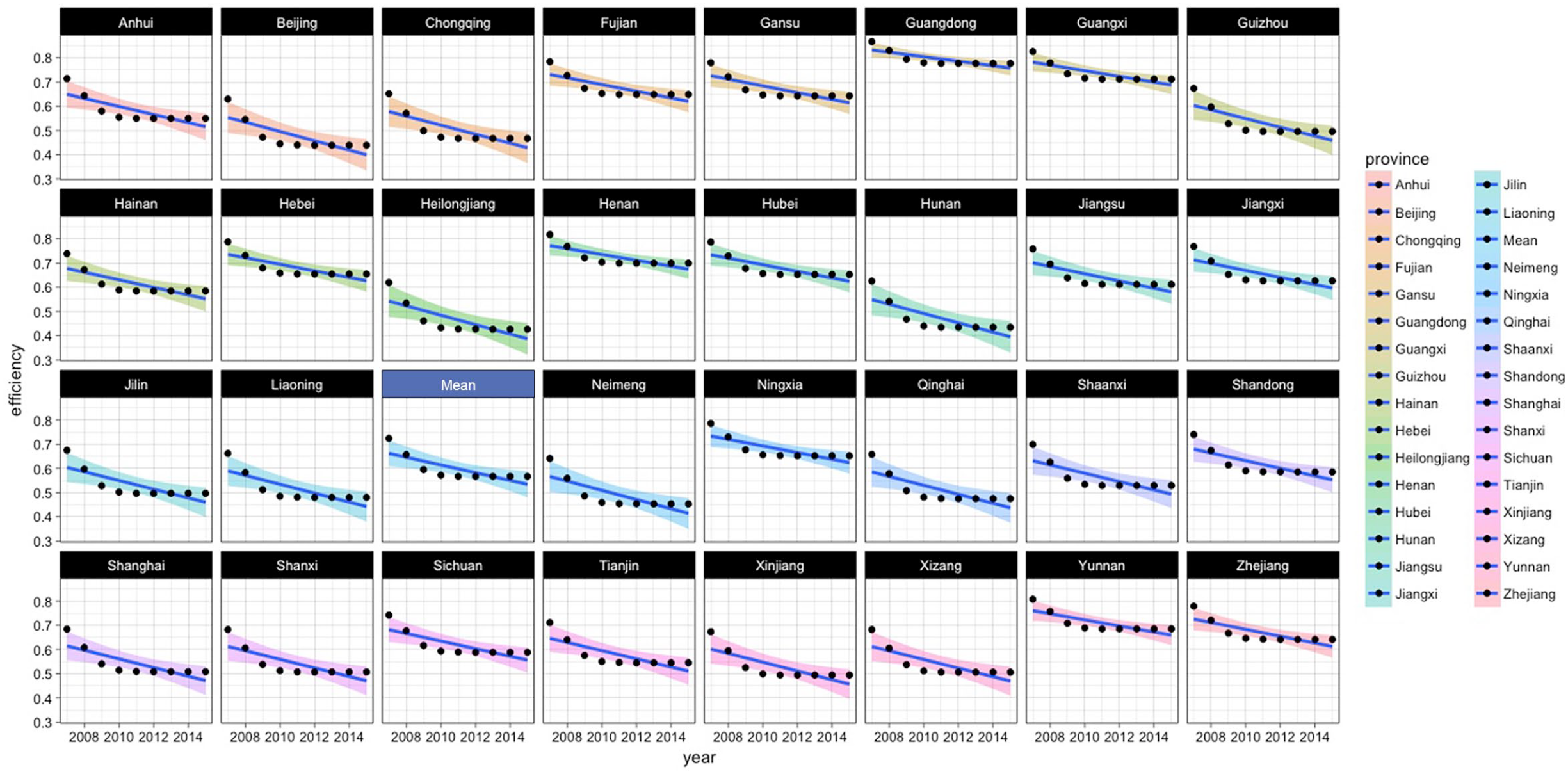
HIT efficiency of 31 regions in mainland China during 2007–2015.
Stochastic frontier parameters
Parameters of stochastic frontier models were estimated and are shown in Table 2. Total input and EMR are strongly significant and positive, while the percentage using PACS is significant and negatively associated with healthcare efficiency. There was no significant effect shown by the number of beds or healthcare staff or their wages.
Stochastic frontier estimation results of China HIT (2007–2015).
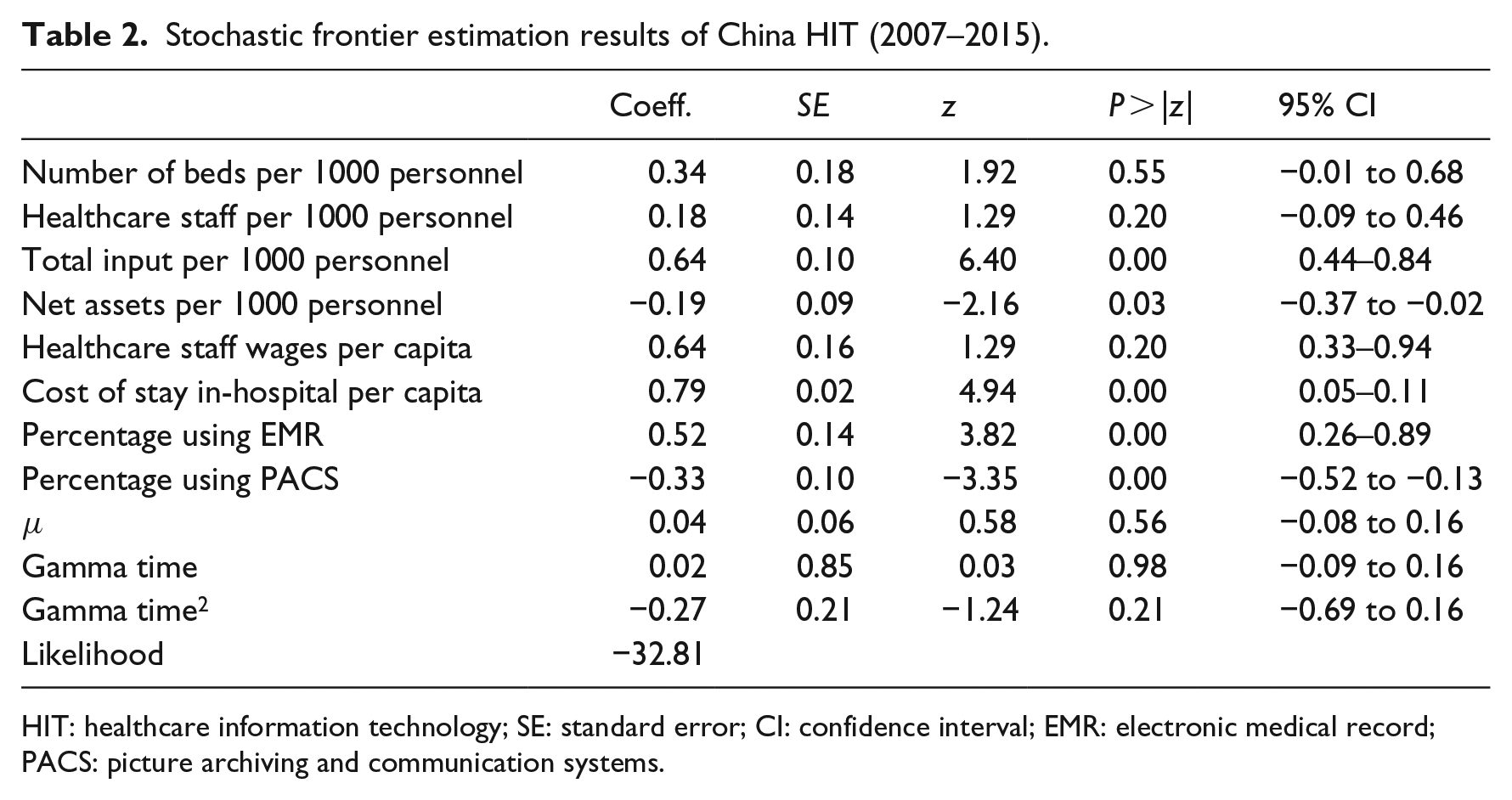
HIT: healthcare information technology; SE: standard error; CI: confidence interval; EMR: electronic medical record; PACS: picture archiving and communication systems.
Spatial analysis results
Figure 2 depicts a quantile map of mean HIT efficiency of the 31 regions (provinces and municipalities) from 2007 through 2015 in mainland China. In general, the HIT efficiency in the southeast is higher than in the northwest, which coincides with the geographical distribution of China’s economy. Interestingly, despite being the three biggest metropolises, Beijing, Shanghai, and Chongqing performed rather poorly during the study period, with mean efficiency scores of 0.50, 0.56, and 0.67, respectively. Less developed regions in west China, Gansu, Ningxia, and especially Guangxi, performed beyond expectations, with mean efficiency scores of 0.84, 0.87, and 0.91. Moran’s I test was needed to analyze the existing spatial autocorrelations.
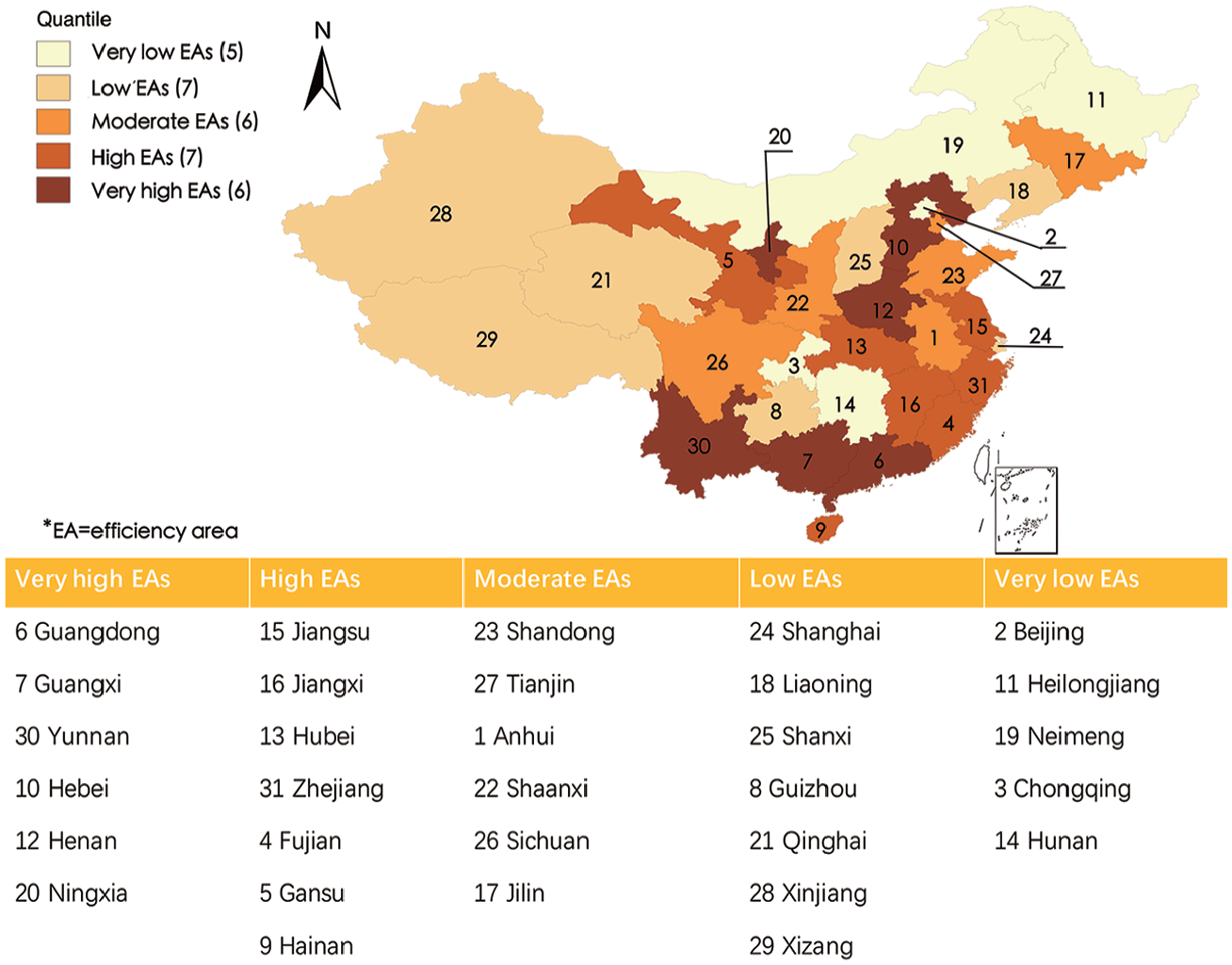
Quantile map of mean healthcare efficiency of 31 regions.
The spatial correlations were conducted for the 31 areas in each of the years 2007, 2011, and 2015. First, with standardized spatial weight matrix
The individual correlations were obtained via LISA analysis as shown in Figure 3; positive and negative correlations are shown as blue and pink, respectively. For example, pink areas in Anhui and Jiangxi show a significant high–low spillover effect, which represents high values surrounded by low values at the neighborhood level (Figure 3(a)). Blue in Beijing, Shanxi, Heilongjiang, Xinjiang, and Hunan indicate low–low clusters, where low values are surrounded by low values at the neighborhood level. Low clustering is shown in gray. The westernmost and northernmost areas of China show low efficiency and indicate an inability to obtain resources and techniques from their neighbors.
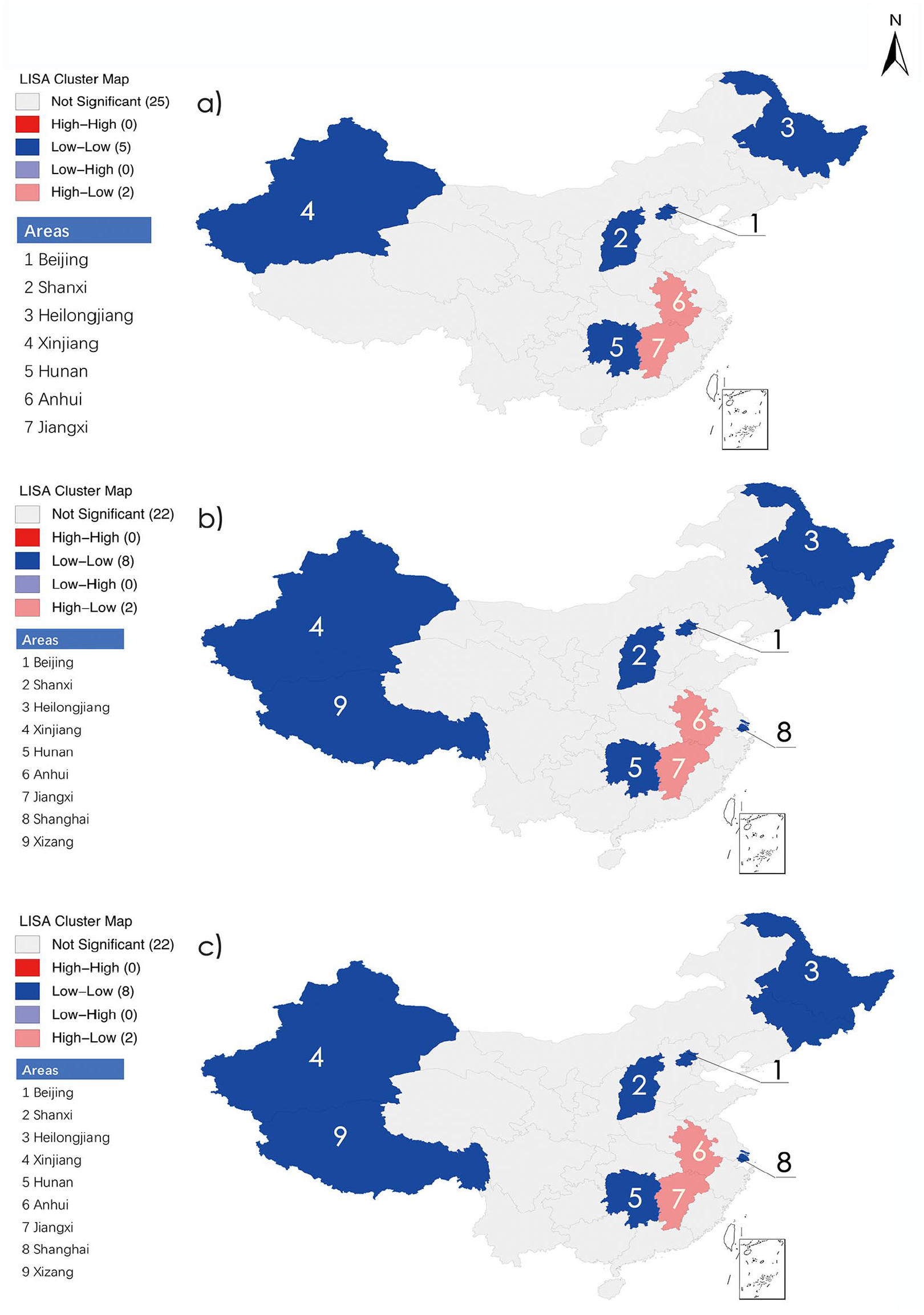
LISA test for a local spatial autocorrelation: (a) 2007 efficiency spatial cluster, (b) 2011 efficiency spatial cluster, and (c) 2015 efficiency spatial cluster.
Discussion
Main findings
China has made great economic achievements in the past few decades. While the quantity and quality of medical services have increased, so too has the inefficiency in the allocation of health resources across regions. No other studies have examined the spatial clustering of efficiency in the healthcare system of China. However, this study determined that the efficiency of technical healthcare has decreased, and regional differences expanded in the years 2007 through 2015.
In March 2009, as part of the new healthcare reform, the Chinese government set a goal to achieve universal health coverage by 2020. 50 This reform reversed the tendency for commercialization in the public hospitals, which have a leading role in healthcare. 51 The efficacy of these reforms may be reflected by the inflection in efficiency score observed in 2010 in this study (Figure 1).
Previous studies have shown that healthcare efficiency is positively associated with regional economic development.52,53 In this study, less developed areas had lower efficiency scores, including Xinjiang, Qinghai, and Xizang. Yet Ningxia, which is nationally recognized as a pilot of reform, achieved a high efficiency score and thus is an exception to this tendency. Ningxia has instituted Internet medical and health information services and a healthcare information platform across the entire province, including villages that have been inaccessible.
The LISA results indicated that more funds and technicians are needed for these low–low cluster effect areas. The areas with high–low or low–high spillover effect should receive more attention, as the low-efficient area can benefit from technical spillover from the high-efficient area. Policies should be formulated to promote the effective use of the HIT system and the technology flow from high efficiency areas, including the development of user-friendly applications and hands-on workshops. 54 HIT system designers should also consider the integration of different systems to avoid a digital divide.
The most important finding of this study is that the two components of HIT, EMR, and PACS, showed opposite and nonlinear associations with performance. The positive effects of EMR on the performance shown by our study are in accord with the overall results for HIT reported previously, specifically by meeting the demands of patients for quality healthcare, 55 providing data for allocating decisions by hospitals,20,56 reducing medical errors,57,58 and decreasing administrative expenses. 59 However, our study showed a negative association between PACS and performance, which is consistent with strong research that indicates no association between HIT investment and hospital performance.21,33,60,61
This may be due to several reasons. First, the uniformity of medical services in China is complicated by its vastness, socioeconomic and ethnic diversity, and imbalance in development. Unlike EMR, PACS can only be implemented in big hospitals, equipped with medical imaging systems, and staffed with professional technicians. Second, the quality and age of hospital medical equipment varies greatly, and often cannot be integrated with PACS. The expense of integrating PACS includes the replacement of outmoded medical imaging equipment. This makes the adoption of PACS more complicated than conversion to EMRs. According to the 2016 CHIMA report, 62 the adoption rate for EMR systems by hospitals is 83.4 percent, while that of PACS is only 60.5 percent. Third, EMR was implemented earlier and more vigorously than PACS. These barriers may help prevent improvements in healthcare performance. Zhao et al. 63 found that it may be difficult for HIT systems to show a positive effect on hospital performance within 1–2 years.
Factors related to China’s healthcare performance
Net assets can help indicate the extent or scale of the region’s healthcare system. Generally, developed areas have larger net assets. For example, Beijing and Shanghai are ranked as the top two in net assets per 1000 personnel among the 31 regions. However, a large net asset is not always associated with high efficiency. In this study, net asset significantly but negatively correlated with performance, which agrees with other studies concerning the healthcare system in China. 53 This may be because of an imbalance in the distribution of healthcare resources. It is generally believed that superior healthcare resources are disproportionately allocated to economically developed areas. However, increasing visits from patients outside the area because of this belief can lead to spiraling overextension in resources and costs, and inefficiency.
The positive and significant effect of the cost of inpatient stay per capita on hospital performance observed in this study suggests that healthcare efficiency rises with investments in healthcare spending. This coincides with the research of Evans et al. 61 The finding that total input is positively associated with healthcare performance, is contrary to other previous studies.64,65 Because of the insufficient medical resources per capita and inadequate hospital infrastructure in China, more funding is needed.
This study broadens the understanding of HIT performance in several ways. First, by evaluating the effect of HIT on performance in China at the regional level, this study developed a means to assess HIT and maximize the positive effects of HIT, while avoiding the negative effects. In addition, two dimensions of HIT applications were differentiated, EMR and PACS, which adds depth to the analysis of HIT and its association with performance. Moreover, contrary to previous findings that suggest either a linear positive or negative overall effect of HIT on performance, this study proposes two opposite nonlinear associations between EMR or PACS and performance. The inputs and outputs of EMR balance, and are sufficient to justify its utilization. However, more funding and political support is needed to develop and integrate PACS, if a negative contribution to performance is to be avoided.
This may be the first study of HIT performance in China to use cross-sectional time-series (i.e. longitudinal or panel) data, which improves the accuracy of the estimate, and solves the problem of omitted variables. Finally, this study adopts a spatial perspective by analyzing the clustering effect of the efficiency score, and our finding offers important insights into the imbalance of development of HIT in China.
Limitations and future research
Three main limitations of this study point to future research opportunities. First, the focus of this study was on clinical HIT, including systems used for patient data collecting, diagnosis, and treatment, rather than administrative systems. Meredith 66 wrote that the true value of the technology becomes evident only when “separate islands of automation” start to integrate. Second, the sample was limited to the healthcare system in a single country, and such conclusions only apply to China. Therefore, more finely resolved data are needed in empirical research to reach a better understanding of HIT performance. Finally, this study assumes that HIT is used effectively in healthcare institutions. However, hospitals may differ when using these high-tech systems, and HIT utilization was not analyzed in this study.
To our best knowledge, this is the first study to analyze in detail the regional differences in HIT efficiency in China. We believe the findings of this study are valuable and will help administrators in improving HIT policies.
Conclusion
The adoption of HIT increased in China during the years 2007 through 2015, but healthcare performances and geographical differences in technical efficiency did not improve. Policymakers should differentiate the kinds of HIT, and regional differences should be considered in detail, especially with regard to financial and technical support.
Research Data
data – Supplemental material for The efficiency analysis and spatial implications of health information technology: A regional exploratory study in China
data for The efficiency analysis and spatial implications of health information technology: A regional exploratory study in China by Dan Li, Jianqian Chao, Jing Kong, Gui Cao, Mengru Lv and Man Zhang in Health Informatics Journal
Footnotes
Acknowledgements
The authors thank the participants for their cooperation in the study and to Medjaden Bioscience Limited for language editing.
Author contributions
All the authors confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship that are not listed. D.L. conceived/designed the study, collected primary data, analyzed data, drafted the manuscript, and gave final approval of the submitted version. J.C. and J.K. revised the manuscript and finally approved the submitted version. G.C. analyzed data for spatial clustering. M.L. and M.Z. collected primary data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 81872711) and the Nanjing Medical Science and Technology Development Fund (grant number YKK16196). The funding played no part in either the design of the study or the collection, analysis, and interpretation of data, or in writing the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.